
Abstract
Study Design
Meta-analysis and systematic review.
Objective
This study aims to investigate and compare patient-reported outcomes, perioperative data, and complications between 2 common endoscopic approaches for lumbar disc herniation: transforaminal and interlaminar endoscopic lumbar discectomy, by published high-quality evidence.
Methods
Electronic databases were searched for reported outcomes following TELD and IELD. Oswestry Disability Index (ODI), visual analog scale of back (VASB) and leg pain (VASL), and MacNab criteria were evaluated. Operative time, hospital stays, blood loss, radiation exposure, and complications were investigated. Odds ratio (OR) and mean differences (MD) with 95% confidence intervals (CI) were calculated using random and fixed-effect models.
Results
Total of 1948 patients from 18 studies were included, consisting of 1006 patients (51.6%) in TELD group and 942 (48.4%) patients in IELD group. TELD had better improvement of postoperative ODI (MD = 1.26; 95% CI: .07-2.16; P = .04), postoperative VASB (MD = −.23; 95% CI: −.40 to −.05; P = .01) and last follow-up VASB (MD = −.25; 95% CI: −.41 to −.09; P = .002), but with longer operative time (MD = 10.1 min; 95% CI: 1.925-18.77; P < .00001) and more fluoroscopic time (SMD = 4.12; 95% CI: 3.22-5.03; P < .00001), especially in L5-S1 operation. Bed rest time was significantly longer following IELD, with no difference in VASL, hospital stays, or complication.
Conclusion
We found comparable clinical outcomes in terms of ODI, VAS, patient satisfaction, hospital stays, and complication between both techniques. TELD required more radiation exposure and longer operative time at L5-S1 level than IELD. Our study provided results to help consider appropriate approaches for selected patients and informed consent of benefits from each approach.
Introduction
Lumbar disc herniation (LDH) is one of the most common spinal disorders predominantly affecting lower lumbar nerve roots. Symptoms occurred when the herniated intervertebral disc causes mechanical compression and inflammation of the adjacent nerve root, leading to radicular pain, numbness, or weakness of the lower limb.
1
Despite various non-surgical interventions available, many patients with LDH failed conservative treatment and ultimately required surgery to remove the herniated disc material and decompress the affected nerve root.
2
Microdiscectomy is the standard surgical procedure for treating LDH.
1
Due to an attempt to reduce surgical invasiveness, a spinal endoscope has been developed and applied to perform discectomy with many published evidence of its effectiveness and safety.3,4 As a minimally invasive surgery procedure, endoscopic lumbar discectomy requires a small incision with significantly reduced damage to the spinal musculature while providing excellent visualization of the spinal anatomy through different approaches.5,6 The endoscopic lumbar discectomy can be divided into 2 main approaches, the transforaminal lumbar endoscopic discectomy (TELD) described by Kambin
7
and interlaminar lumbar endoscopic discectomy (IELD) described by Choi and Ruetten.8-10 Both techniques have been proved to successfully provide good surgical outcomes with low complications in treating LDH. However, consensus on the standard for decision making to use which approach has not been reached, and results of comparative studies between these techniques have been inconsistent. To the best of our knowledge, a systematic review and meta-analysis regarding approaches of endoscopic lumbar discectomy had rarely been investigated. Therefore, the goals of this study were to collect and comprehensively analyze the reliable evidence on comparison of outcomes following TELD and IELD for treating LDH including functional outcomes, perioperative data, and complications (Figure 1). PRISMA (Preferred Reporting Items for Systematic Review and Meta-analysis) flow diagram.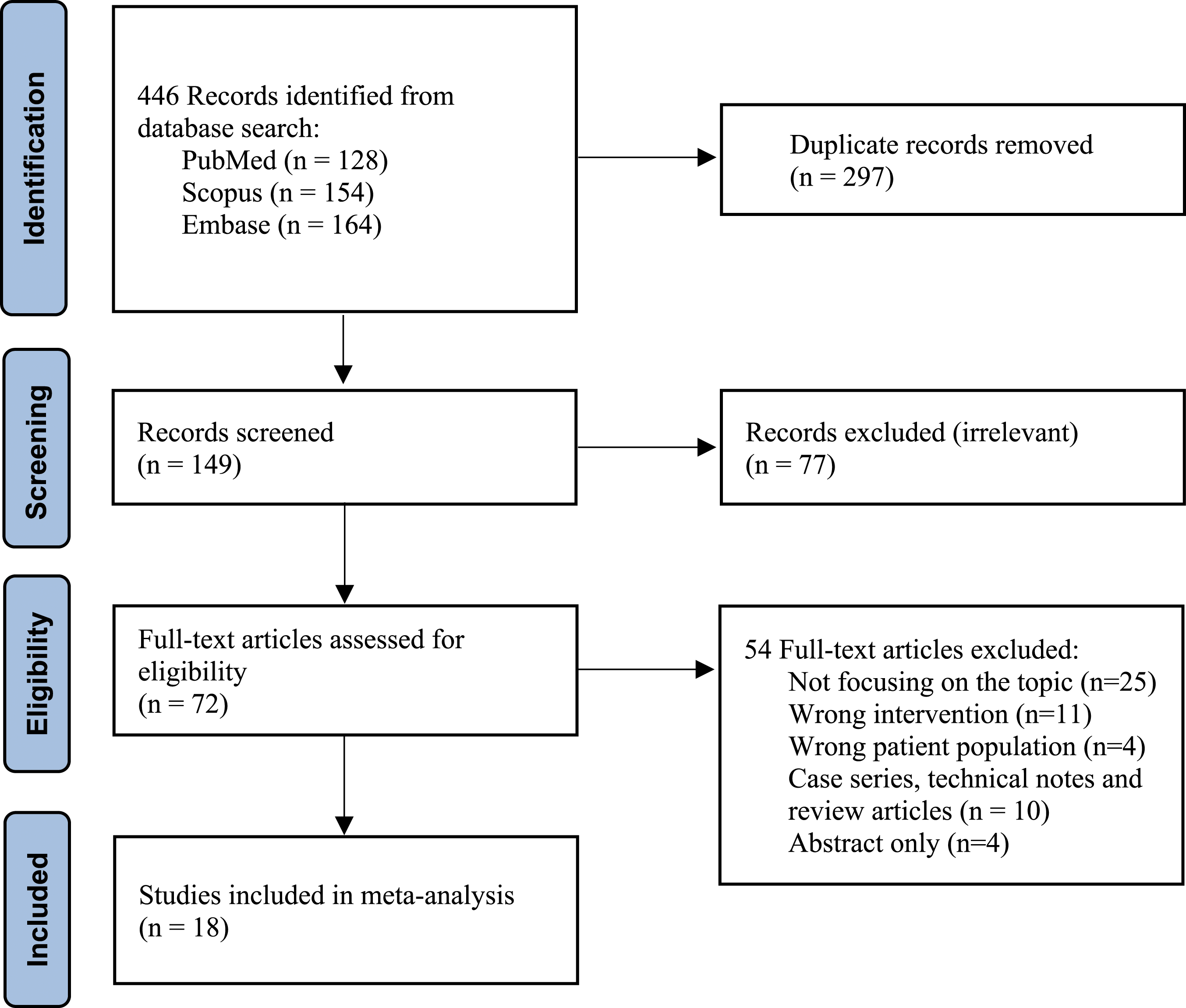
Material and Methods
Literature Searches
We conducted a systematic review and meta-analysis in line with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines. Since the endoscopic lumbar discectomy was first reported in 1973, all articles published from January 1973 until 31 March 2022, were electronically retrieved. MEDLINE, Embase, and Scopus were searched for peer-reviewed published articles including retrospective and prospective studies of outcomes following endoscopic discectomy for LDH that compare transforaminal and interlaminar approaches. We used the following search terms: endoscopic, discectomy, disc herniation, PELD, transforaminal, TELD, interlaminar, and IELD. All reference lists in the retrieved studies were manually checked for relevance and suitability.
Inclusion and Exclusion Criteria
The inclusion criteria for our meta-analysis were: (1) published retrospective or prospective studies, (2) including more than 10 patients in each group with at least 3 months of follow-up period, (3) focusing on comparing TELD and IELD for treatment of LDH, (4) providing sufficient data including operative data, postoperative clinical or functional outcomes or complications and (5) articles written in the English language. Studies were excluded if they met any of the following criteria: (1) case series, case reports, or technical notes, (2) review articles, (3) duplicated reports, or (4) incomplete statistical data. The titles and abstracts of all reports were manually screened then full-text studies were assessed for eligibility according to the inclusion and exclusion criteria. The included reports were thoroughly reviewed and relevant data were recorded. The screening process of all eligible studies was organized by Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, VIC, Australia).
Outcomes
Baseline characteristics of patients in each record were obtained, including author name, country, study type, number of subjects, age, sex, disc location, and follow-up time. The primary outcome was patient-reported outcome measure in a form of Oswestry Disability Index (ODI), visual analog scale of back (VASB) and leg pain (VASL) improvement, and MacNab evaluation (excellent/good/fair/poor). Secondary outcomes included perioperative data and complications. Perioperative data concerning operative time, fluoroscopic time, estimated blood loss, length of hospital stays, and postoperative bed rest time were recorded. Complications were obtained with subgroup analysis on dural tear and recurrent disc herniation.
Data Extraction and Quality Assessment
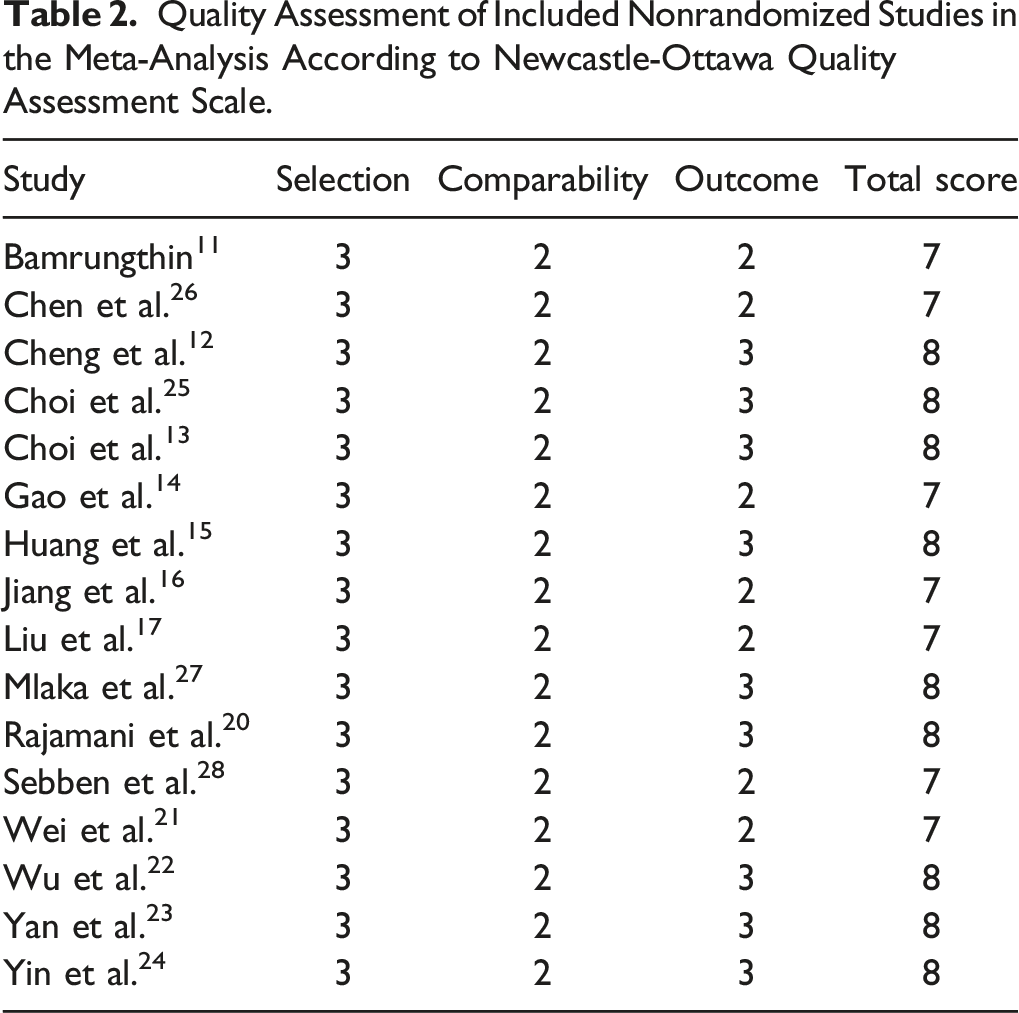
Data were extracted and assessed the quality by 2 authors (KJ and YL) independently using the Review Manager 5.4 (Cochrane Collaboration). Any disagreement between the 2 authors was solved by a discussion with the third author to reach a consensus. The quality of the eligible studies and risk of bias were evaluated using the Newcastle-Ottawa scale (NOS), which consists of 3 major categories: selection, comparability, and exposure, with a maximum of 9 stars to be assigned to each included study.
Statistical Analysis
Data analyses were processed with Review Manager 5.4 (Cochrane Collaboration). Odds ratio (OR) were used for comparison of dichotomous variables, including MacNab evaluation and complications. Mean difference (MD) and standard mean difference (SMD) with 95% confidence interval (CI) were used for continuous data, including age, operative time, fluoroscopy time, hospital stay, bed rest time, ODI, and VAS score. The heterogeneity among included studies was assessed by the degree of inconsistency (I2 statistic). The fixed-effect model was used for data without significant heterogeneity (P > .05, I2 < 50%), and the random-effect model was applied if the data had significant heterogeneity. The risk of bias assessment among the studies was investigated with the funnel plot. A P-value < .05 was defined as statistically significant.
Results
Study Characteristics and Quality Assessment
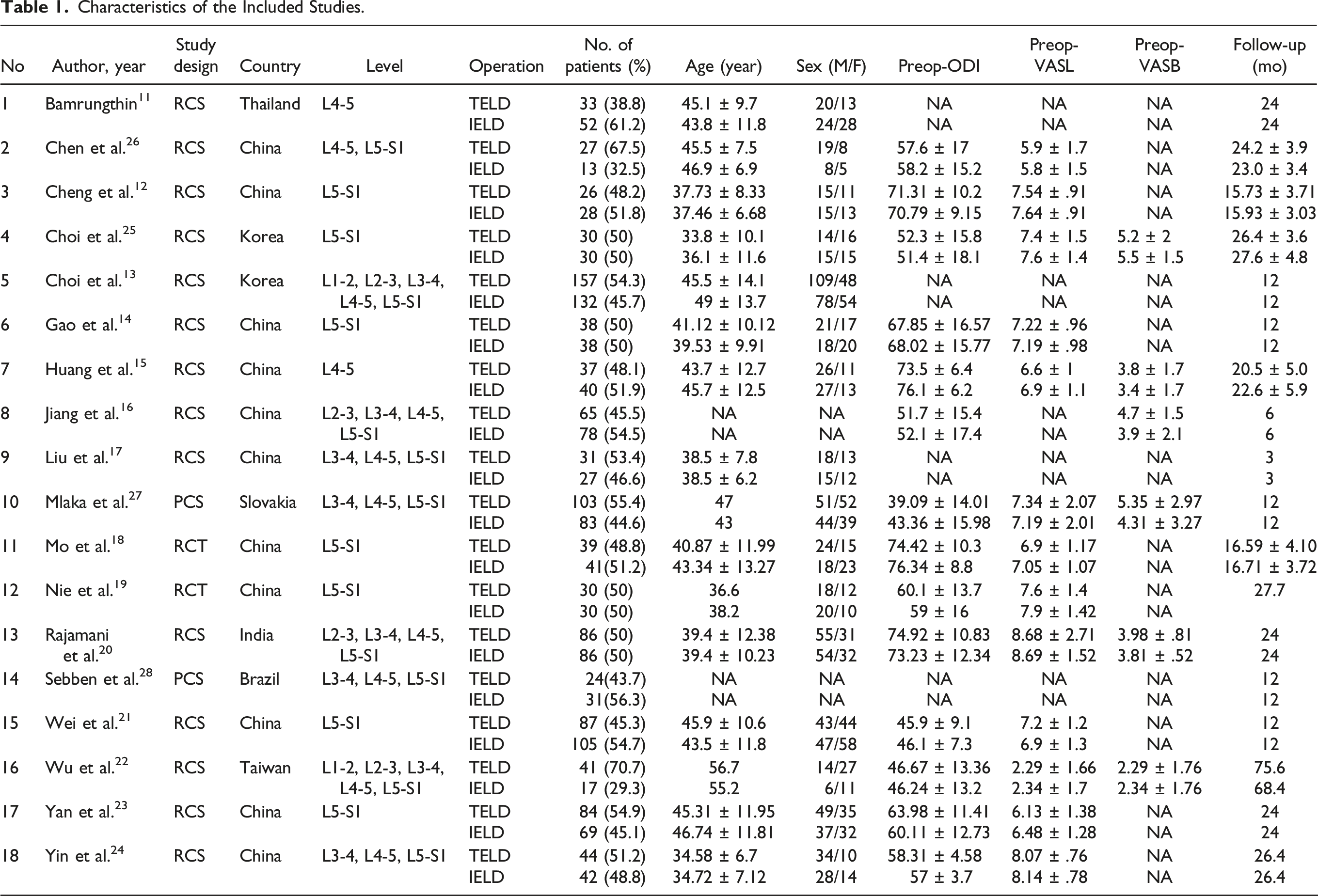
Characteristics of the Included Studies.
Quality Assessment of Included Nonrandomized Studies in the Meta-Analysis According to Newcastle-Ottawa Quality Assessment Scale.
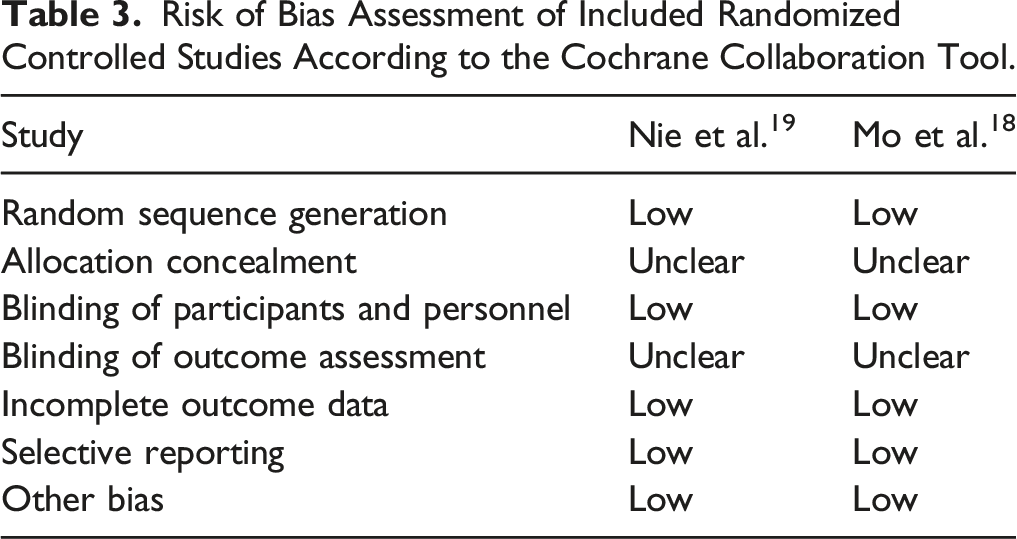
Risk of Bias Assessment of Included Randomized Controlled Studies According to the Cochrane Collaboration Tool.
Demographics
Demographic characteristics of the TELD and IELD groups were summarized in Table 1. For comparisons of sex, age, and follow-up time, no obvious heterogeneity was observed. Demographic data were not significantly different between TELD and IELD group, regarding sex (male vs female; OR = 1.18; 95% CI: .95-1.45; P = .14), age (MD = −.41 years; 95% CI: −1.49-.68; P = .46), and follow-up time (MD = −.41 months; 95% CI: −1.32-.50; P = .37).
Similarly, no significant heterogeneity of preoperative functional scores (ODI, VASB, and VASL) was detected among the included studies and the fixed-effect model was used. Among the included studies, there was no significant difference of preoperative ODI (MD = .16; 95% CI = −.82-1.14; P = .75) and VASL (MD = −.06; 95% CI = −.20-.08; P = .32), however, preoperative VASB was significantly higher in TELD group (MD = .25; 95% CI: .07-.42; P = .006).
Perioperative Data
Operative Time
There were 14 studies that reported operative time, including 1586 patients with 801 and 785 patients in TELD and IELD groups, respectively.11-24 The random effect model was used for comparison since the heterogeneity was high (P < .00001, I2 = 98%). As depicted in Figure 2A, comparative results revealed significant differences in surgical duration between the 2 approaches. TELD tended to have significantly longer operative time than IELD group. (MD = 10.1 min; 95% CI: 1.925-18.77; P < .00001). However, subgroup analysis indicated that LDH at the L5-S1 level had a significant effect on operative time. We found that TELD for L5-S1 LDH significantly required longer operative time (MD = 18.43 mins; 95% CI: 6.63-30.2; P = .002), while operation at other levels did not demonstrate a significant difference in surgical duration. Forest plot showing effect sizes and 95% CI in the perioperative data, comparing operative time (A), estimated blood loss (B), hospital stay (C), bed rest period (D) and fluoroscopy time (E) between TELD and IELD. TELD, transforaminal endoscopic lumbar discectomy; IELD, interlaminar endoscopic lumbar discectomy; SD, standard deviation; CI, confidence interval; df, degrees of freedom.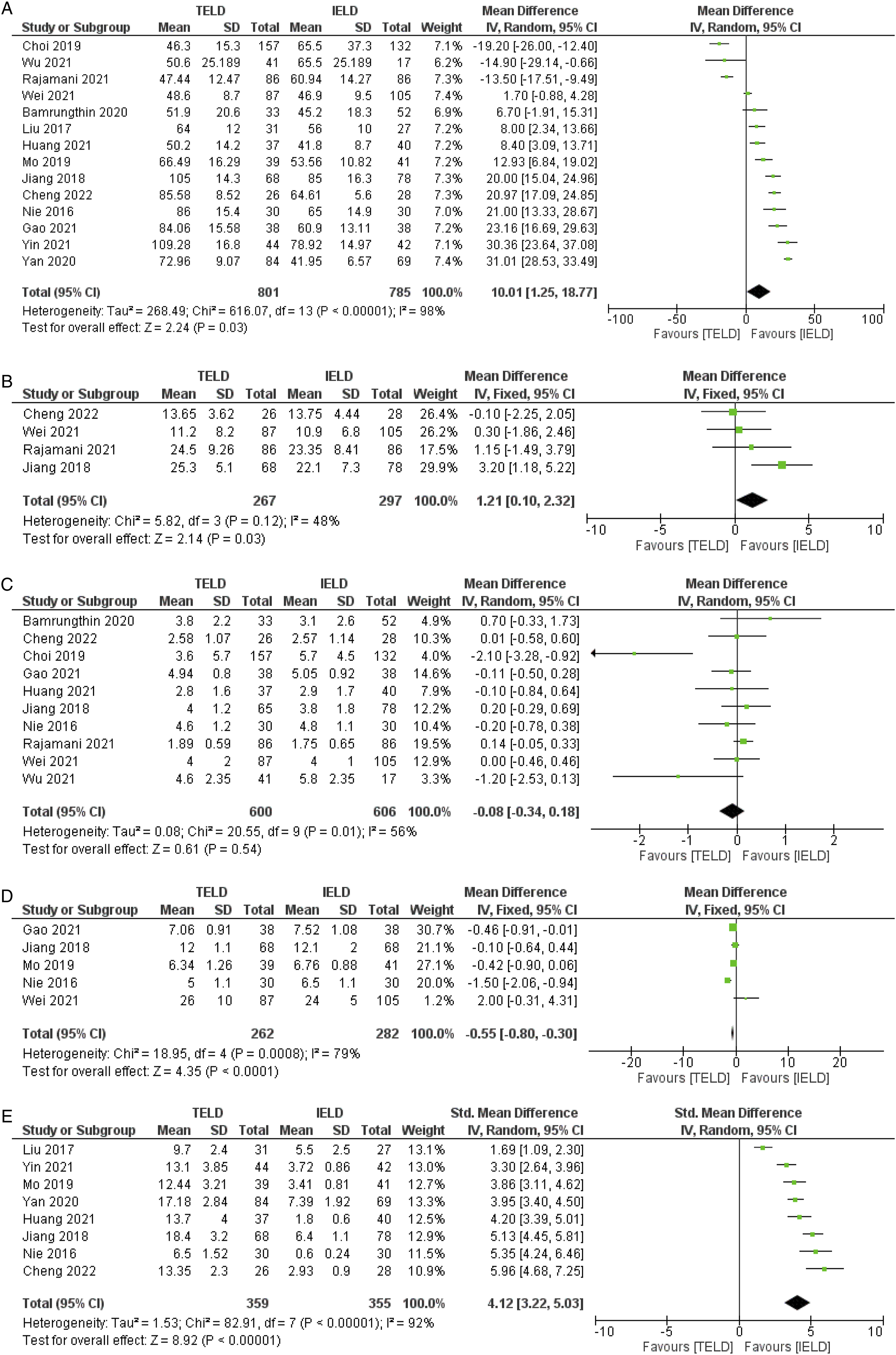
Estimated Blood Loss
As shown in Figure 2B, the estimated blood loss during the surgery was reported in only 4 studies including 564 patients.12,16,20,21 The test for heterogeneity revealed no significant heterogeneity existed (P = .12, I2 = 48%) and the fixed-effect model was used. TELD group demonstrated statistically significantly higher blood loss than participants in the IELD (MD = 1.21 ml; 95% CI: .1-2.32; P = .03).
Hospital Stay and Bed Rest Time
Length of hospital stay was recorded in 10 studies, including 600 and 606 patients in TELD and IELD groups respectively.11-16,19-22 The test revealed that moderate heterogeneity existed (I2 = 56%; P = .01). The source of high heterogeneity was influenced by the study of Choi et al. 13 However, data analysis revealed no significant difference in hospital stay between both groups (MD = .08 days, 95% CI: −.34-.18; P = .61) (Figure 2C).
The postoperative bed rest period was available in 5 studies, consisting of 262 and 282 patients in TELD and PELD groups, respectively.14,16,18,19,21 Significant heterogeneity was detected among these studies (I2 = 79%; P = .008). The source of high heterogeneity was influenced by the study of Nie et al. 19 As demonstrated in Figure 2D, the comparative analysis indicated that TELD had a slightly shorter length of postoperative bed rest time than IELD with a statistically significant difference (MD = .55 h, 95% CI: −.83-.33; P < .0001).
Radiation Exposure From Fluoroscopy
A total of 8 studies documented the radiation exposure via fluoroscopy time, including 359 patients in TELD group and 355 patients in IELD group.12,15-19,23,24 The analysis indicated the heterogeneity was high (P < .00001, I2 = 92%) and the random effect model was used. The study by Liu et al. 17 that focused on surgery of highly migrated disc herniation revealed higher fluoroscopic time in IELD than other studies and this study was the resource of heterogeneity. Different parameters of fluoroscopic use measurement were recorded among these studies so the standard mean difference (SMD) was used. Based on the comparison, the fluoroscopic time was significantly longer in the TELD than IELD group as illustrated in Figure 2E (SMD = 4.12; 95% CI: 3.22-5.03; P < .00001). Subgroup analysis focusing on operation for L5-S1 and other levels also demonstrated similar results.
Patient-Reported Outcomes
The patient-reported outcomes improvement (ODI, VASL, VASB) was calculated from the difference of the functional scores recorded before and after the surgery. The improvement of outcomes was presented in 2 periods: at the early postoperative period and the last follow-up. The early postoperative improvement represented the short-term functional outcome following the surgery, while the last follow-up ODI represented the long-term functional outcome.
ODI
The early postoperative ODI improvement was available in 7 studies.12,14,18,20,22,24,25 The fixed-effect model was used since the heterogeneity was low (P = .40, I2 = 3%). As depicted in Figure 3A, the postoperative ODI improvement was significantly better following the TELD than the IELD group (MD = −1.26; 95% CI: .07-2.16; P = .04). However, the minimally clinically important difference (MCID) was not reached. Forest plot showing effect sizes and 95% CI in the patient-reported outcomes, comparing the postoperative ODI (A), last follow-up ODI (B), postoperative VASL (C), last follow-up VASL (D), postoperative VASB (E), last follow-up VASB (F) and the MacNab excellent/good rate evaluation (G) between TELD and IELD. TELD, transforaminal endoscopic lumbar discectomy; IELD, interlaminar endoscopic lumbar discectomy; ODI, Oswestry Disability Index; VASL, visual analog scale of leg pain; VASB, visual analog scale of back pain; SD, standard deviation; CI, confidence interval; df, degrees of freedom.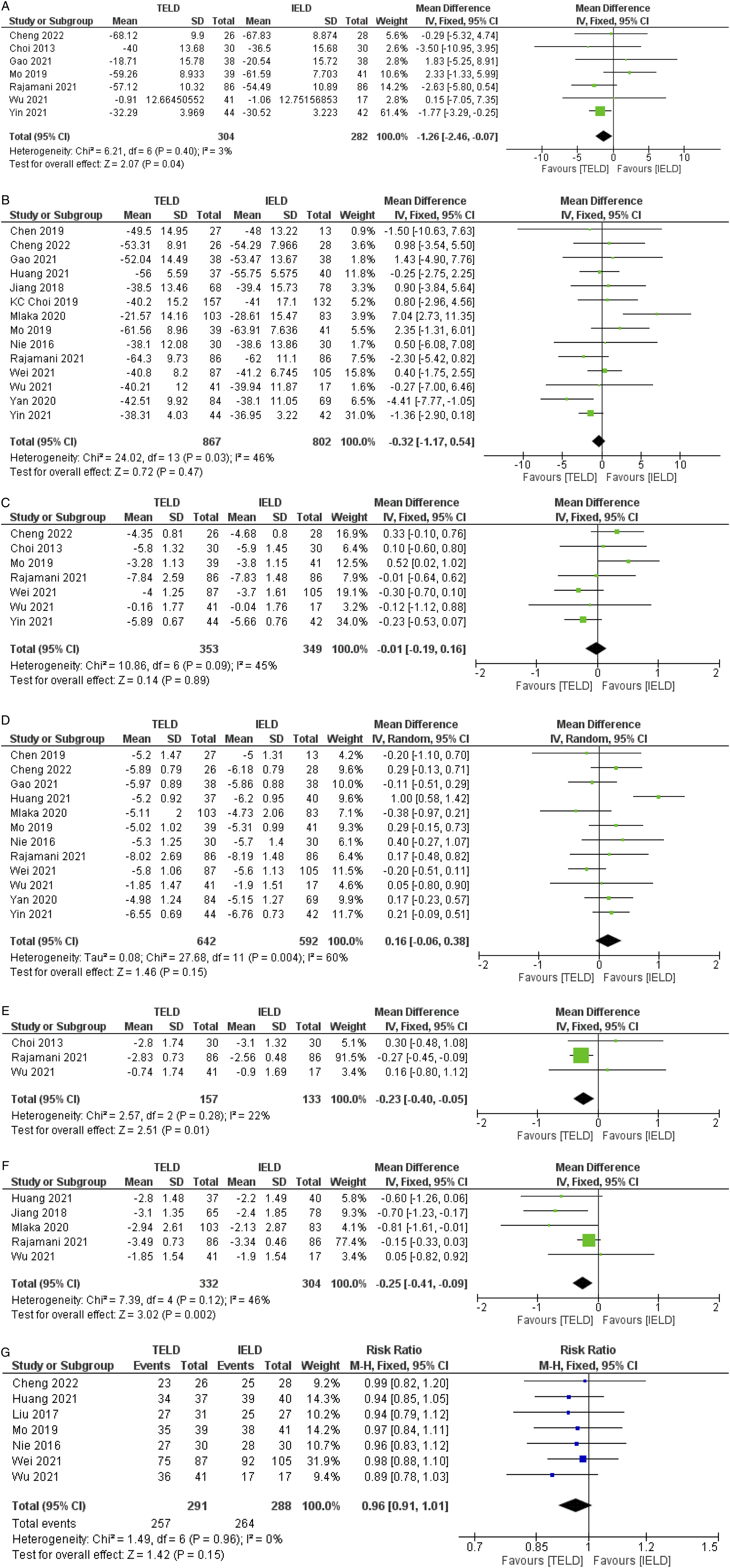
The ODI improvement at the final follow up period was available in 14 studies.12-16,18-24,26,27 Moderate heterogeneity was detected (P = .03, I2 = 46%) and the fixed-effect model was used. As illustrated in Figure 3B, the last follow-up ODI was not significantly different between both approaches (MD = −.32; 95% CI: −1.17-.54; P = .47). Subgroup analysis for TELD and IELD at L5-S1 level revealed similar results to operation at other levels.
VAS of Leg Pain and VAS of Back Pain
The early postoperative VASL improvement was recorded in 7 studies.12,18,20-22,24,25 The fixed-effect model was used since the heterogeneity was not significant (P = .09, I2 = 45%). As depicted in Figure 3C, the postoperative VASL improvement was not significantly different between 2 approaches (MD = −.01; 95% CI: −.19-.16; P = .89).
At the last follow-up, the VASL improvement was available in 12 studies.12,14,15,18-24,26,27 Moderate heterogeneity was detected (P = .004, I2 = 60%) and the random-effect model was used. The source of heterogeneity was from Huang et al. 15 As illustrated in Figure 3D, the last follow-up VASL was not significantly different between both approaches (MD = .16; 95% CI: −.06-.38; P = .15) (Fig. 3D).
For VASB, the comparison in the early postoperative period was recorded in only 3 studies.20,22,25 The results showed low heterogeneity among the included studies (P = .28, I2 = 22%), thus the fixed-effect model was used. The early postoperative VASB reduction was significantly better in TELD than IELD group (MD = −.23; 95% CI: −.40 to −.05; P = .01), as shown in Figure 3E. However, the MCID for VASB reduction between both techniques was not reached.
VASB at the final follow-up was available in 5 studies.15,16,20,22,27 No obvious heterogeneity was detected (P = .12, I2 = 46%) and the fixed-effect model was used. Likewise, VASB reduction at the final follow-up was significantly better following TELD than IELD group (MD = −.25; 95% CI: −.41 to −.09; P = .002), as shown in Figure 3F. Similarly, the MCID of VASB reduction was not reached.
Patient Satisfaction
Patient satisfaction was classified by the MacNab evaluation which was recorded in 7 studies, including 291 and 288 patients in TELD and IELD group, respectively.12,15,17-19,21,22 The rate of patient satisfaction postoperatively was relatively high for both groups. The MacNab criteria were assigned to be “excellent” or “good” for over 80% of the participants following TELD and IELD in all included studies. However, there were no statistically significant differences between the 2 approaches (RR = .93; 95% CI: .91-1.01; P = .15), and the fixed-effect model was used as there was no heterogeneity (P = .96, I2 = 0%) as demonstrated in Figure 3G.
Complications
There were 9 studies which recorded the complications, as illustrated in Figure 4A.12,17-21,23,27,28 The overall complication rates were relatively low with approximately 11.8% in TELD and 11.2% in IELD group, except for the study by Mlaka et al.
27
which reported higher complication rates in both groups, 15.5% and 18.1% in TELD and IELD group, respectively. The fixed-effect model was performed for the analysis due to the low heterogeneity (P = .87, I2 = 0%). The overall complication rates were not significantly different between the TELD and IELD groups (OR = 1.03; 95% CI: .70-1.52; P = .88). Forest plot showing effect sizes and 95% CI in the complications, comparing overall complications (A), rate of recurrent disc herniation (B) and dural tear (C) between TELD and IELD. TELD, transforaminal endoscopic lumbar discectomy; IELD, interlaminar endoscopic lumbar discectomy; SD, standard deviation; CI, confidence interval; df, degrees of freedom.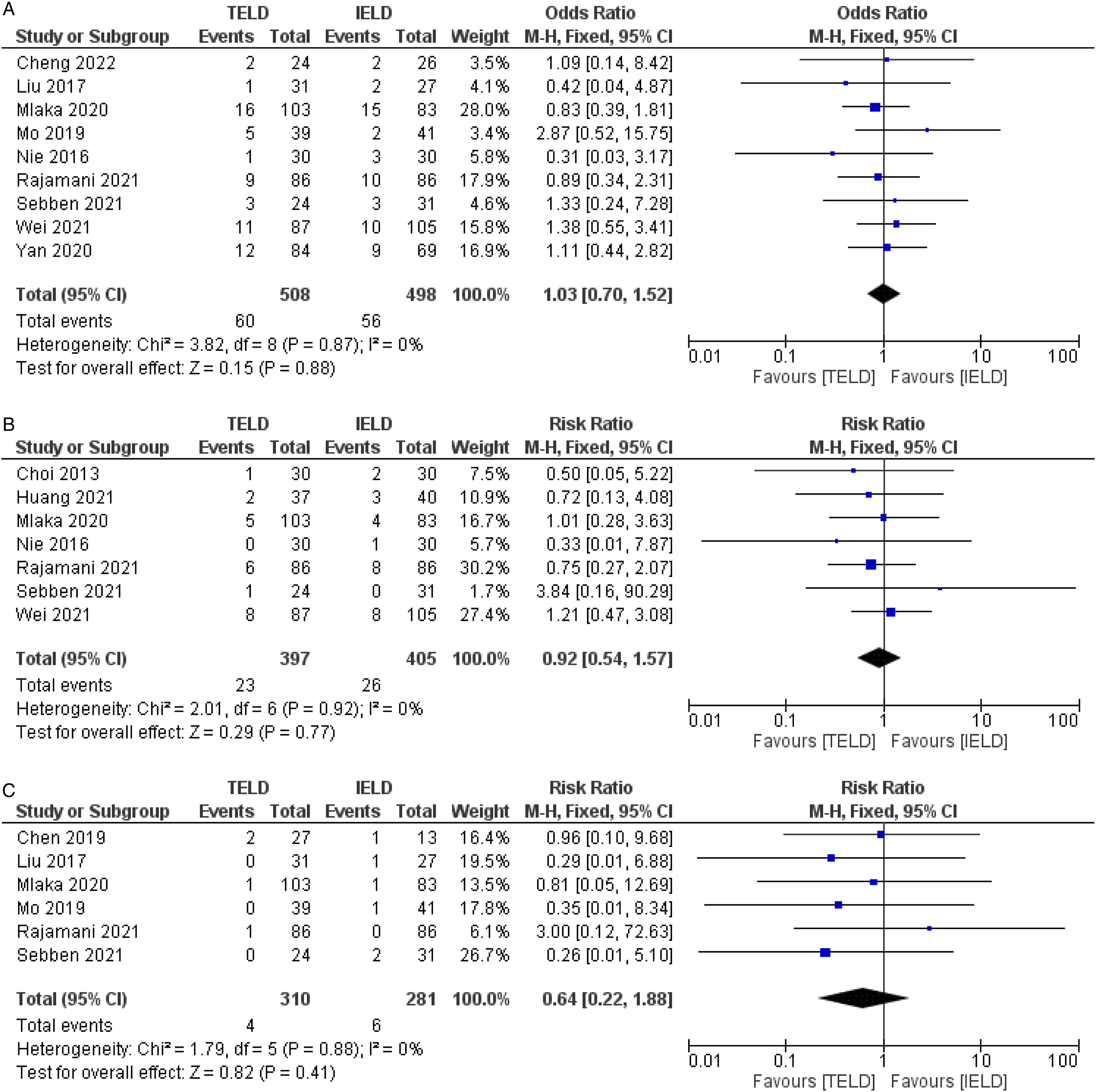
Rates of recurrent disc herniation were recorded in 7 studies with average rates of 5.8% and 6.4% following TELD and IELD, respectively.15,19-21,25,27,28 The heterogeneity was low (P = .92, I2 = 0) and the fixed-effect model was used. There was no significant difference of rates of recurrence following the surgery between the TELD and IELD groups (RR = .92; 95% CI: .92-1.57; P = .77), as illustrated in Figure 4B.
Rates of dural tear were available in 6 studies.17,18,20,26-28 The average rates dural tear were 1.3% and 2.1% following TELD and IELD, respectively. The heterogeneity was low (P = .88, I2 = 0) and the fixed-effect model was used. Also, there were no significant differences in rates of dural tear between both techniques (RR = .64; 95% CI: .22-1.88; P = .41), as illustrated in Figure 4C.
Publication Bias
Risk of bias assessment was performed through the funnel plot and Egger’s test, indicating that low risks of bias were detected among the included studies. All the funnel plots were symmetric and the Egger’s test for publication bias was not statistically significant results for all outcome variables, including operative time (P = .505), fluoroscopy time (P = .379), estimated blood loss (P = .708), length of hospital stay (P = .089), postoperative bed rest time (P = .497), ODI (P = .251), VASL (P = .986), VASB (P = .214), MacNab evaluation (P = .979), and overall complications (P = .794).
Discussion
In this study, we performed a meta-analysis of 18 high-quality evidences, including 1924 patients to compare 2 popular approaches for endoscopic lumbar discectomy: transforaminal and interlaminar approaches, in terms of perioperative data, clinical outcomes, and complications.
For the comparison of the perioperative data, IELD had shorter operative time, less estimated blood loss, and shorter fluoroscopic time. These findings were similar to the meta-analysis by He et al. 29 and the prospective study by Ahn et al. 30 that reported surgeon’s radiation exposure during TELD. They found that, within the maximum allowable dose of radiation hazard, surgeons could safely perform only 291 cases of TELD without radiation shielding. Since TELD required a more complicated puncture technique and fluoroscopic guidance for an accurate surgical trajectory with a more rigid working window, especially at L5-S1 which the high iliac crest and the narrow space to access L5-S1 foramen led to difficulty in determining the correct puncture direction and also more challenges when treating migrated LDH. In contrast to IELD at the L5-S1 level, the interlaminar space is relatively wide and most surgeons were more familiar with the anatomy when operating through posterior lumbar approach so the interlaminar approach for L5-S1 LDH was less complicated and usually required less operative time and less complicated fluoroscopic guidance.15,26,31 However, Wu et al. 22 reported that IELD had a longer operative time than TELD when approaching for high-grade migrated LDH due to more bone resection and soft tissue work. Our study also found that TELD had a slightly shorter duration of postoperative bed rest period, according to the analysis. This finding was potentially caused by different types of anesthesia. Usually, TELD was performed under local anesthesia, while IELD was operated under general anesthesia which possibly led to a slight delay in postoperative ambulation due to the effects of anesthetic agent. Nevertheless, from the current study, this delay in ambulation was very subtle and unlikely to affect patient’s condition and satisfaction postoperatively. In addition, the length of hospital stay was not different between both approaches. For the comparison of estimated blood loss, despite of significant difference in amount of blood loss between both techniques from our analysis, no studies had mentioned the methods of measuring blood loss under endoscope. Thus, we believed that this difference would not have any clinical significance.
The improvement of functional outcomes was analyzed as the primary outcome of this meta-analysis. Postoperative results were favorable following both techniques with significant improvement of functional scores, demonstrating that both approaches were effective in alleviating patients’ symptoms and recovering their function. To the best of our knowledge, our study is the first meta-analysis to detect the improvement of clinical outcomes, by analyzing the difference between pre- and postoperative function scores. ODI improvement in the early postoperative period was slightly better following TELD than IELD but did not achieve MCID, and no difference was detected at the last follow-up. Interestingly, the VASB reduction was more effective with IELD at both early postoperative period and the last follow-up with statistical significance. Nevertheless, the mean difference in back pain reduction was very subtle (less than one point) and failed to achieve the MCID. These findings were in accordance with previous meta-analyses that identified similar effects in pain reduction and function recovery between 2 approaches.29,32 In addition, our study found that the VASL reduction was also not different between both groups, but with significant heterogeneity. The source of heterogeneity was from Huang et al. 15 who reported clinical outcomes following endoscopic discectomy focusing only highly down-migrated LDH. Complete removal of highly down-migrated disc material was likely more difficult to achieve via TELD approach, possibly leading to a residual remnant of disc fragment following the surgery and unrelieved leg pain. 15 Patient satisfaction assessed by MacNab criteria was also not different between both approaches. Moreover, subgroup analysis for TELD and IELD at L5-S1 level revealed similar results to operation at other levels. Our demonstrated findings were correlated with previous studies, indicating that both techniques could successfully remove the herniated disc material, and adequately decompress the nerve root, while preserving spinal stability in comparable effectiveness. However, performing TELD in L5-S1 level or highly migrated disc herniation was feasible but could be a challenge, requiring surgeon’s experience, longer operative time and more fluoroscopic use.
For evaluation of procedure safety, we performed a comparative analysis of the complications. Our study found no evident differences in overall complications between TELD and IELD. Regardless of the surgical approaches, the overall complication rate was approximately 11% which was correlated with previous meta-analysis by Yin et al. 33 regarding complications following TELD and IELD. Moreover, rates of recurrent disc herniation and dural tear did not significantly differ between both groups. The rates of dural tear following both techniques were relatively low (less than 3%), in accordance with a survey study by Lewandrowski et al., 34 but they reported a higher risk of dural tear in IELD than TELD due to the use of power tools or sharp instruments during ligamentum flavum resection and the fragile posterior dural sac exposure. However, we believe that surgeons’ learning curve significantly affected the complication rates.
According to the surgical anatomy combined with our comparative results between the 2 approaches, our recommendations on approach selection for endoscopic discectomy were as follows: Basically, the zone of disc herniation should be the first factor to consider. Foraminal or extraforaminal disc herniation should be treated with transforaminal approach. Herniated disc at L5-S1 level is more easily accessed with interlaminar approach due to the hindrance of iliac crest height. Usually, high-grade migrated disc removal is more comfortably performed with interlaminar approach due to more flexible working window than the transforaminal trajectory. However, due to the possibility to operate under local anesthesia, TELD has advantages in patients with multiple comorbidities with high risk of general anesthesia. Apart from these considerations, the results following TELD and IELD were comparable and decision-making on approach selections should depend on the surgeon’s preference, experiences, and individual, case-by-case consideration.
The strengths of this meta-analysis were as follows: First, as mentioned earlier, this study is the first meta-analysis that focuses on the comparison of the degree of improvement of clinical outcomes which was more valuable, in contrast to previous meta-analyses that mostly compared the functional scores directly. Moreover, the functional outcome improvement was analyzed in both early postoperative and last follow-up periods. Second, we conducted a subgroup analysis for the highly heterogeneous outcome, such as functional outcomes in L5-S1 LDH surgery. Third, the current study included updated high-quality evidence with a large number of total participants from different countries, as most of the previous literature included articles in Chinese which may affect generalizability.
There were some limitations to our study. First, most of the included studies were retrospective and nonrandomized prospective studies that were subjected to selection bias and incomplete data. Second, some of the outcome variables had significant heterogeneity that may affect the reliability of the comparative analysis. Third, several confounding factors may contribute to postoperative outcomes following TELD and IELD such as different surgeon’s skills, learning curve, and modifications of endoscopic techniques from each center or subjects from different countries may affect the outcome measures.
Despite these limitations, our meta-analysis reported comparative results of TELD and IELD, focusing on functional outcomes improvement and could guide spine surgeons to consider evidence from this study to select the appropriate approach of endoscopic lumbar discectomy for their patients and also informed consent for risk and benefits of each procedure.
Conclusion
This meta-analysis was the first to compare TELD and IELD for treating LDH focusing on the improvement of clinical outcomes. We found comparable functional outcomes in terms of ODI and VAS improvement, patient satisfaction, hospital stays, and similar complication rates between both techniques. IELD required a slightly longer period of postoperative bed rest. TELD required more radiation exposure than IELD and also had a longer operative time at L5-S1 level. Our study could be helpful for surgeons to consider which approach is suitable for selected patients and also informed consent of the advantages of each approach before performing endoscopic lumbar discectomy.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.-S.K. is a consultant of Richard Wolf, GmbH, and Elliquence, LLC.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be available by contacting J.-S.K. the corresponding author, at the above address.