
Abstract
Study Design
Cadaveric specimens.
Objective
To perform a pathomorphological analysis of the degree of facet joint (FJ) degeneration utilizing fresh cadaveric models and correlating these structural changes with imaging findings.
Methods
L1-L5 FSU including all tissue between the anterior longitudinal ligament to the posterior spinal structures were obtained on 28 patients at a mean of 5.7 hours post-mortem. The samples were fixed in an agar medium and CT and MRI were performed. The level of FJ degeneration was identified based on prior classifications Osteoarthritis Research Society International (OARSI), as was the facet angle and tropism. Pathomorphological assessment including articular cartilage cell density was performed according to prior established methodology.
Results
Radiographically, a direct association was identified between FJ degeneration and patient age. Facet angle and tropism did not significantly vary by patient age. Pathomorphologically, there was a decrease in the cellular density of articular cartilage with increasing patient age. Similarly, there was a significant direct correlation between radiographic degree of degenerative changes in FJs with the age of cadavers and the degree of degeneration of FJs according to the morphological classification of OARSI, as well as a significant inverse correlation with cell density.
Conclusion
A comprehensive assessment of various signs of FJ degeneration using cadaveric material has established that, based on radiographic imaging, it is possible to assess the microstructural state of FJ, including at an early stage of the disease. This data may be useful for surgeons in guiding therapeutic strategies based on individual biometric parameters of the FJ.
Keywords
Introduction
The facet joints (FJ) of the lumbar spine ensure provide structural stability, allow for motion, and aid in correct spatial configuration of the spine. 1 Previously, biomechanical studies have established that increases in axial load and lateral bending results in the greatest stress at the lower lumbar FJ (L4-L5, L5-S1), resulting in higher degeneration rates. Whereas the upper lumbar FJs (L1-L2, L2-L3) even with increased amplitudes of movements in the functional spinal unit (FSU) tend to remain intact.2,3
It has previously been established that degenerative diseases of the FJ along with other spondylotic pathology such as disc degeneration/herniation and spondylolisthesis may be a cause of low back pain, which could limit daily physical activity and quality of life.3,4 While nonoperative management such as physical therapy, injections (eg facet blocks), and adjunct anesthetic techniques (eg denervation, facetoplasty) may be effective in some, ultimately some patients require formal decompression, facetectomies, and spinal instrumentation.2,5 The type and volume of surgical treatment is influenced on the patient’s presenting symptoms as well as on the degree of the surgeon’s proficiency in surgical techniques.6-8
Structural changes to the FJ can be assessed with pathomorphological analysis, which in prior studies has primarily been limited to samples obtained from surgical pathology.9,10 Therefore, this analysis is limited to patients who are deemed to meet surgical indications and excludes the remainder of the pathological spectrum. Cadaveric specimens may be more appropriate to fully assess the morphological spectrum of the FJ at various stages of the degenerative cascade. 8 The association between pathomorphological FJ changes and imaging findings including X-ray (XR), computed tomography (CT, and magnetic resonance imaging (MRI) has not been clearly elucidated.11,12
Many of the developed XR and MRI-based classifications of the degrees of degeneration of the intervertebral discs (IVDs) and FJs have no histological confirmation.13-15 A frequently utilized CT-based classification was developed by Pathria et al 16 and expounded upon by Fujiwara et al 17 in an MRI-based classification that grades facet joint (FJ) osteoarthritis on a four-point scale with grade 1 corresponding to a normal joint, grade 2 with mild joint space narrowing/osteophytes, grade 3 with moderate sclerosis/osteophytes, and grade 4 with severe ankylosis and osteophyte burden. Other important radiographical parameters to consider include facet angle and tropism. Pathomorphological analysis is based upon the Osteoarthritis Research Society International (OARSI) classification and assess cell density of articular cartilage. 18
Given the dearth of studies linking pathomorphogical analysis of the FJ with imaging findings, the purpose of this current study was to perform a pathomorphological analysis of the degree of FJ degeneration utilizing fresh cadaveric models and correlate these findings with imaging findings.
Materials and Methods
Study Design
Analysis of cadaver material from 28 corpses (comprising 112 FSU) was carried out. The study was approved by the Ethical Committee of the Irkutsk State Medical University (Protocol #1 of November 28, 2015). Informed consent was not required, they have been deemed exempt from requirement. Specimens were collected from January 2016 to December 2020. Corpses are obtained in a sequential, random manner, regardless of age, gender, cause of death, etc. The causes of death included ischemic heart disease (N = 9), mechanical asphyxia (N = 7), alcoholic cardiomyopathy (N = 5), ethyl alcohol poisoning (N = 4), and poisoning with narcotic substances (N = 3). Patients who suffered severe spinal trauma, had prior lumbar spinal surgery, history of systemic chemotherapy or localized radiotherapy, or had history of inflammatory arthropathy (eg ankylosing spondylitis) were excluded from this current study. The mean duration from time of death to collection of specimens was 5.7 hours (interquartile range 3.7 - 8.1 hours).
The FSU obtained were isolated at the level of the upper edge of the vertebral body at L1 and the lower edge of the vertebral body at L5. This was due to the anatomical difficulties and the need for resection of the sacral bone connected to the pelvic ring. In addition, aesthetic reasons associated with significant aggression to the tissues of the corpse and accompanied cosmesis were a limitation to the removal of the lumbosacral junction of the spine. The extracted FSUs included the vertebral bodies with preservation of the anterior and posterior longitudinal ligaments, adjacent IVDs, endplates, and FJs. The sampling of the material was carried out no later than 12 hours after death and a complex morpho-instrumental analysis–within the first day.
Outcomes Study
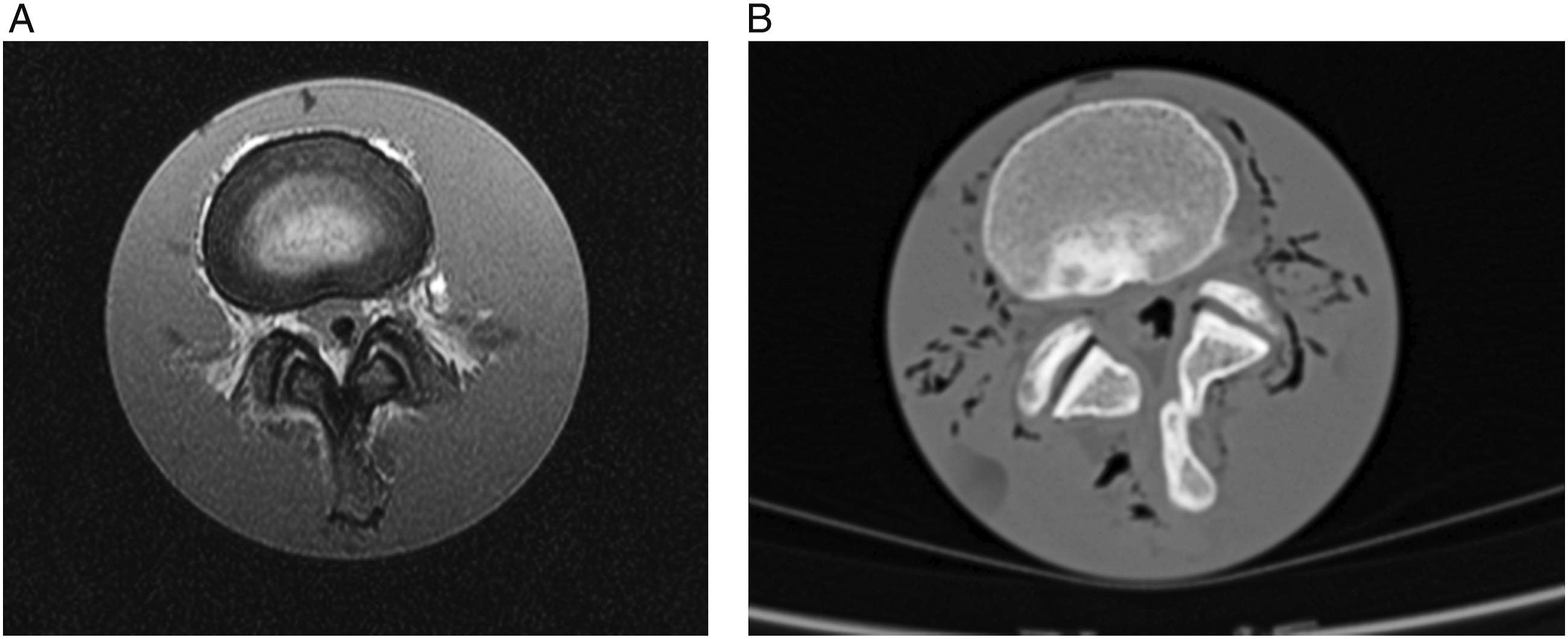
The FSU was placed in a thermocontainer with saline solution at room temperature for delivery to the laboratory. Then it was placed into a plastic container for its complete filling with .8% agar (Bargus Production; Russia) in a vertical position. The models of FSU with agar were subjected to radiographic assessment using MRI and CT (Figure 1), after which, FSUs were removed from the container for subsequent morphometric analysis of FJs using a binocular magnifier with preservation of the integrity of the articular space. The severity of degenerative changes in the FJ was classified according to the classification of Fujiwara A. et al [17] on a 1.5 T MRI device (Siemens Magnetom; Essenza, Germany) (Figure 2). The value of the facet angle and tropism of the FJ was assessed according to a methodology previously established by Karacan et al
19
using CT scan (Philips Brilliance CT 64-slice apparatus; Netherlands) using the RadiAnt DICOM Viewer program. On axial CT scans, the facet angle is formed by the intersection of a line drawn through the middle of the articular space of the facet joint for each side, and a line drawn through the center of the IVD and the spinous process. Facet joint tropism is defined as a difference of greater than 10° between the right and left facet angles (Figure 2). Extracted cadaver material of the lumbar spine (male 39 years old): (a) – sagittal MRI; (b) - sagittal CT. Neuroimaging images of the cadaver Functional spinal unit L3-L4 (male 32 years old) on: (a) – axial MRI (degree of degeneration according to Fujiwara A. classification, grade II for both FJ). (b) – axial CT (right facet angle 44.1°, left facet angle - 46.0°, no FJ tropism).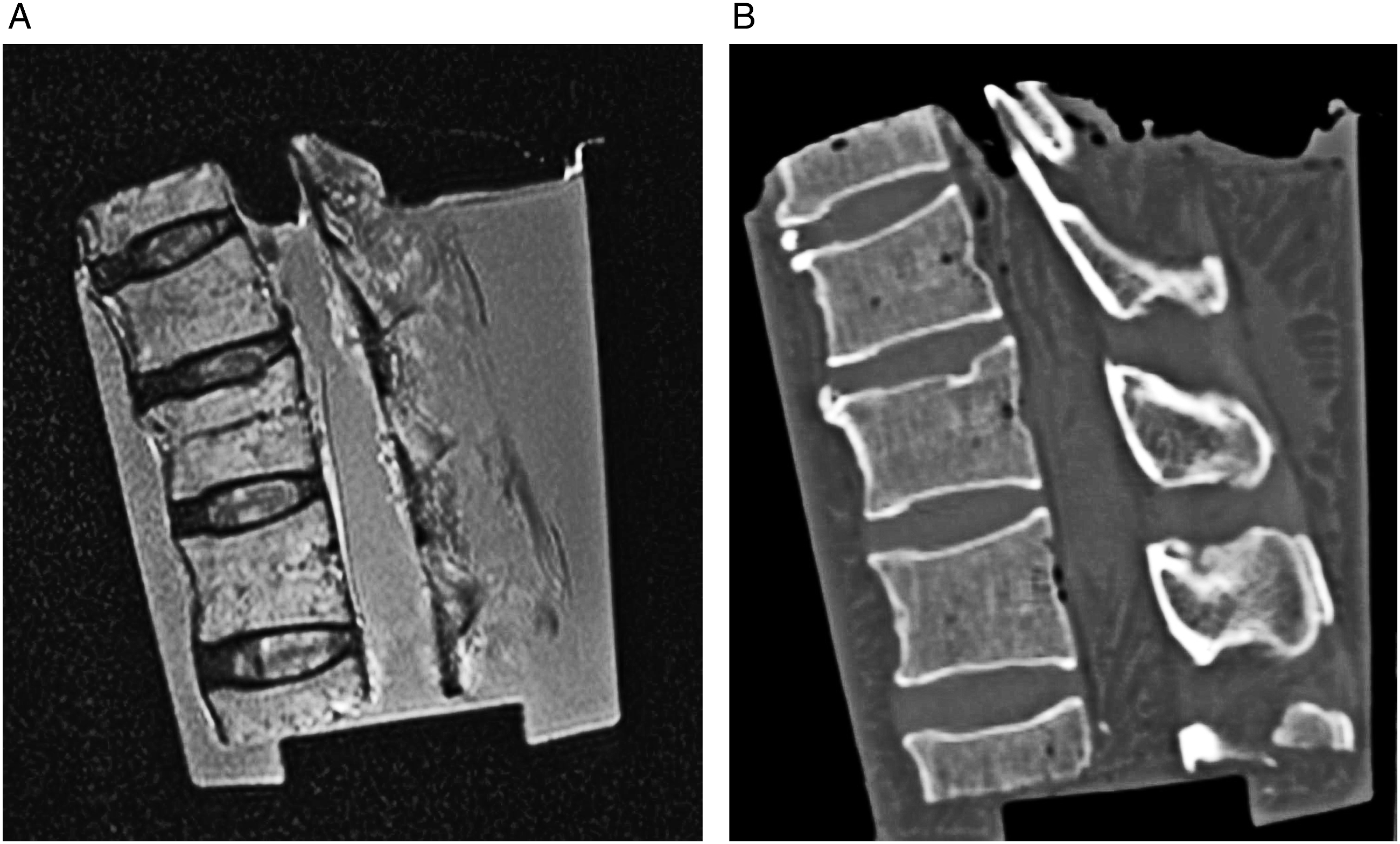
Cadaver FJ for morphological studies was fixed in a buffered 10% solution of neutral formalin in a VIP-E150F machine from Sacura (Japan) and poured into TEC-IV paraffin by (Sacura; Japan). Cutting of standard serial sections with a thickness of 3-5 μm was carried out on semi-automatic rotary microtomes (Microm CM-502; Walldorf, Germany). The preparations were dewaxed in a Clear Rite 3 solution (Thermo Fisher; Waltham, Massachusetts), then in alcohols 100, 95, 90, and 70%. The preparations were stained with Mayer's hematoxylin solution (Biovitrum, Stockholm, Sweden) for 4 minutes. At the last stage, the preparations were embedded in Fluoromount Aqueous Medium (F4680, Sigma Aldrich; St Louis, Missouri) and a cover glass was mounted on top. Pathomorophological analysis was performed by assessing cell density in articular cartilage using high-powered microscopy at 400x magnification (Carl Zeiss Eye Mag ProS binocular magnifier; Oberkochen, Germany) and cell density (cells/mm3) was quantified using the Automatic Cell Counting Java Image J software. The degree of FJ degeneration in histological examination was graded according to the morphological classification of Osteoarthritis Research Society International, OARSI (Figure 3).
18
Histological section of the left FJ (woman, 42 years old), stained with hematoxylin-eosin, magnification 120: (a) – joint space; (b) – hyaline cartilage containing homogeneous accumulations of chondrocytes. The histological picture is typical for stage II degeneration according to the OARSI classification.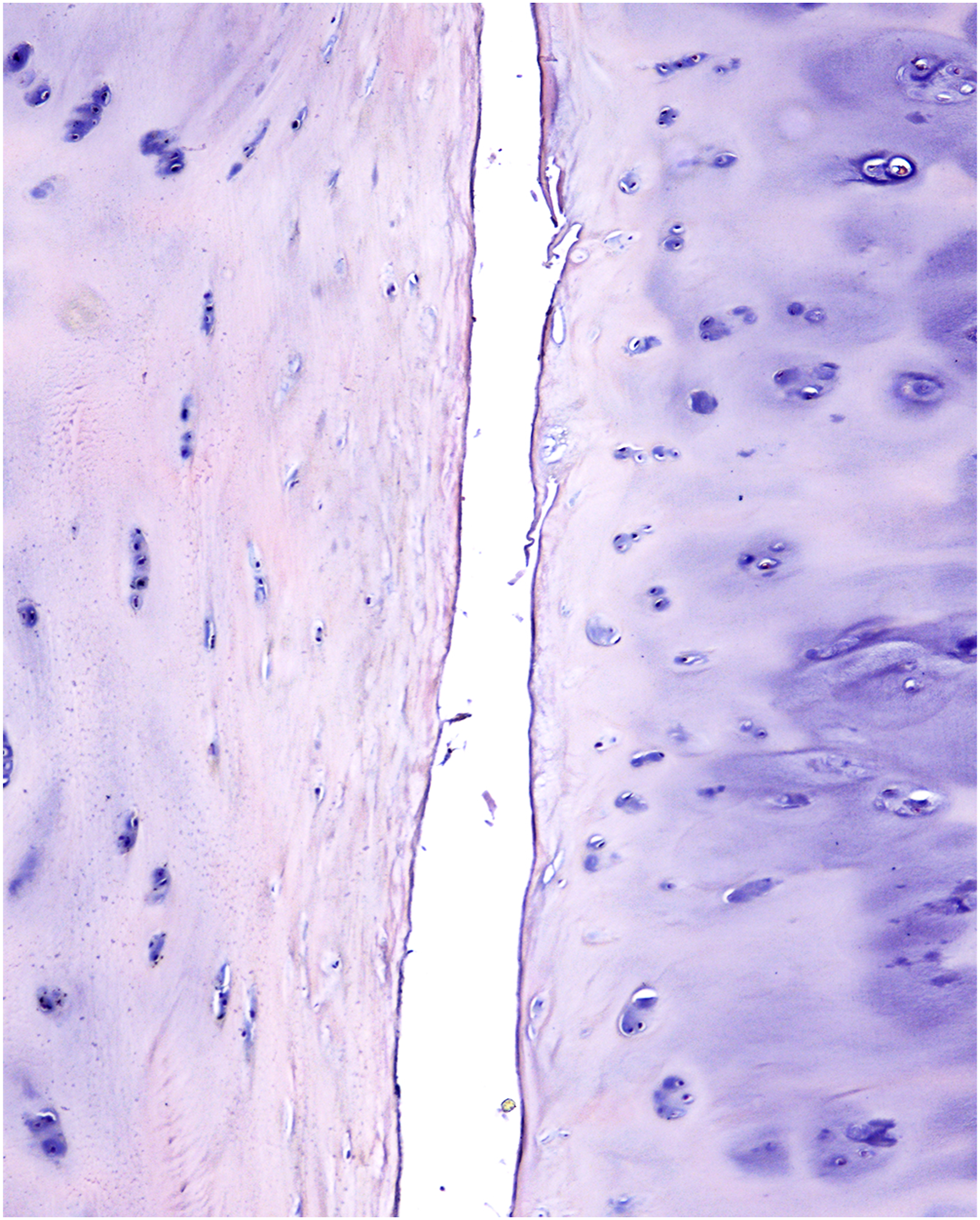
Statistical Analysis
Statistical analysis was carried out using Microsoft Excel and Statistica 8.0 software. The distribution pattern was identified utilizing the Shapiro-Wilk, Kolmogorov-Smirnov, and Lil'efors tests. Considering the presence of significant differences according to these tests (P < .05), the distribution was considered to be different from normal. Comparison of continuous variables in the groups of respondents was performed using one-way ANOVA as amended by Bonferroni. Comparison of categorical variables in all of the scoring systems was performed using a Kruskal–Wallis test. A P-value less than .05 was considered significant. Correlation analysis was carried out using Spearman's rank correlation coefficient.
Results
The study included 112 FSUs from 28 cadavers (18 males and 10 females), the mean age was 57 (IQR 47-72.5) years. The FSUs models are assigned to 4 age groups according to WHO (World Health Organization) 20 : from 18 to 44 years old (young age, N = 6), from 45 to 59 years old (middle age, N = 9), from 60 to 74 years (elderly age, N = 7), and from 75 to 90 years (senile age, N = 6).
Radiographic Assessment
Distribution of cadaveric material depending on the individual parameters of the degree of degeneration of the FJ according to the classification of Fujiwara A. and the values of the facet angles.
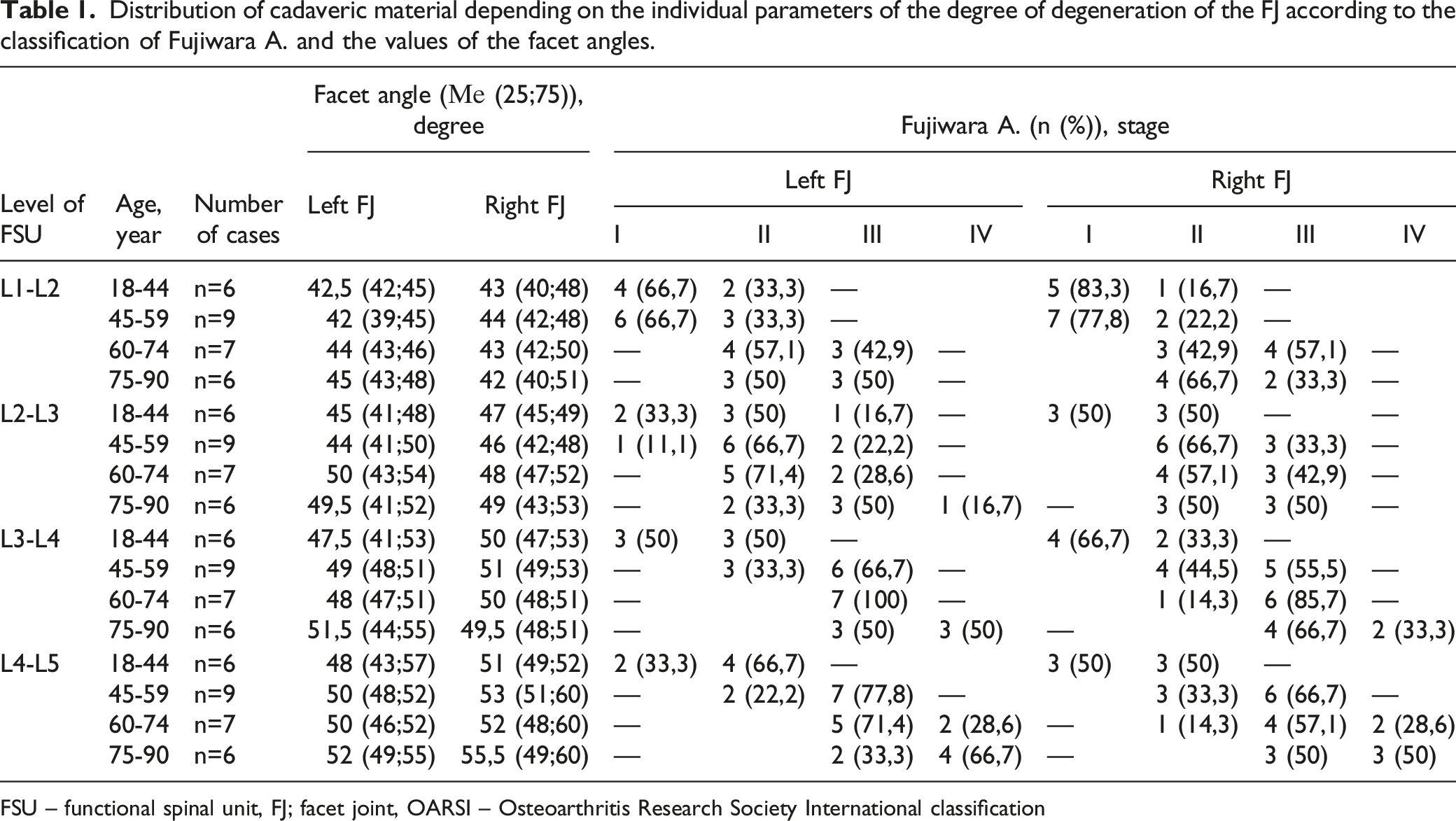
FSU – functional spinal unit, FJ; facet joint, OARSI – Osteoarthritis Research Society International classification
Pathomorphological Assessment
Distribution of cadaveric material depending on the individual parameters of the degree of degeneration of the FJ according to OARSI and the value of the cell density of the articular cartilage
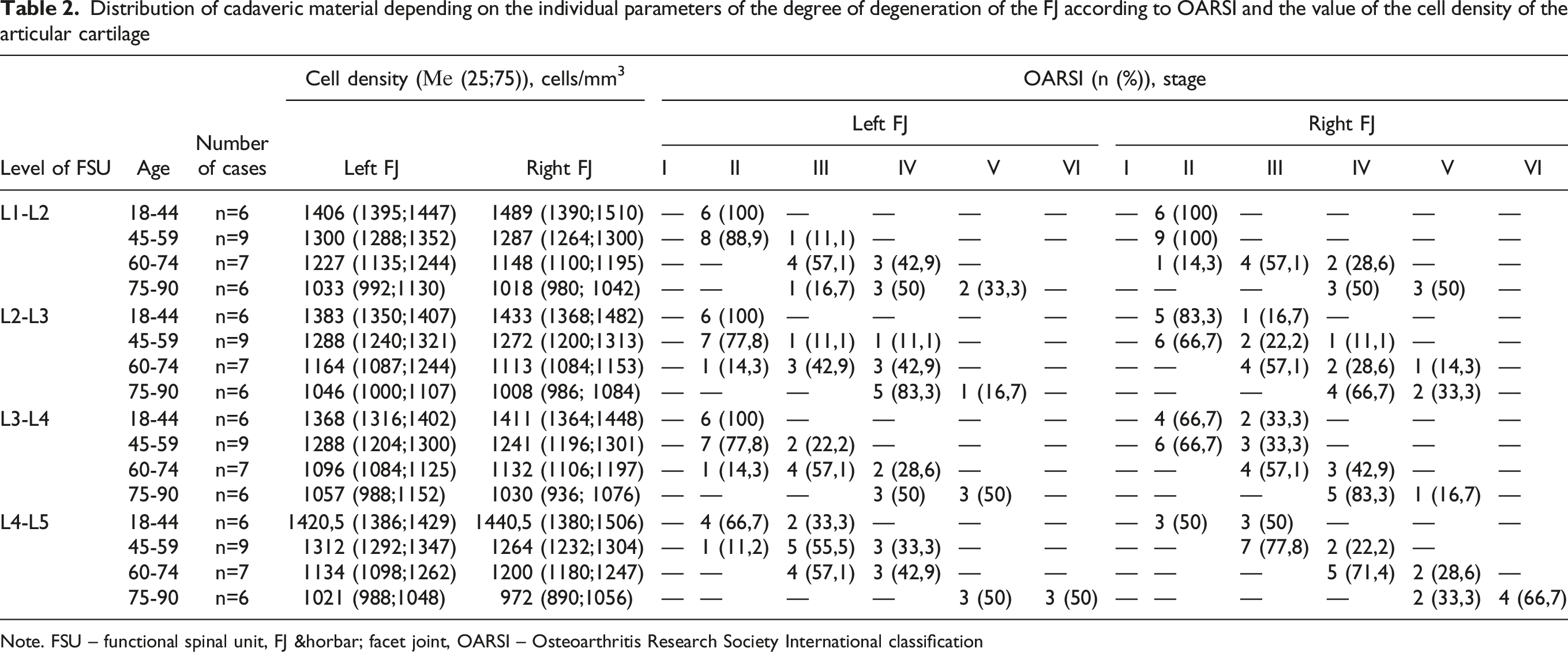
Note. FSU – functional spinal unit, FJ ― facet joint, OARSI – Osteoarthritis Research Society International classification
Radiographic and Pathomorphological Correlation
Correlation of the degree of degenerative changes in FJ according to Fujiwara A. with the analyzed morphological and radiographic characteristics of FJ
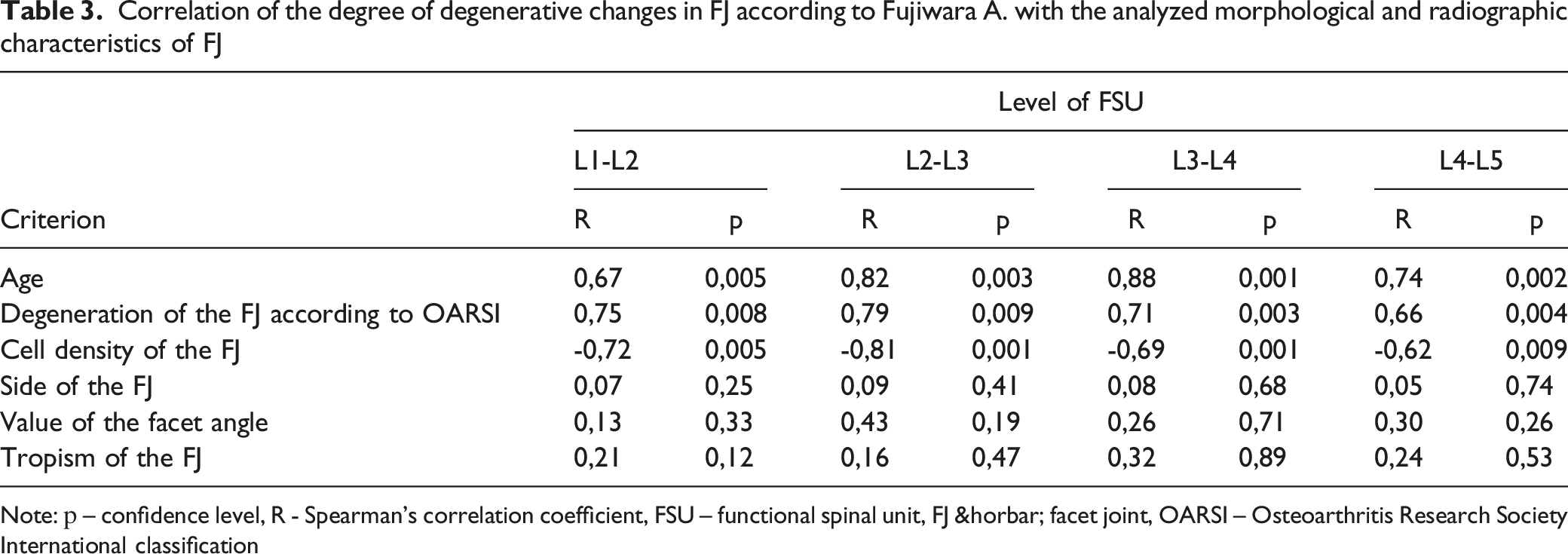
Note: р – confidence level, R - Spearman's correlation coefficient, FSU – functional spinal unit, FJ ― facet joint, OARSI – Osteoarthritis Research Society International classification
Discussion
In cases of failed nonoperative management or absolute indications for surgery in lumbar spondylosis, precise understanding of the degenerative and functional states of the FJ is important for choosing the type of surgical procedure. For example, in order to determine the need for wide decompression, facetectomies, and instrumented spinal fusion vs a simple decompression or disc arthroplasty with preservation of the posterior support complex, 1 needs to have a comprehensive understanding of all of the spinal elements.2,10 Accurately identifying the degenerative state of the FJ in terms of morphological structure and pathology may aid in the implementation of patient-specific treatment strategies.9,14 We therefore undertook this analysis to determine the pathomorphological findings associated with FJ degeneration and to correlate these findings with imaging findings
In the current study utilizing cadaveric specimens, we found that the degree of FJ degeneration seen on MRI, according to the Fujiwara classification, has a direct correlation with the severity of FJ changes according to the OARSI morphological classification and the patient's age, as well as an inverse correlation with the cellular density of the articular cartilage. To our knowledge, this is the first study to correlate FJ degeneration seen on MRIs with the microstructural architecture. Cadaveric studies also make it possible to examine the findings at the initial stage of FJ degeneration, when the collection of surgical material for histological confirmation from patients is not readily available.
Duan et al 21 measured the subchondral bone thickness of lumbar FJ using MRI and CT imaging in 81 patients with a mean age of 37 years. The authors stratified patients based on the presence of symptoms and were assigned to 2 groups, symptomatic or non-symptomatic. The data were compared with cadaver material (n = 12). The authors found that vertebral body subchondral bone hypertrophy was identified in patients with chronic back pain and was recorded mainly in the lower lumbar segments. The results obtained indicate that the thickening of the subchondral bone occurs with an increase in the load on the FSU. Connecting anterior spondylotic changes with posteror FJ degeneration, Alpaycı et al 22 assessed the relationship of FJs degeneration according to the classification of Pathria et al 16 with the classification of changes in the MR signal of the endplates of the vertebral bodies according to Modic 23 . The study involved 120 respondents with a mean age was 55.18 ± 9.47 years. Four groups of 30 people representative by sex and age were stratified by Modic endplate change type (no changes, type 1, type 2, type 3). As a result, the authors found that the degree of FJs degeneration increased with the degree of endplate changes according to the Modic classification.
Zhou et al 24 conducted a study on 42 patients to assess the correlation between the degree of FJs degeneration according to the classification of Pathria et al 16 and Grogan et al 25 with the data from preoperative radiographic methods of examination (MRI, CT). After performing a medial facetectomy, the material obtained was stained with hematoxylin-eosin and toluidine blue .5%, followed by histological examination. As a result, the authors obtained a positive correlation between the histological examination data and radiographic examination methods. In addition, the study found that the MRI examination is more informative than the assessment of the severity of the FJ degeneration compared to CT data. However, this study was limited to only surgical specimens.
Finally, Cui et al 14 studied the morphological and instrumental data of 42 lower articular processes of the lumbar FJs obtained from 29 patients aged 65 (41-84) years during the dorsal decompression and stabilization intervention. The degree of IVD degeneration was assessed by MRI based on the classification of Prirrmann C. et al 26 , as well as FJs by CT based on the classification of Pathria M. et al 16 and by MRI based on the Weishaupt D. classification et al 27 ; the facet angle was studied using the Noren R. method. et al 28 ; the tropism of FJs was studied by applying method of Vanharanta H. et al 29 ; morphological analysis was carried out after decalcification with subsequent staining of the preparations with safranin. The authors established a correlation between FJs tropism and IVD degeneration by MRI (.346 (pъ = .033)), as well as histological assessment of FJs with FJs degeneration by CT - .317 (P = .031) and MRI - .557 (P < .001). No correlation was found between FJs tropism and its degeneration, FJs and IVD degeneration according to the results of radiographic, histological examination of FJs and IVD degeneration by MRI.
Limitations
In the studied groups, a limited number of cadaveric FSU was assessed for each age group, which may make some of our subgroup analyses underpowered. Additionally, we did not analyze the lumbosacral FJ. In the study and comparative analysis of FJ by age groups, the influence of environmental factors and the anthropometric characteristics of the deceased were not taken into account. In addition, a significant limitation of the present study was the absence of pathological analysis of other anatomical elements of the FSU causing neurological symptoms, for example, ligamentum flavum, IVD, size of the intervertebral foramen, etc. Also, the study did not take into account the possibility of the influence of a magnetic field and computer radiation on postmortem changes in the FJs. Additionally, in this study, the MRI and histological classifications were done by a unique rater. Finally, the data may be too fragmented into small groups (age, side, levels), which can lead to a multiple comparisons problem.
Potential Clinical Relevance
This basic science study has potential for laying the groundwork for future studies and clinical applications. By correlating the cellular findings with radiological studies, 1 can non-invasively determine the status of the FJ. Based on the correlation between the MR images of facet joints and their microstructural state confirmed in our study, future studies may further elucidate the required amount of surgical correction that results in better clinical outcomes. For example, after verification of isolated facet syndrome and minimal severity of FJ degeneration according to MRI results in young patients, injections of hyaluronic acid 30 or PRP therapy 31 and platelet rich plasma has been reported. In the presence of isolated facet syndrome in elderly patients caused by significant lumbar spondyloarthrosis with MRI demonstrating pronounced morpho-structural degradation of articular cartilage, it may be appropriate to use radiofrequency ablation 32 .
The results of this study may be useful in choosing a method of treatment for lumbar degenerative conditions, taking into account the severity of changes in the FJ and the associated clinical symptoms, which can be confirmed by facet blockade 33 and / or disc puncture 34 provocative tests. The relevance of the results obtained is due to the high frequency of registration of back pain associated with arthropathy of the lumbar spine in patients both at a young age and in the older age group 33 . Our study is relevant in that back pain can often be due to facet arthropathy of the lumbar spine in both the young and older age groups. It has been established that symptomatic lumbar spondyloarthrosis typically begins in the third decade of life, with the frequency steadily increasing with age along with the progression of degenerative changes in the posterior support complex. 35 Determining the optimal method of surgical treatment for patients with varying severity of facet degeneration based on comprehensive morphological and radiological analysis of cadaveric material has not been previously carried out.
In our opinion, treatment of patients with a combination of facet syndrome with compression symptoms should be based on a comprehensive preoperative radiological analysis of all spinal structures, including the FJ, IVD, yellow ligament, as well as the spinal canal diameter. The potential choice of decompression, stabilization, or a combination of both, should be based on clinical manifestations and their correlation with all of these structures.
Conclusion
A comprehensive instrumental-morphological assessment of various signs of FJ degeneration on cadaver material established that MRI data according to the Fujiwara classification reliably correlate with morphological changes according to the OARSI classification, the patient's age and cell density of the articular cartilage. This allows for a radiographic analysis of lumbar spine FJ to provide information about the microstructural state of the FJ throughout the spectrum of FJ disease. Future studies may be of use to identify the role that these findings may play in guiding operative and nonoperative management of patients with FJ pathology, ranging from injections or ablations at the initial stage of the degeneration to partial or total facetectomy with pronounced degenerative changes in FJs.
Footnotes
Author Contributions
Made significant individual contributions to this manuscript.
VAB, AAK, RAL and VB were the main contributors to the drafting of the manuscript.
VAB, AAK, YYP and VVS performed perform cadaver study and gathered radiological and morphological data.
AAK, YYP, VVS, MYB and BAJ evaluated the data from the statistical analysis.
VAB, AAK, RAL, VB and KDR performed the literature search and review of the manuscript, and contributed to the intellectual concept of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.