
Abstract
Study design
Systematic review.
Objectives
Surgical procedures for lumbar degenerative diseases (LDD), which have emerged in the 21-century, are commonly practiced worldwide. Regarding financial burdens and health costs, readmissions within 30days following surgery are inconvenient. We performed a systematic review to integrate real-world evidence and report the current risk factors associated with 30-day readmission following surgery for LDD.
Methods
The Cochrane Library, Embase, and Medline electronic databases were searched from inception to April 2022 to identify relevant studies reporting risk factors for 30-day readmission following surgery for LDD.
Results
Thirty-six studies were included in the review. Potential risk factors were identified in the included studies that reported multivariate analysis results, including age, race, obesity, higher American Society of Anesthesiologists score, anemia, bleeding disorder, chronic pulmonary disease, heart failure, dependent status, depression, diabetes, frailty, malnutrition, chronic steroid use, surgeries with anterior approach, multilevel spinal surgeries, perioperative transfusion, presence of postoperative complications, prolonged operative time, and prolonged length of stay.
Conclusions
There are several potential perioperative risk factors associated with unplanned readmission following surgery for LDD. Preoperatively identifying patients that are at increased risk of readmission is critical for achieving the best possible outcomes.
Introduction
With the increase in average life expectancy, lumbar degenerative diseases (LDD), including spondylolisthesis, disc degeneration, and spinal stenosis, are becoming increasingly common worldwide. 1 LDD often induce lower back pain, lower extremity numbness or pain, claudication, and disability, 1 which results in negative effects on the patient’s quality of life. Surgical treatment is indicated for patients in whom medical therapy fails. With advances in patient care and medical technologies, an increasing number of patients are willing to undergo surgery. Therefore, surgical procedures for LDD, such as decompression, discectomy, fusion and implantation of prostheses, have emerged in the 21st century. 2 Spine surgery and related care expenditures significantly contribute to healthcare economics. 3 Regarding financial burdens and health costs, readmissions within 30 days following surgery (30-day readmission) are troublesome.4,5
The American College of Surgeons National Surgical Quality Improvement Program (NSQIP) 6 has registered 30-day readmissions following spine surgery in the database since 2011. 7 The incidence of 30-day readmissions following spine surgery for LDD is approximately 5-10%, varying according to the procedure.8,9 Although several studies aimed to identify predictors of 30-day readmissions from either nationwide or institutional databases, the reported risk factors or predictors were not consistent in the literature.
From the literature review, only 1 meta-analysis in 2014, 10 summarized the predictors of 30-day readmission following not only surgeries for LDD but all spinal surgeries. Therefore, a great diversity of spinal pathologies, including tumors, deformities, trauma, infection, and degeneration were included at the surgical level, encompassing the cervical, thoracic, and lumbar spine. In recent years, there has been an increase in publications focusing on readmission following surgeries for LDD. Therefore, we aimed to perform a systematic review to integrate real-world evidence and update the risk factors associated with 30-day readmission following surgery for LDD.
Methods
We conducted the present systematic review based on the Cochrane Handbook for Systematic Reviews and Interventions 11 and reported the results following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and Meta-analysis Of Observational Studies in Epidemiology guidelines (eMethods 1 and 2 in the supplementary information). This review was registered on the PROSPERO online platform (ID: CRD42022312510). Electronic databases of the Cochrane library, Embase and Medline were searched, from the inception of the database until April 2022 encompassing all languages. Two investigators (LYC and YC) independently conducted the search to identify relevant studies to be included, and any discrepancy was addressed by reaching a consensus or by consulting senior reviewers (PHL, CCH and JSL). The search details are presented in eMethod 3 in the supplementary information.
Eligibility Criteria
The articles meeting the following criteria were included:
(1) Prospective/retrospective cohort or case-control studies were included; in contrast, case reports, editorials, letters to the editor, review articles, and conference abstracts were excluded; (2) studies reporting at least 1 risk factor for 30-day readmission following spine surgeries were included; (3) studies of spine surgeries with non-degenerative conditions were excluded (eg, traumatic injuries, infections, deformities, or tumors); (4) studies with less than 20 readmitted patients were excluded; and (5) studies of robotic surgeries and endoscopic spine surgeries were excluded because of the apparent variation compared to conventional surgical procedures.
Data Extraction
Two investigators independently extracted relevant information from the tables or results of eligible articles. Extracted data included the first author’s name, publication year, country where the study was conducted, data source, inclusion criteria, exclusion criteria, follow-up time, number of participants, and significant risk factors for readmission with multivariable adjustment.
Quality Assessment
Two investigators independently completed a critical appraisal of the included literature using the Quality In Prognosis Studies (QUIPS) tool. 12 The domains included patient selection, study attrition, measurement of prognostic factors, outcome measurement, study confounding, statistical analysis, and reporting, which were rated as having a low, moderate, or high risk of bias. Any item on which assessors did not reach consensus was addressed through discussion with a third investigator (JSL).
Results
Study Selection
Our search strategy identified 6482 references from the Cochrane Library, Embase, and Medline electronic databases. After screening the titles and abstracts, we excluded duplicates (n = 676) and irrelevant references (n = 5714). The remaining 92 studies were retrieved for full-text review, 367-9,13-45 of which were included in the review. (Figure 1). PRISMA diagram. We initially extracted 6482 potential references. Eventually, 36 studies fulfilled the eligibility criteria, and were included.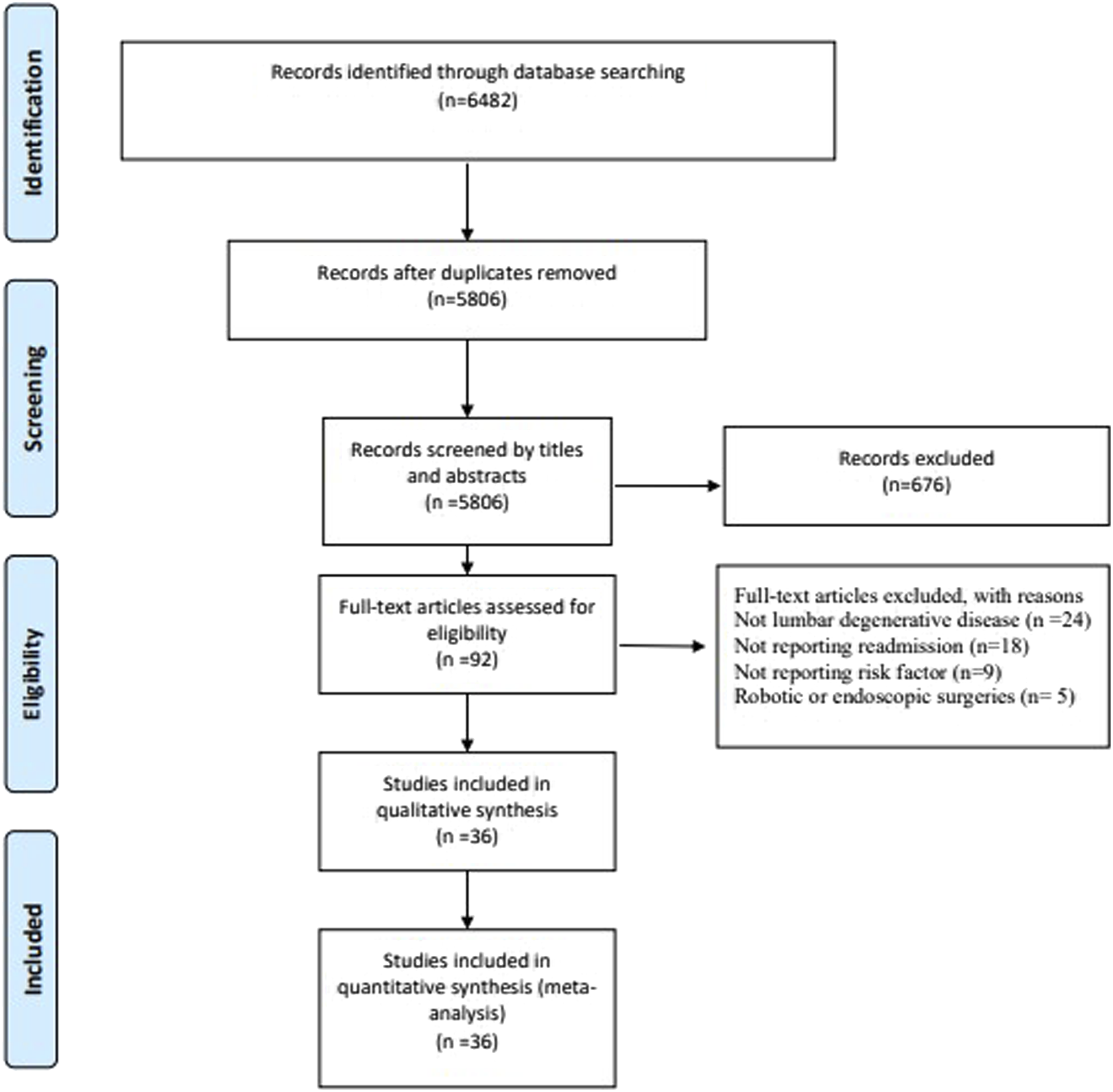
Study Characteristics and Risk Factors
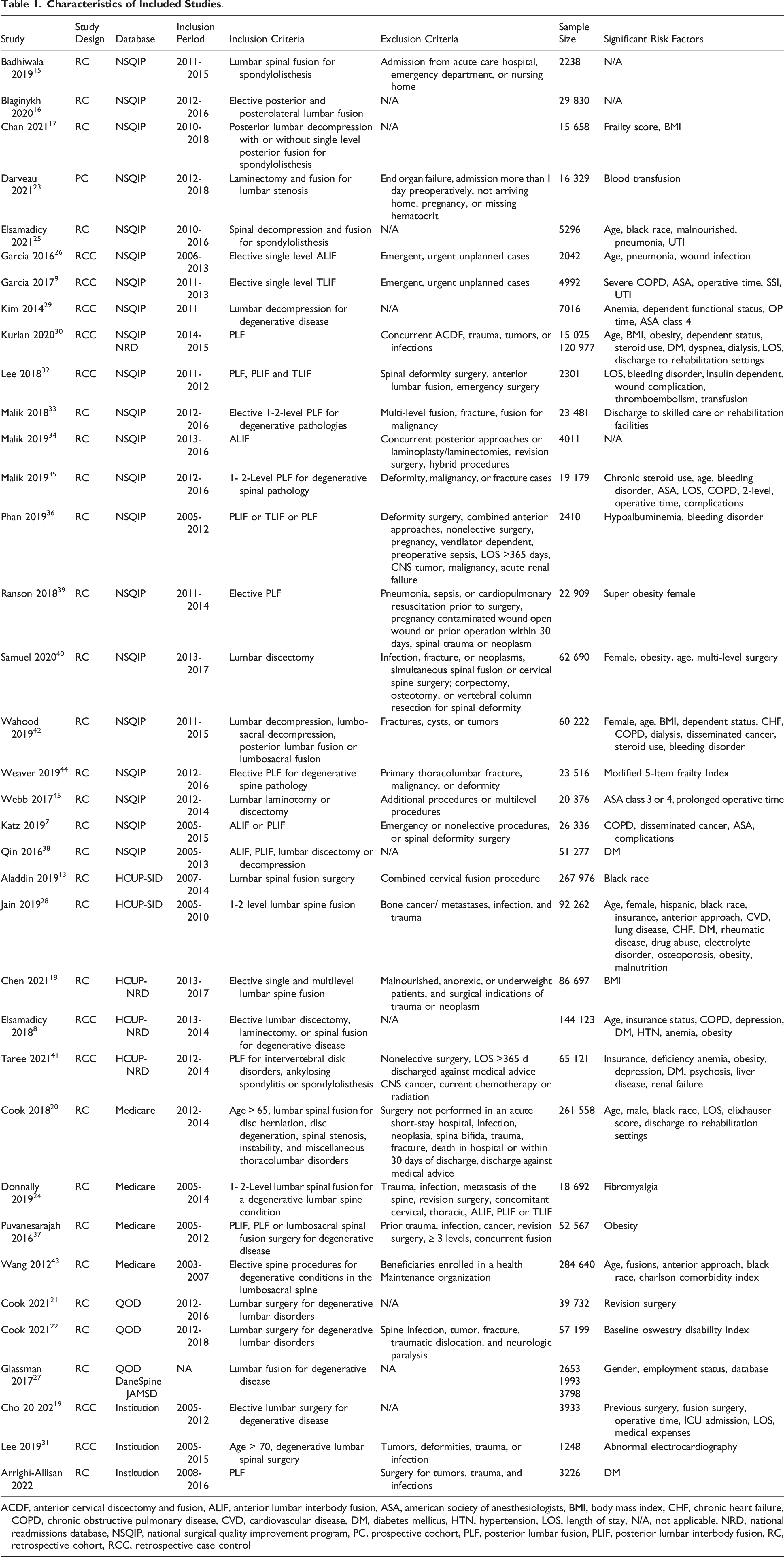
A total of 36 studies7-9,13-45 were included (Table 1). Of these, 267,13-18,20-22,24,25,27,28,33-40,42-45 were retrospective cohort studies, 1 23 was a prospective cohort study and 98,9,19,26,29-32,41 were case-control studies. Among them, 207,9,15-17,23,25,26,29,32-36,38-40,42,44,45 included patients from the NSQIP database, 2 from State Inpatient Databases (SID)13,28, 3 from Nationwide Readmissions Database (NRD)8,18,41, 4 from the Medicare database20,24,37,43, 2 from the Quality Outcomes Database (QOD)21,22, and 3 from institutional database14,19,31. In addition, 1 study 30 enrolled patients from both the NSQIP and NRD and another 1 27 enrolled patients from the QOD, DaneSpine database and Japan Multicenter Spine Database (JAMSD).
Quality Assessment of the Included Studies
The quality assessment of the inclusion studies using QUISP is summarized in Supplemental eTable 1.
Risk Factors for 30-day Readmission
The risk factors with multivariate analysis reported in more than 2 studies are summarized in Supplemental eTable 1 and 2 in the supplementary information.
Patient Risk Factors (eTable 1)
Fifteen studies7,8,15,19,20,25,26,28-31,35,40,42,43 reported the association of age and readmission with multivariate adjusted odds ratio, with significant correlation observed in 6 studies7,19,20,25,26,43 using linear regression and 68,15,28,35,40,42 using cut-off value of age.
Five studies investigated the risk of readmission in different races,13,20,25,28,43 with Black patients exhibiting a significantly higher risk. The impact of obesity was analyzed in 107,8,18,25,28,30,31,39-41 studies, 58,18,28,30,39,41 of which reported obesity as a significant risk factor, 218,40 reported that body mass index (BMI) > 30 was associated with a higher risk of readmission and 1 30 found similar correlation using linear regression of BMI.
Eleven studies7-9,20,25,28,31,39,40,42,43 compared the incidence of readmission between men and women with only 5 studies20,28,39,40,42 reporting a significant difference (4 of the studies reported a higher risk for females28,39,40,42 and 1 for males 20 ). There was no difference in the risk of readmission between inpatient and outpatient surgery.16,30 The impact of the American Society of Antitheology (ASA) score was reported in 8 studies.7,9,25,29-31,35,45 Kim et al 29 reported that ASA 4 was a significant risk factor compared to ASA 1. Katz, 7 Malik 35 and Webb 45 reported that ASA 3 or 4 was significantly associated with readmission compared with ASA 1 or 2. Garcia 9 also reported ASA was a significant risk factor using linear regression. Increased rates of readmission were observed in 4 of the 5 studies reporting bleeding disorder.32,35,36,42 Anemia was considered as a risk factor in 3 of the 4 studies where it was reported.8,29,41 Chronic pulmonary disease (non-specified) was reported in 8 studies,7-9,26,28,29,35,42 of which, Elsamadicy 8 and Jain 28 considered it as a significant risk factor. Among these studies, 5 reported a history of chronic obstructive pulmonary disease (COPD)7,9,26,35,42 associated with readmission. Eleven studies7,8,14,28-32,38,41,42 reported diabetes mellitus (DM) as a potential risk factor, 97,8,14,28,30,32,38,41,42 of which showed statistically significant results in this regard. Three studies7,28,42 reported heart failure and 2 of them28,42 found that patients with heart failure had a higher risk of readmission. Five studies8,29-31,42 reported hypertension and only 1 8 considered it as a significant risk factor. Two studies8,28 investigated the impact of hypothyroidism and found no significant differences. The impact of underlying malignancy on the risk of readmission was investigated in 3 studies7,28,42 with only Wahood 42 reporting a significant risk in patients with disseminated cancer. Three studies7,30,42 investigated the influence of hemodialysis (HD) and 230,42 of them reported significant higher risk. Two studies investigated the impact of comorbidity with 1 using the Charlson comorbidity index 43 and the other using the Elixhauser score. 20 A higher frailty index was associated with higher risk of readmission in 3 studies.17,25,44 A higher Oswestry disability index was associated with a higher risk of readmission in 1 study. 22 Three studies29,30,42 reported that patients with dependent status had a higher risk of readmission. Regarding preoperative nutritional status, 3 studies25,28,36 found malnutrition to be a significant risk factor for readmission. Two studies8,28 found that depression significantly increased readmission rates. Six studies7,25,29,30,35,42 compared readmission rates between patients with baseline chronic steroids and non-users and significant detrimental effect was found in 3 studies.30,35,42 There are 2 studies28,30 reporting alcohol abuse with significant elevated risk of readmission in 1. 30
Perioperative Risk Factors (eTable 2)
Three studies19,31,43 compared the incidence of readmission following decompression alone vs fusion, and only 1 study 43 showed a significant difference. Two studies28,43 investigated surgical approaches, and patients receiving surgery with anterior approach have higher 30-day readmission rate compared to posterior approach. Regarding postoperative complications, Malik, 35 Katz 7 and Lee 32 reported that non-specific complications were associated with a higher incidence of readmission. Garcia9,26 identified surgical site infection, pneumonia, and urinary tract infection (UTI) as significant risk factors, and Elsamadicy 25 found that adverse events including pneumonia and UTI are predictors of readmission. Four studies7,21,28,40 compared readmission in patients undergoing primary vs revision surgery, and Cook 21 and Katz 7 found revision surgery to be associated with a higher risk of readmission; however no difference was found in the other 2 studies.28,40
The impact of prolonged operative time was reported in 5 studies9,19,29,35,45 with significant findings observed in 3 studies9,19,29 using linear regression and 2 using cut-off values (151 45 and 210 35 minutes). Three studies31,35,40 reported relevant results regarding surgical levels, and multi-level surgeries led to a higher risk of readmission in 2 studies35,40 but no significant difference in the other 1 that reported surgical level by linear regression. 31 Two studies23,32 reported post/intra-operative blood transfusion and an increased risk of readmission was noted. Six studies19,20,30-32,35 reported the association between prolonged length of stay (LOS) and readmission rate with a positive correlation was observed in 5 studies.19,20,30,32,35 The impact of discharge destination was reported in 4 studies20,30,33,34 and discharge to inpatient care facilities 33 or rehabilitation-based facilities20,30 was associated with higher risk of readmission.
Discussion
To our best knowledge, this is the first systematic review to provide an overview of predictors of 30-day readmission following spine surgeries for LDD. We identified potential risk factors associated with 30-day readmission, including age, race, obesity, higher ASA score, anemia, bleeding disorder, chronic pulmonary disease, heart failure, dependent status, depression, DM, frailty, malnutrition, chronic steroid use, surgeries with an anterior approach, multi-level spinal surgeries, perioperative transfusion, presence of postoperative complications, prolonged operative time, and prolonged LOS, which were categorized into patient risk factors and perioperative risk factors in the following discussion.
Patient Risk Factors
Spine surgery can be safely performed in older patients and old age alone is not a contraindication for lumbar surgery. 46 However, the prevalence of co-occurring chronic diseases and disorders increases greatly with age, 47 which may negatively impact postoperative condition, recovery, and quality of life. In addition, an increase in aging bone, the degeneration of discs and facet joints, and the wasting of ligaments and muscles may lead to great destabilization and imbalance of the spine. 48 Owing to the severity of degeneration in older patients, surgical procedures have become more complex, such as longer instrumented segments, which are associated with a higher risk of complications and relatively worse clinical outcomes. 49 Based on our review, patients over 70-year-old exhibited much higher risk of 30-day readmission, which could be related not only to the surgical procedures but also to the patients’ preoperative condition.
Obesity imposes more loading on axial bones and inevitably accelerate spinal degeneration.50,51 Furthermore, compared to the general population, obesity can lead to more adverse events following lumbar spine surgery, 52 including increased surgical time, extended length of stay, wound complications, higher blood loss, urinary complications and thromboembolism events, 53 which subsequently lead to a higher incidence of unplanned readmission. Obesity is defined as a BMI ≥30, with morbid obesity being defined as a BMI ≥40. While the prevalence of obesity is on the increase, there are limited studies investigating strategies for weight loss before spine surgery in obese patients (BMI 30-40). 52 The benefits of bariatric procedures for morbid obesity before spine surgery have been reported in several studies, including fewer overall and wound-related complications, reduced in-hospital mortality, and improved healthcare utilization.54-56
Unplanned readmission may be related to underlying diseases and medical conditions, not the surgical procedures themselves. DM, 57 COPD 58 and heart failure 59 are common medical problems with high prevalence among older adults. Most included studies demonstrated a positive correlation of these conditions and unplanned readmission following surgery. Moreover, patients undergoing HD are vulnerable during the perioperative periods and the maintenance of stable homeostasis during hospitalization is a clinical challenge for surgeons and nephrologist. 60 On the surgical aspect, both DM and renal failure negatively impact wound healing and increases the risk of surgical site infection, which may further necessitate readmission and inpatient managements. 61
Anemia and bleeding disorders are associated with a higher risk of unplanned readmissions.8,25,29,41 Intraoperative transfusion may be required in patients with unstable hemodynamics. However, transfusion has been reported as an independent predictor of adverse postoperative outcomes,62,63 postoperative infection, 64 and prolonged hospital stay, 65 which could explain the higher unplanned readmission rate. 23
It is evident that patients’ underlying comorbidities are detrimental to their postoperative outcomes and recovery. In this line, a positive correlation between overall comorbidities and the incidence of readmission following lumbar spinal fusion surgery has been shown.20,43 This finding is in consistence with that higher ASA is also a significant risk factor in several studies.9,29,35,45 There are studies17,44 investigating the association of frailty index and unplanned readmission of patients receiving elective spinal fusion surgery, which yield the similar results. General functional status is also associated with postoperative morbidity and mortality.29,42 Performance assessment can partially reflect the aforementioned medical comorbidities since patients with multiple underlying medical co-morbidities usually have worse functional status. Malnutrition impairs wound healing postoperatively and compromise the immune system against infection, therefore, associated with several adverse events including wound complications and surgical site infections in not only spine surgery but other orthopedic surgery.66-68 It should be noted that presence postoperative adverse event is a strong predictor for unplanned readmission. Identifying malnourished patients and preoperative nutrition support may have benefit on postoperative outcome. 69
Chronic steroid use is associated with poor wound healing, infection, and minor or major complications following surgery. 70 Moreover, patients receiving steroids have poor bone quality, which increases the risk of implant loosening and readmission. 71 No doubt, chronic steroid use increases the risks 30-day readmission following surgery for LDD.
Aside from the patients’ physical medical conditions, mental issues, such as affective disorders, are topics of interest in multiple medical and surgical fields. Affective disorders, especially depression is associated with chronic back pain in general population and unsatisfactory outcomes in spine surgeries. 72 This is evident from the result of 2 large population-based studies8,28 in which patients with depression were associated with higher 30-day readmission following surgeries for LDD.
Perioperative Risk Factors
With the growing number of lumbar spinal surgeries for LDD and the increasing variety of fusion techniques, it is important to clarify the comparative risk of complications and postoperative outcomes of various types of surgery. Surgical complexity may influence its results and potential complications owing to prolonged surgical time, increased tissue damage, and blood loss. Our review demonstrated that anterior lumbar surgeries were associated with a higher risk of readmission. Anatomically, in order to access to the vertebrae, the anterior approach requires the dissection and retraction of abdominal vessels, while the posterior approach needs the subperiosteal muscle dissection. The great vessels overly the disc spaces, and their retraction is essential when exploring the discs of interest through an anterior approach. Direct vascular injury can result in immediate complications and mortality, but may not necessitate readmission within 30days. However, prolonged retraction of the great vessels during ALIF may be associated with a higher risk of DVT than posterior lumbar surgery. 73 Furthermore, since the posterior approach is standard for most spinal pathologies, it is the most commonly practiced procedure for spinal surgeons and particularly for entry-level residents. 74 Owing to the complex vascular anatomy and lower frequency of utilization, the anterior approach may impose an increased risk of vascular and wound events, resulting in a higher readmission rate than the posterior approach. 75 However, only 2 studies28,43 have compared the 30-day readmission risk of the anterior and posterior approaches. Wang et al 43 grouped patients into anterior, posterior, and concomitant anterior and posterior approach groups. Their analysis found that an anterior only approach was associated with a significantly higher incidence of readmission compared to the posterior only approach. In the other study, Jain et al 28 investigated patients undergoing posterior lumbar fusion, and found that patients operated on through a concomitant anterior approach experienced a significantly higher risk of readmission. Due to the limited data obtained from these studies, as well as their heterogeneity, further studies focusing on readmission with respect to surgical approach are warranted.
At the surgical level, multi-level spinal surgery is associated with a prolonged operative time, subsequently lead to postoperative complications and unplanned readmission. 76 However, Lee et al. 31 Reported that multi-level spinal surgery is not a significant risk factor, possibly because of advances in minimally invasive surgical techniques combined with appropriate patient selection.
The prevalence of complications following spine surgery is reported in around 20-40%77,78 of the patients, and is associated with increased morbidity, mortality, length of hospital stay, and health costs. 77 In our review, postoperative UTI, pneumonia, thromboembolism, and wound infection, were highly associated with unplanned readmission. The incidence of complications following surgery for degenerative spine disease is lower than that for trauma, infectious or malignant etiologies, which may be the result of underreporting owing to the retrospective design of most studies. The complication rate is associated with not only the complexity of the surgery but also the surgeons’ experience, which could constitute a potential bias that may be challenging to take in consideration. Moreover, there is a lack of a generalized classification system assessing complications following spinal surgery, which makes it difficult to determine its impact on postoperative outcomes. Therefore, a robust correlation between postoperative complications and unplanned readmission should be clarified with large-scale and well-designed prospective studies.
Limitations
The present systematic review had some limitations. First, we included only studies that focused on LDD. Therefore, surgeries for deformities, fractures, and spinal tumors were excluded. Also, based on our inclusion criteria, some newly developed procedures such as endoscopic spine surgery or robotic spine surgery were not included in our review.
Second, nearly half of the included studies were from the NSQIP databases, and the duplication of cohorts made the quantitative analysis of risk factors impracticable. In addition, studies from national databases or single institutions were included, and considerable variations in patient characteristics and sample sizes were observed. Third, we believe that short-term outcomes, including unplanned readmission, were influenced by the surgeon’s technical experience, which could represent a potential performance bias.
Conclusions
Through a systematic review, we identified the predictors of 30-day unplanned readmission in patients undergoing surgery for LDD. These findings may be used to identify patients at a higher risk of readmission, for whom caution should be exercised by clinicians.
Supplemental Material
Supplemental Material - Risk Factors for 30-day Unplanned Readmission following Surgery for Lumbar Degenerative Diseases: A Systematic Review
Supplemental Material for Risk Factors for 30-day Unplanned Readmission following Surgery for Lumbar Degenerative Diseases: A Systematic Review by Liang-Yi Chen, MD, Yu Chang, MD, Chia-En Wong, MD, Kuan-Yu Chi, MD, Jung-Shun Lee, MD, MSc, Chi-Chen Huang, MD, and Po-Hsuan Lee, MD in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.