
Abstract
Study Design
Retrospective study.
Objective
To analyze the causes of and factors influencing early recurrence after TELD performed in the treatment of lumbar disc herniation.
Methods
We included 285 patients with single-segment lumbar disc herniation treated using transforaminal endoscopy lumbar discectomy TELD from January 2017 to December 2019 at the First Affiliated Hospital of the University of South China. Patients were classified into early recurrence and non-early recurrence groups based on clinical symptoms and MRI reexamination. Imaging data (eg, disc height index (DHI), Pfirrman grades, base width, postoperative annulus-fibrosus tear size, cross-sectional area of the foramen (CSAF), etc.)were analyzed, and multivariate, binomial logistic regression was utilized to determine which factors were associated with early recurrence after TELD.
Results
A total of 285 patients completed surgery and clinical follow-up, during which 19 patients relapsed within 6 months postsurgery, for an early recurrence rate of 6.7%. There were statistically significant differences between DHI, Pfirrman grades, base width, postoperative annulus-fibrosus tear size, herniation sites, CSAF and Modic changes between the early recurrence and non-early recurrence groups (P < .05). On multivariate logistic regression,the degree of disc degeneration (OR = .747, P = .037), CSAF (OR = 5.255, P = .006), degree of Modic change (OR = 1.831, P = .018) and base width of the herniation (OR = 4.942, P = .003) were significantly correlated with early recurrence after TELD.
Conclusions
Postoperative annulus-fibrosus tear size, DHI, and location of the disc herniation were associated with early recurrence after TELD. Increased base width of the herniation, severe disc degeneration, decreased CSAF and Modic change were risk factors for early recurrence after TELD.
Keywords
Introduction
Lumbar disc herniation (LDH) is the most common cause of lumbago, leg pain and radiculopathy. Approximately 70-85% of people develop lumbago or leg pain at least once in their lifetimes. 1 Surgery is required when standardized conservative treatment is unable to relieve the symptoms. Compared with conventional open surgery, transforaminal endoscopy lumbar discectomy (TELD) has advantages such as decreased probability of paravertebral muscle injury or destruction of bone structure, shortened duration of surgery, and decreased intraoperative bleeding and length of hospitalization.2–4 Moreover, TELD has been shown to be efficacious in the treatment of LDH5,6, rendering this approach the most common surgical procedure presently used for this condition. Despite these advantages, the postoperative recurrence rate for recurrent lumbar disc herniation (rLDH) after TELD is higher than after conventional discectomy and endoscopic nucleus-pulposus resection.7,8 Additionally, rLDH after TELD occurs earlier than after discectomy and endoscopic nucleus-pulposus resection. 9 Suk defined rLDH as disc herniation at the same level in a patient after a pain-free period of at least 6 months from the initial surgery; this criterion is widely used to diagnose rLDH. 10 In recent years, reherniation occurring within 6 months after postoperative remission has been classified as early recurrence, while late recurrence is defined as reherniation occurring more than 6 months after postoperative remission. Late recurrence is determined by the individual constitution and genetics of the patient, while early recurrence often results from technical failure.11–13 At present, few studies have examined the factors influencing postoperative early recurrence14,15. In this study, we compared patient radiologic data to retrospectively analyze the incidence of early LDH recurrence after TELD and factors influencing this early recurrence.
Patients and Methods
General information
All study participants provided signed informed consent. For this study, we selected patients with LDH who underwent TELD, after failing 3 months of strict conservative therapy and pediatric patients were not included, at the First Affiliated Hospital of the University of South China, Department of Spine Surgery, from January 2017 to December 2019. The diagnosis of LDH was confirmed using clinical nerve compression symptoms and MRI scan showing herniation. The inclusion criteria were as follows: 1) definitive diagnosis of LDH not accompanied by other lumbar vertebral diseases, such as central canal stenosis, spondylolisthesis, or instability; 2) significant postoperative improvement in symptoms, with MRI showing complete decompression of the nerve root; 3) reherniation at the same lumbar vertebral segment; 4) complete radiologic results from preoperative/postoperative or reherniation assessment performed at our hospital; and 5) unilateral single-segment surgery. The exclusion criteria were as follows: 1) other lumbar vertebral comorbidities, such as lumbar vertebral tumor, lumbar vertebral infection, lumbar spondylolisthesis, or spinal stenosis; 2) absence of a remission period after the first surgery; 3) newly developed reherniation of discs at other levels; and 4) missing radiologic data. A total of 285 patients met our screening criteria. The follow-up period was 12-24 months.
Surgical Methods
Each patient was placed in a lateral recumbent position on the contralateral side, and a cushion was placed under the waist. After confirming the target segment, a longitudinal incision of measuring approximately 7 mm in length was made through the skin, subcutaneous tissue, and deep facia, with a 3-stage cannula used to expand the incision step by step. After the cannula position was satisfactory, a working cannula and foraminoscope were inserted through the intervertebral foramen under C-arm fluoroscopy navigation. A disposable bipolar radiofrequency knife was used to perform complete hemostasis under endoscopic observation prior to observing anatomical structures such as the superior articular process and target intervertebral disc. Under endoscopic observation, nucleus-pulposus forceps and blue forceps were used to resect the herniated nucleus-pulposus tissue and free the nucleus pulposus at the target intervertebral disc to decompress the nerve root and dural sac as much as possible. The nerve root was carefully examined until compression was no longer observed. During resection, care was exercised not to damage the nerves and dura. Finally, a disposable bipolar radiofrequency knife was used to ablate the annulus-fibrosus tear, and hemostasis was carefully performed. After confirming that there was no large bleeding and no dural tears, the foraminoscope and working cannula were removed. The incision was sutured once and bandaged with sterile dressing. All TELD surgeries were performed by spinal surgeons with the rank of deputy chief physicians and above.
Postoperative Management
On day 2 postsurgery, patients wore waist braces and were allowed to leave the bed for exercise. MRI scans were performed within 48 h of surgery, and patients wore a waist brace for at least 4 weeks after surgery. Patients were instructed to avoid bending, carrying heavy loads, and performing strenuous exercise for 3 months after surgery and to gradually resume normal physical activity afterward. All patients underwent lumbar vertebral MRI at 6 months after surgery to assess whether the operated segment had recovered. Postoperative follow-up was conducted for at least 12 months after surgery.
Diagnostic Criteria for Early Recurrence
The diagnostic criteria for early recurrence were as follows: significant alleviation of nerve root-related symptoms after TELD and immediate postoperative review of MRI showing complete loosening of the compressed nerve roots, recurrence of nerve root-related symptoms within 6 months after TELD, and MRI scan showing reherniation, displacement of ipsilateral or contralateral neural structures and the contralateral nerve in the operated segment. Recurrence 6 months after surgery was seen as non early recurrence. At least 1 spinal surgeon and radiologist determined whether recurrence had occurred in the patient.
Study Variables
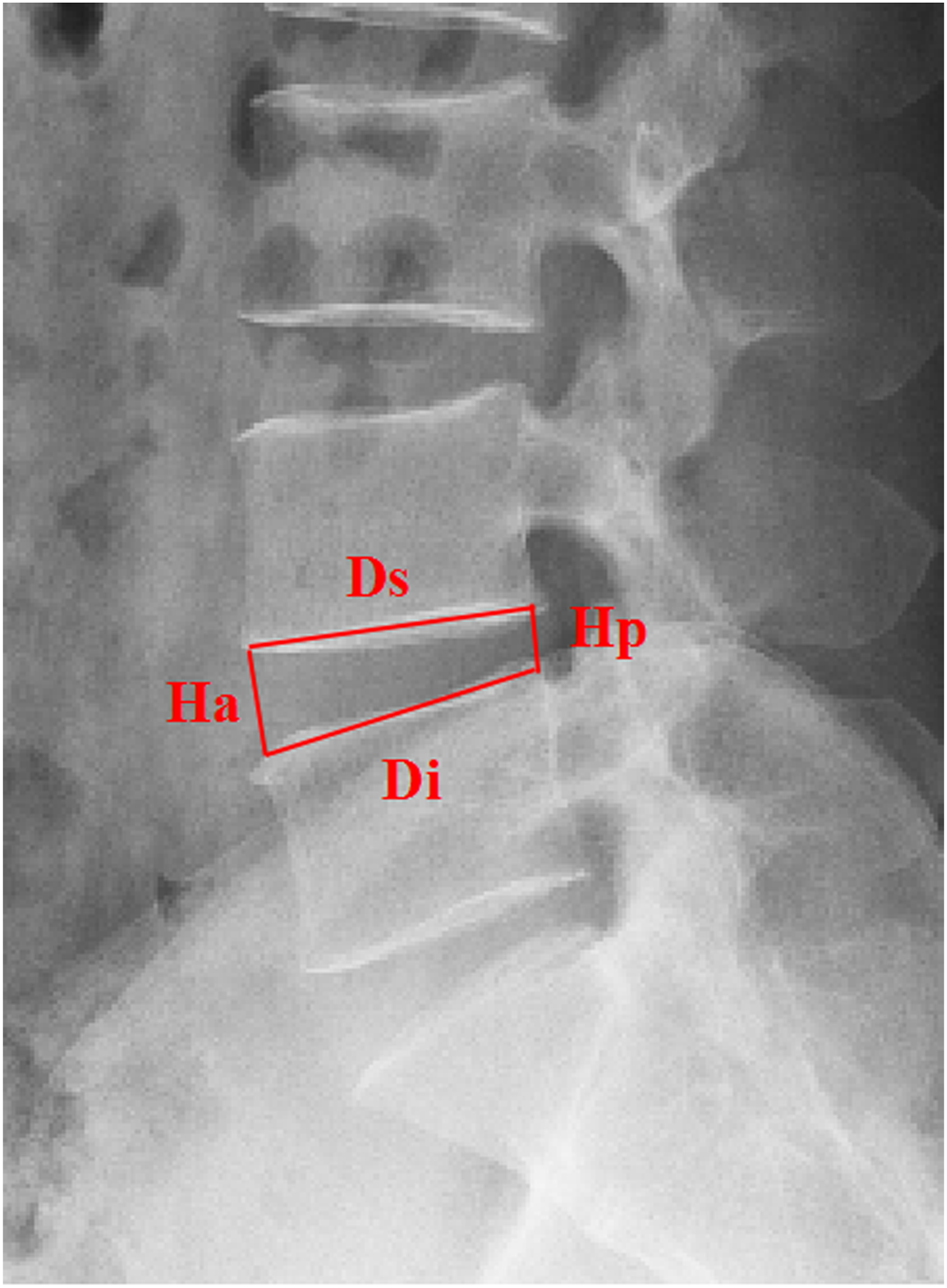
A visual analog scale (VAS) was used to assess the pain level in all the study participants immediately before and after surgery. Two spinal surgeons performed measurements using radiologic data, and the average of the 2 measurement results was obtained. Observation markers included disc-height index (DHI), sagittal range of motion (sROM), herniation level, base width, degree of intervertebral disc degeneration, herniation site, postoperative annulus-fibrosus tear size, cross-sectional area of the foramen (CSAF), Modic change and migrated herniation. 1. The DHI was defined as the ratio of the sum of the anterior and posterior edge heights of the intervertebral disc to the sum of the neighboring endplate widths, as assessed using lateral X-rays (Figure 1).
16
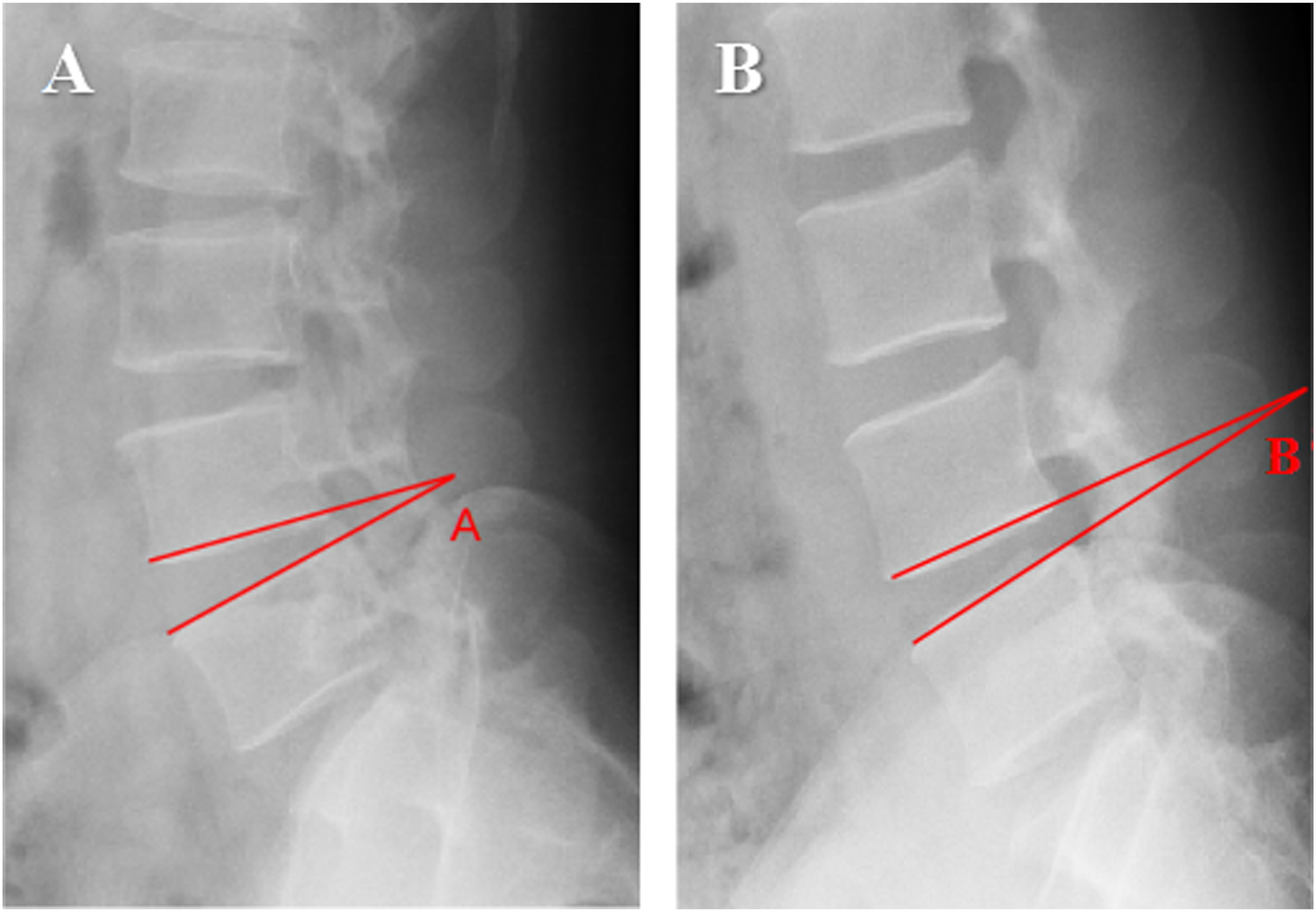
2. The sROM was defined as the difference in the angle between adjacent vertebral bodies at hyperflexion and hyperextension positions, as assessed using lumbar vertebral dynamic posture X-rays (Figure 2).
17
An sROM greater than 11° was considered indicative of lumbar vertebral instability.
18
3. Pfirrmann grading based on MRI sagittal plane signals, divided into grades I–V, was used to assess the degree of intervertebral disc degeneration.
19
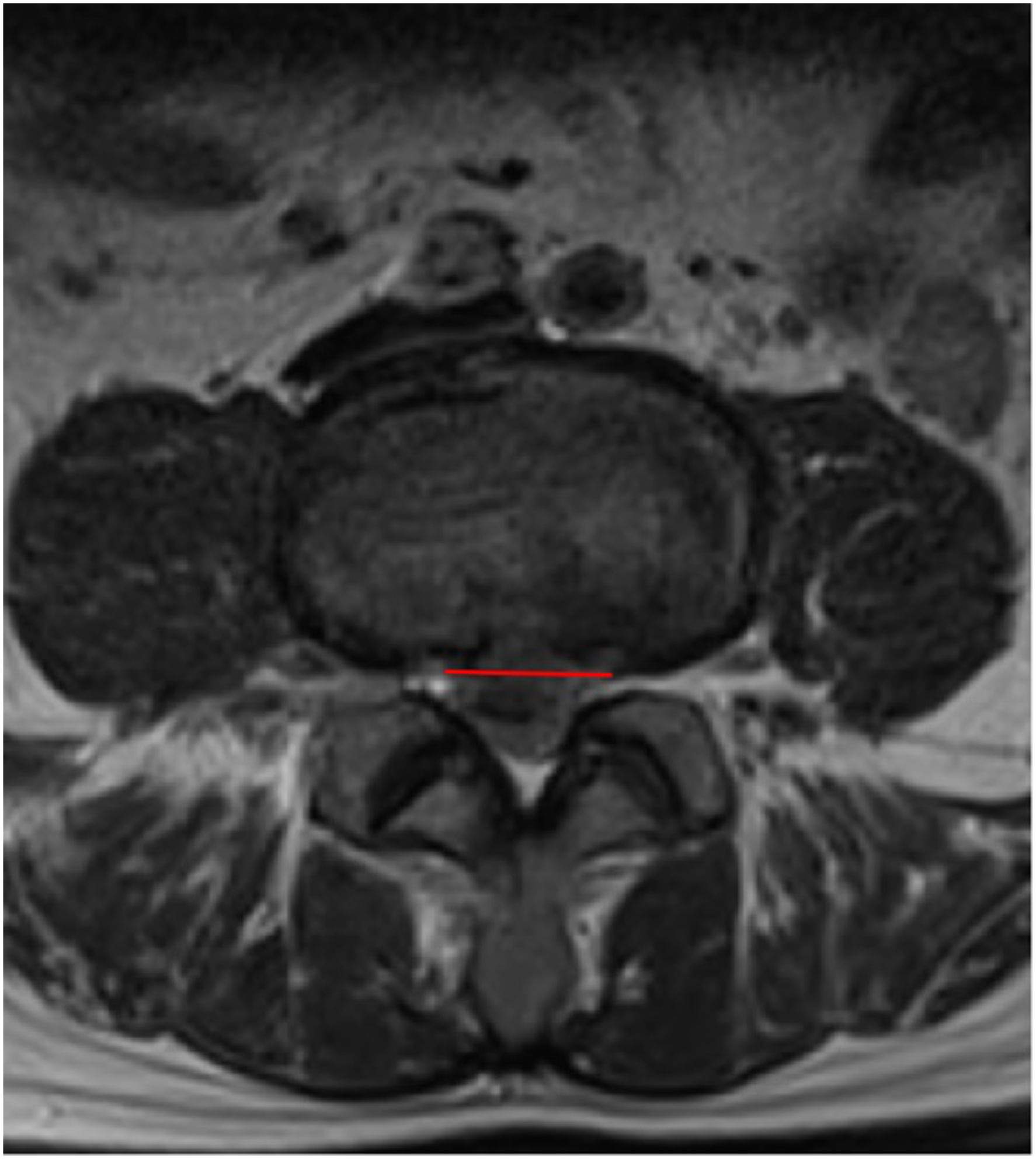
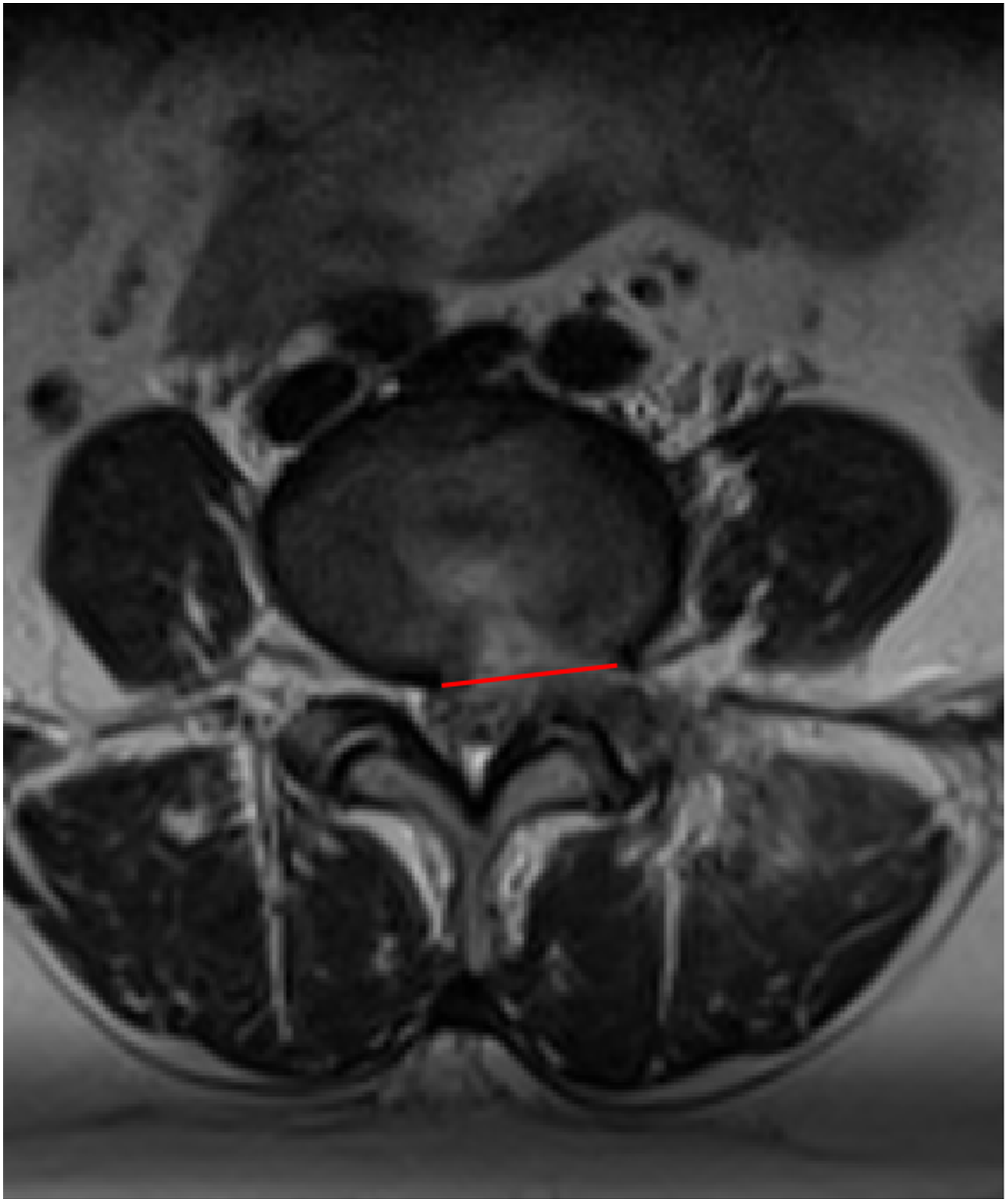
4. The base width was expressed as the width of the overlap between the herniated nucleus pulposus and outermost layer of the annulus fibrosus on the transverse plane on MRI (Figure 3). 5. The postoperative annulus-fibrosus tear size was defined as the annulus-fibrosus tear size on the outermost layer of the transverse plane on MRI (Figure 4). 6. The CSAF was measured using an imaginary line around the neural foramen on the surgical side in a parasagittal plane on MRI (Figure 5).
20
7. Migrated herniation was defined as a herniation mass cranially or caudally reaching more than a quarter of the height of the vertebra
21
. 8. The degree of Modic change was evaluated based on the MRI signal in the sagittal plane and was divided into grades I–III.
22
Visual representation of disc-height index, where DHI = [(Ds + Di)/(Hp + Ha)] × 100. Hp: posterior edge height of disc; Ha: anterior edge height of disc; Ds: lower endplate width of superior vertebra; Di: lower endplate width of inferior vertebra Visual representation of sagittal range of motion (A) Angle of hyperextended segment; (B) angle of hyperflexed segment. sROM =∠A−∠B Visual representation of base-width of herniation Visual representation of postoperative annulus-fibrosus tear Visual representation of cross-sectional area of the foramen

The same equipment was used for all preoperative and postoperative MRI scans and X-rays, and all imaging was performed using the same settings. T1- and T2-weighted turbo spin-echo sagittal images were used for MRI measurements. Available software (CarestreamVue PACS, Canada) was used to measure all parameters.
Statistical Analysis
All statistical analyses were completed using SPSS 25.0 (Chicago, Illinois, USA). The independent-samples t test was used to compare differences in the DHI, sROM, base width, CSAF and postoperative annulus-fibrosus tear size between the 2 groups. Ranksums were used to analyze the degree of intervertebral disc degeneration. The location of the herniation, the presence of migrated herniation, Modic change, and herniation level were analyzed using a chi-squared test. Logistic regression analysis was used for multivariate analysis of factors associated with early recurrence after TELD, the outcome variable is either early recurrence or not. Age, gender and BMI variables were controlled in the model. A two-tailed P value<.05 was considered statistically significant.
Results
Two hundred and eighty-five patients were included in this study. The mean follow-up duration was 15.5 months. The mean VAS scores were 7.38 ± .79 and 2.74 ± .89, for preoperative and postoperative testing, respectively, respectively. After surgery, 19 patients experienced recurrence within 6 months, accounting for 79.2% (19/24) of all patients with recurrence. The early recurrence rate was 6.7%, and the mean recurrence time was 73.4 days (3-168 days). Thirteen patients were readmitted for treatment after recurrence. Of these 13 patients, 2 underwent open spinal fusion surgery, 6 underwent TELD surgery, and 5 received conservative treatment. Symptoms were significantly alleviated after treatment in these patients (Figure 6). 26-year-old male, L4/5 herniated and treated by TELD, pain in the left lower limb appeared again after 32 days, review of lumbar MRI see the original segment recurrence. (A) Preoperative MRI(B)Postoperative MRI (C)Recurrence lumbar MRI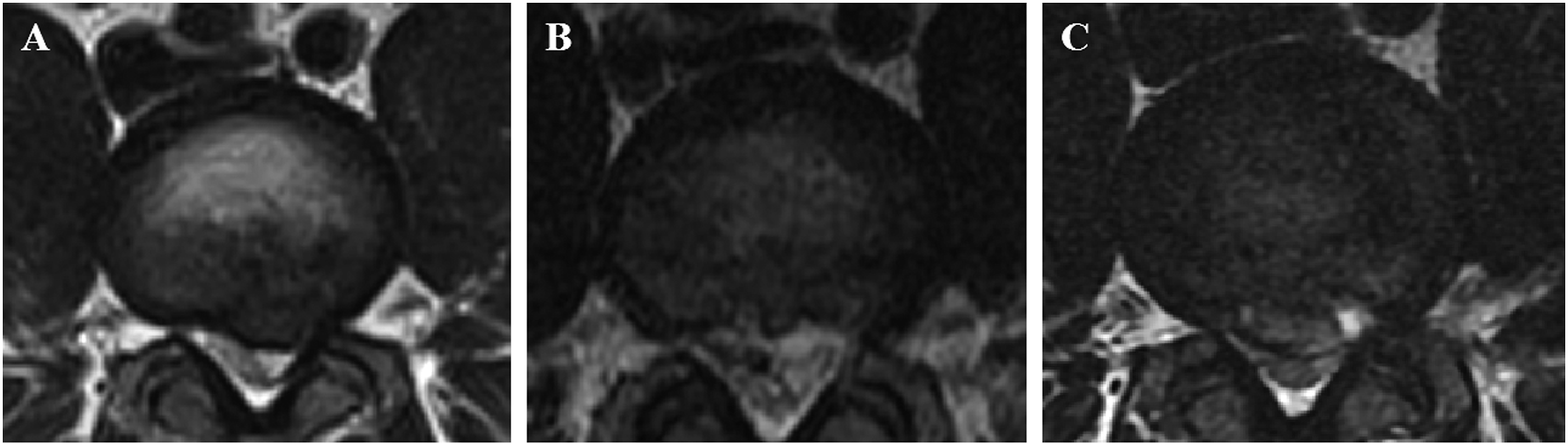
Comparison of radiologic data between early recurrence and non-early recurrence groups of patients
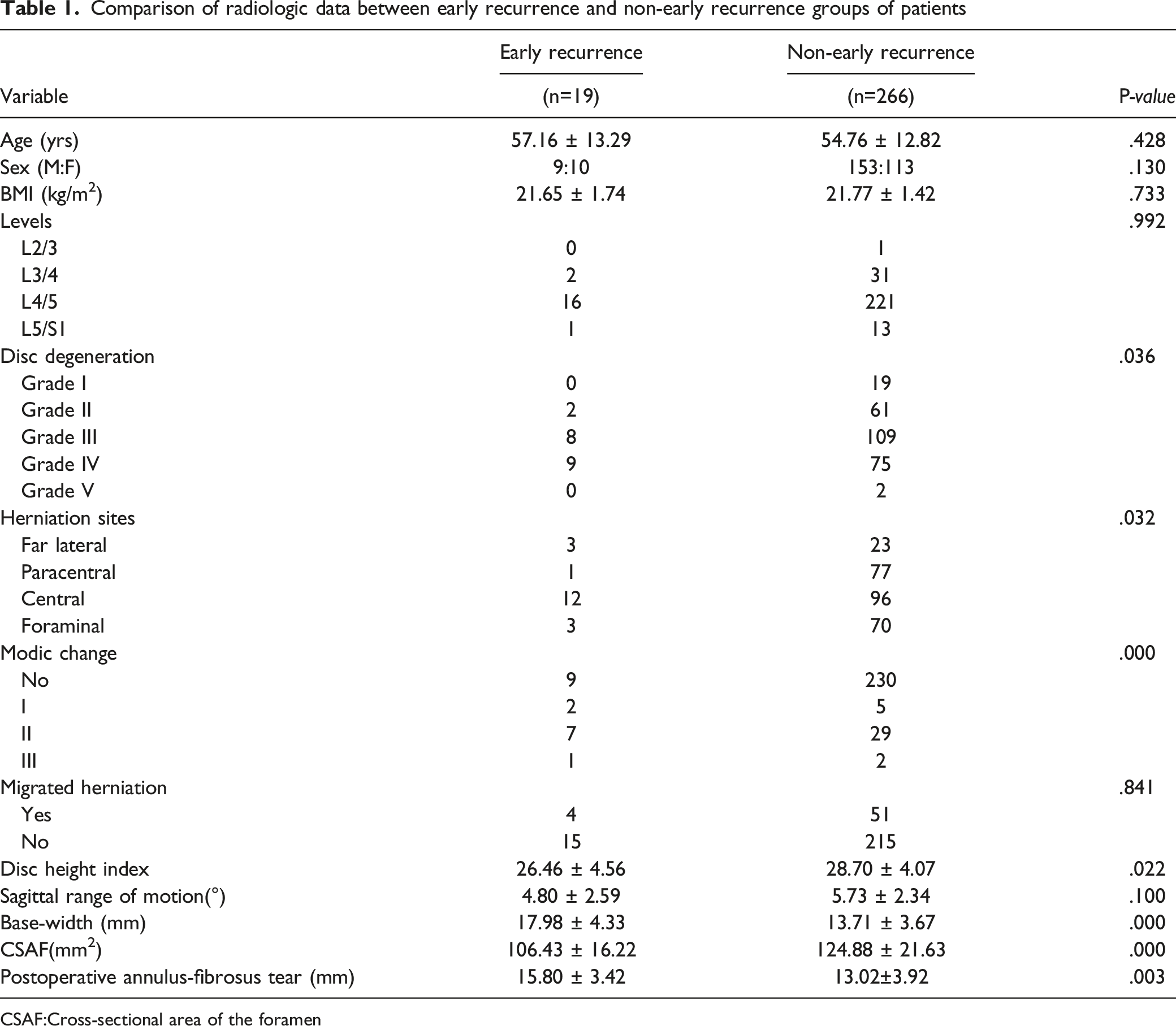
CSAF:Cross-sectional area of the foramen
Multivariate logistic regression analysis
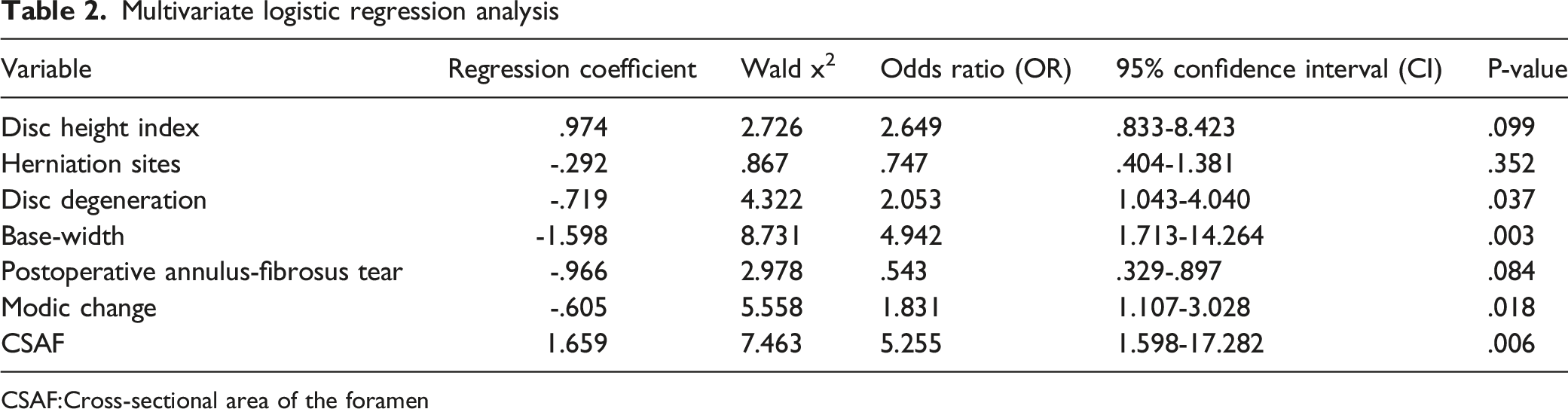
CSAF:Cross-sectional area of the foramen
Discussion
The results obtained in our present study will aid spinal surgeons in decreasing the recurrence rate of rLDH. Our results indicate that first, relevant radiologic examinations should be completed before surgery. A personalized approach to the surgical procedure should be used if risk factors for postoperative recurrence are discovered. In addition, it is important to implement a postoperative (at least 6 months) follow-up plan for these patients. Second, the working channel should be positioned correctly at the beginning of the operation, and damage to the annulus fibrosus should be minimized while ensuring complete nerve-root decompression during TELD; this approach is reliant on the surgical techniques used by the surgeon.
Reherniation, a common complication after lumbar disc herniation surgery, is the most common cause of repeated surgery after LDH. The incidence of rLDH ranges 5.7-15%,23–26 but time period for the occurrence of rLDH is currently undefined. One essential condition for a diagnosis of recurrence that a segment of the nerve root must experience a symptom-free period before postoperative symptoms appear.27–29 Studies show that approximately 60-80% of patients experience rLDH within 6 months after TELD 15,29,30. Therefore, examining the risk factors for early recurrence of LDH after TELD surgery is important for decreasing the incidence of rLDH. Factors that affect the recurrence of LDH after discectomy include age, body mass index, occupation, smoking, type and degree of intervertebral disc degeneration, lumbar vertebral mobility, postoperative exercise intensity, and the learning curve of the operating surgeon; these factors, however, remain debated.31–34 Thus far, few studies have reported on the factors influencing the early recurrence of LDH after TELD.
Intervertebral disc degeneration is themain cause of LDH. The results obtained in our present study indicate that the risk of developing rLDH increases with worsening severity of intervertebral disc degeneration, which has also been shown in other studies.12,17 During intervertebral disc degeneration, the content of type I collagen increases, while that of type II collagen decreases. Concurrently, proteoglycan and elastin content decreases, causing the nucleus pulposus to lose elasticity and enabling tears in the annulus fibrosus. As intervertebral disc degeneration becomes more severe, the self-repair capacity of the annulus fibrosus decreases, leading to nucleus-pulposus herniation. 35
Sagittal range of motion is a marker used to reflect lumbar vertebral stability. Studies have shown that increased sROM (particularly when sROM >10°) is associated with an increased risk of rLDH.31,36 Moreover, sROM is mainly impacted by intervertebral discs and facet joints. When sROM increases, the instability between lumbar vertebrae and the resultant stress may cause rLDH. 17 Interestingly, we found no significant correlation between sROM and rLDH, which may have been due to the low number of patients with early recurrence enrolled in our present study. It is also possible that extension was affected by lumbago during the acquisition of preoperative X-ray images, which were acquired in the extended position.
Studies have not only reported that DHI can objectively reflect intervertebral disc height but also indicate that it is a potential risk factor for rLDH; 37,38 however, that study did not find that the DHI was significantly lower in patients with recurrence than in those without recurrence, in agreement with the results of Kong. 39 We speculate that this is because an increased DHI may provide sufficient space for surgical resection of the nucleus pulposus. In addition, Hasegawa theorized that postoperative intervertebral disc collapse can result in greater intervertebral disc stability. 40 However, our study did not indicate that a low DHI is a risk factor for rLDH.
Kim et al 12 found that the risk of recurrence is higher in patients with paracentral herniation than in those with central and far lateral herniation. Conversely, we found that patients with central herniation were more prone to postoperative recurrence than those with paracentral herniation, in agreement with the results of Yao et al. 32 Yin et al. 30 also found that central herniation is an independent risk factor for recurrence after TELD. We believe that this discrepancy may be related to the working position of the foraminoscope during the intervertebral-foramen approach used for nucleus-pulposus resection. Therefore, performing this procedure for central herniation using a working cannula will inevitably result in further damage to the annulus fibrosus, which may account for the likely recurrence of central herniation.
Park et al. 15 found that small herniated discs were associated with early recurrence and the smaller the size of the herniated disc was, the earlier recurrence occurred. Conversely, we found that patients with increased base width and postoperative annulus-fibrosus tears tended to develop early recurrence after TELD. This may be because an increased base width usually indicates that the size of the annulus-fibrosus tear, caused by LDH, is also increased, as is the tendency for residual nucleus-pulposus fragmentation during surgery. Hence, to achieve complete decompression, the surgeon may further expand the area for resection of the annulus fibrosus. Annulus-fibrosus tears and defects will accelerate intervertebral disc degeneration, increase the likelihood of nerve-root adhesion and sterile inflammation and are the main cause of chronic lumbago after discectomy. 41 Lee et al. 29 found that the site of rLDH was generally identical to the original herniation site. This finding indicates that nucleus-pulposus herniation in most rLDH patients is caused by reherniation via the original annulus-fibrosus tear, which may be related to the repair of the annulus-fibrosus tear after TELD. The intervertebral disc is the largest avascular organ in the human body, and its self-repair capacity is limited. Using animal models, Melrose 42 showed that only the outer 1/3 of the annulus-fibrosus tissue can slowly heal using scar formation after damage to the annulus fibrosus. Therefore, a larger tear indicates an increased risk of reherniation at the early postoperative stage when the annulus fibrosus has not yet been repaired; this notion is consistent with the results obtained in previous studies.37,43,44 In addition, suturing and repair of the annulus fibrosus during discectomy can effectively decrease the rate of recurrence.45,46 This finding also indirectly demonstrates that defects in the annulus fibrosus are associated with recurrence after discectomy.
The Modic change is defined as the change in the signal intensity change of the endplate on MRI and indicates the corresponding area of pathology and its association with disc degeneration. 22 In studies by Brooks 47 and Yao, 14 Modic change was identified as a risk factor for recurrence. In this study, the degree of Modic change remarkably affected early recurrence after TELD. Modic change usually means reactive vertebral modification associated with inflammation, an unstable microenvironment, or degenerative disc disease. When the endplate presents with changes, its protective effect is weakened.
The CSAF was identified as a risk factor for TELD recurrence in this study. The foramina are the direct channels for surgical entry in TELD, and their size affects the placement of working channels. Improper placement of working channels could interfere with the operation and affect the treatment of the intervertebral disc. 13 Moreover, foraminal area is affected by the disc height, and the disc height collapse after PTED will make the foraminal area smaller, which will result in a reduced effective activity space of the nerve root and increase the possibility of nerve root compression.
Matsumoto’s studies showed that migrated herniation was a potential risk factor for recurrent herniation because of the difficulty in removing fragments beyond the working area due to the limited endoscopic view. 48 However, no significant difference was observed between the nonearly recurrence group and the early recurrence group in our study in terms of migrated herniation. We speculate that the surgeon's experience and technical factors compensate for the insufficient field of vision.
Our present study had several limitations. First, the number of patients with early recurrence was low, resulting in the difficulty to perfectly obey the normal distribution due to the sample size. Second, we only analyzed the relationship between several radiologic factors and early recurrence after TELD and did not perform a multivariate analysis of epidemiological, anatomical, postoperative-care, and other factors such as osteophytes, high-intensity zones, loss of lordosis, which may have affected the study results. Thrid, we excluded patients with incomplete radiographic data, missing data may lead to changes in database studies. 49 Therefore, a study using detailed statistical analysis will be conducted in the future to verify the results of our present study. Furthermore, it is a novel way to investigate rLDH with a simplified nomogram. 50
Conclusion
The disc-height index, postoperative annulus-fibrosus tear size, and location of disc herniation were associated with early recurrence after TELD. Increased base width of the herniation, severe disc degeneration, decreased CSAF and Modic change were risk factors for early recurrence after TELD. Decreasing intraoperative damage to the annulus fibrosus and implementing early postoperative follow-up were positively associated with a decreased incidence of early recurrence after TELD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Project of Hunan Provincial Health Commission (Project number 202104070077), Hunan Provincial Clinical Medical Technology Innovation and Guidance Project (2020SK51807) and Hunan Provincial Natural Science Foundation (2020JJ4549).