
Abstract
Study Design:
Retrospective multicenter study.
Objectives:
To compare the selective anterior spinal fusion (ASF) versus posterior spinal fusion (PSF) on postoperative pulmonary function testing (PFT) whether thoracotomy with separation of the diaphragm by anterior approach influences the PFT in thoracolumbar and lumbar adolescent idiopathic scoliosis (AIS).
Methods:
A multicenter series of AIS patients who underwent selective spinal fusion were retrospectively reviewed. Seventy-nine female patients were included (mean 15.8 years). There were 35 patients in the ASF group and 44 patients in the PSF group. Patient demographics, radiographic measurements, and PFT data from preoperative to 2-year follow-up were analyzed.
Results:
Preoperatively, there were no significant differences in PFTs between the groups. The ASF group patients were more likely to undergo shorter fusions (4.5 instrumented vertebral levels) than those in the PSF group (5.2 levels). At 2-year follow-up, forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) in ASF group were statistically lower than those in PSF group. When comparing preoperative and 2-year changes on each procedure, only %FVC showed significant difference in ASF while FVC, FEV1, and %FEV1 did not. Meanwhile, the ASF group showed a significant decrease in FVC at 6 and 12 months compared to preoperative values. In PSF group, there was a decrease at 6 months, returned to preoperative value at 1-year follow-up.
Conclusions:
Pulmonary function after ASF and PSF was similar at 2 years; however, anterior group did not return to the baseline at 6 months and 1 year suggesting anterior approach may affect early postoperative pulmonary function.
Keywords
Introduction
One of the goals for surgical correction of adolescent idiopathic scoliosis (AIS) is to achieve spinal balance while maintaining or improving pulmonary function. There is a well-known relationship between progression of the thoracic deformity and deterioration of pulmonary function. Several additional factors such as curve rigidity, number of vertebrae involved in the thoracic deformity, a more cephalad location of the curve apex, and concomitant sagittal plane deformity have also been reported to influence pulmonary function testing (PFT). 1 -5 PFT after surgical correction has been well investigated. 6 -11
In contrast to thoracic curves, PFT in thoracolumbar and lumbar (TL/lumbar) curves has not been well investigated because it is not directly related to the chest cage deformity. In most TL/lumbar curve with moderate thoracic curve cases, selective spinal fusion is considered an appropriate and effective surgical treatment. Selective anterior spinal fusion (ASF) has been a choice of the treatment in TL/lumbar curves AIS. 12 -16 One of the advantages of ASF is the ability to achieve good coronal correction with fewer levels fused than in posterior spinal fusion (PSF). However, the anterior approach to the thoracolumbar spine requires thoracotomy with separation of diaphragm. Currently, similar curve correction of TL/lumbar curves approached posteriorly has been reported using segmental pedicle screw fixation. 17,18 The objective of this study was to compare the effect of ASF versus PSF on PFT in TL/lumbar curve and to analyze an influence associated with surgical approach.
Methods
This is a retrospective multicenter cohort that recruited female AIS patients who were diagnosed thoracolumbar or lumbar scoliosis (Lenke type 5 and 6) and underwent selective ASF or PSF with an upper instrumented vertebra of T9 or below (Figure 1).
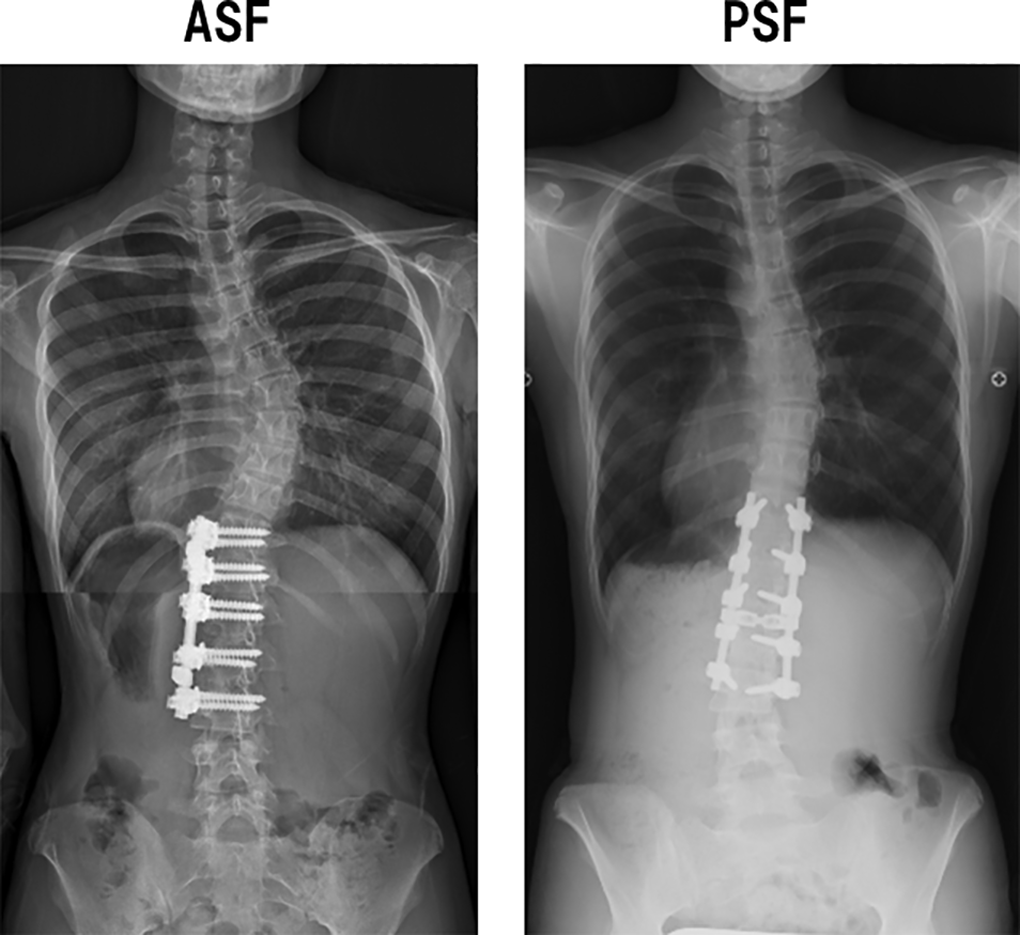
Surgery after anterior spinal fusion (ASF) and posterior spinal fusion (PSF).
PFT prior to surgery and at 2-year postoperative follow-up was performed in all patients. In addition, PFT at 6 months and 1 year postoperatively was performed in 36 patients. Forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) were obtained from the PFT exams. Percent predicted values for each parameter were adjusted according to the report by Polgar et al 19 utilizing gender- and height-matched standards.
Preoperative radiographic evaluation including full length, standing anteroposterior (AP) and lateral radiographs of the spine were obtained. Radiographic parameters, including thoracic and lumbar curves (standing, bending), thoracic kyphosis (T2 to T12 and T5 to T12), lumbar lordosis (T12 to sacrum), and coronal and sagittal balance were recorded. At 2-year follow-up, degree of correction of each curve was assessed.
Statistical data was analyzed using SPSS 23 (IBM Corp, Armonk, NY). Each variable was reported as the mean ± standard deviation. A P value <.05 was considered significant.
Results
Overall Description
Seventy-nine female patients were included in the study. Mean age at the time of the surgery was 15.8 ± 2.0 years (range 11-19 years). There were 74 patients with Lenke type 5 curves and 5 with type 6. The sagittal modifier was normal in 69, hyper in 4, and hypo in 6 patients. There were 35 patients who underwent ASF and 44 patients who underwent PSF. Before 2009, ASF was performed in 3 institutes but after 2010, only PSF was selected in all institutes. The distribution of upper instrumented vertebra (UIV) was T9 in 4, T10 in 11, T11 in 46, and T12 in 18 patients. The lower instrumented vertebra (LIV) was L2 in 5, L3 in 72, and L4 in 2 patients. The mean number of levels fused was 4.9 ± 0.8 vertebrae.
The radiographic and pulmonary parameters are presented in Table 1. The average preoperative TL/lumber and thoracic Cobb angles were 49.3° ± 8.1° and 29.6° ± 9.8°, respectively. At 2-year follow-up, these angles decreased significantly to 18.4° ± 5.3° and 20.1° ± 8.2°, resulting in correction rates of 62.1% and 32.9%, respectively. The average preoperative and 2-year follow-up thoracic kyphosis and lumbar lordosis did not show significant change.
Overall Radiographic and Pulmonary Parameters.
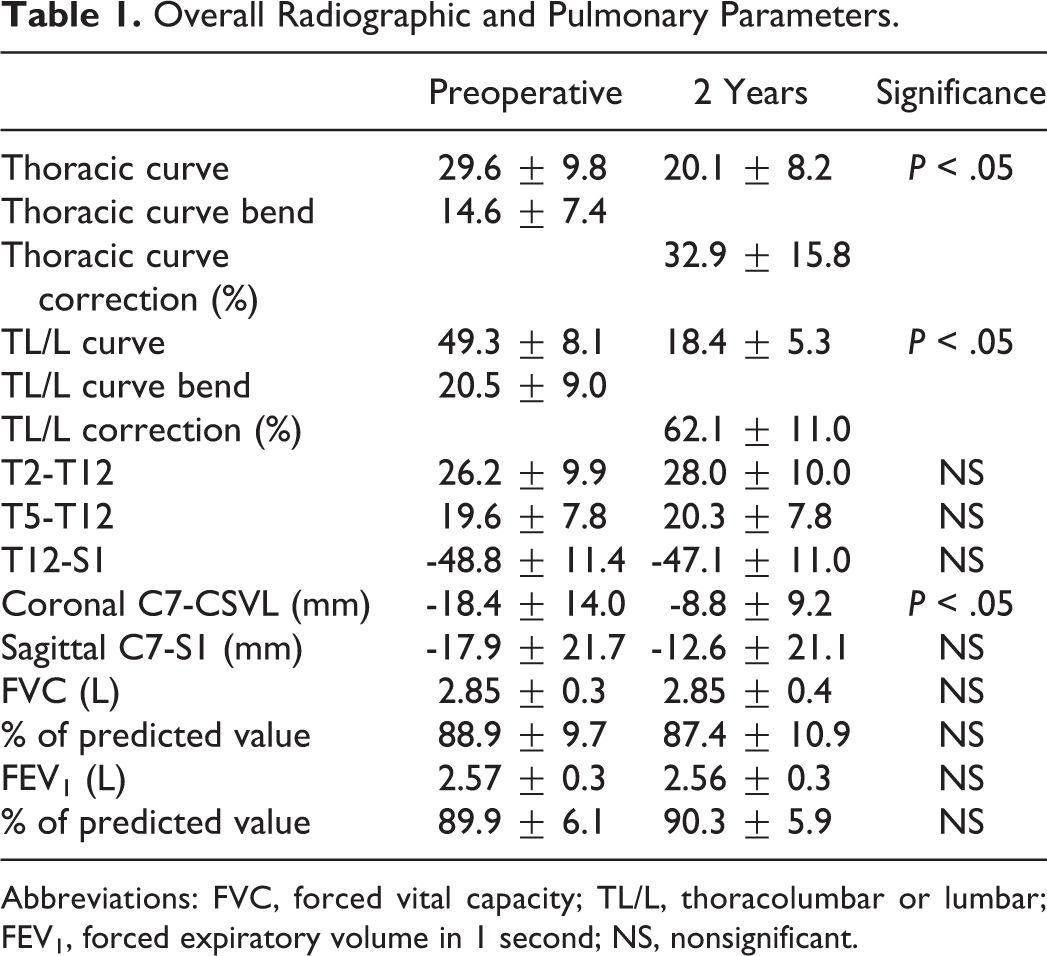
Abbreviations: FVC, forced vital capacity; TL/L, thoracolumbar or lumbar; FEV1, forced expiratory volume in 1 second; NS, nonsignificant.
The average preoperative and 2-year follow-up values of FVC, %FVC, FEV1, and %FEV1 are also shown in Table 1. Compared with preoperative values, no statistically significant changes were observed at 2-year follow-up.
PFT and Radiographic Parameters Depending on the Surgical Procedure
Fusion levels of the ASF group patients were shorter (4.5 instrumented vertebrae) than of the PSF group (5.2, P < .05). Tables 2 and 3 show the demographic and radiographic data, respectively, of each group.
Demographic Data of ASF and PSF.
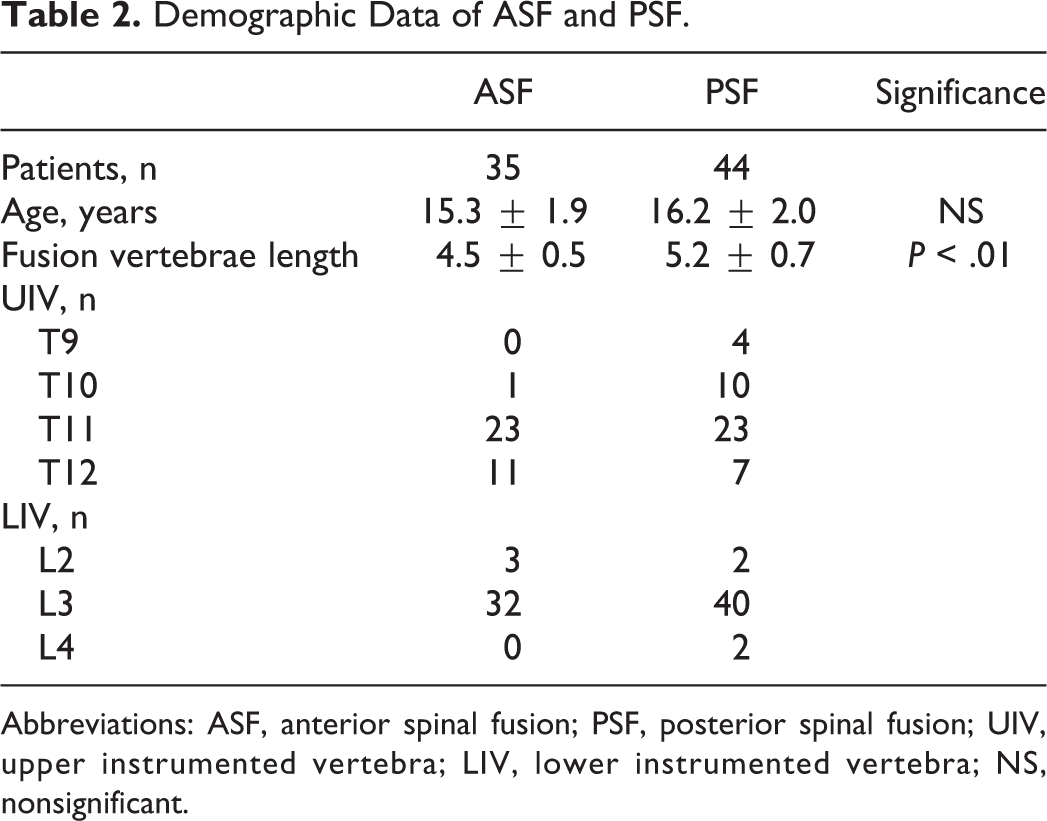
Abbreviations: ASF, anterior spinal fusion; PSF, posterior spinal fusion; UIV, upper instrumented vertebra; LIV, lower instrumented vertebra; NS, nonsignificant.
Comparison of Radiographic Parameters.
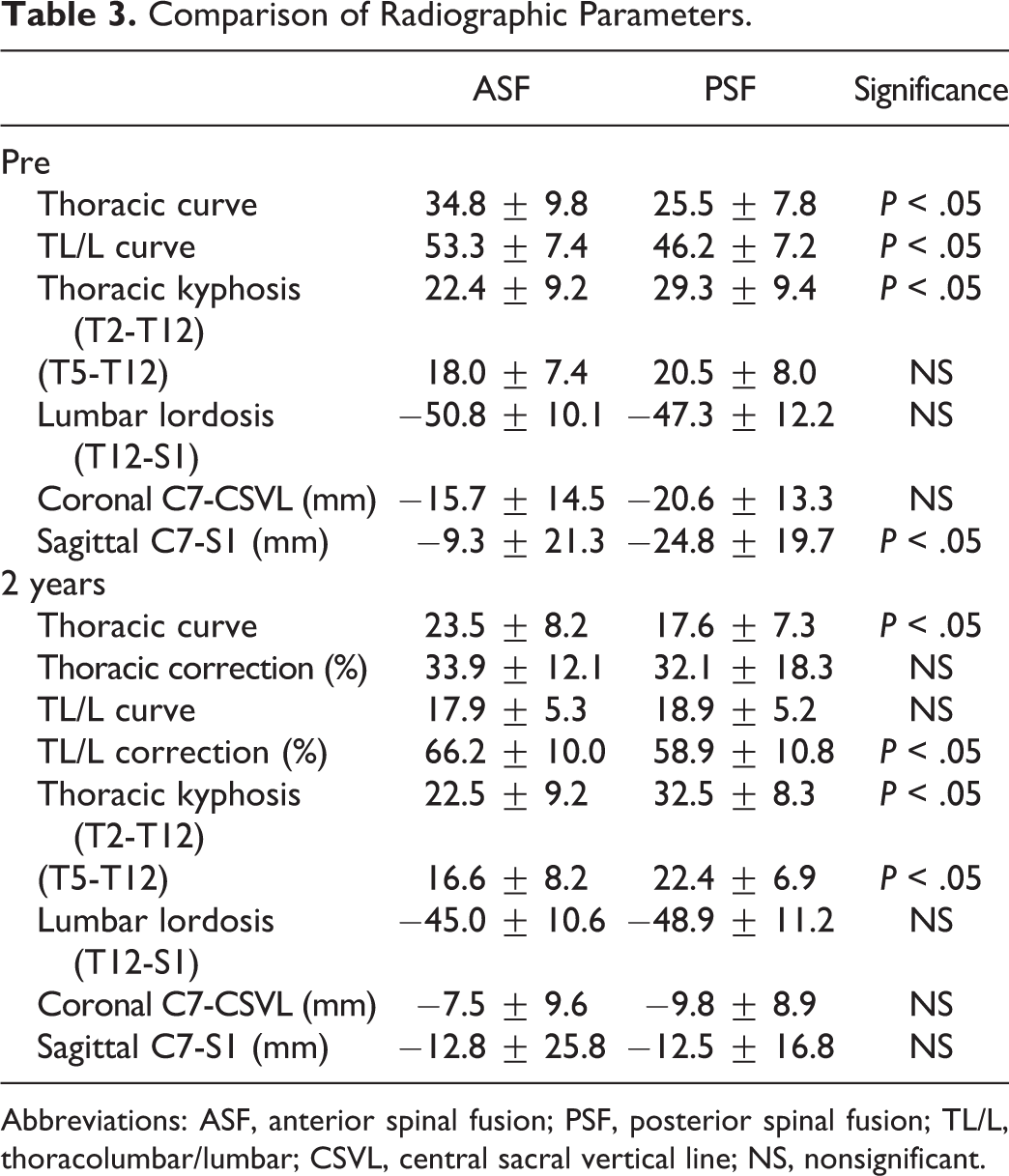
Abbreviations: ASF, anterior spinal fusion; PSF, posterior spinal fusion; TL/L, thoracolumbar/lumbar; CSVL, central sacral vertical line; NS, nonsignificant.
There were no significant differences in preoperative PFT between the groups. At 2-year follow-up, FVC and FEV1 in the ASF group were significantly lower than those of the PSF group (Table 4). When comparing preoperative and 2-year follow-up PFT on each procedure, there were no significant differences in FVC, FEV1, and %FEV1. There was a significant difference of 2-year follow-up %FVC in ASF group; however, this 1.8% difference seems to have no clinical relevance at 2-year (Table 5).
Comparison of PFT Based on the Surgical Procedure.
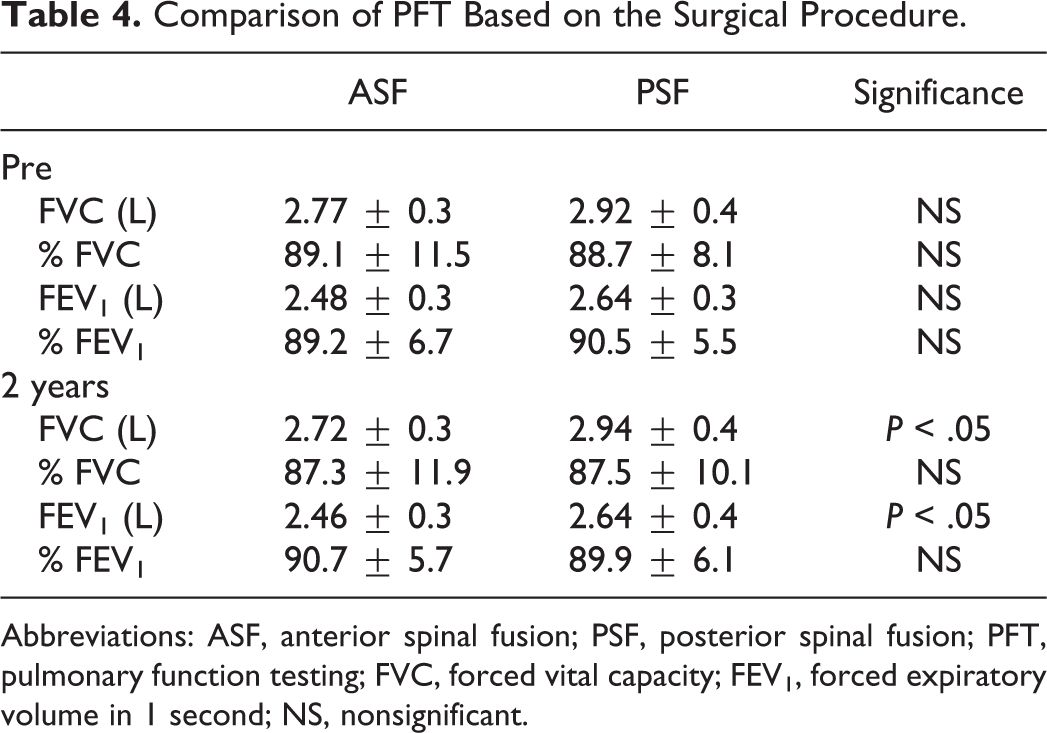
Abbreviations: ASF, anterior spinal fusion; PSF, posterior spinal fusion; PFT, pulmonary function testing; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; NS, nonsignificant.
Comparison of the Preoperative and 2-Year Pulmonary Parameters.
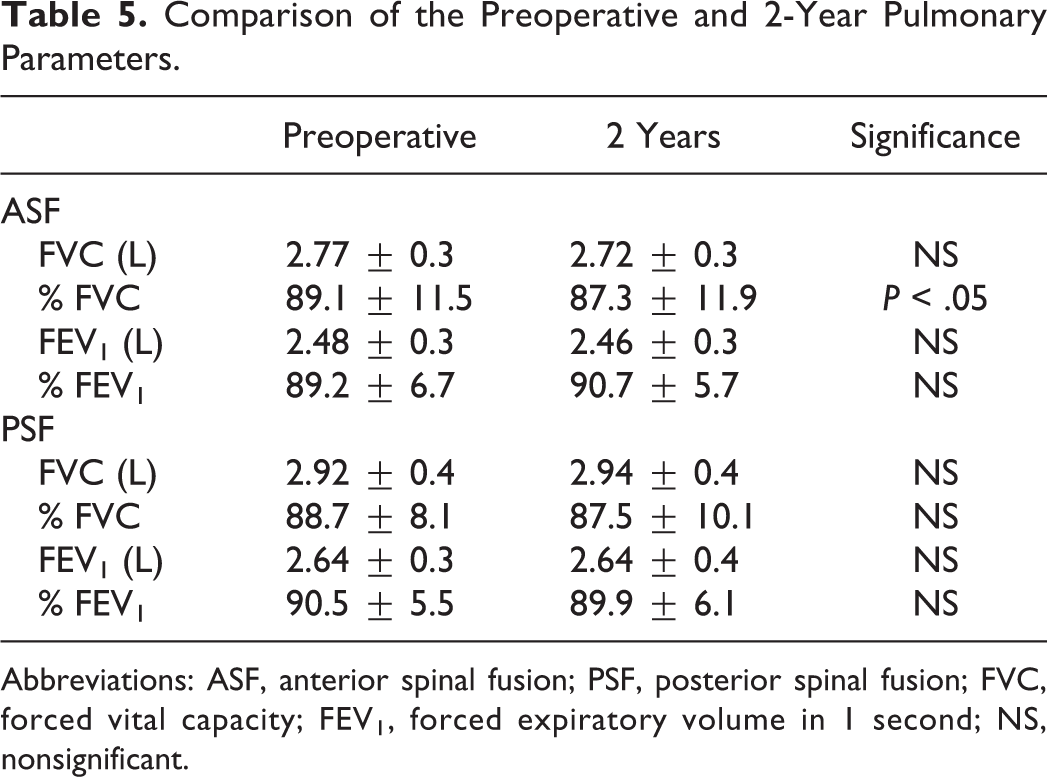
Abbreviations: ASF, anterior spinal fusion; PSF, posterior spinal fusion; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; NS, nonsignificant.
Comparison of Pulmonary Function in the Early Postoperative Period
Thirty-six of 79 patients underwent additional pulmonary function testing at 6 months and 1 year. The ASF group showed decreasing in FVC at 6 months and 1 year postoperatively compared with preoperative values. FVC in PSF group also decreased at 6 months but returned to preoperative value at 1-year follow-up (Figure 2).
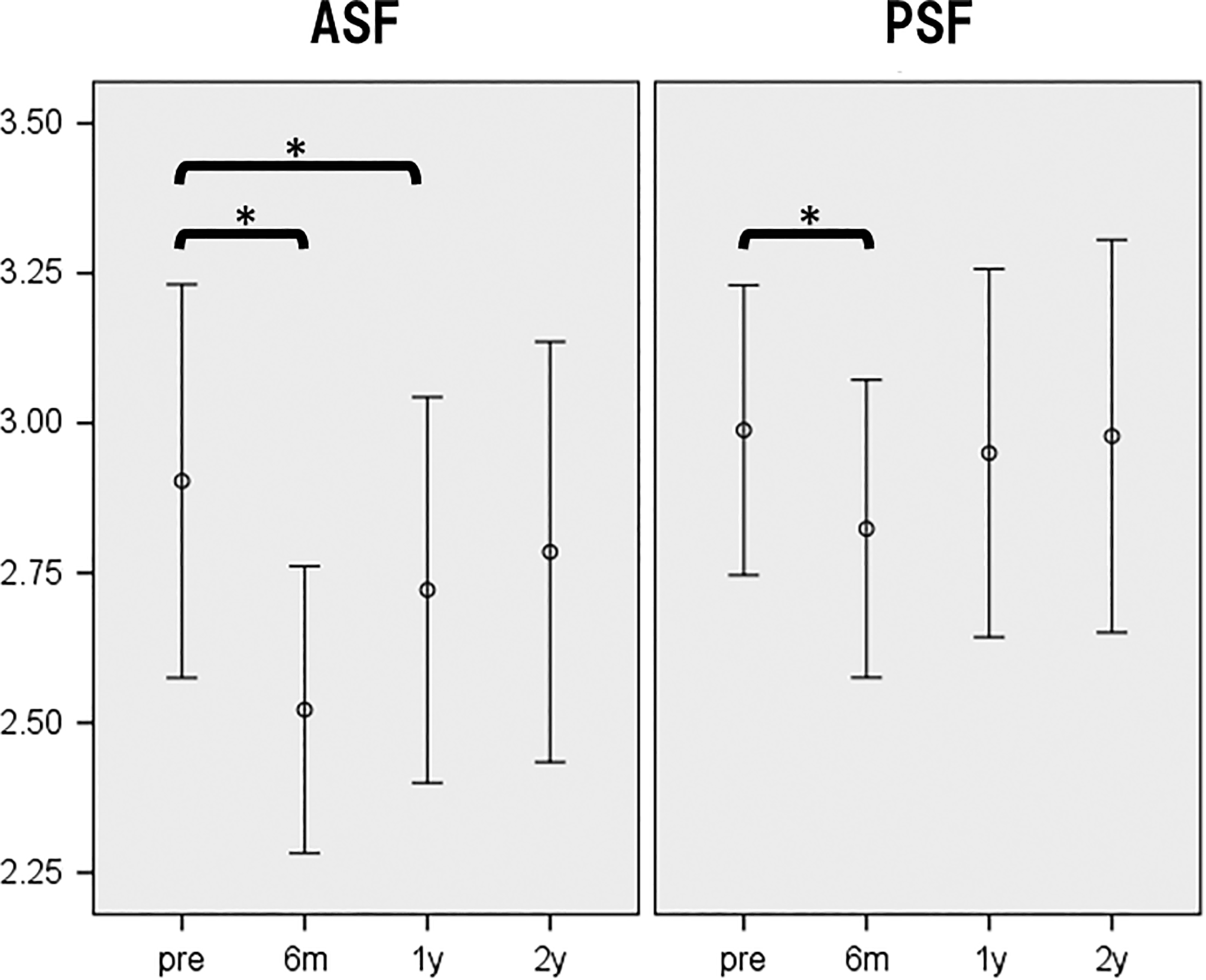
Pulmonary function in the early phase. ASF, anterior spinal fusion; PSF, posterior spinal fusion.
Discussion
The influence of surgical correction of thoracic spinal deformity on pulmonary function has been well investigated. Several authors have reported the superiority of a posterior only approach on PFT parameters. Chest cage disruption in anterior approach was shown to be an important cause of deterioration in pulmonary function at early postoperative follow-up. Even though, at long-term follow-up, postoperative PFT values returned to preoperative values, patients without chest cage disruption had greater improvement of pulmonary function. 7,10 Moreover, invasiveness of chest cage disruption also affected the long-term PFT. More patients undergone open anterior approaches and thoracoplasty experienced reduction in 2-year PFT values compared with posterior or thoracoscopic procedures. 10 Faro et al 20 compared PFT after open and thoracoscopic approaches in thoracic AIS patients. Violation of the chest wall in open thoracotomy through latissimus dorsi and intercostal muscle dissection for rib retraction on the convex side was the primary cause of decline in PFT values. In most cases, the anterior approach to the TL/lumbar spine requires thoracotomy with separation of the diaphragm. In this study, the effect of ASF versus PSF on PFT was compared.
Pulmonary function after TL/lumbar curve correction has not been well investigated because these deformities are not directly related to the chest cavity. Therefore, there have been only few reports addressing PFT after selective fusion of TL/lumbar curves. Kim et al 21 compared PFT after ASF using an open thoracotomy or thoracoabdominal approach for curve correction in AIS. They showed that an open thoracotomy approach resulted in significant decreases in postoperative absolute pulmonary function. Sudo et al 22 evaluated the long-term outcome of pulmonary function after anterior dual rod instrumentation in TL/lumbar AIS. They found no significant differences between preoperative pulmonary function and PFT at more than 12-year postoperative follow-up. Neither of the studies compared the pulmonary function between anterior and posterior approaches. In our current study, the absolute PFT values in ASF group were significantly lower than that of PSF group at 2-year follow-up. When comparing preoperative and 2-year changes on each procedure, only %FVC showed 1.8% significant difference, which seems to have no clinical relevance while in FVC, FEV1, and %FEV1 had no significant differences. On the other hand, the ASF group showed decreases in FVC at 6 months and 1 year compared with preoperative values. Meanwhile, FVC in PSF group returned at preoperative value at 1 year. These results indicate a possible adverse influence of performing a thoracotomy with separation of diaphragm on PFT in the early postoperative period. In long-term follow-up, FEV1 was reported to be slightly under the reference values in patients who underwent open anterior surgery in TL/lumbar AIS; however, percentage-predicted values were within normal limits and did not differ from preoperative value while FVCs were similar to the reference value, 23 so anterior approach is considered to have very mild negative effect on pulmonary function. At 2-year follow-up in this study, absolute FVC and FEV1 in the ASF group were less than that of PSF group significantly; however, when we take a look at the baseline preoperative values, FVC and FEV1 of ASF group was already less than PSF group. Moreover, %FVC and %FEV1 were considered within normal range (above 80%) so ASF did not cause clinical significant deterioration of pulmonary function compared with PSF in long-term follow-up in our study.
The limitations of this study are that the current study is a retrospective multicenter study that did not include matched case analysis and additional factors such as level of physical activity or periods of postoperative brace treatment, which might affect pulmonary function. However, this study included a homogenous population of patients with respect to diagnosis, curve pattern, and preoperative PFT values.
In conclusion, pulmonary function after ASF and PSF was similar at 2 years; however, anterior group did not return to the baseline in the early postoperative period (at 6 months and 1 year), suggesting a possible influence associated with anterior approach. It would be a reasonable information to counsel patients of the pulmonary function depending on the surgical procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Japan Spinal Deformity Institute.