
Abstract
Study Design
Retrospective cohort Study.
Objectives
To identify predictive factors for coronal imbalance after selective fusion in adolescent idiopathic scoliosis (AIS) with Lenke type 1 curves.
Methods
AIS patients with Lenke type 1 curve with A, B and C lumbar modifiers underwent selective thoracic fusion. The curve fulcrum flexibility and fulcrum bending correction index (FBCI) was studied. Coronal imbalance was defined as more than 2 cm of truncal shift or more than 2 cm list at two-year follow-up.
Results
A total of 301 patients were included in the study. Coronal imbalance at two-year follow-up was found in 38 patients (13%). At the preoperative stage, we found a significant difference in main curve flexibility with 66±15% in the balanced group and 60±15% in the imbalanced group (P = .032). At the immediate postoperative stage, mean curve correction was 71±13% vs 70±13% and mean FBCI was 112±29% vs 122±29% in the balance and unbalanced group, respectively (P = .031). Postoperative FBCI of more than 125% (third quartile) resulted in an odds ratio of 2.1 (95%CI:1.1-4.3) for coronal imbalance at two years (P=.031). No significant changes in fusion mass or LIV tilt was observed.
Conclusions
A decreased preoperative flexibility and a higher FBCI was significantly associated with coronal imbalance. A high FBCI is an indication of a curve correction that exceeds the inherent flexibility of the spine, and our results add to a growing body of evidence that “overcorrection” of the main curve can lead to postoperative imbalance.
Keywords
Introduction
Surgical treatment of adolescent idiopathic scoliosis (AIS) aims to correct deformity, and maintain a balanced spine while minimizing the number of fused segments without risking deformity progression in the unfused spine.1,2 Selective fusion in Lenke type 1 curves is generally recommended3,4 but is associated with a risk of distal or proximal decompensation as well as coronal imbalance. 5 Majdouline et al 6 surveyed 50 experienced spine surgeons and members of the Spine Deformity Study Group asking them to rank the most important goal of corrective surgery in AIS. There was overall agreement that sagittal and coronal balance were the most important parameters for an optimal correction. Coronal balance can be quantified by the coronal “list”, which is the distance between the coronal C7 plumbline and the central sacral vertical line (CSVL). However, while the head may be satisfactorily balanced over the pelvis, the patient may still exhibit a significant truncal imbalance. 7 Irrespective of the specific definition of coronal imbalance, they lead to unsatisfactory results,6,8 although the long-term implications of coronal imbalance are not known. The Harms study group in a multicenter study on 954 patients defined coronal imbalance as more than 2 cm deviation of the C7 plumbline to the CSVL. 9 They found coronal imbalance in 31% of patients on the immediate postoperative radiographs but noted a significant “rebalancing” at two-year follow-up with only 12% remaining imbalanced. 9 Ghandehari et al, 10 also using a cut-off of 2 cm noted a significant correlation between coronal balance correction and higher SRS-30 score in patients as well as higher treatment satisfaction. It is of interest to examine the frequency and cause of imbalance to optimize surgical results. Hence, the aim of the study was to access the rate of coronal imbalance and identify possible reversible predictors of imbalance.
Methods
We included AIS patients with a Lenke type 1 curve with A, B and C lumbar modifiers. No patients had limb length discrepancies. All patients were surgically treated over a 20-year period with selective fusion defined as a lowest instrumented vertebra at L2 or cranial. All patients were instrumented with alternate-level all-pedicle screw constructs with titanium rods and had two-year follow-up. All patients had only excisions of the inferior articular processes without further osteotomies or releases. A standardized correction maneuver with differential rod contouring, concave rod rotation followed by segmental concave distraction and convex compression. Radiographic variables were measured at the preoperative, immediate and two-year postoperative stages. Ethics was approved by the local institutional review board and written informed consent was obtained from all participants.
Preoperative flexibility of the main curve was assessed with fulcrum bending radiographs (FBR). The methods for obtaining FBR and determination of fusion levels have been reported in previous studies.11,12
From the standing whole spine posteroanterior radiograph, the following variables were measured: tilt of lower instrumented vertebra (LIV) and upper instrumented vertebra (UIV), major curve Cobb angle and apical translation of the main thoracic and lumbar curve. Additionally, we measured: • List was measured as the distance from the C7 plumb line to the CSVL. • Truncal shift was defined by measuring the perpendicular distance from the CSVL to a line that bisects the distance from the lateral edges of the rib margins in the mid thoracic level.
13
• Radiographic shoulder height (RSH) was defined as the height difference in the soft tissue shadow directly superior to the acromioclavicular joints.
14
• Fusion mass shift: a perpendicular line is drawn from the lower endplate of the LIV. Fusion mass shift is the distance from this line to the midpoint of the upper endplate of the UIV.
15
• Fusion mass angle was the Cobb angle measured from the upper endplate of the UIV and the lower endplate of the LIV. • LIV disc angle was measured as the angle between the inferior endplate of the LIV and the superior endplate of the LIV +1
The fulcrum-bending correction index (FBCI) of the main curve was calculated 16 :
FBCI = Curve correction/fulcrum flexibility * 100%
We defined patients as having coronal imbalance in cases of
1) More than 2 cm of truncal shift at two-year follow-up
13
OR 2) More than 2 cm list at two-year follow-up
17
Statistical analysis
The primary outcome was coronal imbalance at two-year follow-up. Data was reported as proportions (%), mean ± standard deviation or median with range, and data distribution was assessed by histograms. For the univariate comparative analysis, continuous data was compared between groups using unpaired, two-tailed t test or Wilcoxon rank sum test. Categorical variables were compared using Pearson’s chi-squared test. The significance level was set at .05.
Results
Baseline clinical and radiographic variables.
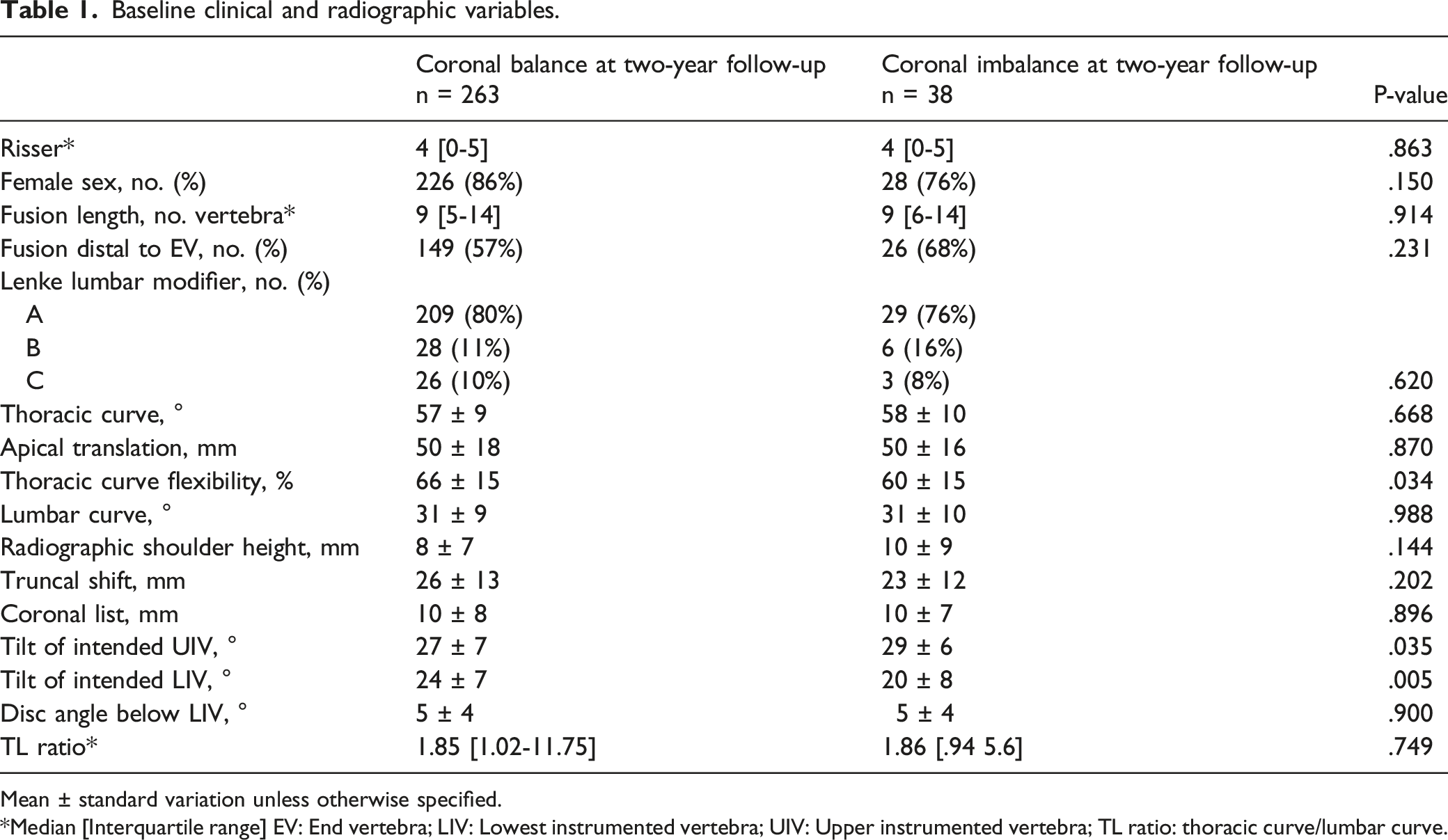
Mean ± standard variation unless otherwise specified.
Median [Interquartile range] EV: End vertebra; LIV: Lowest instrumented vertebra; UIV: Upper instrumented vertebra; TL ratio: thoracic curve/lumbar curve.
At two-year follow-up, mean FCBI was 103±32% in the balanced group vs 112±30% in the unbalanced group (P = .029). Thoracic and lumbar curve correction was similar in the balanced and imbalanced group, respectively (Table 3).
189 patients (63%) showed coronal imbalance preoperatively. 78 patients were imbalanced at the postoperative stage. At the two-year follow-up, 17/78 (21.8%) remained imbalanced. This imbalanced group (Figure 1) showed a lower preoperative flexibility (52±15% vs 65±15%) and a higher postoperative FBCI (133±32% vs 118±26%) (P = .040) compared to the 61 patients that corrected the imbalance. Left: Lenke type 1A with a 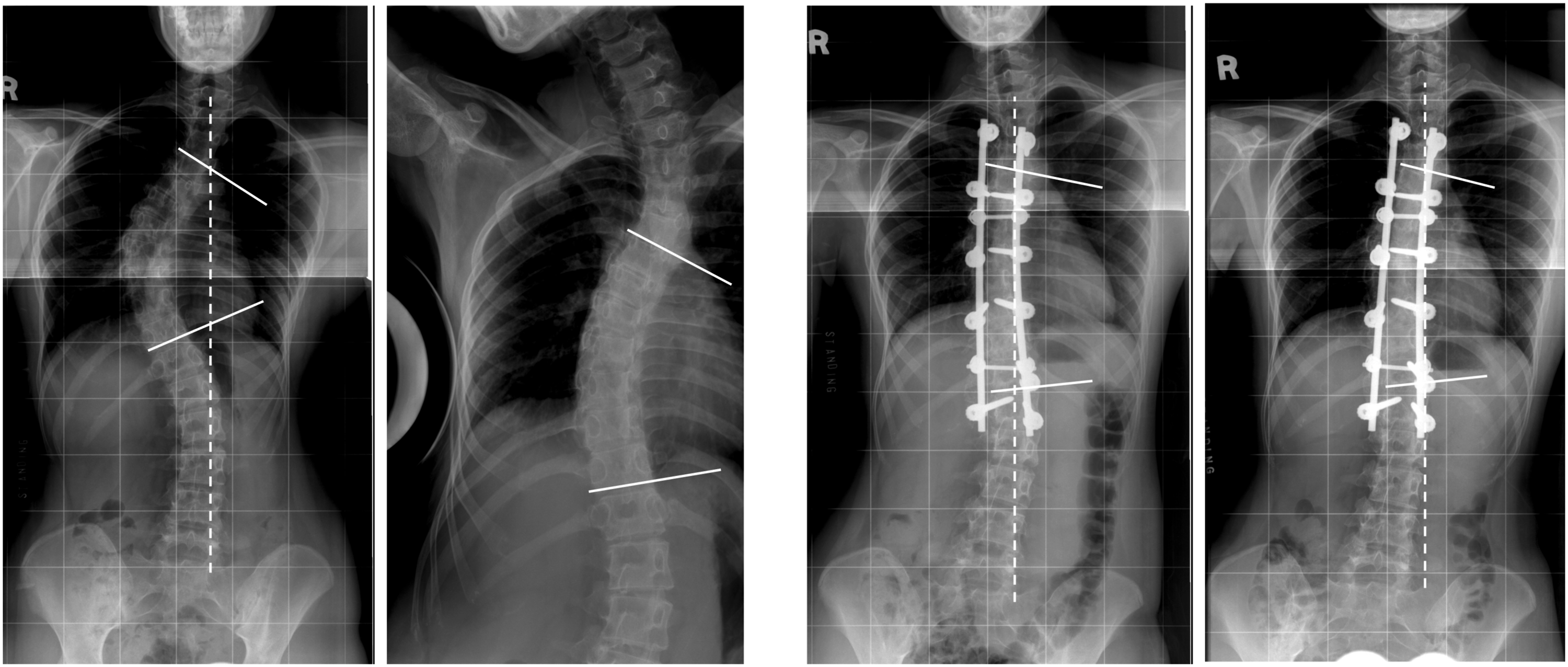
Postoperative variables according to two-year coronal imbalance.
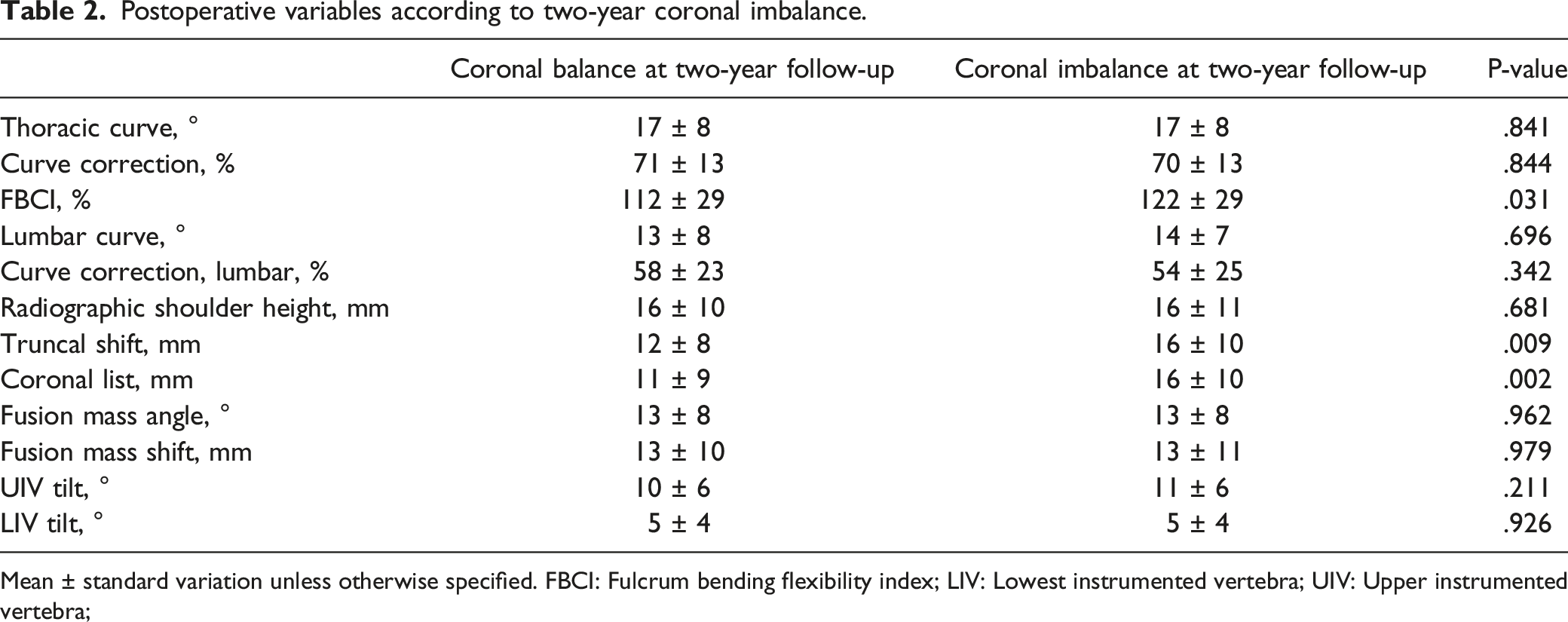
Mean ± standard variation unless otherwise specified. FBCI: Fulcrum bending flexibility index; LIV: Lowest instrumented vertebra; UIV: Upper instrumented vertebra;
Radiographic variables at two-year follow-up according to coronal imbalance.
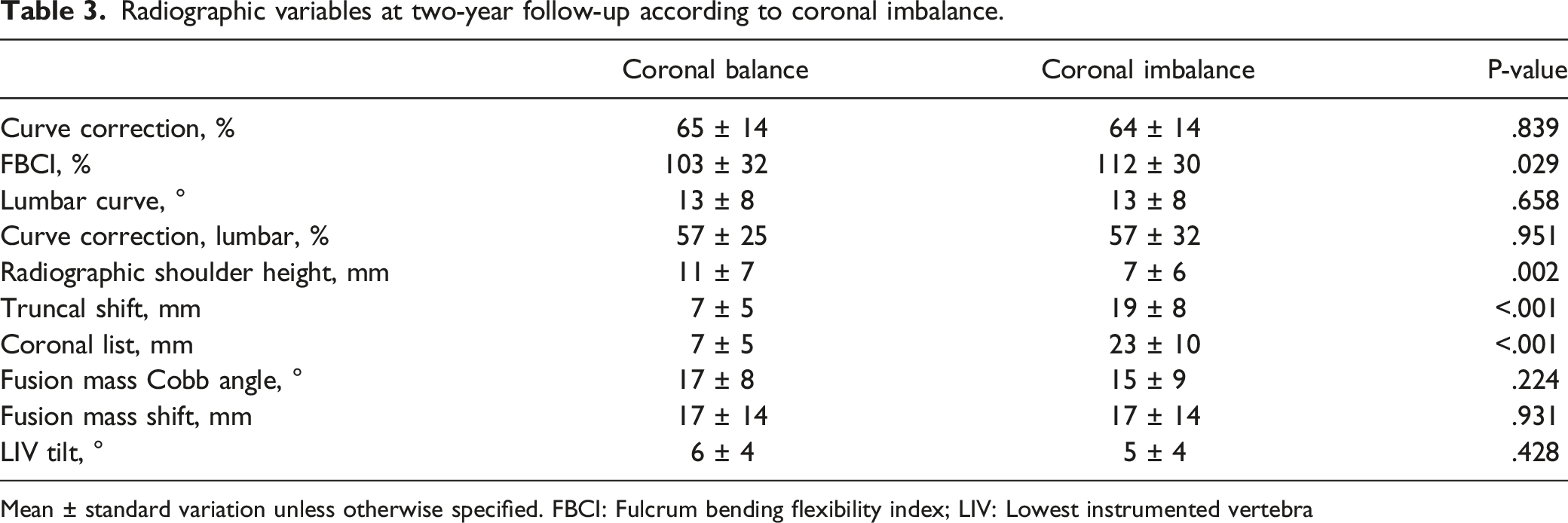
Mean ± standard variation unless otherwise specified. FBCI: Fulcrum bending flexibility index; LIV: Lowest instrumented vertebra
Post hoc analysis of lumbar modifier B and C curves. Postoperative variables according to two-year coronal imbalance.
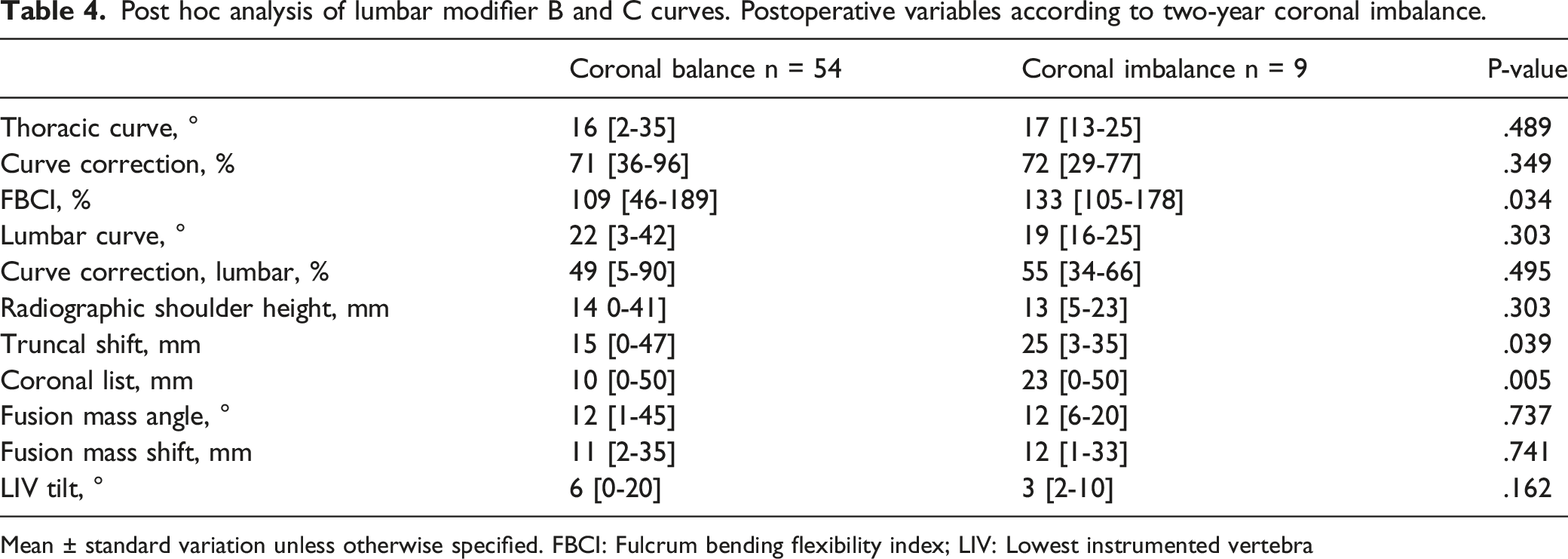
Mean ± standard variation unless otherwise specified. FBCI: Fulcrum bending flexibility index; LIV: Lowest instrumented vertebra
Discussion
Selective fusion in Lenke type 1 curves is the most frequent surgical procedure in AIS and the Lenke 1 curve is the most common. Many studies on coronal balance in AIS are limited by the inclusion of different curve types that behave differently in response to fusion. We studied a large cohort of homogenous curves (all Lenke 1) and focused on pre- and postoperative variables to identify potentially surgically addressable predictors of imbalance. The main difference was found in flexibility and postoperative FBCI. FBCI was developed as an expression of curve correction incorporating the preoperative flexibility. A FBCI of more than 100% indicates that the curve correction was more than the inherent flexibility of the curve. Modern implants and correction techniques have become increasingly powerful, and correction is often substantially more than the “natural” flexibility of the curve. Therefore, the secondary compensatory mechanism of the unfused spine and pelvis may become less predictable. Anari et al 18 found that very low preoperative flexibility was a substantial risk factor for severe imbalance (>4 cm). However, the rate of severe imbalance was less than 1% (n=9).
There are some studies indicating that a high level of correction may come at a cost in terms of a less balanced spine and torso. Thompson et al first described this phenomenon in 1990 using Cotrel-Dubousset instrumentation showing that deformity correction excessive in relation to curve flexibility resulted in spinal imbalance. 19 Dobbs et al 20 reported on selective fusion (anterior or posterior) in type B and C lumbar modifiers and found that postoperative balance was better in patients where the thoracic curve was “close to but not more” than the push-prone correction. Imrie et al showed that curve correction above 80% resulted in a loss of thoracic kyphosis. 21 It is important to note that in this cohort of patients, only type 1 osteotomies were performed. Larger scale osteotomies will achieve further correction of the deformity. However, through this study’s findings, this may be a greater risk factor for coronal imbalance postoperatively. Overcorrection especially in stiffer curves may lead to inability of residual spinal segments to compensate. This relationship will require further study to elucidate.
Looking further at the cohort, we found that at the postoperative stage, the balanced and unbalanced groups had only minor differences in truncal balance and listing (Table 2). Out of the 78 patients who were imbalanced at the postoperative stage, only 17 remained imbalanced at two-year follow-up. When comparing the postoperative and the two-year FU parameters (Table 2 and 3) the coronal imbalance does not seem to be driven by an increase in the lumbar curve or distal adding-on. Lumbar curve correction was 57% in both groups and the LIV tilt was similar. Also, the fusion mass angle and shift remained stable, but here was a significantly higher RSH in the balanced group. Our group previously showed that low flexibility (and high FBCI) was a predictor for postoperative shoulder imbalance. 14 The results indicate that most of the postoperative compensation occur in the proximal spine. We did not record proximal curve flexibility or magnitude in our prospective cohort of Lenke 1 curves so we cannot elaborate further on this hypothesis. A few studies have suggested that Type 1C curves may be at higher risk of imbalance and should be analyzed separately.22,23 We found similar results when looking at the lumbar modifiers but the difference in postoperative FBCI between the balance and imbalanced groups was even more pronounced (109% vs 133%).
The main strength of the current study is a homogenous patient sample of only selective fusion of Lenke type 1 curves. This was a single center study, which limits the bias of different instrumentation and correction strategies. In addition, pelvic obliquity may be an important variable to influence coronal alignment but unfortunately this data was not collected in this cohort. Furthermore, data on Lenke 1A-R and 1A-L curve patterns was not collected and may be important for postoperative adding-on. 24 Although coronal imbalance is generally considered nonsatisfactory, only a few studies6,8,25 have described an association between coronal imbalance and worse patient-rapported outcome (PRO). We did not have a sufficient number of patients with pre- and postoperative PRO data to report in this study. As with all cohort studies on AIS patients, clinical implications of radiographic imbalance may not be evident until much later in life than the typical two-year follow-up. Pedicle-screw instrumentation has now been practiced for over 20 years and hopefully we will soon see long-term data on these patients.
Conclusion
Coronal imbalance in type 1 AIS can be expected in 10% of cases. A decreased preoperative flexibility and an increase in FBCI was significantly associated with an increased rate of imbalance. Future studies may clarify whether correction strategy should aim to “under correct” less flexible curves or extend the fusion to address this issue.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was supported by the RGC Research Impact Fund (R5017-18F).
Ethical Approval
This study was ethically approved by Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (IRB reference number: UW 15-596)
Informed Concent
All patients provided written informed consent to have their clinical and radiological data used for research.