
Abstract
Study Design
Retrospective case series.
Objectives
To investigate the influence of screw size on achieving bone fusion in posterior lumbar interbody fusion (PLIF).
Methods
In total, 137 consecutive patients with L4 degenerative spondylolisthesis who underwent single-level PLIF at L4-L5 were evaluated. Factors investigated for their contribution to bone fusion included: 1) age, 2) sex, 3) body mass index, 4) bone mineral density, 5) intervertebral mobility, 6) screw diameter, 7) screw length, 8) screw fitness in the pedicle (%fill), 9) screw depth in the vertebra (%depth), 10) screw angle, 11) facetectomy, 12) crosslink connector, and 13) cage material.
Results
Bone fusion was confirmed in 88.2% of patients. The comparison between fusion (+) and fusion (-) groups showed no significant differences in screw size. The %fill and %length were significantly greater in the fusion (+) group than in the fusion (-) group (%fill: 58.5% ± 7.5% vs 52.3% ± 7.3%, respectively, P = .005; %depth: 59.8% ± 9.7% vs 50.3% ± 13.8%, respectively, P = .025). Multivariate logistic regression analysis revealed that %fill (odds ratio [OR]= 1.11, P = .025) and %depth (OR = 1.09, P = .003) were significant independent factors affecting bone fusion. Receiver operating characteristic curve analyses identified a %fill of 60.0% and a %depth of 54.2% as optimal cutoff values for achieving bone fusion
Conclusions
Screw size should be determined based on the screw fitness in the pedicle (%fill > 60%) and screw insertion depth in the vertebral body (%depth > 54.2%) according to individual vertebral anatomy in L4-L5 PLIF.
Keywords
Introduction
Spinal instrumentation is essential in ensuring spinal stability until biological bone fusion is achieved. The pedicle screw system, specifically, provides rigid fixation and is widely used as the gold standard for spinal fusion. Three major factors affect the fixation of pedicle screws: the bone properties, size and design of the screw, and insertional technique. 1 Among these, screw size selection is 1 of the important factors allowing surgeons to control the fixation. Since a large part of pedicle screw fixation relies on the engagement of the denser bone at the pedicle,2,3 the screw diameter can be reasonably determined based on the pedicle size. Many studies have shown the biomechanical advantages of increasing the screw diameter or screw fitness within the pedicle.4-6
Regarding screw length, several biomechanical studies have shown that the influence of screw length within the vertebral body on the pullout strength was negligible unless screws were placed deep enough to penetrate the anterior vertebral cortex.4,7 Conversely, deeper screw placement has been recommended to reduce the risk of screw loosening and to apply rotational force to the vertebra successfully.6,8,9 In clinical practice, despite the biomechanical advantages of using a longer pedicle screw, the screw length is limited by the anatomical risk of vascular injury anterior to the vertebral body, and the decision on the screw length or insertion depth depends heavily on each surgeon’s experience and preference. Depending on the pathologies, some doctors believe that placing the screw through the pedicle, rather than deep into the vertebral body, is sufficient.
Numerous reports have been published on the effect of screw size on its fixation. However, little is known about its clinical impact, especially on bone fusion, which is the most critical objective of spinal fusion surgery. Surgeons need to know the ideal screw size and how screw size could affect the status of bone fusion for decision-making. In this study, we evaluated the radiological outcomes, focusing on the depth of screw insertion, after single-level posterior lumbar interbody fusion (PLIF), with the aim of investigating the influence of screw size on lumbar spinal fusion and determining the cutoff values to achieve successful bone fusion.
Methods
This study was a retrospective radiological evaluation of prospectively enrolled patients approved by the research ethics committee of the authors’ affiliated institution (ID: 12-10). Written informed consent was not required because all clinical and radiographic interventions followed routine assessment. The study population included 137 consecutive patients with L4 degenerative spondylolisthesis who underwent single-level L4-L5 PLIF performed by board-certificated spine surgeons at our hospital from January 2015 to June 2019. The following were considered indications for spinal fusion: sagittal translation of more than 3 mm or segmental angulation of more than 10° on dynamic radiographs or posterior widening of more than 5° on a flexion radiograph. The exclusion criteria were patients with rheumatoid arthritis, ongoing hemodialysis, metabolic bone disease (except osteoporosis), previous lumbar surgery, and incomplete data. Two patients with postoperative infection were excluded. Of the 135 remaining patients, 119 who were followed up for more than 2 years postoperatively were enrolled (follow-up rate: 88.1%; mean ± standard deviation [SD] follow-up: 42.6 ± 15.1 months). The final study population consisted of 43 male and 76 female patients with a mean ± SD age of 69.3 ± 8.4 years (range: 46-85 years).
Surgical Procedure
Surgical exposure was made through a midline skin incision. Pedicle screws were inserted without bicortical purchase according to the Weinstein method. 2 As a standard procedure, after posterior decompression with partial or total facetectomy and interbody preparation, 2 rectangular interbody cages were placed with local bone harvested during decompression. No posterolateral fusions were performed in any case, and no allograft or bone morphogenetic proteins were used. Lastly, bilateral rods were applied in situ without intentional slip reduction, and compression between the screws was then performed. All patients wore a lumbosacral orthosis for 3 months postoperatively.
Radiological Evaluation
The status of bone fusion was assessed by radiography or CT on the last follow-up. CT was performed at 1 and 2 years postoperatively and thereafter as needed. Bone fusion was determined by confirming the presence of a continuous fusion mass between the vertebral bodies and the absence of motion of the fused segment of more than 3° on dynamic radiographs.10,11 The evaluation was performed twice by a single observer who was not enrolled as a surgeon in this study. Of 119 randomly selected patients, 40 were assessed by 2 independent observers to evaluate the reproducibility.
The influence of the following factors on bone fusion was investigated: 1) age, 2) sex, 3) body mass index (BMI), 4) bone mineral density (BMD), 5) intervertebral mobility, 6) screw diameter, 7) screw length, 8) screw fitness in the pedicle (%fill), 9) screw depth in the vertebra (%depth), 10) screw angle, 11) facetectomy (partial or total), 12) crosslink connector (with or without), and 13) cage material (titanium, titanium-coated polyether-ether-ketone, or polyether-ether-ketone). BMD was measured in Hounsfield units (HU) of each vertebral body using a protocol described by Schreiber et al and the BMD of the L4-L5 vertebrae was averaged.11,12 Intervertebral mobility was determined as sagittal vertebral translation (%) and angulation of L4-L5 segments on preoperative dynamic radiographs. The %fill was defined as the ratio of the outer screw diameter to the narrowest endosteal width of the pedicle in the axial plane.
13
The %depth was defined as the ratio of the screw length within the vertebral body (excluding the screw length outside the vertebra by screw perforation) to the anteroposterior diameter of the vertebral body in the axial plane (Figure 1).
11
The screw angle was defined as the angle between the screw path and the vertebral midline in the axial plane. These measurements were performed based on a postoperative CT image obtained immediately after surgery. Each value was averaged for each patient. Evaluation of screw depth. %depth was defined as the ratio of the screw length within the vertebral body (A) to the anteroposterior length of the vertebral body (B) in the axial plane.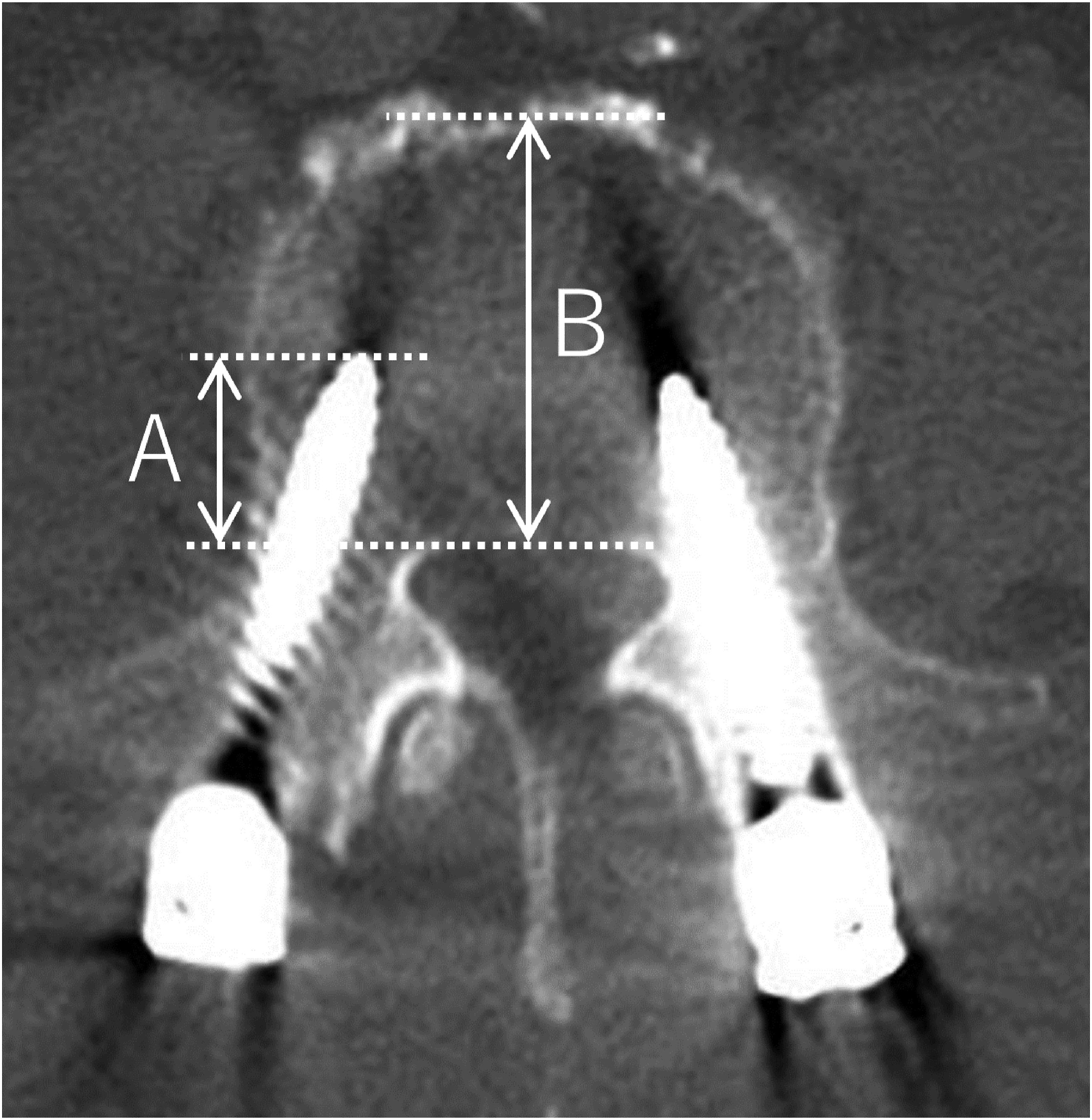
Statistical Analysis
Continuous and categorical variables are presented as the mean ± SD and number, respectively. The kappa coefficient was used to evaluate intraobserver and interobserver reliability in the assessment of bone fusion. To analyze the differences between groups with (+) and without (-) bone fusion, the unpaired t-test and Mann-Whitney U-test were used for continuous variables, while the chi-square test and Fisher’s exact test were used for categorical variables. Multivariate logistic regression analysis was performed using variables with P < .20 in univariate analysis to identify the independent factors affecting bone fusion. Lastly, receiver operating characteristic (ROC) curve analysis was performed to determine the optimal cutoff value for achieving bone fusion. JMP version 14 (SAS, Cary, NC) was used for all analyses, with the significance level set at P < .05.
Results
Univariate Analysis of Bone Fusion.
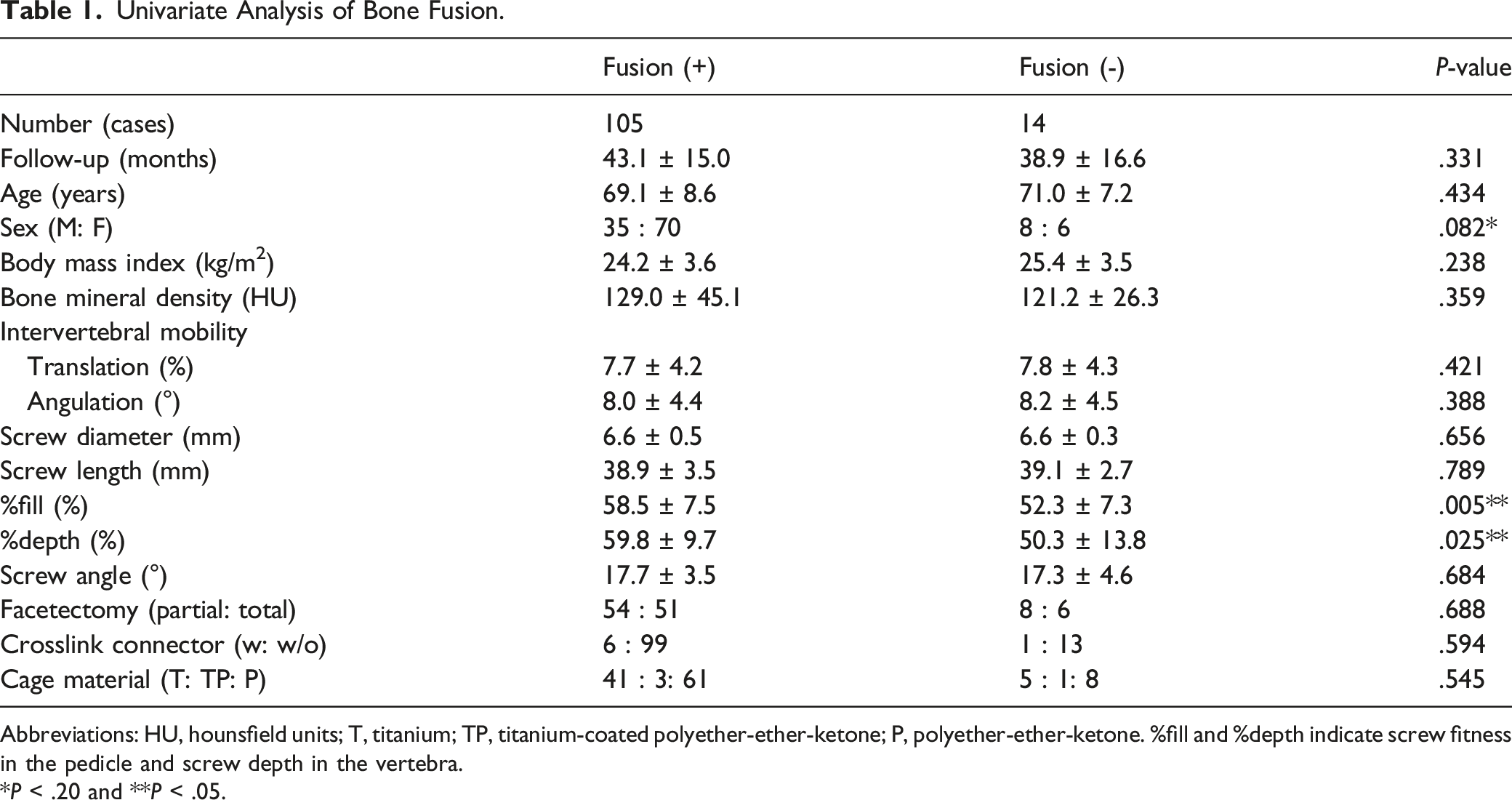
Abbreviations: HU, hounsfield units; T, titanium; TP, titanium-coated polyether-ether-ketone; P, polyether-ether-ketone. %fill and %depth indicate screw fitness in the pedicle and screw depth in the vertebra.
*P < .20 and **P < .05.
Multivariate Logistic Regression Analysis of Bone Fusion.
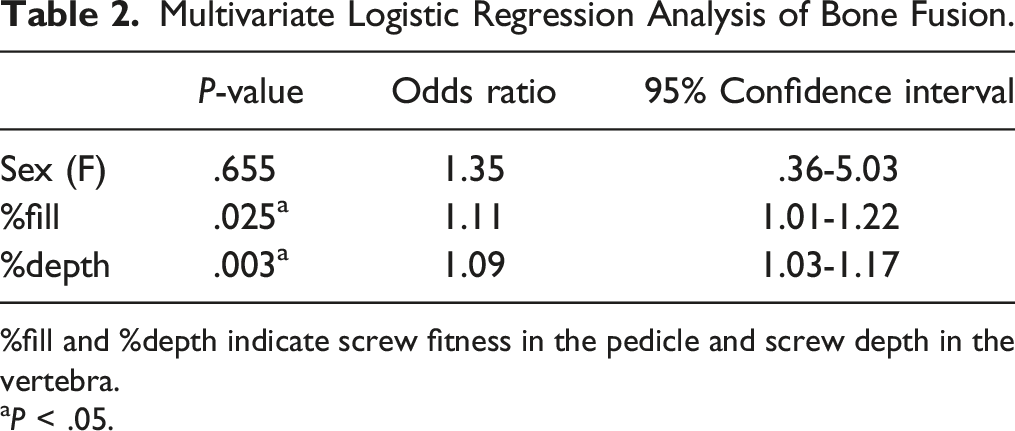
%fill and %depth indicate screw fitness in the pedicle and screw depth in the vertebra.
aP < .05.
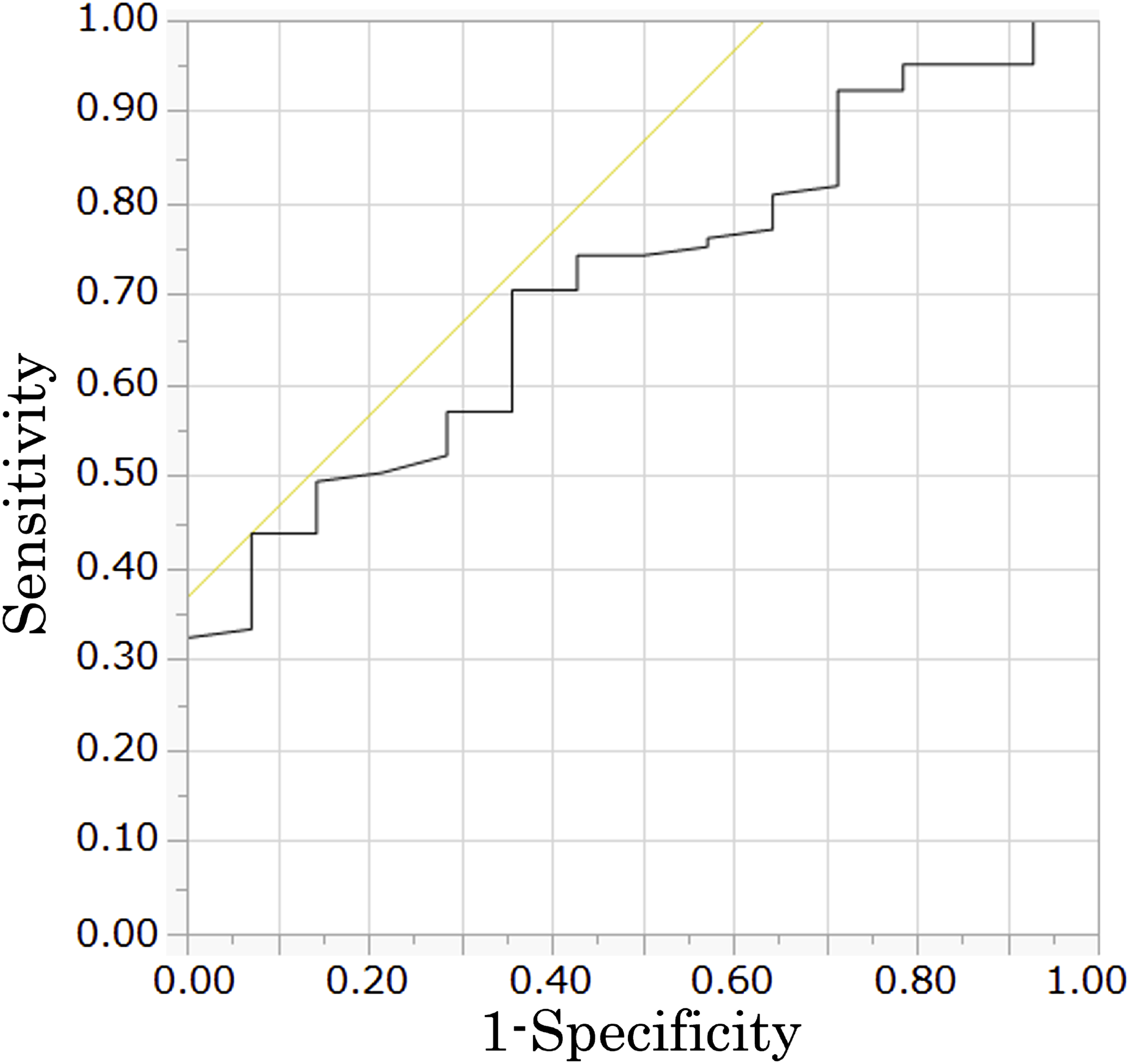
Receiver operating characteristic curve showing the effect of %fill on bone fusion. The area under the curve was .711.
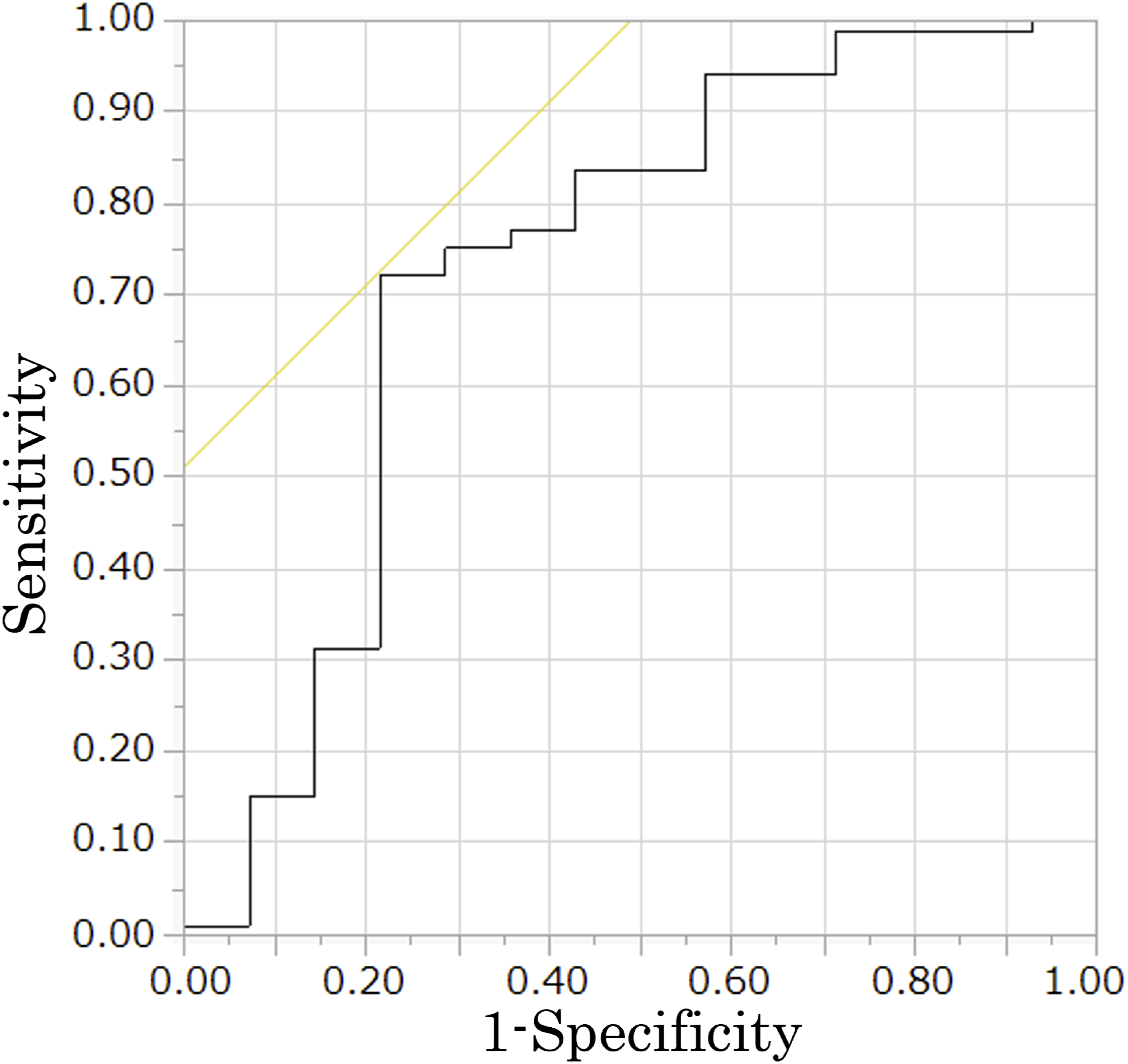
Receiver operating characteristic curve showing the effect of %depth on bone fusion. The area under the curve was .733.
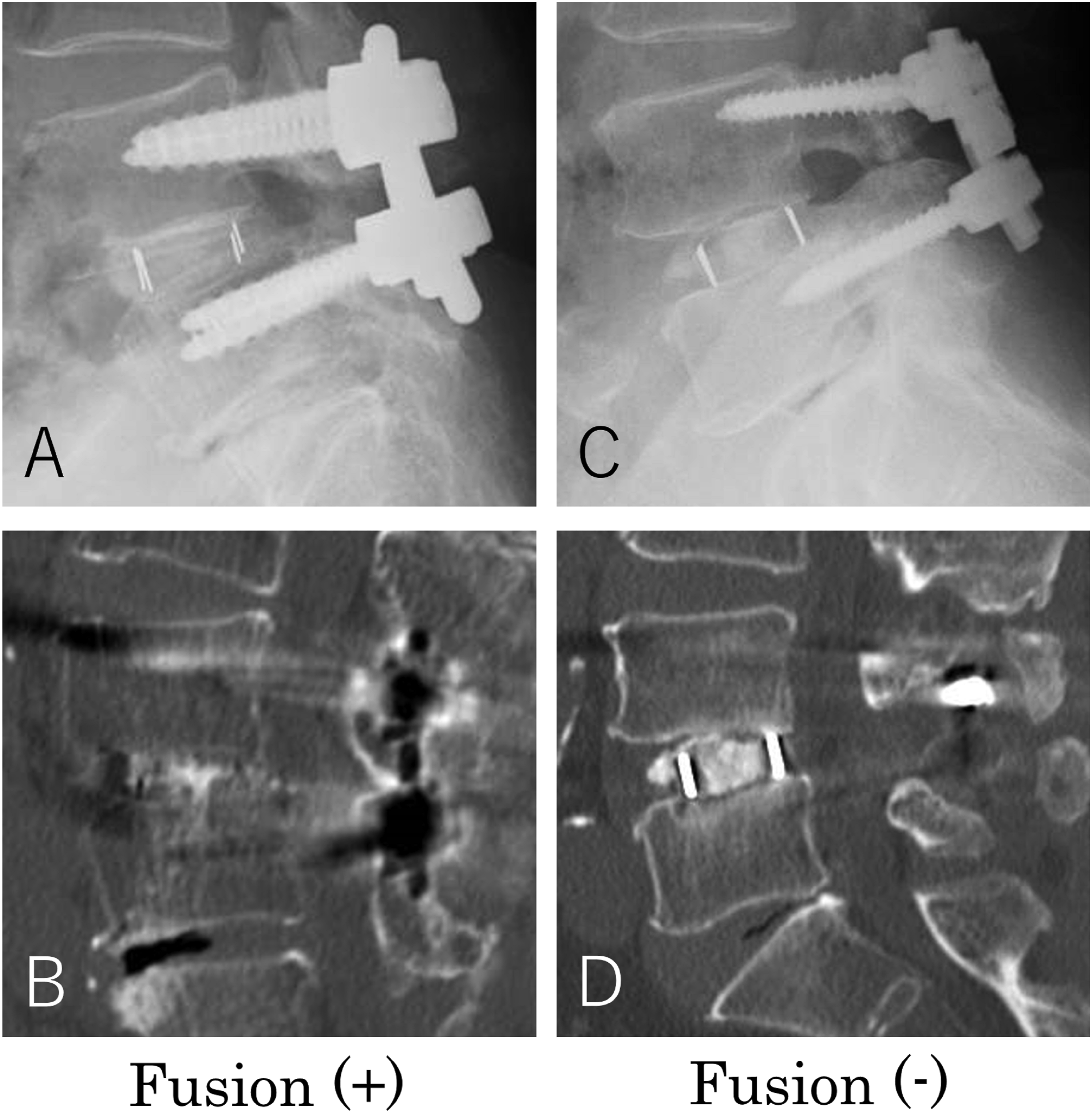
Illustrative cases of the fusion (+) and (-) groups. (A and B) Screw insertion in a 72-year-old female patient at a %depth of 65.0% with bone fusion. (C and D) Screw insertion in a 66-year-old male patient at a %depth of 36.8% with a clear zone around the intervertebral cages.
Discussion
Pedicle screw instrumentation has been fundamental in promoting fusion and early mobilization after posterior spine surgery. While screw size selection could ensure the quality and quantity of bone purchase and fixation, its clinical significance has not been fully elucidated. The present study investigated the impact of pedicle screw size on bone fusion. The cutoff values for achieving bone fusion in L4-L5 PLIF for L4 degenerative spondylolisthesis were 60% screw fitness in the pedicle in the axial plane and approximately 55% screw depth in the vertebral body.
Numerous biomechanical studies have investigated the effect of pedicle screw size on screw fixation.2-8 Fixation depends on the dense structural characteristics of the pedicle,1,3,14 and the pedicle region contributes to 60% of the fixation to resist screw pullout and 80% of torsional stability.2,3 Accordingly, the use of larger diameter screws can achieve contact with the subcortical bone within the pedicle,4-6 which is consistent with the finding that %fill, which indicates screw engagement with peripheral bone in the pedicle, was a significant independent factor affecting bone fusion in the present study. Conversely, longer screws could achieve additional fixation by increasing contact with cancellous bone in the vertebral body, which is an anatomically lower-density region.3,14 Although the effect of screw insertion depth on pullout resistance is limited without penetration of the anterior vertebral cortex,4,7 several studies have reported the significance of the screw insertion depth in the vertebral body on torsional stability. Krag et al 8 showed that screw stability against flexion and torsion loads was increased by 30% by increasing the screw depth from 50% to 80% of the maximum available insertion depth. A unique study by Bezer et al 15 comparing torsional stability between a short divergent bicortical screw and a long convergent monocortical screw demonstrated that the failure load was significantly greater using the long convergent screw, even without bicortical purchase. Notably, in the present study, the screw insertion depth in the vertebral body, rather than the actual screw length, was identified as a factor affecting bone fusion. This may be due to individual differences in the anteroposterior diameter of the vertebral body and screw implantation angle.
Regarding the clinical significance of the screw insertion depth, Liu et al 16 investigated the outcomes of posterior screw fixation with different insertion depths for lumbar vertebral fracture, and revealed that the long screw insertion group (%depth > 80%) showed better radiological and functional improvement compared with the short screw group (%depth < 60%). Similarly, Zhou et al 17 reported that a deeper screw insertion resulted in better spinal balance and better quality of life of patients following single-level PLIF for degenerative spondylolisthesis, although no significant differences were found in the bone fusion rate with different screw insertion depths. Their findings were based on univariate analysis, which differed from the multivariate analysis results of the present study. Furthermore, their patient backgrounds and follow-up periods differed, which contributed to differences with the present study. Although using a different screw trajectory, a recent study most similar to the present study demonstrated the significance of screw insertion depth using the cortical bone trajectory technique in PLIF, with a cutoff value of approximately 40% screw depth in the vertebral body for achieving bone fusion. 11 Theoretically, a deeper screw insertion is expected to increase construct stiffness and facilitate effective load sharing within the vertebra,6,8,18 which could promote bone fusion in the intervertebral space, even in short segmental fusion.
The findings of the present study have practical implications, given the insufficient consensus on a standard method of screw size selection within the safe range for achieving bone fusion. Screw size should be determined based on the screw fitness in the pedicle and screw insertion depth in the vertebral body according to each vertebral anatomy, not uniformly or by surgeon’s preference. Chua et al 19 performed radiological analysis to ascertain the optimal screw length for lumbar pedicle screw placement and recommended that screws should not exceed 80% of the vertebral body length for L2-L4 and 75% for L5 to minimize the risk of anterior cortical breach. From this perspective, the cutoff value of 54.2% for %depth obtained in the present study is thus within an acceptable level of safety. Kot et al also investigated anatomical correlations between lumbar vertebrae and prevertebral arteries and showed that the mean distance between the aorta or common iliac artery and vertebrae at L4/5 level was 2.4-3.2 mm. Although the mean distance reported was shorter than that at higher lumbar levels, this study alerted surgeons regarding surgical safety when placing longer screws. 20 Previous studies that evaluated means of lowering the risk of pedicle fracture reported that the maximum screw diameter should be equal to or +1 mm of the minimum endosteal width of the pedicle isthmus.21,22 The cutoff value of 60.0% for %fill may be considered safe, but care should be taken regarding its interpretation. The endosteal width in this study was measured at the narrowest pedicle width in the axial plane, not at the minimum pedicle diameter in the coronal plane perpendicular to the pedicle axis, which may have caused an overestimation of its true value. Makino et al 23 investigated the morphology of the pedicle structure using multiplanar reconstructed CT and found that the true minimum pedicle diameter was significantly smaller than the transverse pedicle width at the lower lumbar spine because of increased pedicle inclination in the coronal plane. Even with this measurement limitation, most spinal surgeons routinely determine the pedicle screw diameter from the transverse pedicle width in the axial plane. We believe our findings can aid surgeons in determining the appropriate screw size.
The present study has several limitations that should be noted. First, this was a retrospective study of patients from a single institution with a relatively small sample size. Second, we only evaluated the radiological outcomes and excluded the clinical functional outcomes. Controversy remains regarding the relationship between radiological fusion and clinical success; thus, further studies with patient-reported outcomes are needed to elucidate the clinical significance of our findings. Third, the bone fusion status was evaluated at the last follow-up, and the time to achieve fusion was not investigated, which may have affected our conclusions. Fourth, the results were limited to L4-L5 PLIF for L4 degenerative spondylolisthesis. Different parameters may be identified depending on different spinal levels and pathologies. Lastly, because of anatomical limitations, the placement of larger and longer screws is technically demanding. The use of intraoperative fluoroscopy or navigation system may become a valid option for improving screw placement accuracy.
Conclusions
This study focused on the influence of screw size on radiological fusion in L4-L5 PLIF for degenerative spondylolisthesis. Screw size should be determined based on the screw fitness in the pedicle and screw insertion depth in the vertebral body according to individual vertebral anatomy. The cutoff values for achieving bone fusion were 60.0% for screw fitness in the pedicle and 54.2% for screw insertion depth in the vertebral body.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflict of interest with respect to the research, authorship, and/or publication of this article: KM reports personal consulting fee from Medacta outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
IRB approval number: Murayama Medical Center 12-10.