
Abstract
Study Design:
Retrospective cohort study.
Objective:
To examine the effects of concomitant decompression adjacent to the posterior lumbar interbody fusion (PLIF) segment on the clinical and radiological outcomes 5 years after surgery.
Methods:
Forty-five consecutive patients who had undergone L3/4 decompression with L4/5 PLIF for multilevel stenosis with degenerative spondylolisthesis (DS), and were followed for 5 years, were enrolled (group D). As a control group, 45 age-, sex- and preoperative disc height at L3/4–matched patients who had undergone L4/5 PLIF alone for L4/5DS were randomly selected (group A). Disc height, vertebral slippage, range of motion, posterior opening angle, segmental lordotic angle, presence of the intradiscal vacuum phenomenon (IVP) at the L3/4 level were measured on radiographs. Japanese Orthopaedic Association (JOA) score and the requirement for additional L3/4 surgery were evaluated.
Results:
In terms of pre-/postoperative radiographic changes between the groups, significant differences were detected regarding disc height narrowing of ≥3 mm (group D 31%, group A 9%) and IVP (group D 33%, group A 11%). There were no significant differences in other radiological parameters. The recovery rate of the JOA score (group D 58%, group A 61%) and reoperation rate (group D 2.2%, group A 6.7%) were not significantly different between the groups.
Conclusion:
Concomitant decompression adjacent to the PLIF segment accelerated adjacent disc degeneration compared to PLIF alone, but it did not predispose to the development of instability 5 years after surgery. Moreover, the JOA score and reoperation rate were not significantly different between groups D and A.
Keywords
Introduction
With regard to the surgical strategy for degenerative lumbar disorders, lumbar arthrodesis is indicated for pathologies with segmental instability such as degenerative spondylolisthesis (DS), while decompression alone is indicated for those without instability such as lumbar spinal stenosis (LSS). Although LSS adjacent to DS is often observed, surgical treatment for such conditions remains controversial. Some surgeons treat these patients with fusion at the DS segment and decompression alone at the LSS segment. 1 There are many reports of favorable clinical outcomes of posterior lumbar interbody fusion (PLIF) for DS. 2 Nevertheless, fusion surgery imposes increased stress on adjacent levels and increases the risk of adjacent segment disease (ASD). 3 -6 On the other hand, decompression surgery alone is the most conventional approach for LSS. Although good clinical outcomes have been reported, 7,8 some studies have shown that decompression surgery alone increases segmental instability. 9,10 Therefore, when decompression surgery is performed concomitantly adjacent to the PLIF segment, there is concern about progressive degeneration and instability at the decompressed segment.
There are few studies focusing on concomitant decompression adjacent to the PLIF segment. 11,12 Regardless of the time-dependent incidence of ASD, 13,14 these studies did not evaluate radiological changes and clinical outcomes at the same time. Therefore, little is known about the degree of postoperative progression of degeneration and instability for the decompressed segment adjacent to the PLIF. In order to clarify the effect of concomitant decompression adjacent to the PLIF segment, patients with PLIF alone and those with decompression and PLIF were compared. To exclude other factors, the present study was limited to patients who underwent L3/4 decompression with L4/5 PLIF for L3/4 LSS with L4/5 DS as the decompression group, while those with L4/5 PLIF alone for L4/5 DS were the control group. Because there was no postoperative stenosis at the L3/4 level for either group, the difference between these two groups was the partially resected posterior elements adjacent to the PLIF segment. Furthermore, clinical and radiological assessments were examined at the same time, 5 years after primary surgery. The purpose of this study was to examine the effects of concomitant decompression adjacent to the PLIF segment on the clinical and radiological outcomes 5 years after surgery.
Methods
Subjects
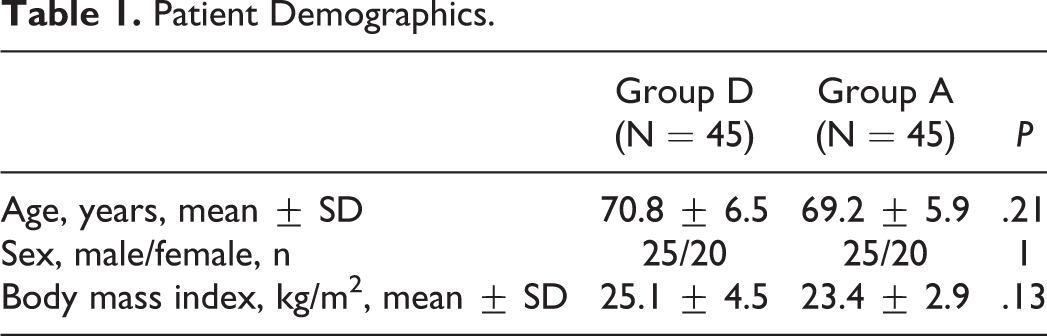
This was a retrospective 1:1 matched case-control study. Forty-five consecutive patients who had undergone L3/4 posterior decompression with L4/5 PLIF for multilevel LSS with DS and were followed for 5 years were enrolled from 2005 to 2011 (group D). The extent of the concomitant posterior decompression at L3/4 was determined by preoperative myelography in all cases. Incomplete block of the myelogram at the L3/4 level in the standing or extended position was considered an indication for concomitant posterior decompression. On the other hand, 109 consecutive patients (38 men, 71 women) had undergone L4/5 PLIF alone for L4 DS in the same period. As a control group, 45 age-, sex-, and preoperative disc height at L3/4–matched patients who were followed for 5 years, were randomly selected (group A). The exclusion criteria were the presence of tumor, infection, destructive spondyloarthropathy, scoliosis (Cobb angle >20°) and previous lumbar surgery. The mean age at the time of primary surgery was 70.8 years (range, 54-86 years) in group D and 69.2 years (range, 56-82 years) in group A. Each group consisted of 25 men and 20 women (Table 1).
Patient Demographics.
Surgical Procedures
All procedures were performed using a technique described elsewhere for PLIF. 15 Briefly, bilateral total facetectomy, subtotal discectomy, and local autologous bone grafting with 2 carbon cages were performed. In terms of posterior decompression at the adjacent segment, the supra- and interspinous ligaments on the caudal side of the spinous process at the L3/4 segment were first removed. Partial laminotomy, flavectomy, and bilateral medial facetectomies up to the pedicle were then performed in a trumpet manner. Complete laminectomy was not performed in any patient.
Radiological Evaluations
Disc height, vertebral slippage, range of motion (ROM) of the disc angle, posterior opening angle, segmental lordotic angle, the presence of the intradiscal vacuum phenomenon (IVP) at the L3/4 level, and lumbar lordosis at L1-S were measured on lateral radiographs (Figure 1A). The disc height was measured using the method reported by Miyakoshi et al. 16 For the disc angle, a lordotic position is indicated by a positive value. For slippage, anterior slippage is indicated by a positive value. Additionally, lateral slippage and the wedging angle at the L3/4 level were measured the anterior-posterior radiographs (Figure 1B). Radiological changes were evaluated before and 5 years after surgery or just before revision surgery. Radiographic instability was defined as a new posterior opening of ≥5° on the flexion lateral radiograph, and a slippage of ≥3 mm compared with the preoperative radiograph.
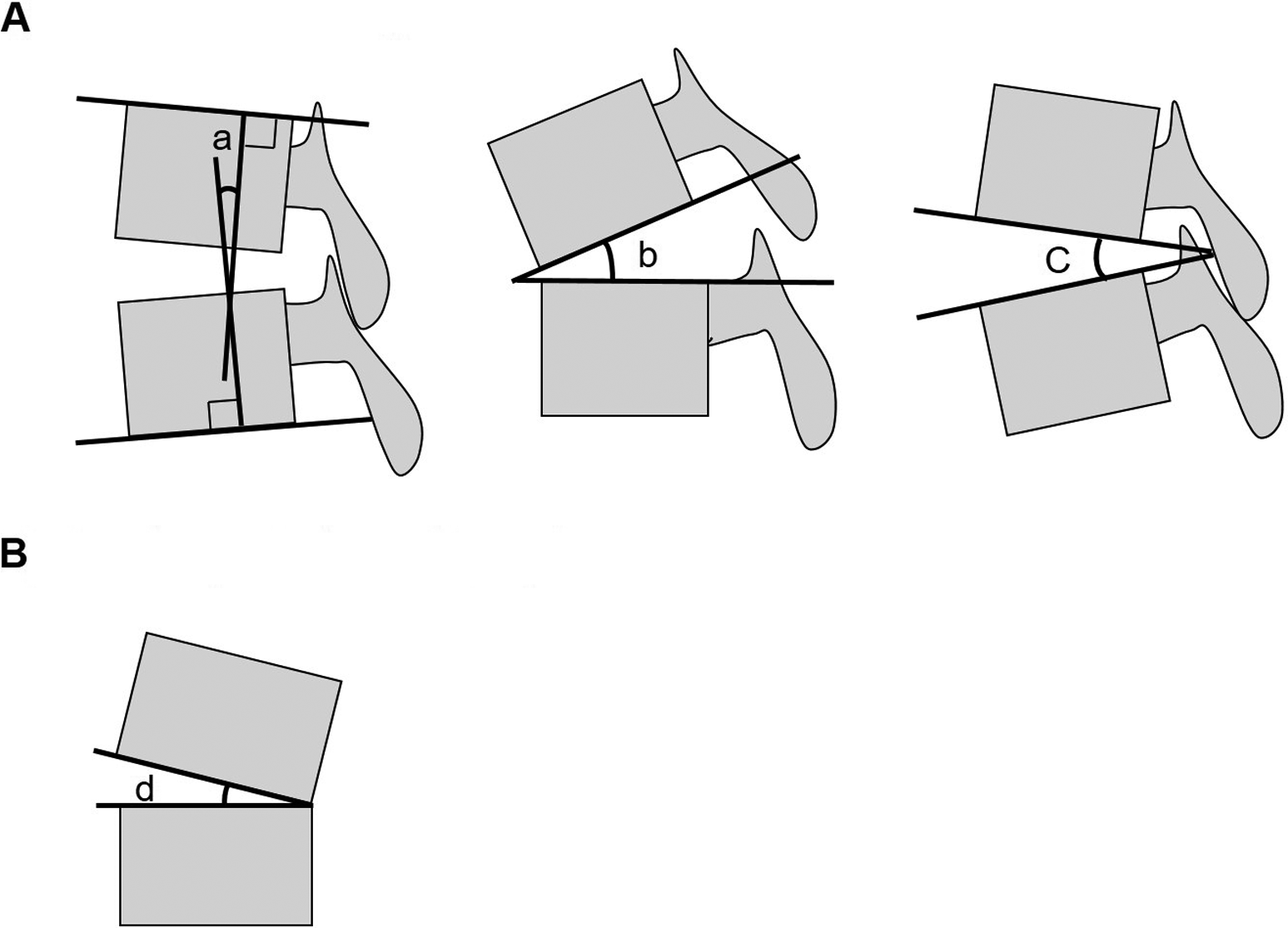
The scheme of angle parameters in radiographs. (A) Lateral radiographs. Segmental lordotic angle was measured by neutral lateral radiograph (a). Posterior opening angle of the disc was measured by maximum flexion radiograph (b). Range of motion (ROM) of the disc angle was measured by maximum flexion and extension lateral radiographs (difference between b and c). Lordosis was calculated as positive value. (B) Anterior-posterior radiograph. Disc wedging was measured by antero-posterior radiograph (d).
Clinical Evaluations
In terms of clinical outcomes, the Japanese Orthopaedic Association (JOA) score and the requirement for additional L3/4 surgery were evaluated. The JOA score consists of 4 categories and has a maximum score of 29 points (Table 2). 17 The low back pain (LBP) score of the JOA score ranges from 0 to 3 points (none, 0; occasionally mild, 1; always mild or occasionally severe, 2; always severe, 3). The recovery rate (%) of the JOA score was calculated as follows: (postoperative JOA score − preoperative JOA score) / (29 − preoperative JOA score) × 100. The JOA score was determined before surgery and 5 years after surgery or just before revision surgery. With regard to the need for additional L3/4 surgery, the rate of revision surgery at the L3/4 level was calculated.
Summary of the Japanese Orthopaedic Association (JOA) Scoring System.a
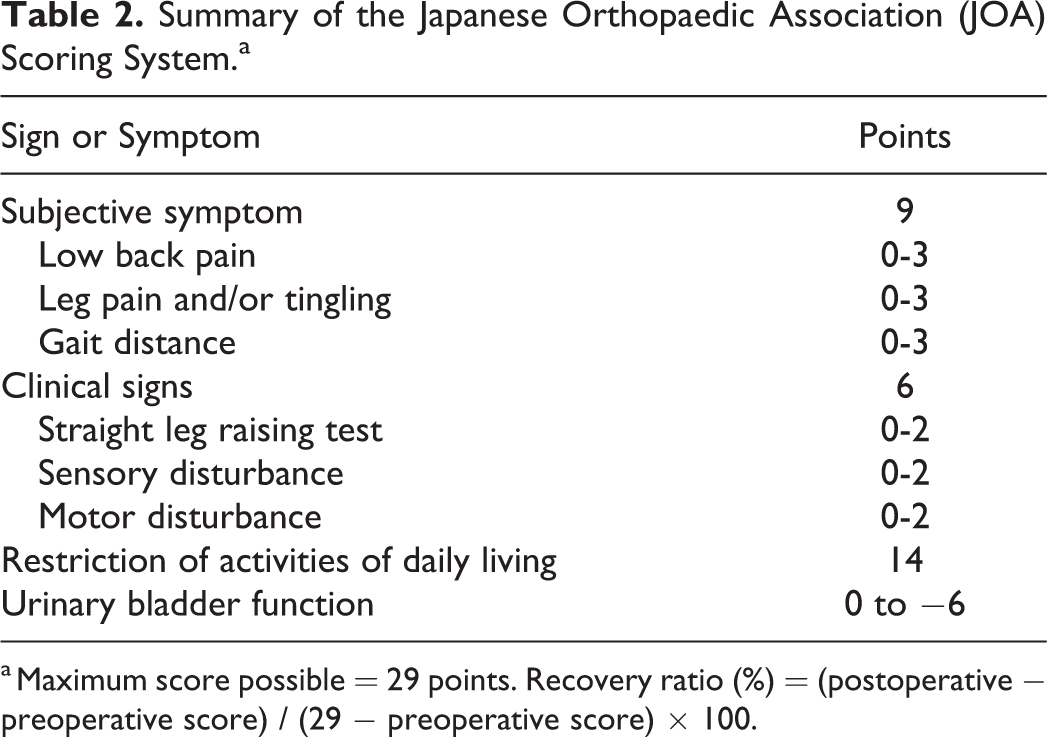
a Maximum score possible = 29 points. Recovery ratio (%) = (postoperative − preoperative score) / (29 − preoperative score) × 100.
To examine the relationship between radiological parameters and clinical outcomes, the recovery rate and the JOA LBP score 5 years after surgery were compared based on the parameters of significant differences.
Statistical Analysis
Radiological factors and clinical outcomes were compared between the 2 groups and within the groups using Student’s t test or the Mann-Whitney U test for continuous variables, and the chi-square test for categorical variables. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 21 (IBM Corp). A P value of <.05 was considered significant.
Results
Radiological Evaluations
Comparison of Preoperative Radiographic Parameters Between the Groups
Although there was a significant difference in preoperative lateral slip, no significant differences were found in other preoperative radiological parameters (Table 3).
Preoperative Radiographic Parameters in Group D and Group A.
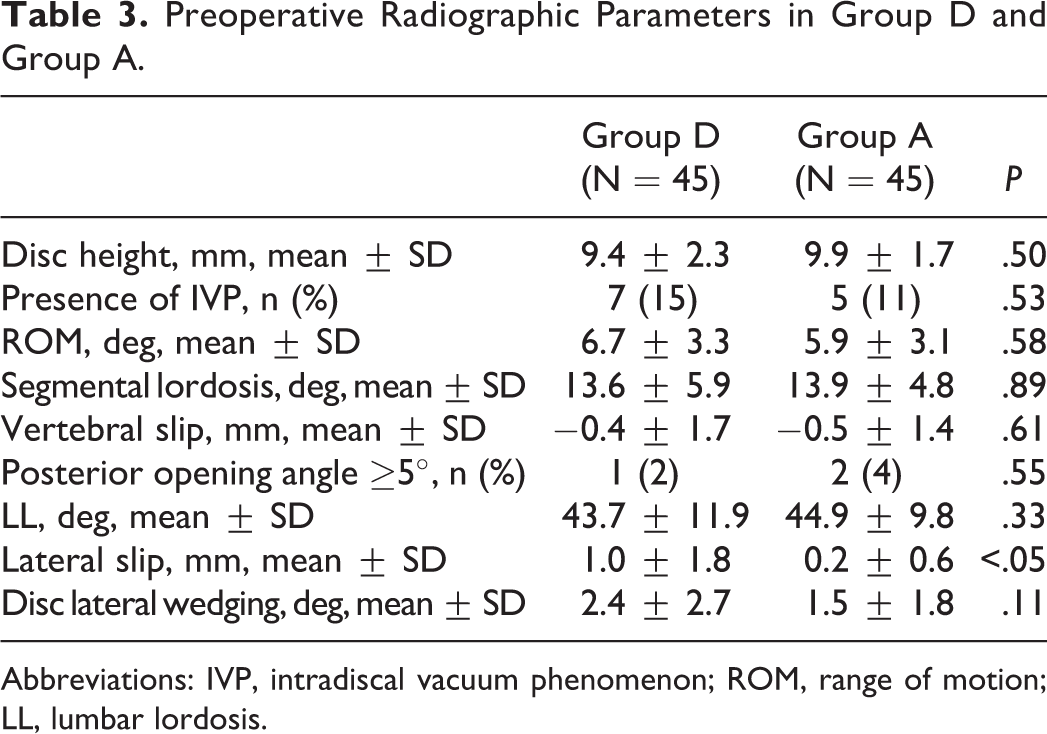
Abbreviations: IVP, intradiscal vacuum phenomenon; ROM, range of motion; LL, lumbar lordosis.
Comparison of Pre- and Postoperative Radiographic Parameters in Group D
Pre-/postoperative radiological parameters in group D are shown in Table 4. Significant differences were observed in disc height (9.4 mm/7.4 mm) and presence of IVP (7 cases 15%/22 cases 49%; P < .01). There were no significant differences in other radiological parameters.
Pre- and Postoperative Radiographic Parameters in Group D.
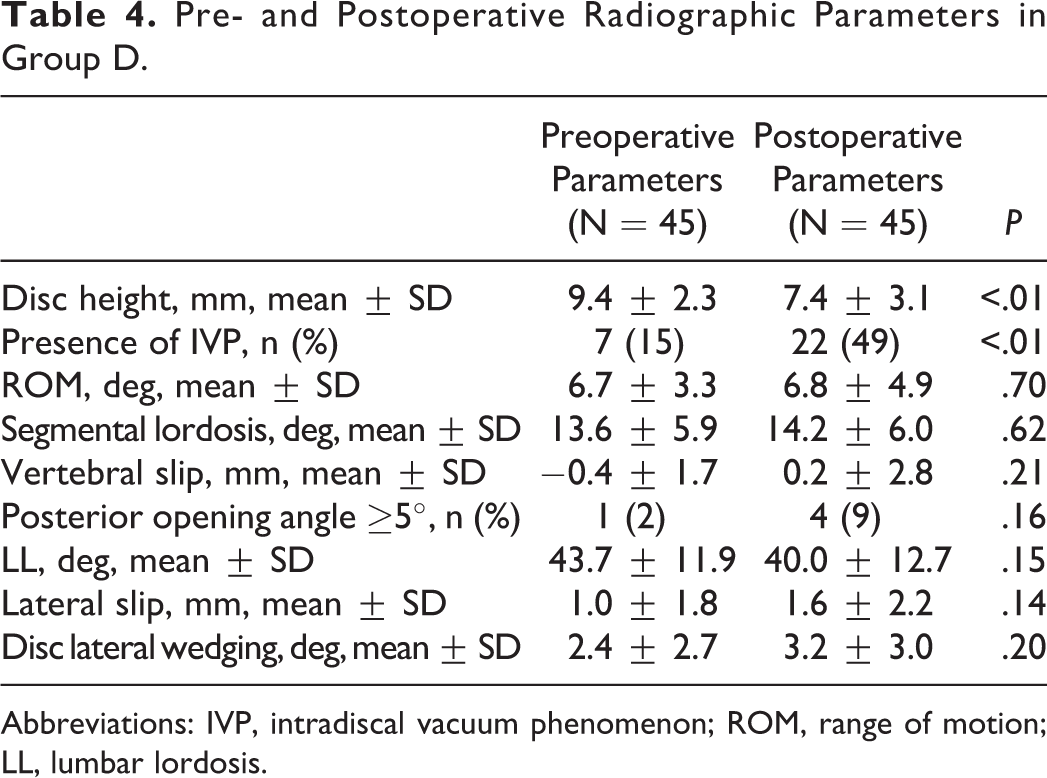
Abbreviations: IVP, intradiscal vacuum phenomenon; ROM, range of motion; LL, lumbar lordosis.
Comparison of Pre- and Postoperative Radiographic Parameters in Group A
Pre-/postoperative radiological parameters in group A are shown in Table 5. An obvious difference was detected in disc height (9.9 mm/9.0 mm) (P < .05). There were no significant differences in other radiological parameters.
Pre- and Postoperative Radiographic Parameters in Group A.
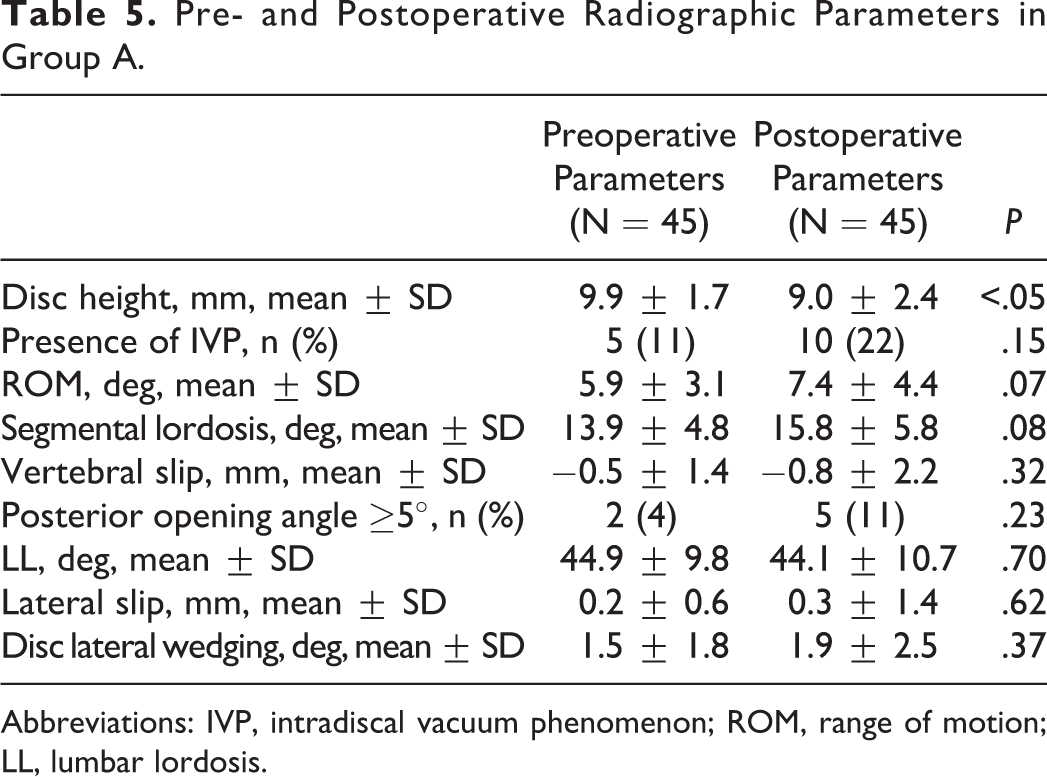
Abbreviations: IVP, intradiscal vacuum phenomenon; ROM, range of motion; LL, lumbar lordosis.
Comparison of Pre- and Postoperative Radiographic Changes Between the Groups
Significant differences were detected for disc height narrowing of ≥3 mm (group D 31%, group A 9%) and IVP (group D 33%, group A 11%). There were no significant differences in other parameters between the groups (Table 6).
Change in Pre- and Postoperative Radiographic Parameters in Group D and Group A.
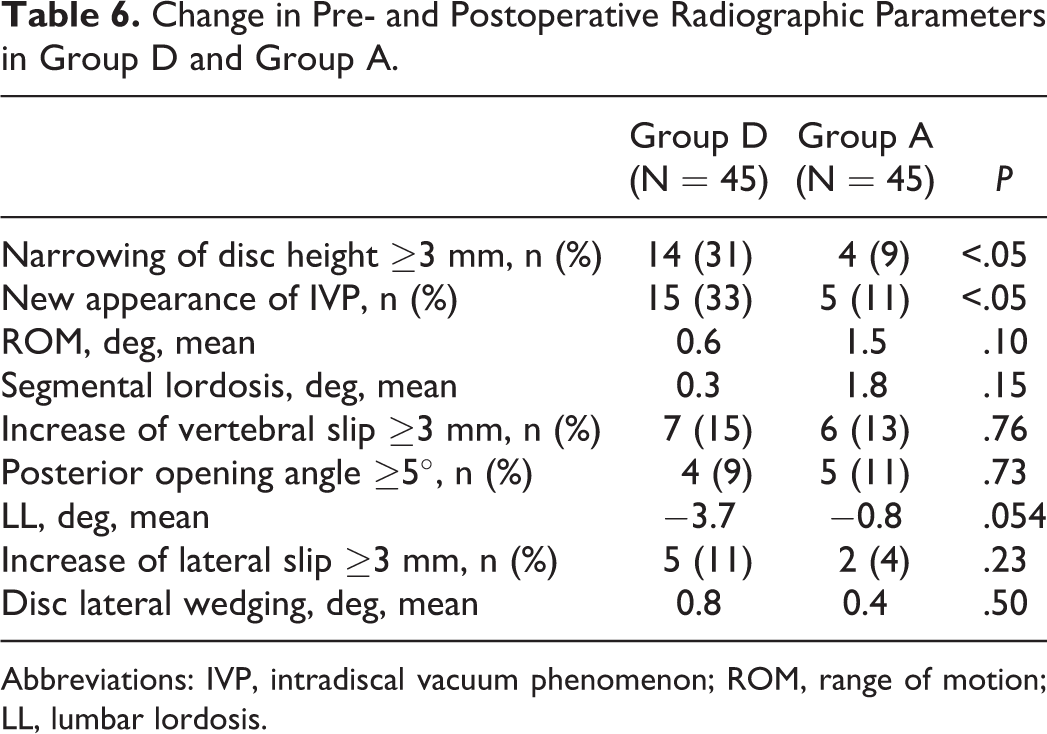
Abbreviations: IVP, intradiscal vacuum phenomenon; ROM, range of motion; LL, lumbar lordosis.
Clinical Evaluations
Preoperative average JOA scores were 11.2 ± 3.8 (range 4-19) in group D and 12.9 ± 3.8 (range 1-21) in group A. Preoperative JOA scores tended to be lower for patients in group D than in group A (P = .03). Five years after surgery or just before revision surgery evaluation, the mean JOA score was 21.7 ± 5.2 (range 1-28) for patients in group D and 22.7 ± 4.2 (range 11-28) for those in group A (P = .36) (Figure 2), and the recovery rate was 58.0% ± 28% for patients in group D and 61.4% ± 25% for those in group A (P = .63) (Figure 3).
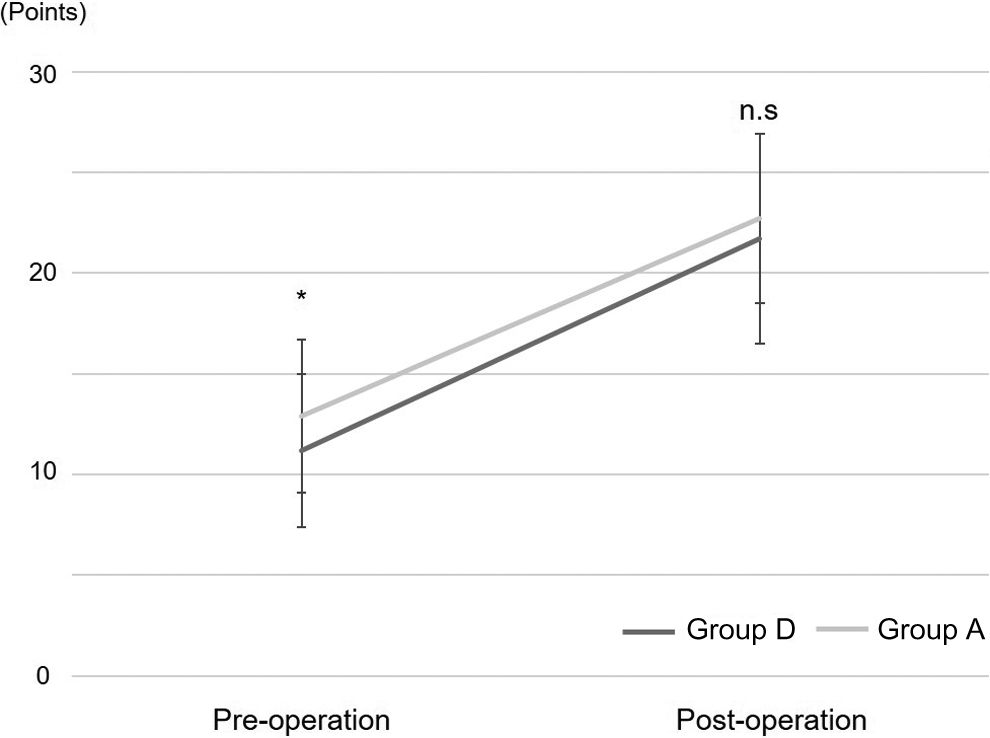
JOA scores in both groups. Preoperative JOA scores are significantly lower in group D than in group A. There is no significant difference between group D and group A in JOA scores 5 years after surgery. *P < .05. Values represent means ± SD. n.s., not significant. JOA, Japanese Orthopaedic Association.
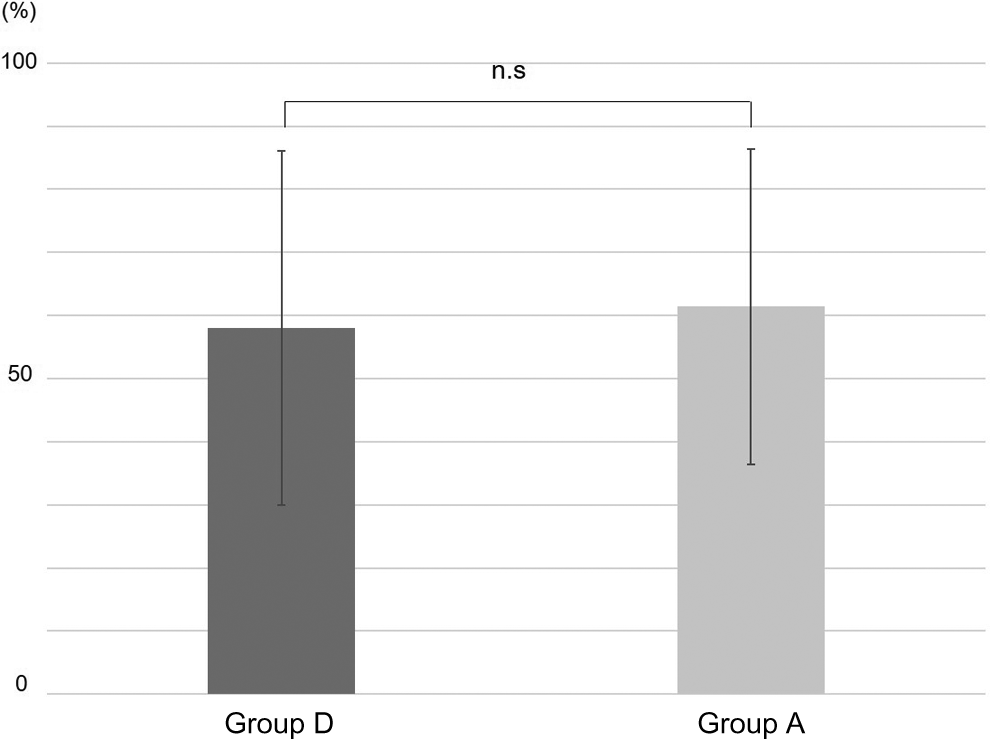
Recovery rate of JOA scores. There is no significant difference between group D and group A in the JOA score recovery rate. Values represent means ±SD. n.s., not significant. JOA, Japanese Orthopaedic Association.
The reoperation rate at the L3/4 level was 2.2% (1 of 45) in group D and 6.7% (3 of 45) in group A (P = .30). The pathologies requiring reoperation were a facet cyst in group D and LSS (2 cases) and DS (1 case) in group A.
Narrowing of the disc height by ≥3 mm was observed in 18 of 90 patients (20%), while 72 of 90 patients (80%) had no disc narrowing (<3 mm). IVP was observed in 32 of 90 patients (36%), while 58 of 90 patients (64%) had no IVP. The recovery rates were 54.7% ± 33% in patients with disc narrowing and 60.9% ± 24% in those without disc narrowing (P = .37). The LBP score was 2.2 ± 0.6 points in patients with disc narrowing and 2.3 ± 0.6 points in those without disc narrowing (P = .51). The recovery rates were 55.4% ± 30% in patients with IVP and 62.2% ± 24% in those without IVP (P = .26). The LBP score was 2.3 ± 0.6 points in patients with IVP and 2.4 ± 0.6 points in those without IVP (P = .62). The recovery rate and LBP score showed no significant differences between groups.
Discussion
To the best of our knowledge, the present study is the first to compare the effects on the clinical and radiological outcomes of concomitant adjacent segment decompression to PLIF and those of PLIF alone at the same level and in the same period. This study showed that concomitant adjacent segment decompression to PLIF caused a predisposition to radiological ASD, especially disc degeneration, but did not cause radiological instability and subsequent symptomatic conditions.
With regard to ASD after PLIF, various risk factors have been reported. 18 -20 Some authors reported that concomitant decompression was one of the risk factors for ASD after PLIF. 3,11,12 Hikata et al 11 demonstrated that simultaneous decompression surgery was a significant factor related to radiological ASD and did not reduce the incidence of symptomatic ASD. Miyagi et al 12 also reported that symptomatic ASD occurred frequently in association with total laminectomy to the adjacent PLIF segment. Furthermore, Lai et al 21 showed that damaging the integrity of the posterior complex between the fused segments and the neighboring motion segments may jeopardize lumbar spine stability. 21 Sacrificing either the supraspinous ligament or the tendon insertion points on the spinous processes leads to accelerated development of adjacent instability. In the present study, concomitant adjacent segment decompression to PLIF caused a predisposition to disc degeneration, but not radiological instability, similar to the report by Hikata et al. 11 Furthermore, concomitant decompression did not affect the clinical outcomes, including the reoperation rate.
There is little evidence on which to base the surgical strategy for multilevel stenosis with DS. Smorgick et al 1 reviewed 207 patients for multilevel stenosis with single-level DS and compared the surgical outcomes of multilevel decompression with single-level fusion and multilevel decompression with multilevel fusion. They reported that there was no significant difference in surgical outcomes between the 2 surgical treatments, although operative time and intraoperative blood loss were significantly higher in the multiple fusion group. Moreover, multiple segment fusion may impose an increased stress on adjacent segments and increase the risk of ASD. 22,23 Park et al 24 demonstrated that patients with multilevel stenosis and DS showed worse outcomes than those with single-level stenosis with DS. Interestingly, in the present study, despite the fact that preoperative JOA scores were lower for patients with multilevel stenosis than for those with single-level stenosis, there were no significant differences in postoperative JOA scores or the recovery rate of JOA between the 2 groups. Hence, these results suggested that concomitant adjacent segment decompression to PLIF may be an effective operative method for multilevel LSS with DS.
The present study showed no significant relationship between clinical outcomes and disc space narrowing or IVP. However, several studies reported that disc degeneration, especially disc space narrowing, was strongly associated with LBP. 25,26 Moreover, IVP has been reported to be associated with degenerative disc disease and endplate changes, 27,28 and furthermore, Morishita et al 29 demonstrated the relationship between IVP and LBP. 29 On the other hand, Imagama et al 30 suggested that soft stabilization may be an option for prevention of degeneration at a decompressed adjacent segment. Therefore, when decompression surgery is performed concomitantly adjacent to the PLIF segment, in order to prevent the progression of disc degeneration and to improve clinical outcomes, the surgical technique of decompression should be considered, preserving the posterior complex of the adjacent segment as much as possible, as in bilateral decompression via a unilateral approach. These less invasive decompression surgeries preserving posterior components might prevent radiological degeneration.
There are several limitations in the present study. First, it was a retrospective review of a small number of patients. Second, the preoperative stenotic condition at the adjacent segment was different in the control group from that in the concomitant posterior decompression group. To clarify whether it is necessary to perform concomitant decompression at the adjacent segment to PLIF, a randomized, controlled trial for almost the same multilevel stenosis with DS would be ideal. However, it is realistically very difficult to select patients who have almost the same stenotic condition at the adjacent segment to PLIF. Further prospective longitudinal studies are needed to identify the proper operative methods for patients with multilevel stenosis with DS.
Conclusions
In conclusion, concomitant decompression adjacent to the PLIF segment accelerated adjacent disc degeneration compared to PLIF alone, but it did not cause a predisposition to the development of instability 5 years after surgery. Moreover, the JOA score and reoperation rate were not significantly different between groups D and A. Hence, these results suggest that concomitant decompression adjacent to the PLIF segment may be an effective operative method for multilevel stenosis with DS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.