
Abstract
Study Design
Retrospective observational study.
Objectives
We aim to evaluate whether age is a risk factor for cage subsidence, and whether other patient characteristics, preoperative radiological or imaging parameters are associated with cage subsidence and the need for revision surgery in patients undergoing transforaminal lumbar interbody fusion (TLIF).
Methods
Patient demographics and surgery-related information were extracted. Cage subsidence was evaluated using upright standing sagittal plane X-rays and defined as more than 2 mm migration of the cage into the adjacent vertebral body. Patients who received revision surgery within 1 year for any reason were recorded. Radiographic parameters were measured. Univariable logistic regression models were used to evaluate the risk factors for cage subsidence and need for revision surgery.
Results
At 3-month and 1-year follow-up, cage subsidence was observed in 28 patients (16.5%) and 58 patients (34.1%), respectively. Twenty-seven patients received revision surgery within the first year after TLIF. Age (odds ratio (OR): 1.07 per year) and male sex (OR: 2.76) had a significantly increased odds ratio for cage subsidence 3 months after TLIF. Male sex (OR: 2.55) but not age was a significant risk factor for cage subsidence 1 year after TLIF. Of all assessed risk factors, only BMI (OR: 1.11 per kg/m2) had a significantly increased risk for the need of revision surgery.
Conclusions
Age was associated with cage subsidence 3 months but not 1 year after TLIF suggesting that age is only a risk factor for early cage subsidence and not in a longer follow-up.
Keywords
Introduction
Degenerative lumbar spinal diseases are a well-known phenomenon in the aging spine and can cause a range of clinical symptoms such as low back pain and neurogenic claudication with lower limb pain as well as weakness in the back or the legs while standing or walking. 1 These symptoms may largely compromise quality of life in those affected.
One of these diseases is degenerative spondylolisthesis that causes 1 vertebral body to slip over the underlying vertebral body. This frequently triggers a spinal stenosis and can be associated with typical neurogenic claudication preventing the patient’s participation in activities of daily living.2,3 In cases where conservative treatment fails and the degree of suffering is high, transforaminal lumbar interbody fusion (TLIF) is 1 of the most commonly performed surgical procedures to treat degenerative spondylolisthesis. 4 Interbody fusion is attempted with a cage that helps reconstructing the anterior column after disc removal and maintaining proper disc height despite weight-bearing while providing solid fixation of the spinal segments. 5 With advances in technology, the unilateral transforaminal approach avoids the dura and nerve roots on the asymptomatic side, and preserves the paraspinal musculoligamentous tissue. 6 However, TLIF still carries a high risk of complications such as perioperative and postoperative complications,7-9 possibly because of the increasing age of patients undergoing TLIF.9,10
Cage subsidence is a common postoperative radiological complication of lumbar interbody fusion that manifests as sinking of the cage towards the adjacent vertebral endplates. 11 For instance, Singhatanadgige et al have reported that the incidence of cage subsidence can reach up to 59.3%. 12 We hypothesize that the incidence of cage subsidence increases with age. Additionally, subsidence may be related to multiple factors including surgical technique, the morphology of the vertebral cage, the use of osteobiologics, and the local bone quality. 13 Although several studies have assessed the association between patient demographics and cage subsidence at long-term follow-up,14,15 the association between early postoperative cage subsidence and patient demographics has rarely been directly examined.
Several radiological parameters may play a role in the development of cage subsidence. Previous studies have reported that lower disc height, 14 higher degrees of degenerative spondylolisthesis, 13 and greater multifidus muscle atrophy 12 are risk factors for cage subsidence. Other parameters such as severity of lumbar spinal stenosis (LSS), disc degeneration, and sagittal alignment may be associated with cage subsidence. Evidence of an association between cage subsidence and these parameters would allow for better preoperative evaluation and surgical planning in patients with a potential indication for TLIF.
The primary objective of this study was to evaluate whether age is a potential risk factor for cage subsidence and the need for revision surgery in patients undergoing TLIF at 3-month and 1-year follow-up. The secondary objective was to determine whether other patient characteristics, preoperative radiological or imaging parameters are associated with cage subsidence and the need for revision surgery in patients undergoing TLIF.
Materials and Methods
Study Cohort
This retrospective study was approved by the regional ethics board (Ethikkommission Nordwestschweiz EKNZ 2021-02227) and performed in accordance with the guidelines specified in the Declaration of Helsinki. We retrospectively included all patients who received TLIF at our clinic between January 2015 and June 2020 using the following inclusion criteria: (1) aged 55 years or older (as only few patients younger than 55 years received TLIF in our clinic), (2) indications for TLIF surgery (e.g., ongoing impairment after at least 6 months of conservative treatment for degenerative spondylolisthesis), (3) existing preoperative standing sagittal plane X-rays of the lumbar spine with clear visibility of the pelvis, sacrum, and femoral head, (4) existing preoperative magnetic resonance images (MRI) of the lumbar region with clear visibility of different fatty infiltration grades and stenosis grades, and (5) complete 3-month and 1-year follow-up data, including clinical and radiological data. Exclusion criteria were: neuromuscular diseases such as Parkinson’s disease or multiple sclerosis according to our records; preoperative infection and/or malignant tumor with involvement of the bony or soft tissue structures of the lumbar spine; presence of a documented consent dissent. This retrospective study on coded data was exempted by the regional ethics board from obtaining informed consent from patients without general consent or dissent.
Demographic and Surgery-Related Information
Demographic information including age, sex, and body mass index (BMI) were extracted from patient files. Surgery-related information including previous surgeries of the lumbar spine, previous spinal fusion surgeries of the lumbar spine, number of TLIF segments, and postoperative infection was collected.
Surgical Technique
The performing surgeons had all been trained in the same clinic. The surgeries were carried out according to the spine clinic standards. The majority of patients was treated with a traditional open technique using a midline approach. In specific cases, a minimally invasive technique using posterolateral percutaneous incisions was chosen. In any case, similar types of polyaxial pedicle screws from a single brand were used. All patients received the same type of TLIF cage whereas the footprint and height of the 8° lordotic angled ProTi 360° PEEK (polyetheretherketon) titanium integrated cage were chosen individually. Fusion was attempted to be achieved by posterolateral autologous bone apposition, and the TLIF cage was filled with a mixture of autologous bone graft and demineralized bone matrix.
Outcome Assessment
Cage subsidence was evaluated at 3-month and 1-year follow-up and its occurrence used as primary outcome. Cage subsidence was evaluated using upright standing sagittal plane X-rays, and defined as cage migration of more than 2 mm into the adjacent vertebral body. 11 All patients who received revision surgery within 1 year for any reason were recorded. In case that a patient had undergone revision surgery within the first year after surgery, the 1-year follow-up from the initial surgery was selected to evaluate cage subsidence
Radiological Measurement
From preoperative standing sagittal and coronal plane X-rays of the lumbar spine, the sagittal spinopelvic parameters pelvic incidence (PI), lumbar lordosis (LL), and PI and LL mismatch (PI-LL) were measured
16
(Figure 1). The measurement of lumbar scoliosis in the coronal plane was based on the definition of a Cobb angle greater than 10°.
17
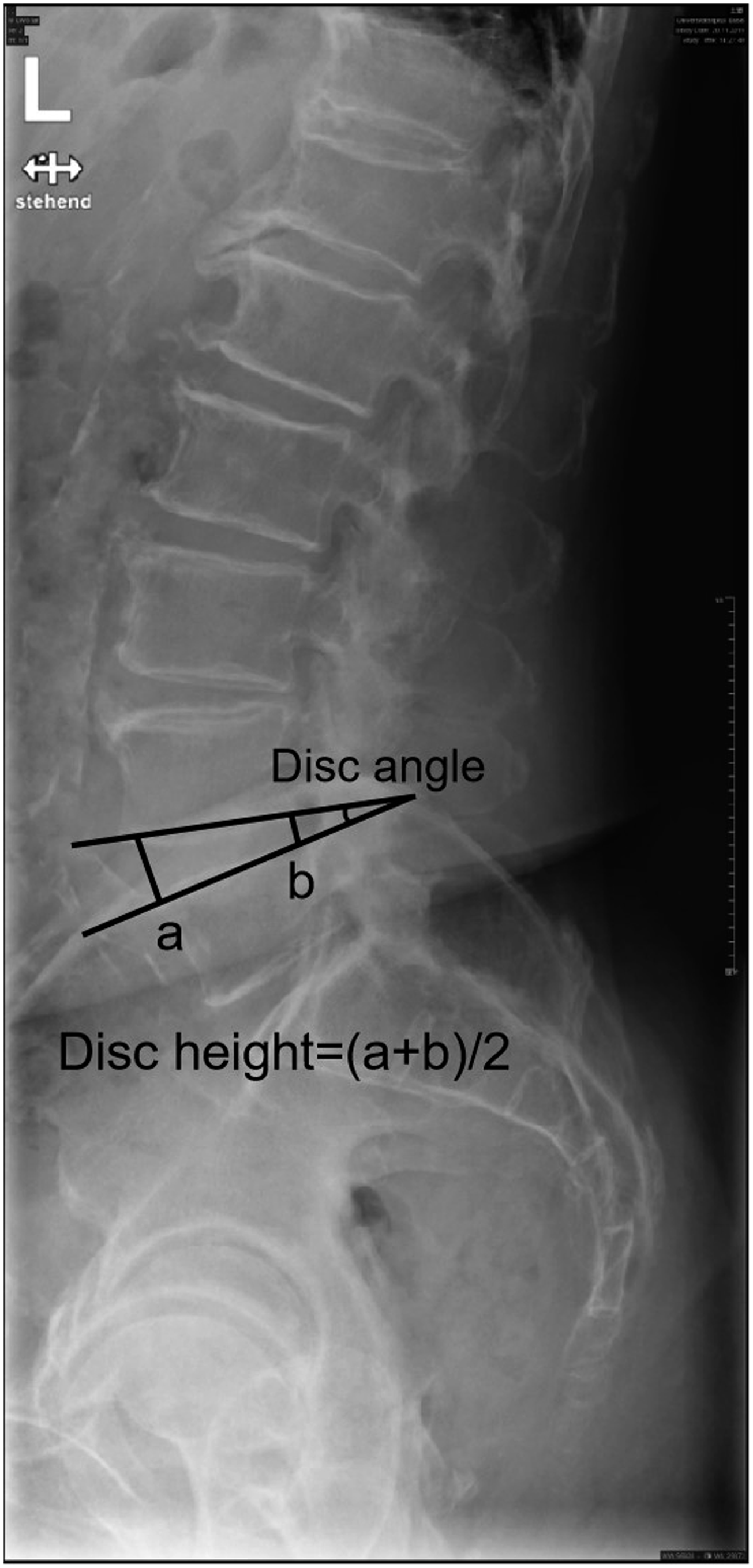
The sagittal disc angle of the surgical level was measured as the angle between the inferior endplate of the superior vertebral and the superior endplate of the inferior vertebral body (Figure 2). Spondylolisthesis was assessed in the standing X-ray using the Meyerding classification system.
18
Standard clinical T2-weighted MRIs of the lumbar spine region were acquired. The patients were in supine position with legs extended. Images at the mid segment of each surgical intervertebral disc were identified, saved and further evaluated. The following parameters were measured at each surgical level. The fatty infiltration was assessed using the Goutallier classification (grade 0 to 4).
19
The severity of LSS was assessed using the Schizas classification (grade A to D).
20
Intervertebral disc degeneration was assessed using the modified Pfirrmann grading system21,22 and disc height at each surgical level was measured using the modified Farfan method23-25 (Figure 2). All measurements were performed using the picture archiving and communication system (PACS). The measurement of PI and LL. The measurement of disc angle and disc height.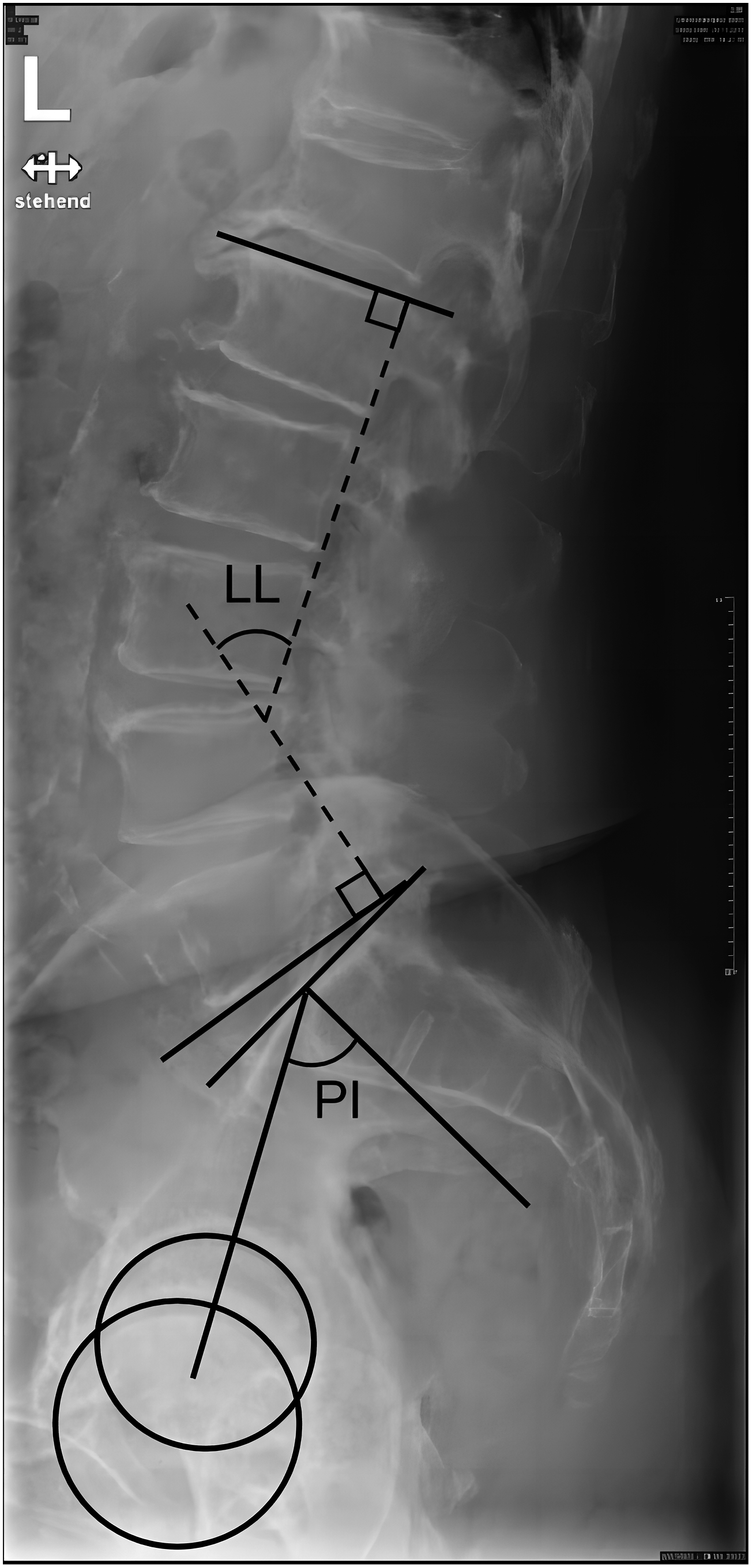
Statistical Analysis
Baseline characteristics were described using descriptive statistics. Median and interquartile range (IQR) were used for all continuous parameters, and N and percentages for categorical parameters. To determine whether age is a risk factor for (1) cage subsidence and (2) need for revision surgery, we used univariable logistic regression models with cage subsidence and the need for revision surgery as outcome variables and the patients’ age at surgery as independent variable. Further, we also assessed whether sex, BMI, surgery-related information (i.e. history of previous lumbar surgery or lumbar fusion, number of fused levels), and preoperative radiological parameters (i.e. spondylolisthesis degree, Pfirrmann grade, stenosis degree, fatty infiltration, PI, LL, PI-LL, scoliosis, disc height, and disc angle) are risk factors for cage subsidence or the need for revision surgery. Because only few patients presented with fatty infiltration grade 4, grades 3 and 4 were grouped for the analysis. We used likelihood ratio tests to calculate P-values and test for differences between risk factors and our outcomes. All analyses were conducted using the statistical software package R, and the significance level for all statistical tests was set a priori to P < .05.
Results
Assessed Parameters of the Patients.
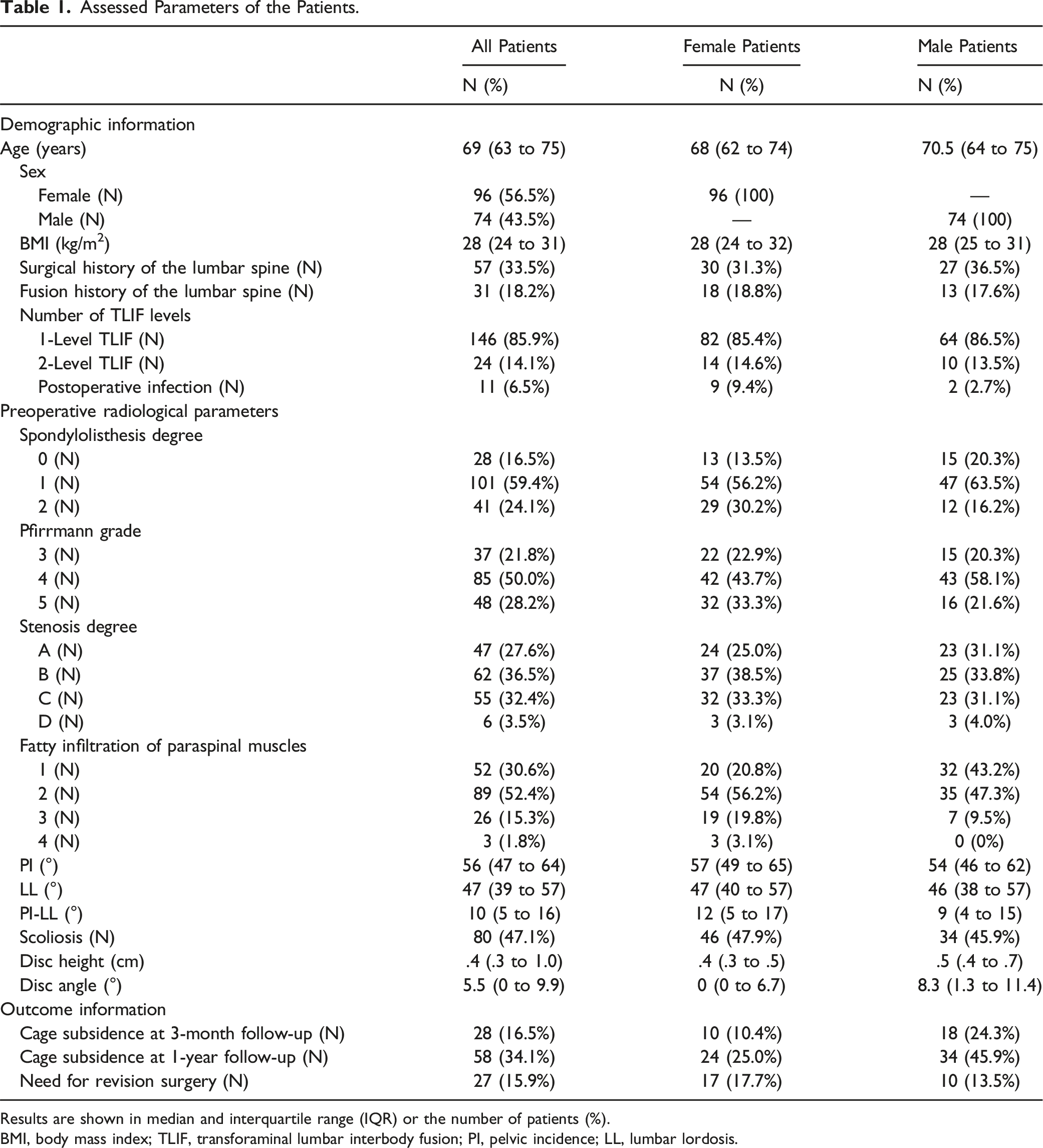
Results are shown in median and interquartile range (IQR) or the number of patients (%).
BMI, body mass index; TLIF, transforaminal lumbar interbody fusion; PI, pelvic incidence; LL, lumbar lordosis.
At 3-month and 1-year follow-up, cage subsidence was observed in 28 patients (16.5%) and 58 patients (34.1%), respectively. Twenty-seven patients received revision surgery within 1 year after TLIF. In 8 of these 27 patients (29.6%) cage subsidence was observed at the follow-up around 1 year after the initial surgery (Table 1). Only in 1 case, cage subsidence was the reason for revision surgery.
Univariable Logistic Regression Results for Cage Subsidence at 3-Month Follow-Up.
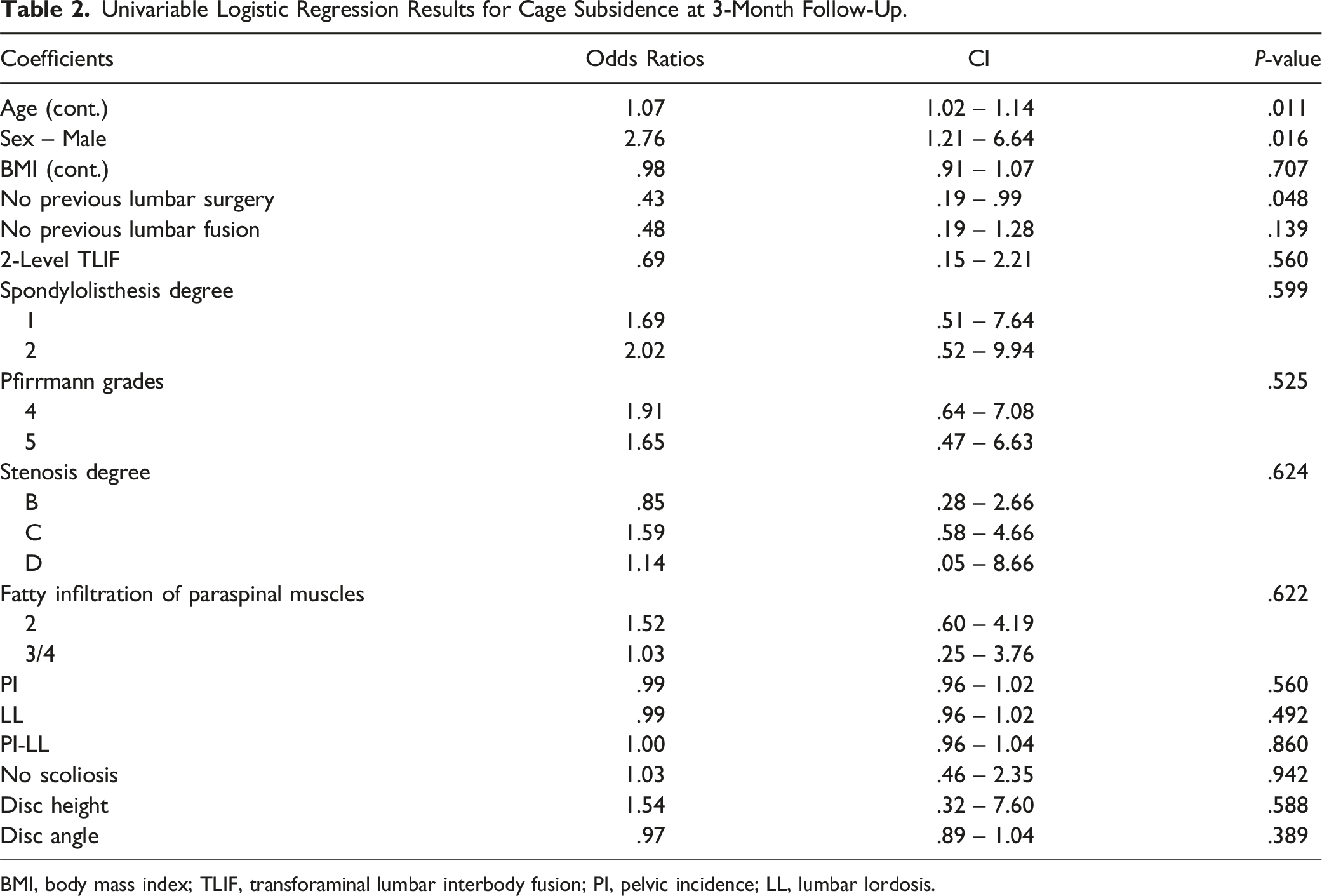
BMI, body mass index; TLIF, transforaminal lumbar interbody fusion; PI, pelvic incidence; LL, lumbar lordosis.
Univariable Logistic Regression Results for Cage Subsidence at 1-Year Follow-Up.
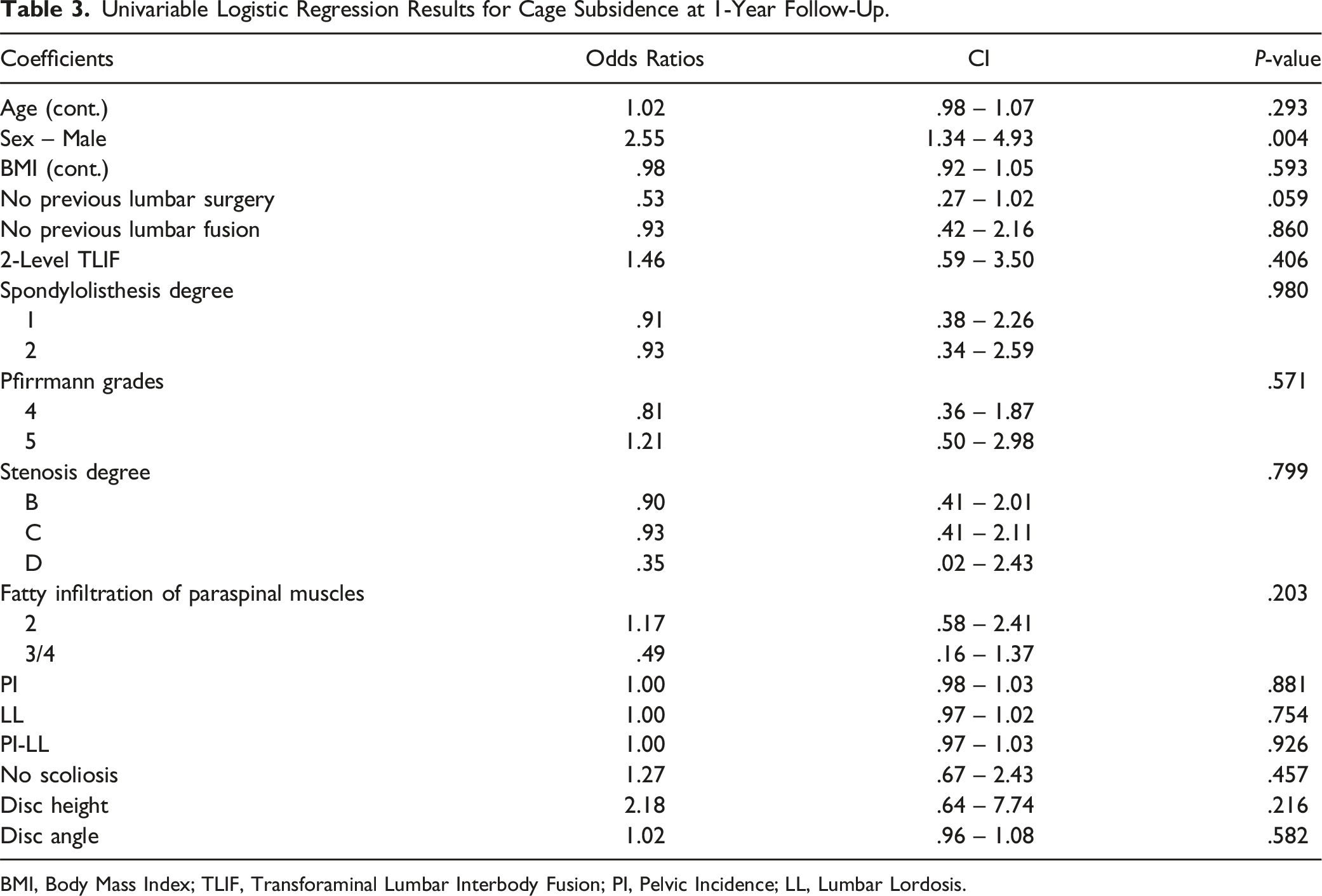
BMI, Body Mass Index; TLIF, Transforaminal Lumbar Interbody Fusion; PI, Pelvic Incidence; LL, Lumbar Lordosis.
Univariable Logistic Regression Results for the Need for Revision Surgery.
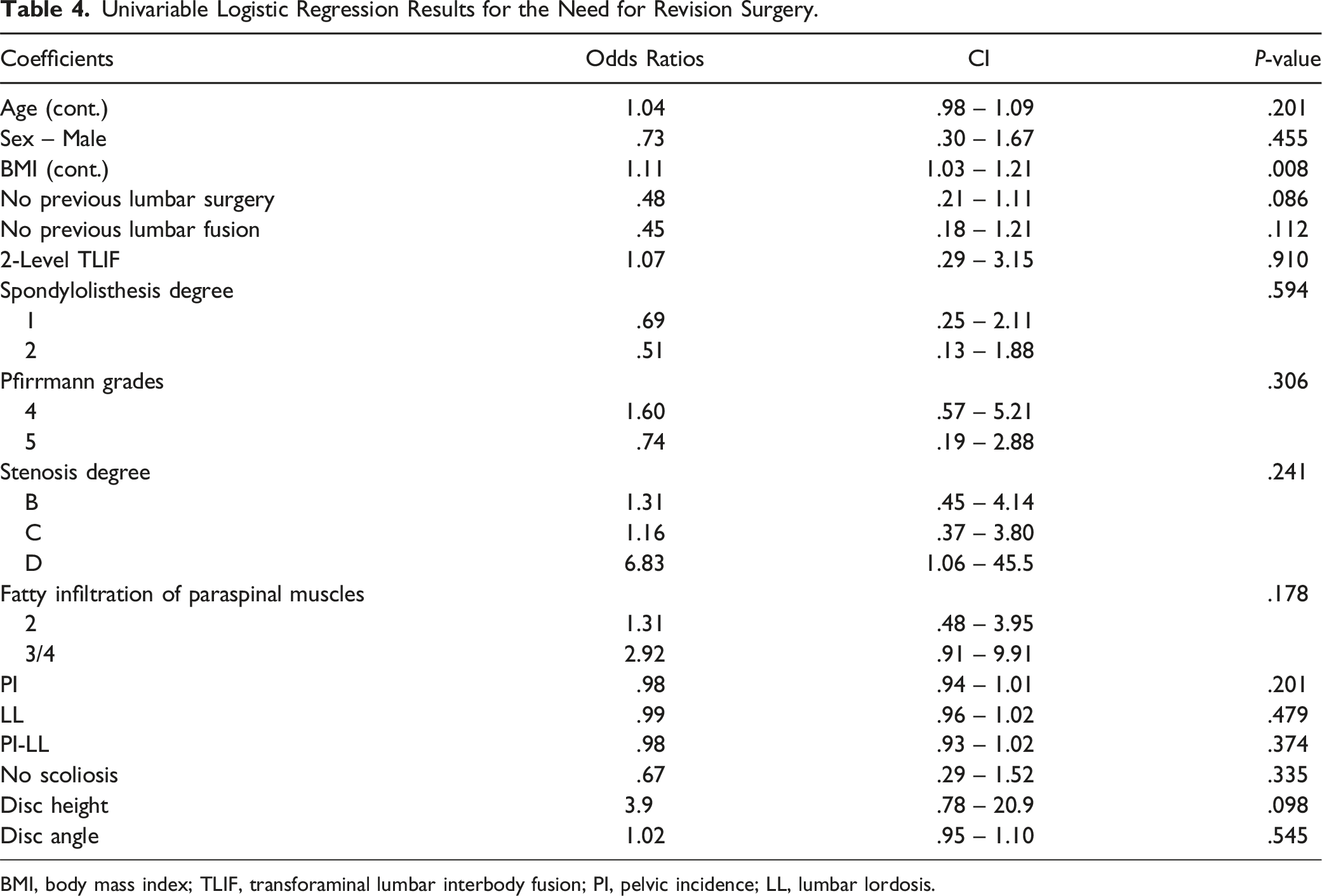
BMI, body mass index; TLIF, transforaminal lumbar interbody fusion; PI, pelvic incidence; LL, lumbar lordosis.
Discussion
The main purpose of this study was to evaluate whether age is a potential risk factor for cage subsidence and the need for revision surgery in patients undergoing TLIF at 3-month and 1-year follow-up. The secondary objective was to determine whether other patient characteristics, preoperative radiological or imaging parameters are associated with cage subsidence and the need for revision surgery in patients undergoing TLIF. We included patients over 55 years of age, and 48% of the patients were over 70 years of age at the time of surgery. We found a significant association between age and cage subsidence 3 months postoperatively, but no significant association 1 year postoperatively. This suggests that cage subsidence is more likely to occur earlier after surgery in older patients. We also found that male sex was associated with cage subsidence 3 months and 1 year postoperatively. Moreover, BMI was associated with the need for revision surgery, with patients with greater BMI having a higher risk of needing revision surgery, suggesting that BMI should be routinely considered preoperatively.
Cage subsidence is a common postoperative radiological complication reported in many studies. Kim et al 11 reported that 32.8% of PEEK cages showed subsidence after TLIF at 2-year follow-up. Yao et al 14 reported that cage subsidence occurred in 34.1% of the operated levels at a minimum 2-year follow-up in patients who received minimally invasive TLIF. Similar results have also been reported in other studies.26,27 In our study, the incidence of cage subsidence was 16.5% at 3-month follow-up and 34.1% at 1-year follow-up. We statistically analyzed the rate of postoperative cage subsidence in patients not in segments. Some patients received TLIF in 2 segments but only 1 segment showed cage subsidence postoperatively, which may lead to a greater rate of cage subsidence in patients than that in segments. Compared to previous studies, the rate of cage subsidence at long-term follow-up was comparable.
Our analyses revealed a significant association between age and cage subsidence within the first 3 months postoperatively but no significant association after 1 year. This suggests that age is an important risk factor for early cage subsidence after TLIF, with older patients being more prone to having cage subsidence within the first 3 months postoperatively. However, at the 1-year follow-up, age was no longer associated with cage subsidence. This result for the 1-year follow-up is in agreement with several studies that found no influence of age on the occurrence of cage subsidence at least 6 months after TLIF or lateral lumbar interbody fusion 13 or at least 2 years after TLIF.11,14 On the other hand, Singhatanadgige et al suggested that age over 65 years is a risk factor for cage subsidence 1 year after TLIF. 12 However, they used computer tomography scans to assess cage subsidence and reported with 59% of the operated levels a much higher occurrence. Hence, it is still controversial whether age is a risk factor for cage subsidence at long-term follow-up after TLIF, and our finding is that age is not a risk factor. Currently, studies assessing the association between age and cage subsidence in the early postoperative period (3 months) are lacking. Nevertheless, age has long been an important factor in degenerative spinal disease due to the overall poorer physical status of older patients, such as decreased bone density, disc degeneration, and poor muscle strength. 28 Thus, our results suggest that these factors might play a role especially in the early postoperative phase while later other factors might contribute to cage subsidence.
In clinical practice, cage subsidence is detected in some cases at the early postoperative follow-up. It is important to consider that the influence of age might level off statistically in the long-term follow-up, since age was no longer related to cage subsidence in our study. The cage subsidence observed in our cohort was based solely on radiographic findings. Revision rates did not differ between those with such radiographic findings and those without these findings. Clearly, studies with longer follow-ups are needed to verify whether cage subsidence is related to long-term adverse symptoms and worse outcomes or the need for revision beyond 1 year after surgery.
In our cohort, male sex was associated with cage subsidence 3 months and 1 year postoperatively. This is an unexpected result and contrary to conventional perception and previous studies.11,14 Due to the higher prevalence of osteoporosis and thus lower bone quality in older (above the age of 50) women than in men due to declining estrogen levels, 29 1 would expect higher risk of cage subsidence in women. As we did not assess the presence of osteoporosis in this study, because no objective measure (such as Dual Energy X-ray Absorptiometry scans) was available for all patients, the influence of bone quality on this surprising result is unknown. Moreover, there were no striking differences between the included male and female patients (Table 1).
Other important parameters generally considered as risk factors for cage subsidence in clinical practice did not reach statistical significance in our study. For instance, Yao et al 14 found a lower disc height and higher presence of degenerative scoliosis in the coronal plane in patients with cage subsidence after TLIF than in those without. The risk of cage subsidence can be reduced by choosing the appropriate size of cage and avoiding damage to the endplate during the operation. While the latter 1 depends on the surgical abilities and responsibilities and is almost impossible to rule out, the careful selection of the appropriate cage size might have generally reduced the risk of cage subsidence in the present study. The number of fused segments of TLIF (single-level or multi-level) might be considered a risk factor for cage subsidence. Due to the vertical transfer of gravity, multi-segment fusions are less flexible than single-segment fusions and have significant cantilever bending torque at the end level, which may result in greater stress on the cage. 30 However, consistent with our study, most previous studies did not observe an effect of multi-level fusion on cage subsidence.14,31 Additional preoperative radiological grading systems such as fatty infiltration of paraspinal muscles, stenosis grade, disc degeneration grade, spondylolisthesis grade, and PI-LL were also assessed in our study, but these were not associated with postoperative cage subsidence. Nevertheless, the severity of spondylolisthesis has been suggested as a risk factor for cage subsidence as Amorim-Barbosa et al 13 reported a tendency for a higher risk of subsidence in Meyerding spondylolisthesis grades ≥2. However, only around 20% of the patients in our study had higher degrees of spondylolisthesis (Meyerding grade = 2). Hence, radiological grading systems cannot fully represent the actual severity of disc degeneration or muscle strength, and studies with larger sample sizes are needed to verify the relationship between the preoperative parameters and cage subsidence.
A higher BMI – indicating obesity – was found to be a risk factor for the need for revision surgery in our study. In a previous meta-analysis by Goyal et al, 32 obesity was shown to have an impact on the rate of revision surgery, and many previous studies have shown that obesity can lead to several complications of spinal surgeries.33,34 In clinical practice, surgical choices for obese patients requiring lumbar fusion surgery should be carefully selected, and the risks of surgical complications and revision should be taken into account.
Overall, an association of age with cage subsidence was found 3 months postoperatively and disappeared at 1-year follow-up suggesting that higher age is an important risk factor for cage subsidence in the early postoperative period after TLIF. This result is relevant to spine surgeons because it suggests that even if a cage subsides within the first 3 months after surgery, this does not necessarily mean worse long-term outcome. In our cohort, the preoperative stenosis grade, disc degeneration grade, spondylolisthesis grade, and PI-LL were not associated with cage subsidence. Whether these parameters are clinically relevant still needs to be assessed in prospective studies.
Strength and Limitations
The main strengths of this study are the large sample size, the inclusion of a wide age range including patients with advanced age. However, several limitations should be acknowledged. Although the sample size was large, there were no patients in some preoperative radiological grades such as higher Meyerding spondylolisthesis grades 3 and 4 precluding assessing their influence on cage subsidence. Moreover, cage subsidence is only a radiological complication, and we did not assess postoperative clinical manifestations such as patient related outcome measures. Hence, whether cage subsidence affects postoperative outcomes such as, quality of life remains to be investigated. The follow-up period was limited to 1 year, therefore longer-term outcomes related to cage subsidence could not be assessed. Finally, because no objective measure for osteoporosis was available for all patients, evaluating the effect of osteoporosis, which is a known risk factor for cage subsidence, on our results was not possible.
Conclusions
Age was associated with cage subsidence 3 months but not 1 year after TLIF suggesting that age is only a risk factor for early cage subsidence and not in a longer follow-up. Hence, especially in older patients, potential cage subsidence should be closely monitored in the first months after TLIF. Whether cage subsidence is related to worse clinical outcome needs to be investigated in further studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.