
Abstract
Study Design
Retrospective cohort study.
Objective
This study was conducted to observe whether patients with more than 50% resection of the inferior articular process (IAP) develop spinal instability.
Methods
Patients who underwent unilateral single-segment Interlaminar Endoscopic Lumbar Discectomy (IELD) were reviewed from March 2017 to March 2023 at the authors’ institution. Patients with more than 50% resection of the IAP were included. All patients were divided into 2 groups:group T (total resection of IAP), group P (partial resection of IAP). Oswestry Disability Index (ODI) score was used to evaluate low back pain. The following radiographic parameters were measured: (1) slip and disc arc on standing lateral flexion/extension radiographs; (2) intervertebral space height (ISH); and (3) length, width, and thickness of the IAP. (4) width of superior articular process (SAP). The volume of the IAP was estimated by multiplying its height, width and thickness. Patients with Δ slip ≥3 mm or Δ arc ≥15° were classified as having segmental instability. All the parameters were compared with their former values. Correlation coefficients were calculated to evaluate the associations among Δslip, Δarc, ODI, changes in ISH, and other metrics. Multiple linear regression analysis was performed to identify independent predictors of recovery rate after IAP resection. The demographic characteristics of the patients, surgical data, radiographic measurements, and ODI were also compared between the 2 groups.
Results
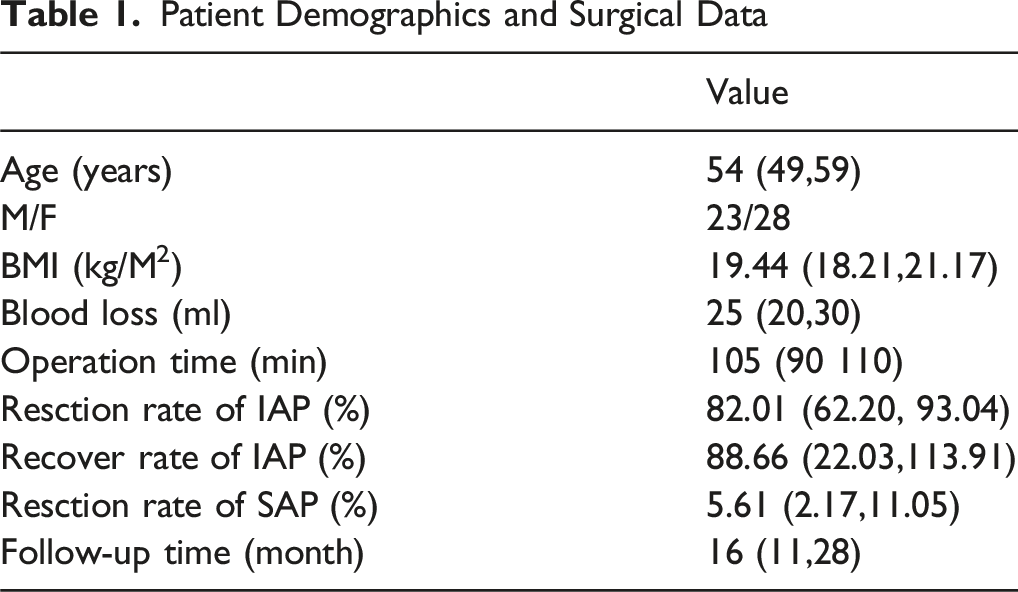
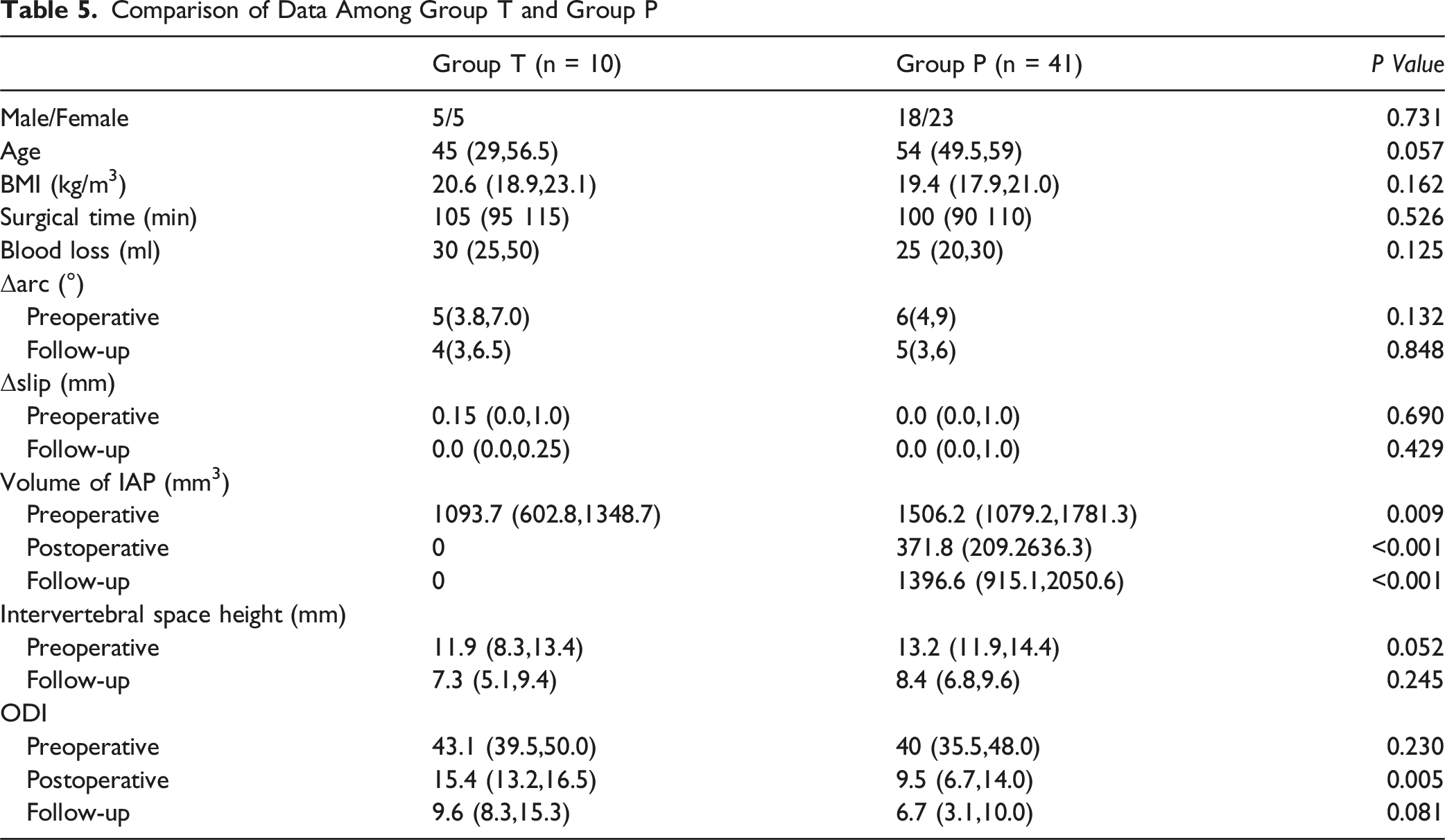
Fifty-one patients were included in the study, and the resection rate of the IAP was 82.01% (62.20%, 93.04%). There was no significant difference in the dynamic arc or slip between preoperative and follow-up (P > 0.05). No case of segmental instability observed at follow-up. The volume of the IAP increased significantly at the final follow-up compared with that immediately after surgery (Z = −5.579, P < 0.001). The recovery rate of IAP was 88.66(22.03,113.91) % with an average time of 16(11,28) months. The follow-up ODI and ISH was 6.5(4.4,11.1) and 7.9(6.5,9.5) mm, respectively. Compared with those before the operation, ODI and ISH decreased significantly (Z = −6.216, P < 0.001; Z = −6.215, P < 0.001). After adjusting for confounding factors, IAP resection rate (β = −0.583, B = −1.821, P < 0.001) and follow-up duration (β = 0.502, B = 0.017, P < 0.001) were the strongest independent predictors of recovery rate, followed by age (β = 0.200, B = 0.010, P = 0.036). No significant independent associations were observed for sex or BMI with IAP recovery rate. At the final follow-up, the volume of the IAP showed no increase in group T, with a significant difference compared with group P (Z = −4.882, P < 0.001). The postoperative ODI score was higher in group T (Z = −2.799, P = 0.005), but there was no significant difference between the 2 groups at the final follow-up.
Conclusion
In the cohort of this study, patients with >50% IAP resection did not develop radiographic instability, and some showed bone regeneration, though those with complete resection did not regenerate.
Keywords
Introduction
Interlaminar Endoscopic Lumbar Discectomy (IELD) is widely used to treat lumbar disc herniation (LDH) and lumbar spinal stenosis because of its advantages in terms of surgical trauma and recovery time. Inferior articular process (IAP) resection is commonly performed for exposure and decompression of the nerve root. This is especially true in patients with LDH who have significant facet joint hyperplasia, joint convergence, or lateral recess stenosis. Inadequate resection of the IAP makes it difficult to expose the nerve root and dural sac, which increases the risk of nerve root and dural sac injury or leads to unsatisfactory decompression. However, long-term instability may occur if too much bone is removed. Some scholars have reported a high incidence of postoperative segmental instability in total facetectomy patients,1,2 and some authors suggest spinal fusion for the unstable segment as a necessary stabilizing component. 3 Therefore, accurate removal of bone during surgery is quite challenging and relies on the professional judgment of the surgeon. Currently, there is no reliable evidence regarding the relationship between the range of IAP resection and segmental instability. Biomechanical studies suggest that resection of more than 50% of the articular process may cause spinal instability,4-7 but these were in vitro studies that only represented the stability of the passive spinal stability system immediately after surgery and could not reflect the actual clinical conditions. Dohzono et al followed up and compared patients with lumbar spondylolisthesis and lumbar spinal stenosis treated by endoscopic decompression. An increase in intervertebral slip and articular process bone formation has been reported after surgery, but this increase does not affect clinical outcomes. 8 However, in their study, the extent of resection of the articular processes was relatively small (27.2% and 16.6% in the 2 groups, respectively), and the impact on segmental stability was limited. Toru Doi 9 et al followed 116 patients who underwent microendoscopic laminectomy and found that the extent of facet joint resection has a minimal impact on radiographic and clinical outcomes. However, the patients included in their study were those with lumbar spinal stenosis. Patients with lumbar spinal stenosis often have articular process hyperostosis and decreased intervertebral space, and their segmental stability is better than that of younger patients (such as those with intervertebral disc herniation). Therefore, the applicability of their conclusions is limited. Therefore, we followed up some patients with lumbar disc herniation who had undergone IELD with more than 50% IAP resected, aiming to observe whether there was segmental instability.
Methods and materials
Patient Selection
The postoperative CT scans of 1172 patients who underwent IELD at our hospital from March 2017 to March 2023 were reviewed (Figure 1). We assessed the extent of postoperative IAP resection on CT scans by measuring the length, width, and thickness of the IAP. The inclusion criteria were: (1) unilateral, single-segment IELD performed more than 6 months ago; (2) resected volume of the IAP exceeding 50%; and (3) age between 20 and 65 years old. (4) patients with complete clinical and imaging data, including preoperative dynamic X-ray films, preoperative/postoperative CT scans, and medical records. The exclusion criteria were: (1) patients with a history of lumbar spine surgery, infection, tumors, or trauma. All patients were divided into the 2 groups:group T (total resection of IAP), group P (partial resection of IAP). This study was funded by Zigong Key Science and Technology Program -Zigong Academy for Medical Big Data and Artificial Joint Intelligence Project (Project No.: 2023-YGY-2–05) and approved by the ethics committee of our institution (No. EC-2023-007), and informed consent was obtained from all participants. The demographic characteristics of the patients included age, sex, and body mass index (BMI, calculated as weight in kilograms divided by the square of height in meters). Surgical data, including blood loss, operative time, complications, and comorbidities, were also recorded. The flow of patient recruitment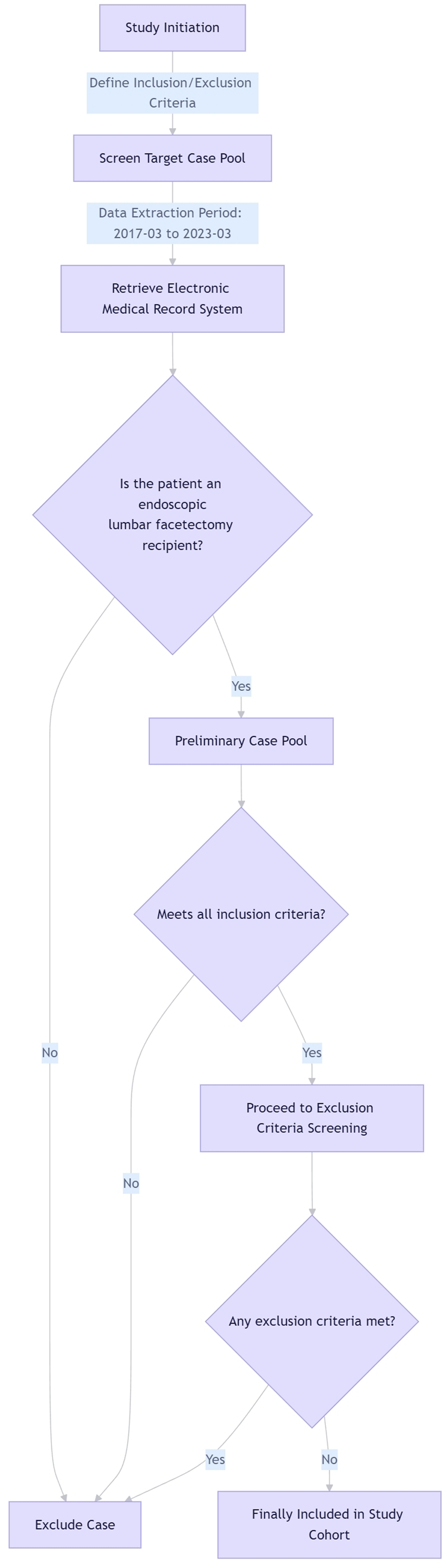
Surgical Technique
Following general anesthesia, the patient is positioned prone on a radiolucent frame. The target lumbar level is confirmed via fluoroscopy. A paramedian skin incision (8-10 mm) is made ipsilateral to the pathology, approximately 1-1.5 cm off the midline. A guidewire is advanced to the interlaminar space. Sequential dilators are passed, followed by placement of a working cannula.
The endoscope is introduced through the cannula. Soft tissues are cleaned to expose anatomical structures (lamina, ligamentum flavum, Inferior Articular Process). Partial IAP resection may be performed using endoscopic burrs or punches to optimize access. The ligamentum flavum is dissected and resected endoscopically.
Under direct endoscopic vision, the traversing nerve root is gently mobilized medially, exposing the herniated disc. Herniated nucleus pulposus fragments are meticulously removed using endoscopic pituitary forceps and radiofrequency probes under continuous irrigation. Endoscopic inspection confirms complete decompression of neural elements and absence of retained fragments.
Hemostasis is achieved endoscopically. The working cannula and endoscope are withdrawn. The small incision is closed with a single suture.
Radiographic Assessment
Patients were followed, and ODI, upright lateral flexion-extension, and CT scans were performed. Dynamic disc arc (Figure 2) and slip (Figure 3) were measured using the method described by Dupuis et al.
10
The differences in slip and disc arc between the flexion and extension positions were calculated as dynamic Δ slip (mm) and dynamic disc arc Δ arc (°), respectively. Patients with Δslip≥3 mm or Δarc≥15° were classified as having segmental instability.
11
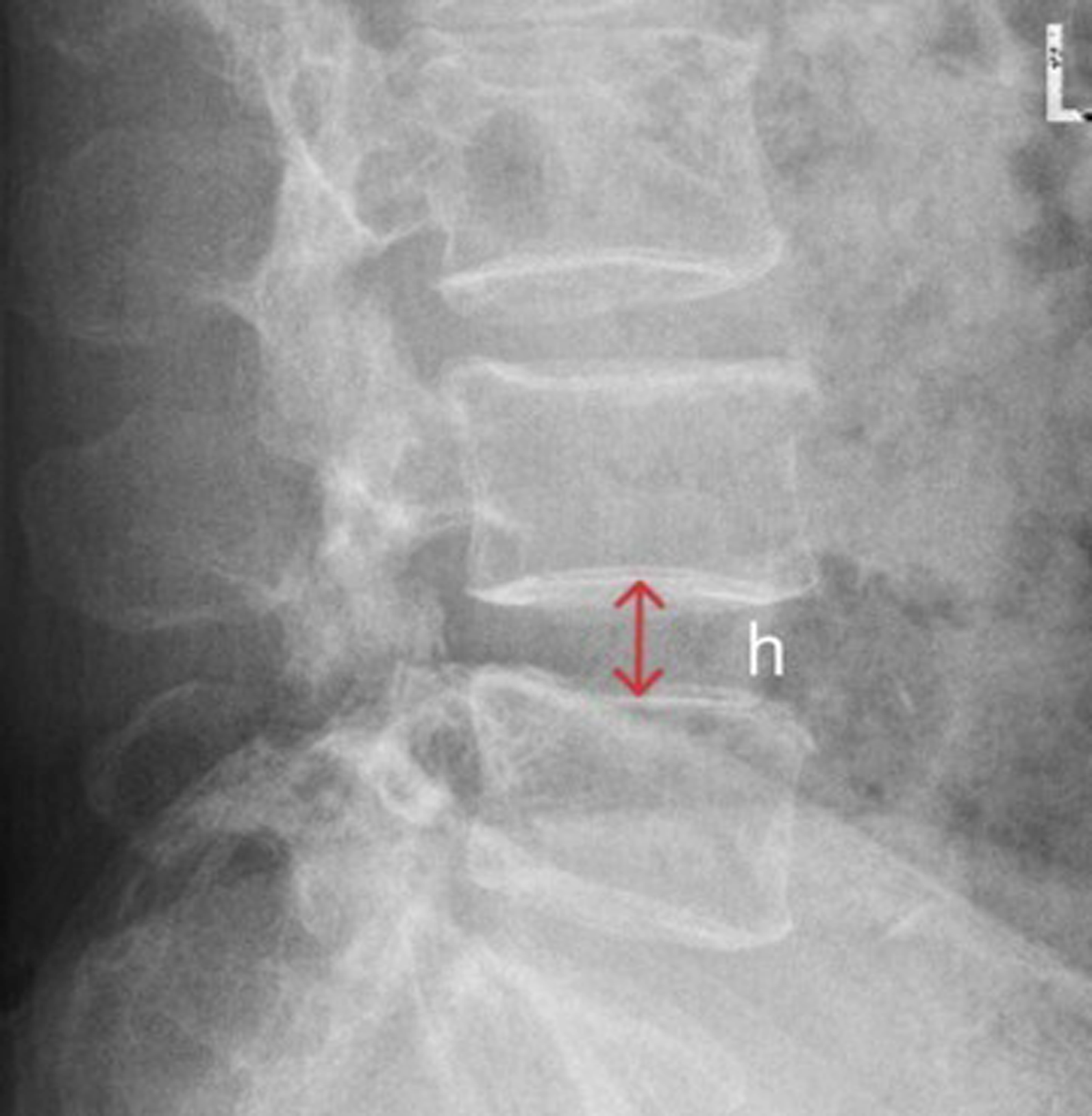
The ISH (Figure 4) was obtained by measuring the height at the middle of the endplates. The thickness, width, and height of the IAP on the surgical side were measured to calculate the volume (Figure 5).The measurement methods referred to those described by Kunkel et al.
12
and Wang et al.
13
Height of IAP: the distance between the superior and inferior margins of the facet articular surface along the facet joint surface; the measurements were made at the level where the facet joint was the longest in the sagittal plane. 2. Width of IAP: the distance from the midpoint of the medial and lateral edges of the facet surface, the measurements were made at the level where the facet joint is the widest in the coronal plane.3. Thickness of IAP: the anterior and posterior diameter of the center of the IAP. Since all patients in this group suffered from lumbar disc herniation, were relatively young, and had mild articular process hyperostosis, it was considered that no or only a small portion of the medial part of the superior articular process (SAP) needed to be resected during endoscopic discectomy. Therefore, we only measured the thickness of the SAP to evaluate its resection rate (Figure 6). Considering the irregular shape of the articular process, the volume of the articular process was estimated as V = thickness × width × height. Flexion-extension radiograph measurements were performed preoperatively and at the final follow-up, and the IAP volume measurements were performed preoperative, postoperative and at the final follow-up. The resection rate of IAP was calculated via the following equation: (Vpreoperative-Vpostoperative)/Vpreoperative*100;The SAP resection rate was calculated as follows: (preoperative SAP width - postoperative SAP width)/preoperative SAP width × 100%;The IAP recovery rate was calculated as follows: (follow-up IAP volume/preoperative IAP volume) × 100%. Radiographic measurements of the dynamic disc arc. α = intervertebral angle on flexion view; β = intervertebral angle on extension view. Δarc = β-α Radiographic measurements of dynamic slip. S1 = distance of slip on extension view; S2 = distance of slip on flexion view. Δslip = S1-S2 Measurement of intervertebral space height. h = height of intervertebral space at middle of endplates on lateral view Radiographic measurements of the IAP volume. b = length of the IAP; c = thickness of the IAP; d = width of the IAP; volume of the IAP (VIAP) = b*c*d Radiographic measurements of the SAP width. e = SAP width measured at the center of SAP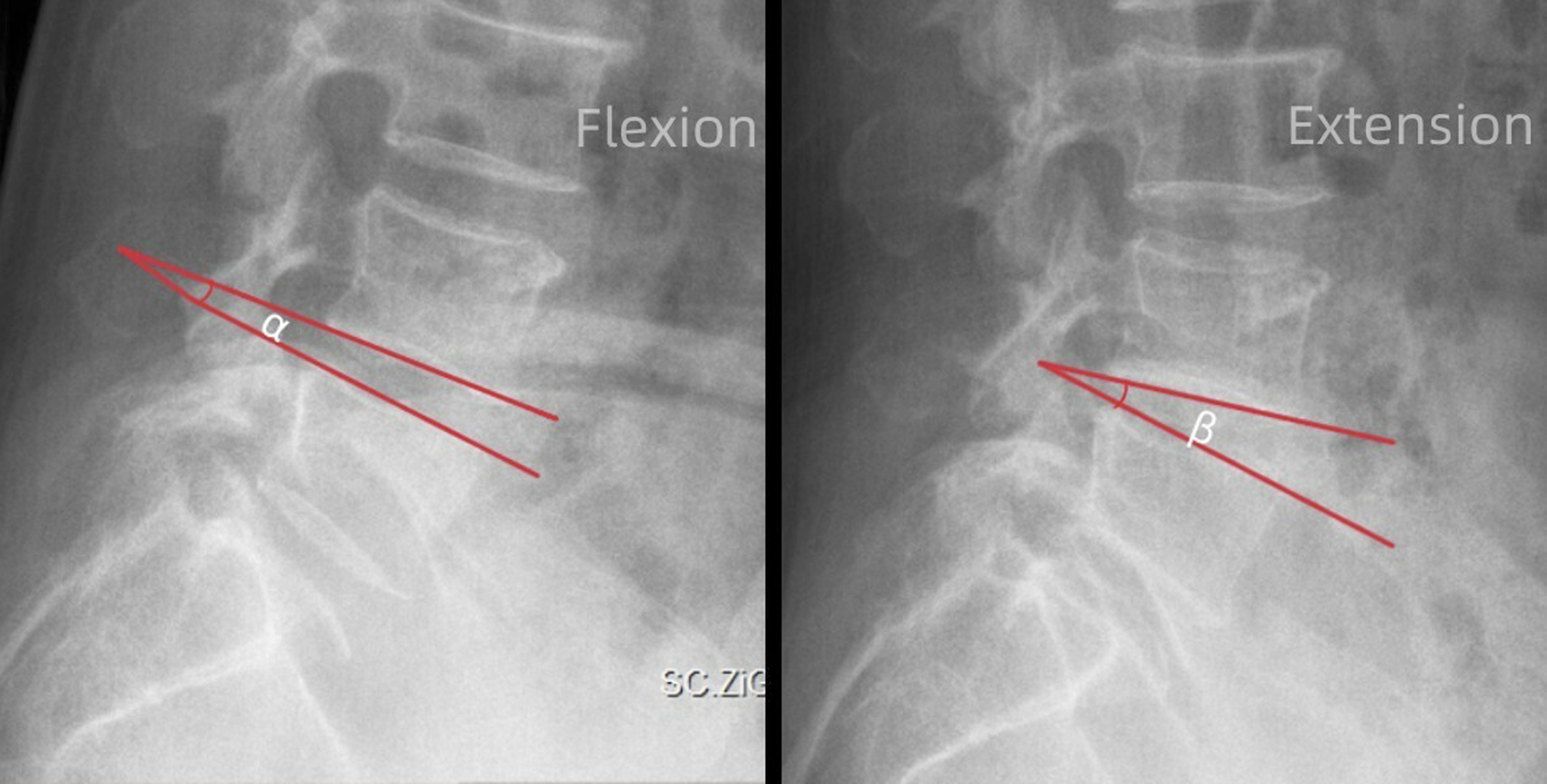



Statistical Analysis
All the data were tested for normality via the Shapiro–Wilk and Kolmogorov‒Smirnov methods. Data with a normal distribution are expressed as the mean ± standard deviation. If the data are skewed, the median and quartiles are used. The following parameters were compared between preoperative and follow-up assessments: Δslip, Δarc, ODI, ISH, and postoperative IAP volume. Wilcoxon rank sum tests were used for skewed data. Mann-Whitney U test was used to compare the parameters between group T and group P. Correlation coefficients were calculated to evaluate the associations between Δ slip, Δ arc, ODI, changes in ISH, and other metrics. Multiple linear regression analysis was performed to identify independent predictors of recovery rate after IAP resection, with age, sex, BMI, facet resection rate, and follow-up duration as independent variables. All analyses were performed using SPSS 19.0 software (IBM Corp., Armonk, New York, USA). P values <0.05 were considered statistically significant.
Results
Patient Demographics and Surgical Data
Comparison of Parameters Between Preoperative, Postoperative and Follow-Up Data
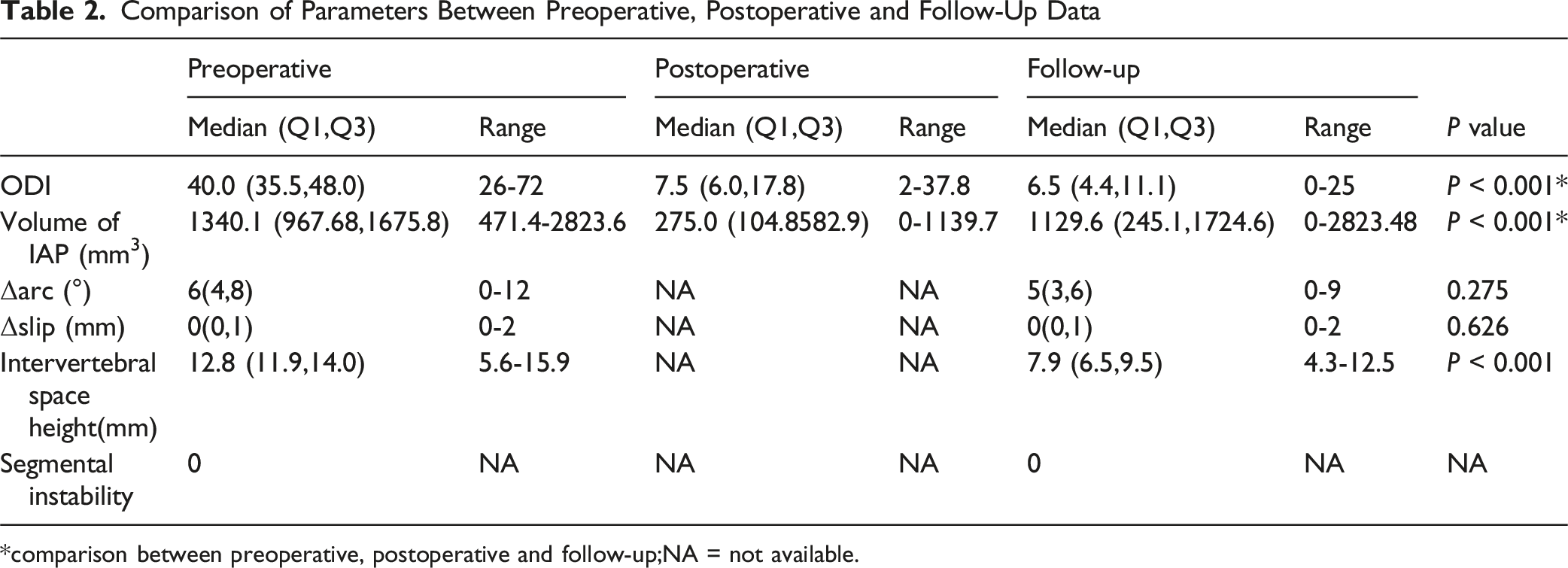
*comparison between preoperative, postoperative and follow-up;NA = not available.
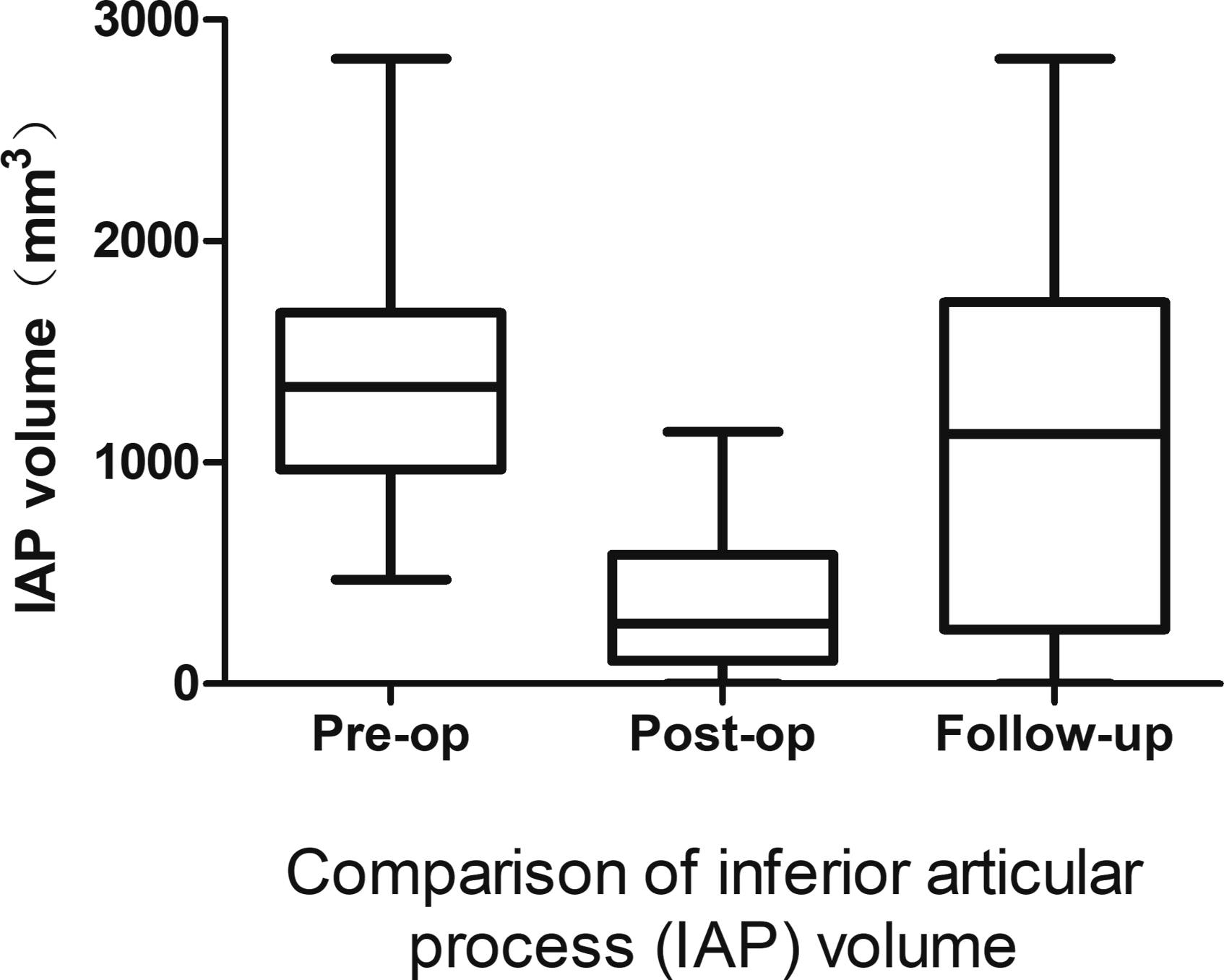
Comparison of IAP volume. The difference between groups was statistically significant
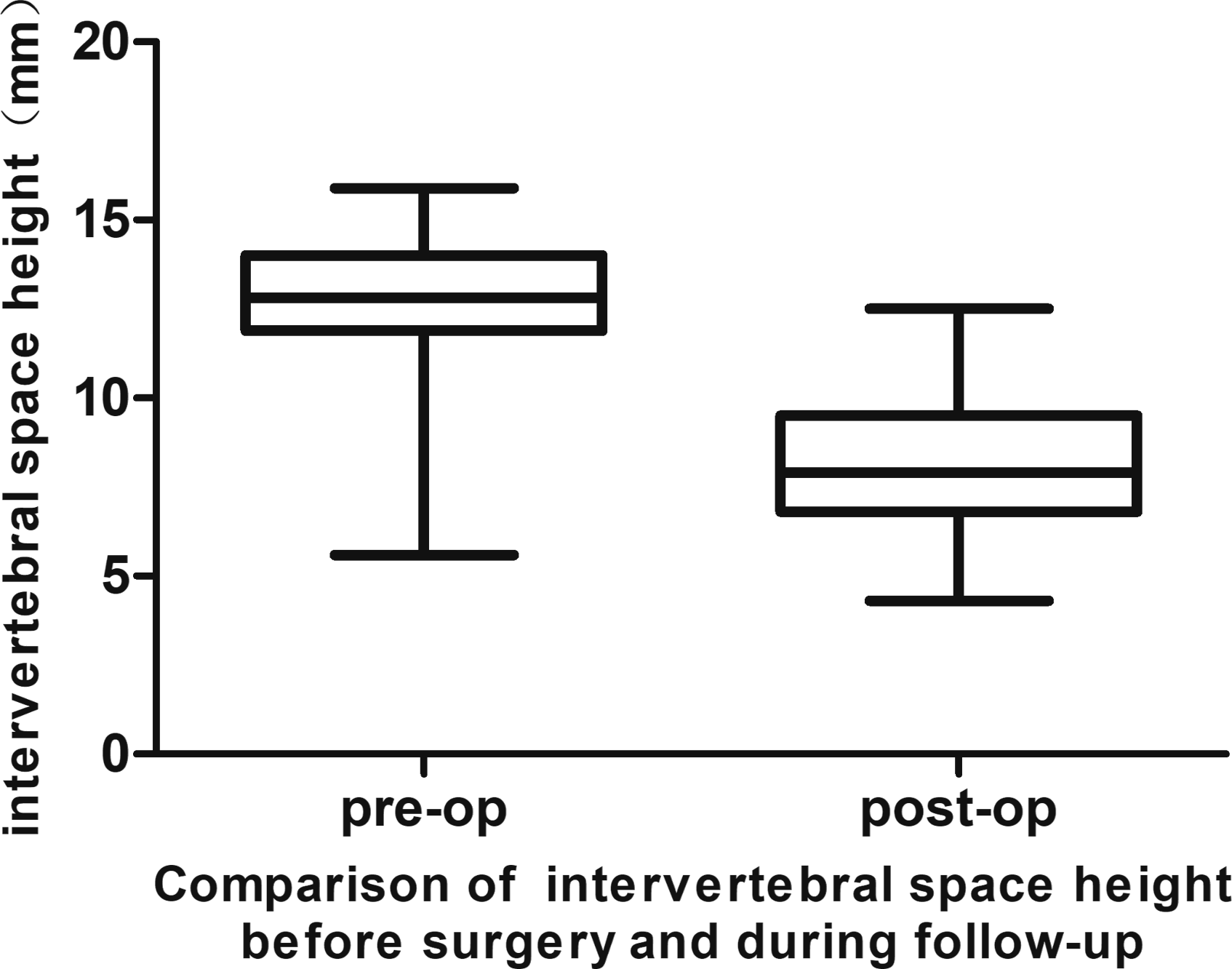
Comparison of intervertebarl space height.The difference between the 2 groups was statistically significant
P Value of Spearman Correlation Between Δslip, Δarc,ODI, and Other Metrics

*Spearman’s P = 0.401.
Multiple Linear Regression Analysis for Predictors of Recovery Rate After IAP Resection

Comparison of Data Among Group T and Group P
Discussion
1. Does IAP resection during IELD actually cause segmental instability?
The facet joint is composed of superior and inferior articular processes and the joint capsule. Its main function is to guide spinal movements and resist various loads, including compression, shear, and axial rotation.
14
The facet joints, along with the intervertebral joints, form the three-joint complex. Within a spinal motion segment, the movements of the 3 joints in the three-joint complex are coupled. Abnormal movement of one component inevitably affects the other 2. Excessive resection of the articular processes is thought to cause segmental instability, leading to recurrent low back pain and nerve injury. In severe cases, revision fusion surgery may even be required.
15
Consequently, during the IELD procedure, protection of the IAP is also important. However, there is a conflict between decompression and preservation of the articular process, which impacts the surgeons’ intraoperative and postoperative decision-making. This includes decisions regarding the safe extent of articular process resection intraoperatively, the need for fixation and fusion, and the use of orthoses postoperatively. There are also studies suggesting that resection of the inferior articular process has little impact on segmental stability. el-Bohy et al reported that the resistance of the facet joints to the flexion load is believed to be provided mainly by the joint ligaments, and the role of the bony structure is minimal.
16
Doi et al.
9
recently reported that the extent of facet joint resection has a minimal impact on radiographic and clinical outcomes at 1 year after single-level MEL surgery. In the present study, we specifically enrolled relatively young patients with isolated lumbar disc herniation. The rationale for this patient selection was that these patients had no evident spinal canal stenosis, thus neither lateral recess decompression nor superior articular process (SAP) resection was required intraoperatively, or only a minimal portion of the SAP was resected. This allowed us to maximally exclude the confounding effect of SAP resection on spinal segmental stability. As reported in the literature, no significant alteration in biomechanical stability is observed when less than one-fourth of the SAP is resected.
17
In our cohort, the resection range of the SAP was extremely limited, with a median value of 5.61% (2.17%,11.05%), which was significantly lower than the threshold reported in previous studies. Therefore, the resection exerted a negligible impact on segmental spinal stability. Through follow-up studies, we found that resection of the IAP of a single segment had a very limited impact on spinal stability. In the cases with more than 50% IAP resection in our follow-up cohort, no radiographic instability was identified. We believe that resection of more than half of the IAP does not cause spinal instability during IELD on the basis of the above findings. Therefore, there is no need to perform additional fixation and fusion during the operation. However, this does not mean that the inferior articular process can be freely resected without limitation for decompression, as long-term follow-up results are still lacking. During follow-up, we found that no IAP regeneration occurred in patients who underwent complete IAP resection. Instead, vertebral axial rotation and osteophyte formation were observed in these patients. Studies have shown that the articular processes also bear part of the compression load.
18
After IAP resection, intervertebral space subsidence may be accelerated, which in turn increases the risk of lumbar segmental instability and low back pain. Furthermore, it may lead to more rapid and severe spinal degeneration and the earlier development of lumbar spinal stenosis. Bone regrowth after decompression surgery is one of the main causes of restenosis requiring revision surgery, and several potential risk factors for new bone formation have been documented.19-21 The results of our study suggest that the IAP cannot regenerate in the complete resection group, and lumbar function is more significantly limited in the early postoperative period, but there is no obvious impact on spinal stability or lumbar function in the middle stage. Therefore, we recommend that during the IELD procedure, the IAP should be retained as much as possible. If more than half of the IAP is actually resected, pedicle screw fixation and fusion are not required. Instead, patients should wear a brace for protection and perform back muscle exercises to improve spinal stability. 2. How does the human body restores segmental stability after resection of the IAP?
We analyzed patients’ preoperative and follow-up X-rays and CT images to explore the mechanisms underlying the restoration of segmental stability. We measured the ISH on lateral X-rays and the IAP volume change using CT. At the final follow-up, the ISH was significantly lower than the preoperative baseline, whereas the IAP volume was significantly greater than the immediate postoperative measurements (partial resection group). The Δslip was positively correlated with ISH, which means a decrease in ISH may reduce intervertebral slippage. Based on these findings, we speculate that following resection of the intervertebral disc and IAP, the human body restores segmental stability through 2 mechanisms: 1. A decrease in the intervertebral space increases the contact area between the superior and inferior articular processes. 2. Regeneration of the articular process.
Studies have shown that surgical removal of the nucleus pulposus can significantly reduce the height of the intervertebral disc.22,23 Yang and King predicted a significant rise in facet joint loading pressure and reported that the percentage of segmental load transmitted through the posterior elements can increase up to 47% with the loss of disc space height.
22
After the intervertebral space height decreases, on the one hand, the superior and inferior articular processes can regain contact and restore partial stability; on the other hand, the contact between the superior and inferior articular processes increases the stress on the facet joints. In accordance with Wolff’s law, under stress, the IAP undergoes bone formation and bone remodeling, resulting in IAP regeneration (Figure 9). Wolff’s Law also explains why facet joint regeneration does not occur when the IAPs are completely resected. Tomohiro followed a patient after endoscopic resection of an osteoid osteoma in the cervical facet joint and reported that the patient’s facet joint remodeled following the operation.
24
Another similar case was also reported by Kotheeranurak et al,
25
the author reported that minimally invasive surgery caused less damage to the surrounding structures. We believe that this is also one of the reasons why the IAP can regenerate. The recovery rate after IAP resection is affected by multiple factors. In the present study, we established a multiple linear regression model that demonstrated excellent predictive power for recovery rate after facetectomy, with an adjusted R2 of 0.639. Our findings revealed that facet resection rate, follow-up duration, and age are independent predictors of postoperative recovery, while sex and BMI have no significant independent impact. Notably, IAP resection rate was the strongest negative predictor of recovery rate (β = −0.583, P < 0.001), indicating that a higher extent of facet resection is significantly associated with a lower recovery rate. This finding is clinically meaningful, as excessive facet resection may impair postoperative functional recovery in the long term. Follow-up duration was the strongest positive predictor (β = 0.502, P < 0.001), suggesting that recovery continues to improve over time after facetectomy, which aligns with the natural course of spinal surgery recovery. Comparison of computed tomography images. The red arrow indicates the surgical position where the articular process has been resected.(A) Immediate postoperative image and (B) 30-month postoperative image showing bone regeneration of the IAP
Age was also a significant positive predictor (P = 0.036), indicating that older patients may have a slightly higher recovery rate in this cohort, which may be related to differences in baseline functional status or activity levels. No significant effects were found for sex or BMI, which suggests that these demographic and anthropometric characteristics are not major determinants of recovery after IAP resection.
Kirkaldy–Willis 15 divided the degenerative process of the intervertebral joints into 3 stages: temporary dysfunction, instability, and restabilization. During the restabilization stage, when segmental spinal instability occurs, fibrous tissues and bone spurs form around the posterior facet joints and the intervertebral discs. These fibrous tissues and bone spurs can limit the relative movement between vertebral bodies, enabling the spinal segment to regain stability. The mechanism of segmental stabilization can be better understood via Kirkaldy-Willis’ theory. Although the mechanisms of restoration of segmental stability proposed in this paper are reasonable, it still requires further verification.
Although a decrease in intervertebral disc height may contribute to the restoration of segmental stability, it may also accelerate spinal degeneration. A reduction in disc height can alter the spinal mechanical axis and increase the mechanical stress on adjacent segments, which may theoretically promote degeneration progression. Studies have demonstrated that significant postoperative disc height loss is accompanied by a higher rate of radiographic progression of adjacent segment degeneration (such as changes in disc signal intensity, subchondral marrow signal alterations, and facet joint osteoarthritis). However, no segmental instability was observed, and the overall clinical outcomes remained satisfactory. 23 Additionally, a 5-year follow-up study revealed that progressive segmental degeneration on imaging occurs in both decompressed and adjacent segments after minimally invasive lumbar decompression surgery, with a higher incidence of degeneration in decompressed segments than in adjacent ones. Nevertheless, there was no significant correlation between radiographic degeneration and patients’clinical symptoms, functional scores, or reoperation rates. This suggests that such degeneration is part of the natural course of lumbar degenerative changes rather than a surgery-related factor leading to clinical deterioration. 26
Our study also has several limitations. First, this was a single-center study with a relatively small sample size, which limits the generalizability of our findings. Second, the follow-up time was relatively short to observe long-term instability and whether spinal stenosis occurred earlier. Third, measurements of the volume of the articular process are not accurate enough, and measuring the volume directly via three-dimensional reconstruction with software such as Mimics could be a better option for the precise assessment of facet joint volume. Fourth, the patients’ nutritional status, activity level, compliance with waist brace wearing, and other related factors may introduce bias into the assessment of spinal segmental stability.
Conclusion
In the cohort of this study, patients with >50% IAP resection did not develop radiographic instability, and some showed bone regeneration, though those with complete resection did not regenerate.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Zigong Key Science and Technology Program -Zigong Academy for Medical Big Data and Artificial Joint Intelligence Project (Project No.: 2023-YGY-2–05).
Correction (May 2026):
This article has been updated to include the Study Design in the abstract.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.