
Abstract
Study Design
A retrospective study.
Objective
This study aimed to comprehensively evaluate the clinical outcomes of lateral lumbar interbody fusion (LLIF) as an indirect decompression technique for degenerative spondylolisthesis (DS) and concomitant degenerative lumbar spinal stenosis (DLSS) patients. We utilized the Japanese Orthopedic Association Back Pain Evaluation Questionnaire (JOABPEQ) to assess treatment success and its impact on patient's quality of life (QOL).
Methods
We included 124 patients who underwent LLIF. Pre- and postoperative JOABPEQ evaluations indicated treatment success. Subgroup analysis categorized patients’ perceptions of surgery as beneficial or non-beneficial.
Results
89% of patients (110/124) reported satisfaction with LLIF. Lateral lumbar interbody fusion achieved successful indirect decompression, increasing canal diameter and central canal area. Significant improvements occurred across all JOABPEQ domains, notably for low back pain, lumbar function, walking ability, social life function, and mental health. Patients who perceived the surgery as beneficial experienced fewer postoperative complications, lower numeric rating scale scores for pain relief, and greater functional outcome improvements compared to non-beneficial patients.
Conclusions
Our findings highlight the utility of JOABPEQ as a valuable and sensitive tool for assessing treatment effectiveness and patient-reported outcomes in DS and concomitant DLSS patients. Patients undergoing LLIF. The results affirm the favorable outcomes of LLIF as a surgical option for DLSS patients and emphasize the importance of considering patient perspectives when evaluating overall treatment success. The study provides valuable insights into the impact of indirect decompression on patients' QOL, supporting the effectiveness of LLIF as a minimally invasive technique for DLSS and DS management.
Keywords
Introduction
Degenerative Lumbar Spinal Stenosis (DLSS) with concomitant degenerative spondylolisthesis (DS) is a prevalent condition predominantly affecting the elderly population, characterized by chronic compression of nerve roots and dura mater due to osteoarthritic changes in the spine.1,2 Initial treatment for DLSS typically involves non-surgical approaches, effectively alleviating symptoms for most patients. However, surgical decompression and fusion of unstable segments may be recommended when conservative treatments fail to provide relief.3,4 There are two main categories of surgical options: direct decompression and fusion procedures and indirect decompression (ID) procedures. ID procedures involve the insertion of a large interbody cage through an abdominal approach, which helps restore disc height and spinal canal dimensions by stretching the ligaments.5,6 These techniques include anterior, lateral, and oblique lumbar interbody fusion.7-10 A previous systematic review and meta-analysis compared the clinical outcomes of patients with degenerative lumbar spinal stenosis and instability who underwent indirect or direct decompression and fusion techniques. 11 The study found that both treatment approaches yielded similar clinical outcomes in these patients. However, it should be noted that indirect decompression failure occurred in approximately 9%, highlighting the importance of patient-reported outcome measures (PROMs) in evaluating treatment success. 12
Assessing disability in DLSS individuals necessitates accessible, cost-effective instruments such as questionnaires, boasting robust psychometric properties and precise statistical values. 13 While the Roland–Morris Disability Questionnaire (RMDQ) and Oswestry Disability Index (ODI) have been clinically useful,14,15 limitations persist—RMDQ primarily addresses low back pain, while ODI raises concerns about response rates to the sex question in specific cultures. In this context, the Japanese Orthopedic Association Back Pain Evaluation Questionnaire (JOABPEQ) developed by Fukui et al. has emerged as an interesting alternative. 16 JOABPEQ’s five domains—low back pain, lumbar function, walking ability, social life function, and mental health—emphasize patient self-reporting, with the original version showing good reliability (kappa ≥.48).17,18 The JOABPEQ has been adapted and validated in Chinese, 19 Turkish, 20 Korean, 21 Thai, 22 , and Arabic languages. 23
Unlike traditional PROMs, JOABPEQ encompasses diverse back pain dimensions and their influence on patient's lives, including social aspects and psychological well-being. Linking PROMs to clinical outcomes comprehensively evaluates the impact of lateral lumbar interbody fusion (LLIF). However, only some studies explore JOABPEQ’s effectiveness post-LLIF surgery.24,25
Despite LLIF’s increasing popularity for DLSS treatment, research integrating PROMs remains crucial to gauging its efficacy. Thus, this study aims to investigate postoperative outcomes of indirect decompression through LLIF and assess patient satisfaction using JOABPEQ as a reliable and comprehensive PROM.
Methods
IRB Statement
We had the study protocol reviewed and approved by the Committee on Ethics and the Institutional Review Board of Tokai University School of Medicine, and the Profit Reciprocity Committee (23R-067). Because this study was retrospective, the requirement for informed consent was waived.
Included Patients
Following approval from the institutional review board, we conducted a retrospective review of medical records of patients diagnosed with DS and concomitant DLSS who underwent the LLIF with posterior fixation at a single academic institution between May 2018 and June 2022. In this study, patients with lumbar canal stenosis, including lumbar disc herniation, degenerative lumbar scoliosis, and synovial cysts, were considered DLSS. A total of 200 patients underwent this surgical treatment during the specified period. To be eligible for inclusion in the study, patients had to meet specific criteria, including age over 18, presence of low back pain, leg pain, and/or leg numbness, unresponsive to conservative treatment for at least three months prior to surgery, minimum one-year postoperative follow-up, and completion of the JOABPEQ.
Our criteria for fusion surgery were >3 mm of sagittal translation or >10° segmental angulation angle on dynamic radiographic evaluation or posterior widening of the disc space of >5° on a flexion radiograph. Exclusion criteria were a previous history of posterior lumbar fusion, significant lumbar scoliosis >30°, or inability to cooperate due to mental illness.
Comprehensive evaluations established preoperative diagnoses, including detailed medical history, neurological and radiographic examinations, myelograms, Computed tomography (CT) scans with myelography, and/or magnetic resonance imaging (MRI). The operating surgeon assessed the location of stenosis based on preoperative imaging studies.
Characteristics of the Subjects in the Present Study.
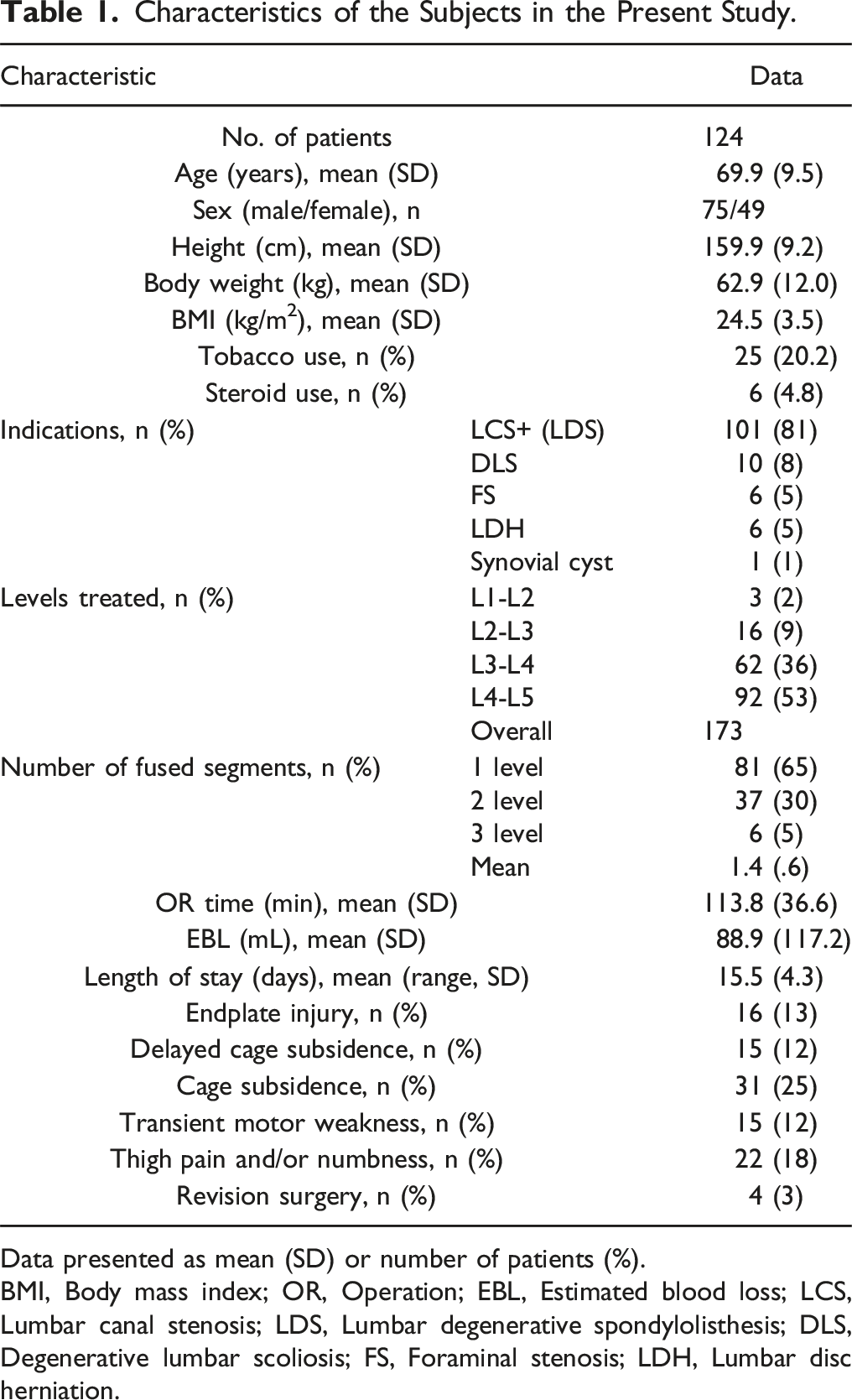
Data presented as mean (SD) or number of patients (%).
BMI, Body mass index; OR, Operation; EBL, Estimated blood loss; LCS, Lumbar canal stenosis; LDS, Lumbar degenerative spondylolisthesis; DLS, Degenerative lumbar scoliosis; FS, Foraminal stenosis; LDH, Lumbar disc herniation.
Furthermore, a postoperative satisfaction questionnaire was administered to the patients, inquiring whether they perceived the surgery as beneficial. The questionnaire offered three response options: “Yes,” “Neither yes nor no,” and “No.” Based on the responses, we categorized the patients into two groups: the “Beneficial” group (comprising those who responded “Yes”) and the “Non-beneficial” group (comprising those who responded “Neither yes nor no” or “No”). Subsequently, a comparative analysis was conducted between these two groups.
Surgical Technique
The basic procedure of our LLIF (ID) and posterior fixation was performed according to the surgical technique described by Ozgur et al., and as explained in our previous papers.26-35 Figure 1 presents a typical case. The procedure of LLIF was performed either by extreme lateral lumbar fusion (XLIF) or oblique lateral interbody fusion (OLIF). There was no clear indication to use either XLIF or OLIF; the decision was left to the surgeon. All patients underwent LLIF through a single incision, mini-open direct visualizing approach. The patient was placed in the lateral decubitus position, and an incision was made on the disc's skin to be treated. After approaching the disc, cage trials and insertions were performed. All LLIF segments were supplemented with percutaneous pedicle screw fixation with an intraoperative fluoroscopy or intraoperative CT navigation system. Typical case of indirect decompression by LLIF.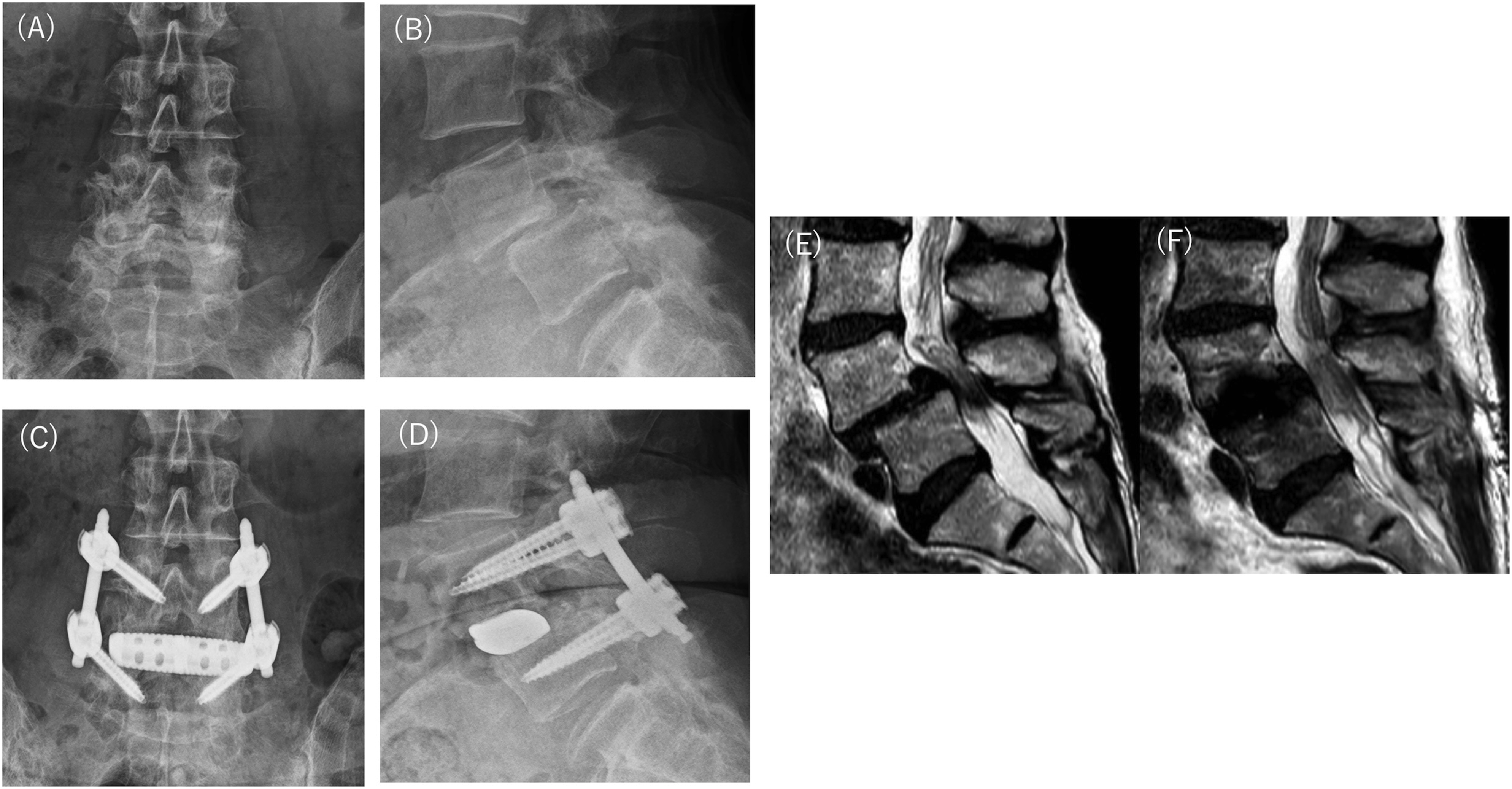
Radiographical Assessment
Standing full-length and lateral spine X-rays were obtained from the base of the skull to the proximal femur preoperatively and at one-year follow-up. We used standard measurements reported elsewhere to assess sagittal vertical axis (SVA), lumbar lordosis (LL, T12-S1), thoracic kyphosis (TK, T5-12), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), and PI-LL. We conducted preoperative and postoperative CT scans to assess cage positioning, identify any instrumentation failure, and detect potential endplate injuries. Furthermore, we utilized X-ray imaging to evaluate the occurrence of cage subsidence during the ongoing case.
We also performed an MRI to determine the midsagittal canal diameter (CD) and axial central canal area (CCA) of the thecal sac before and within two weeks after surgery. 28 This study used a 1.5 or 3.0 T MRI system (Ingenia or Achieva; Philips Medical Systems, Best, the Netherlands). Two reviewers, who are also authors, determined the average image measurements used for the analyses.
Numeric Rating Scale (NRS)
The NRS score indicates the severity of pain using a patient-graded 11-point scale from 0 to 10 (0 = no pain to 10 = worst pain or pain as bad as it could be). The pain intensity before and after the operation was assessed using NRS scores obtained for LBP (NRSLBP), leg pain (LP; NRSLP), and leg numbness (LN; NRSLN). 36 Improvements in symptoms were evaluated by the change in NRS (ΔNRS; 12 months postoperative NRS score– preoperative NRS score).
Japanese Orthopedic Association Back Pain Evaluation Questionnaire
Japanese orthopedic association back pain evaluation questionnaire is a patient-based measure of health-related quality of life (QOL) for patients with low back disorders. From the answers to 25 questions, the examiner calculates five functional scores (low back pain, lumbar function, walking ability, social life function, and mental health) using the provided formulas or by entering the data into the Excel file that is available on the website of the Japanese Orthopaedic Association (http://www.jssr.gr.jp/jssr_web/html/index.html). We evaluated the results of the JOABPEQ preoperatively and at one-year post-surgery. To evaluate the effectiveness, we considered two criteria: effectiveness rate and gained score. The patients were assessed based on a score increase of 20 points or more from post-surgery to pre-surgery, or a score of 90 points or more after treatment, indicating effectiveness. The effectiveness rate was calculated as the ratio of effective patients to the total number of patients examined. The gained score was analyzed by comparing the scores before and after surgery between the two groups.
Statistical Analysis
We calculated means with standard deviations for continuous variables and presented frequencies and percentages for categorical variables. Initially, we assessed the normal distribution of all continuous variables using the Kolmogorov-Smirnov test. Subsequently, we employed the Chi-squared test to examine the relationships between the two groups for categorical variables, conducted a t-test analysis of variance for continuous variables, and utilized the Mann-Whitney U test. Independent-sample t-tests were used for analyzing pre- and postoperative continuous variables. IBM SPSS Statistics software (version 23.0; IBM Corp., Armonk, New York, USA) was employed for data analysis. A P-value of less than .05 was considered statistically significant.
Results
The Five Domains of the Japanese Orthopaedic Association Backpain Evaluation Questionnaire (JOABPEQ) in All Patients From Preoperative to Postoperative Surgery: Low Back Pain, Lumbar Function, Walking Ability, Social Life Function, and Mental Health.
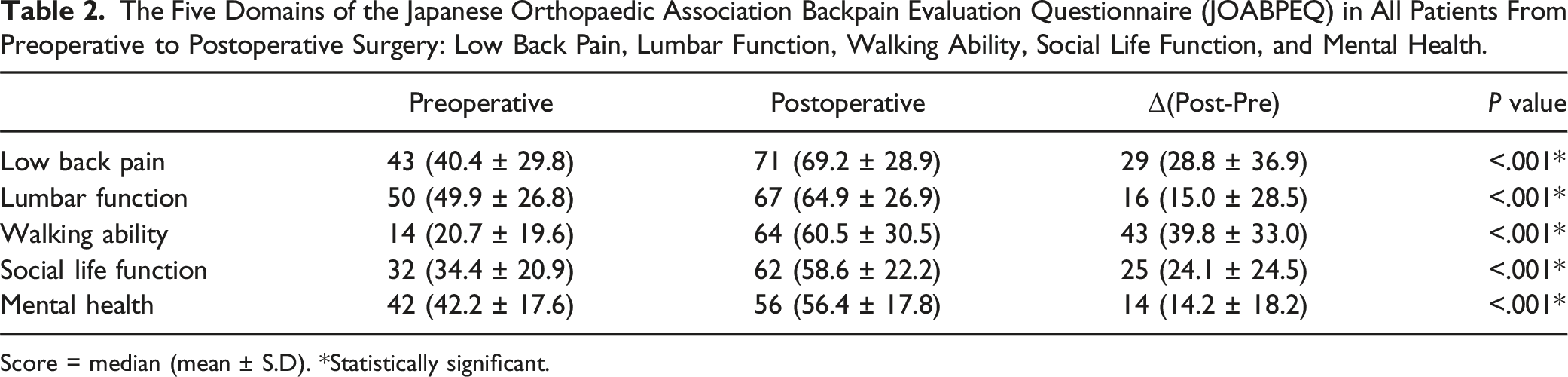
Score = median (mean ± S.D). *Statistically significant.
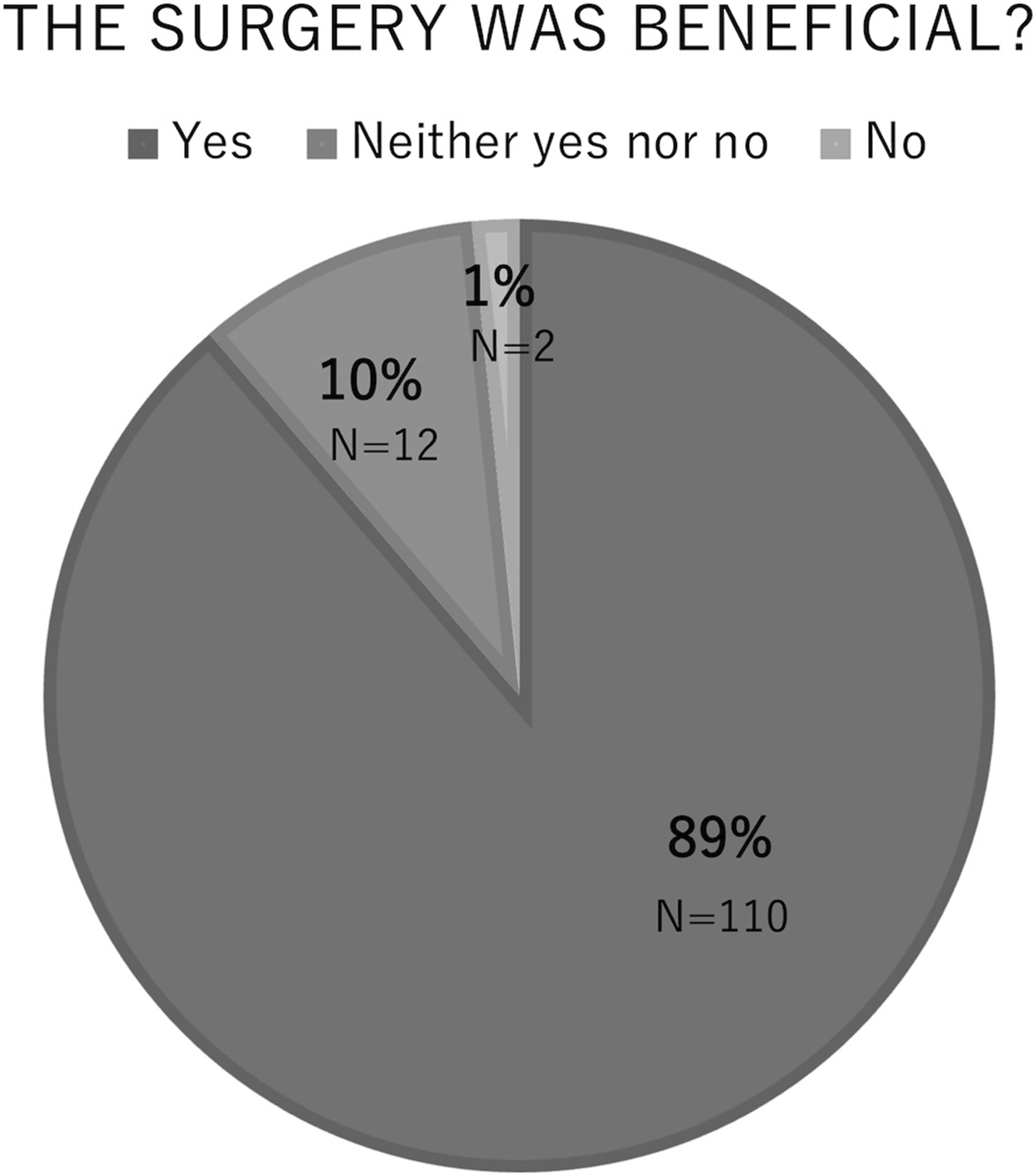
Patient satisfaction survey during postoperative follow-up.
Comparison of Two Groups.
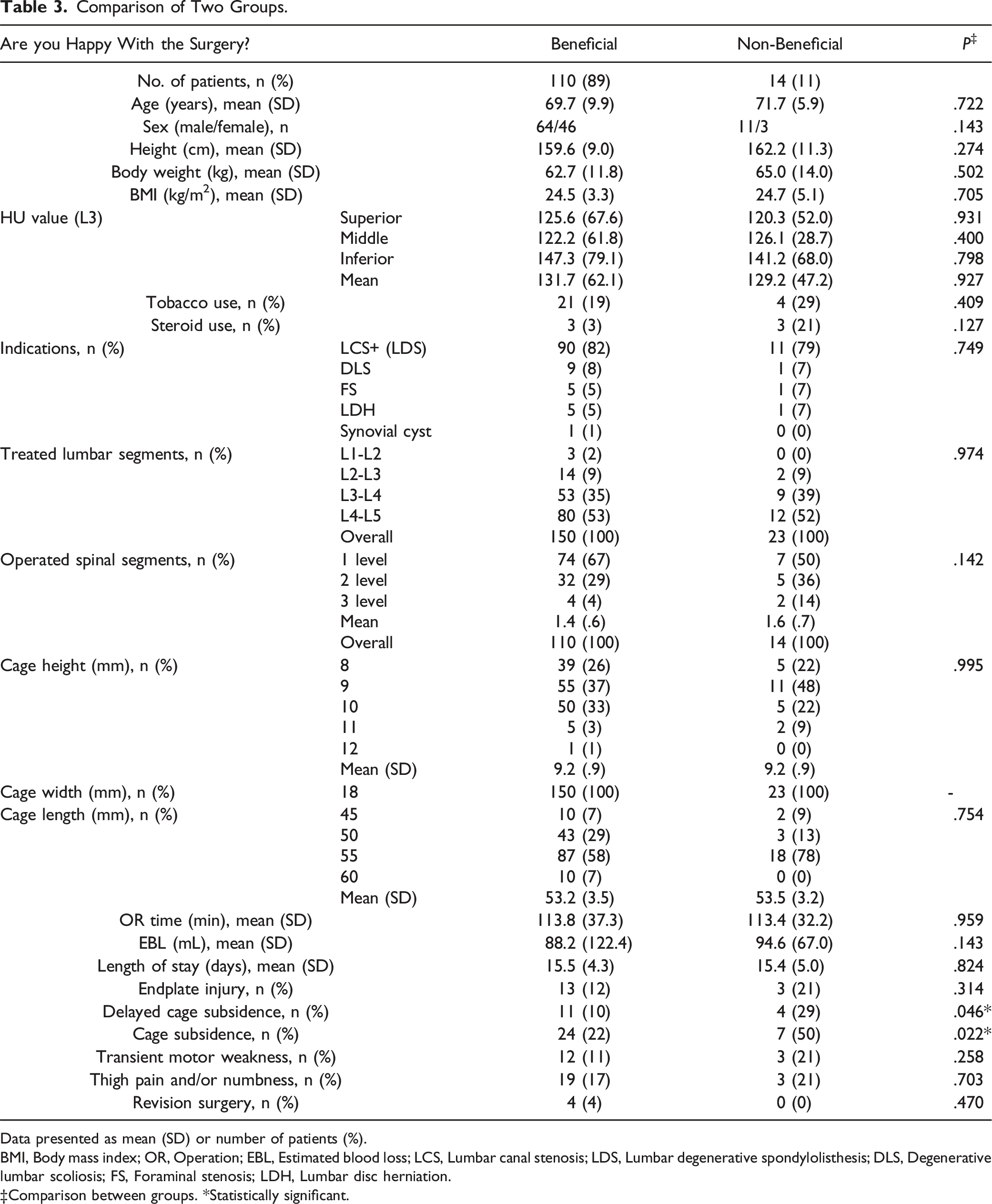
Data presented as mean (SD) or number of patients (%).
BMI, Body mass index; OR, Operation; EBL, Estimated blood loss; LCS, Lumbar canal stenosis; LDS, Lumbar degenerative spondylolisthesis; DLS, Degenerative lumbar scoliosis; FS, Foraminal stenosis; LDH, Lumbar disc herniation.
‡Comparison between groups. *Statistically significant.
Radiographic Measures-Canal Dimension (Canal Diameter and Central Canal Area of Dural Sac) Changes Evaluated on Pre-and Postoperative MRI.
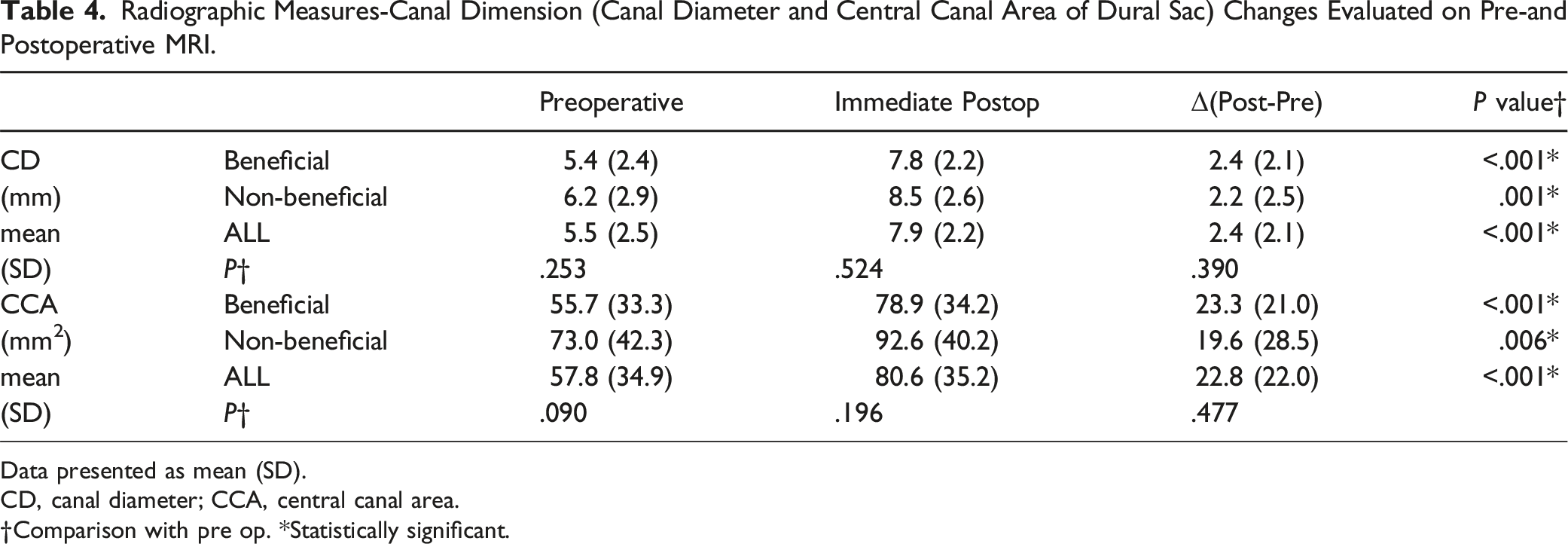
Data presented as mean (SD).
CD, canal diameter; CCA, central canal area.
†Comparison with pre op. *Statistically significant.
Preoperative, Postoperative, and Change From Pre-to Postoperative Sagittal Measurements.
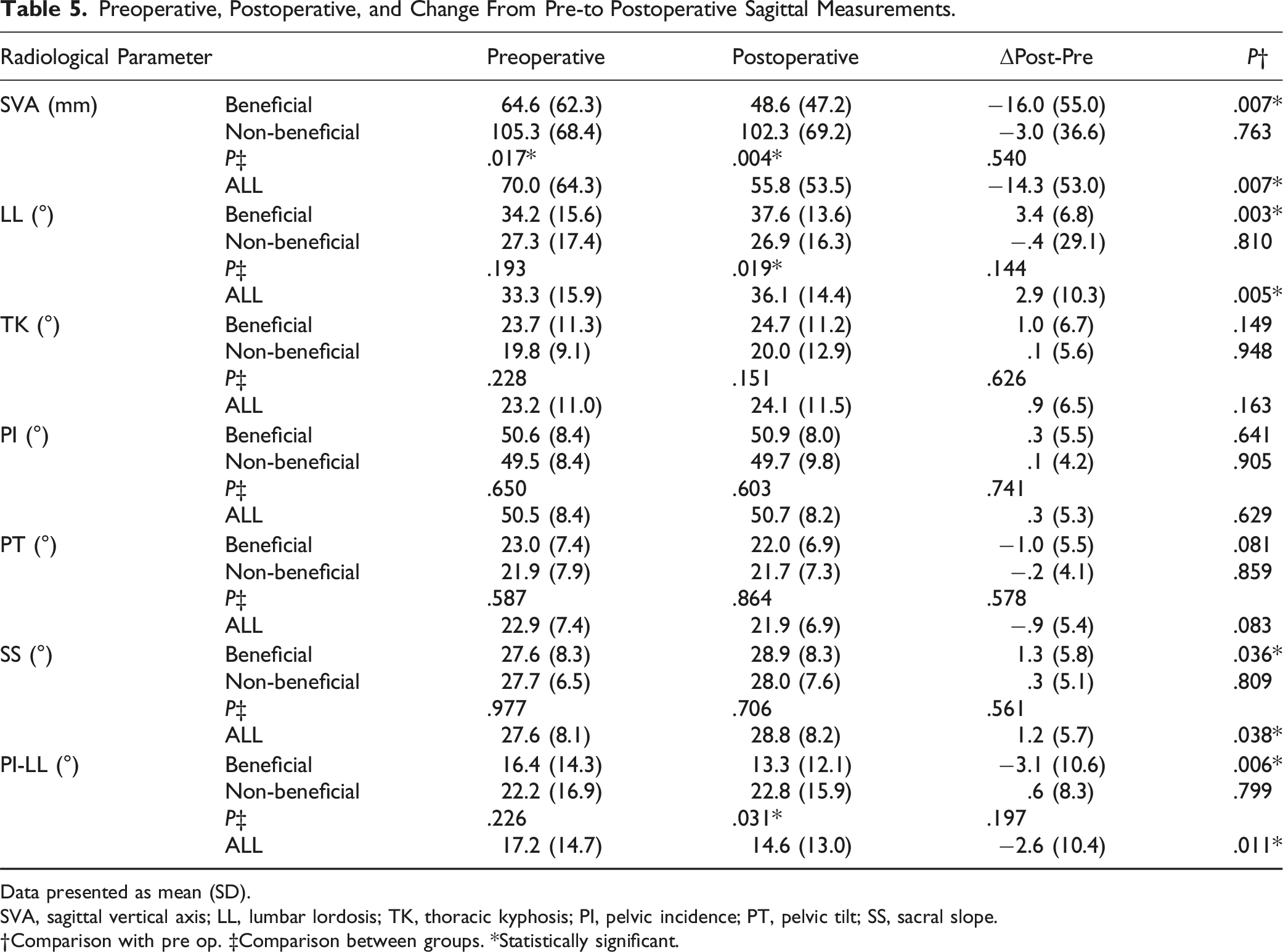
Data presented as mean (SD).
SVA, sagittal vertical axis; LL, lumbar lordosis; TK, thoracic kyphosis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope.
†Comparison with pre op. ‡Comparison between groups. *Statistically significant.
Two-Group Comparison Pre and Postoperative JOABPEQ. (A) Two-Group Comparison of Effective rate. Number of Improved Patients/Number of patients (Effective Rate). (B) Two-Group Comparison of Gained Score (Post-pre Score).
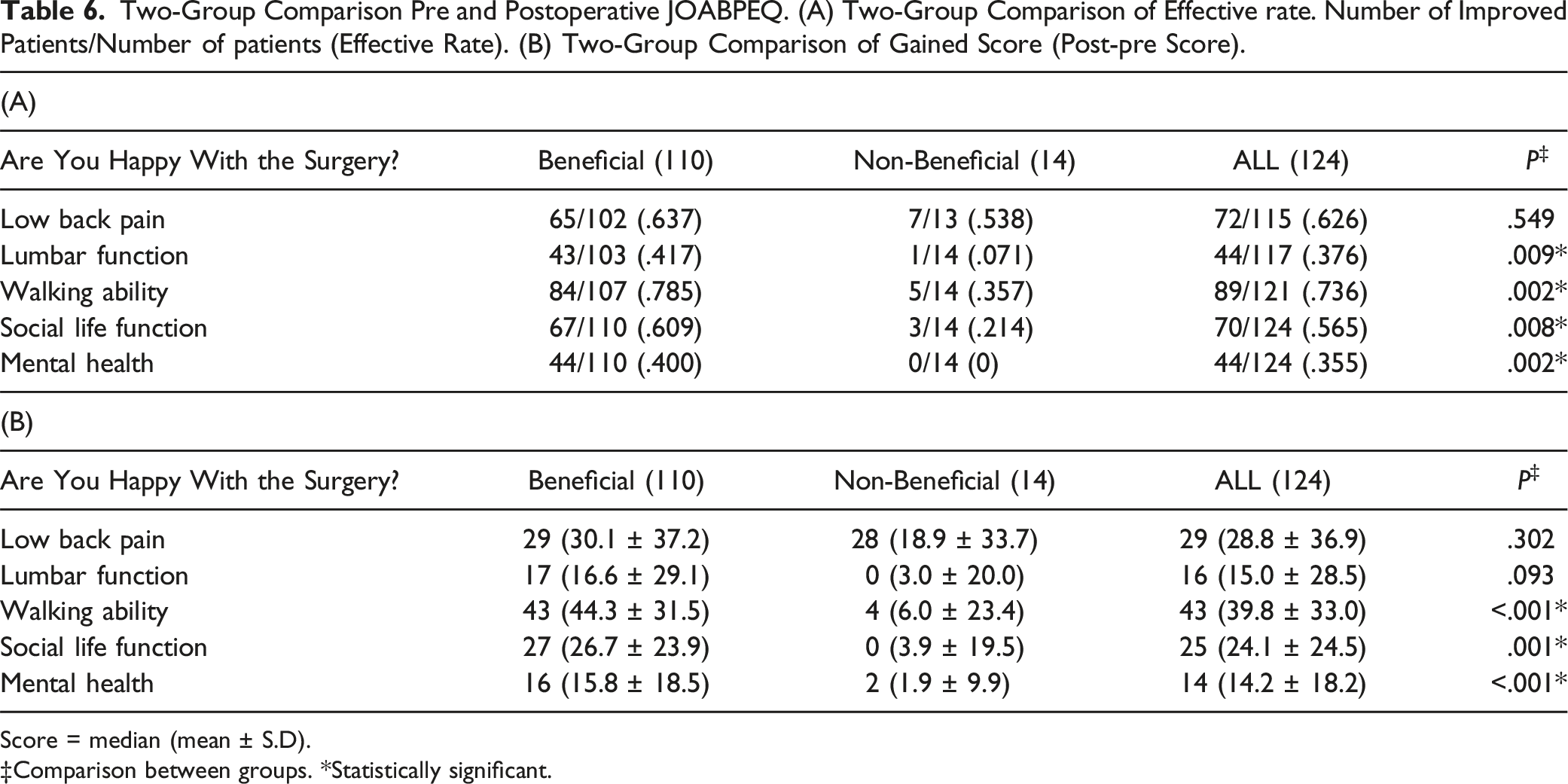
Score = median (mean ± S.D).
‡Comparison between groups. *Statistically significant.
Correlation Analysis Showing Spearman’s Correlation Coefficient (r) Between Each JOABPEQ Domain.
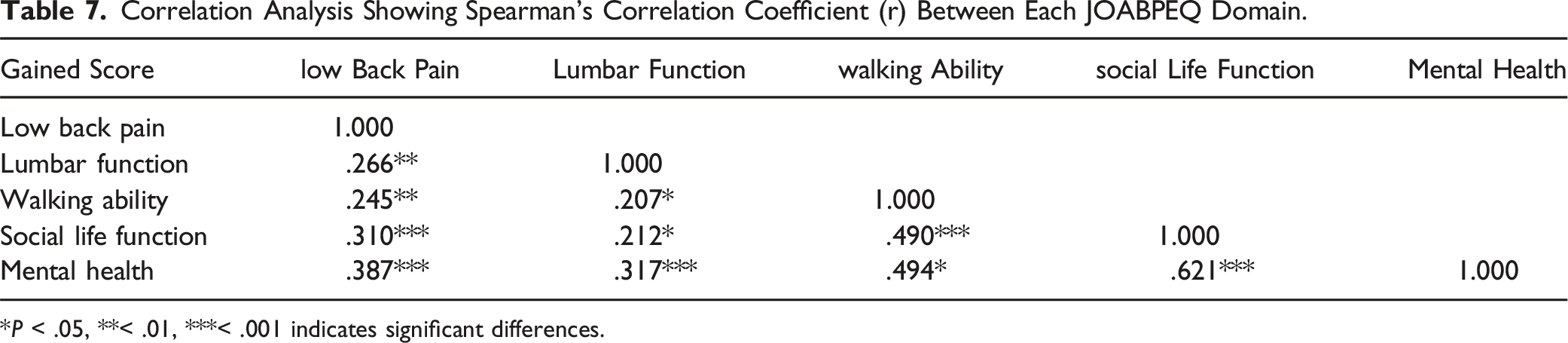
*P < .05, **< .01, ***< .001 indicates significant differences.
Correlation Analysis Showing Spearman’s Correlation Coefficient (r) Between ΔSVA, ΔLL, ΔPI-LL, and Each JOABPEQ Domain.
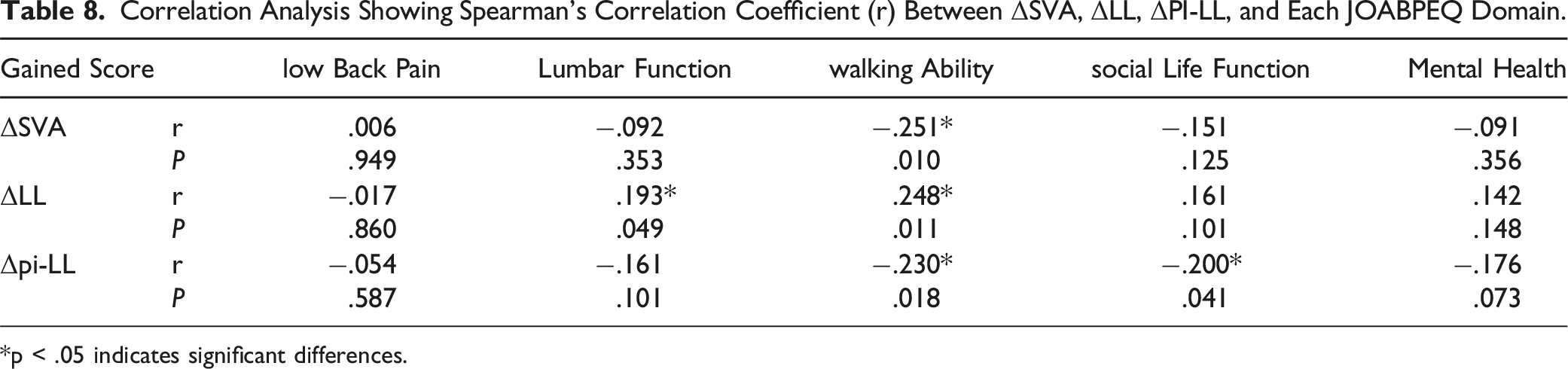
*p < .05 indicates significant differences.
Pain Intensity for Each Group.
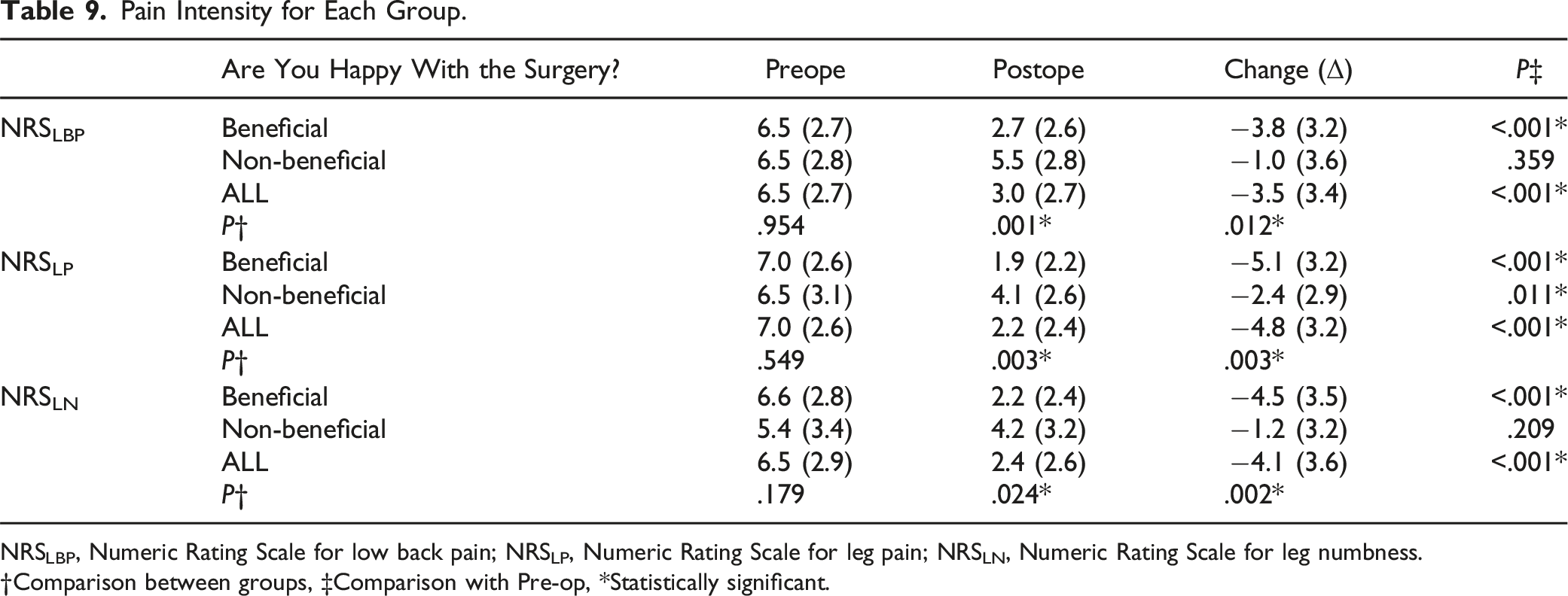
NRSLBP, Numeric Rating Scale for low back pain; NRSLP, Numeric Rating Scale for leg pain; NRSLN, Numeric Rating Scale for leg numbness.
†Comparison between groups, ‡Comparison with Pre-op, *Statistically significant.
These results underscore the multifaceted impact of LLIF surgery on various domains, revealing notable correlations between functional improvements and patient-reported outcomes. The findings further emphasize the significance of patient perceptions and satisfaction as integral components in evaluating the effectiveness of LLIF for DLSS.
Discussion
Degenerative lumbar spinal stenosis with concomitant DS primarily affects older individuals, resulting in chronic nerve root and dura mater compression due to osteoarthritic changes in the spine. When conservative treatments fail, surgical decompression and fusion are necessary. US clinical guidelines for DLSS with DS recommend decompression alone and decompression plus fusion, though controversy exists. Many surgeons consider laminectomy and fusion with added instrumentation as the gold standard. 37 Our study aimed to evaluate outcomes of indirect decompression using LLIF and employed the JOABPEQ as a PROM to assess treatment success.
The JOABPEQ assesses pain-related functional and psychological perspectives, comprehensively evaluating QOL regarding low back pain and lumbar function. A gain of ≥20 points on the JOABPEQ is considered a clinically significant improvement. 38 Our previous study reported significant pain relief one year after LLIF surgery, regardless of the preoperative pain profile. 36 Additionally, Nakashima et al. documented that indirect decompression with LLIF enabled meningeal sac expansion within six months after surgery, continuing gradually until two years post-surgery. 24
We utilized MRI measures to assess the effectiveness of indirect decompression using LLIF, revealing significant improvements. The CD and CCA were significantly improved from preoperative measures.
Furthermore, all domains of the JOABPEQ, including low back pain, lumbar function, walking ability, social life function, and mental health, exhibited remarkable improvements at the one-year follow-up. Moreover, all JOABPEQ domains improved remarkably after one year, including low back pain, lumbar function, walking ability, social life function, and mental health. Notably, preoperative walking ability scores were lowest at 14 points, suggesting surgery to address walking dysfunction.
Interestingly, 89% of the patients reported a more satisfactory outcome and potential QOL improvements following indirect lumbar decompression with LLIF. Comparing patients who reported beneficial surgery with those who were dissatisfied showed significant differences. While there were no significant differences in baseline demographics and perioperative variables between the two groups, certain complications showed significant differences. Specifically, delayed cage subsidence and cage subsidence were more prevalent in the non-beneficial group, indicating that implant-related issues may influence treatment outcomes and patient satisfaction. LLIF, a commonly employed minimally invasive technique for lumbar interbody fusion, effectively addresses conditions such as spondylolisthesis, spinal stenosis, and adult spinal deformity in patients.39-44 Using large interbody cages in LLIF improves radiography, resulting in indirect thecal sac decompression.45,46
However, there is a need for more studies investigating the indirect decompression achieved through LLIF using JOABPEQ as a PROM method. Despite some studies reporting improvements in JOABPEQ scores after surgery for patients undergoing indirect decompression with LLIF,24,25,47,48 no specific analysis has been conducted for each domain. Previous research by Nakashima et al. aligns with our findings. They also compared PLIF and LLIF, finding no significant JOABPEQ score difference. 25 A recent systematic review has reported that the lateral approach can lead to significant radiological correction and similar clinical improvement compared to the posterior approach while reducing surgical blood loss and postoperative complications. 49
Our study demonstrated that while both groups showed similar effectiveness rates in the low back pain domain, significant differences were observed in the domains of lumbar function, walking ability, social life function, and mental health. This suggests that improvements in these domains might have a greater impact on patient satisfaction and perceived treatment success. The strong correlation between social function and mental health highlights the interconnectedness of these domains. In the non-beneficial group, 14 out of 14 (100%) showed no benefit in the mental health domain. Enhancing a patient’s social life function might positively influence their mental health, contributing to overall well-being and satisfaction with the surgical outcome. Therefore, addressing social aspects during treatment and postoperative care could improve patient-reported outcomes. Using JOABPEQ allowed us to assess treatment success from various pain-related functional and psychological perspectives, providing a comprehensive understanding of the patient's QOL after surgery.
Notably, the NRS scores for low back pain, leg pain, and leg numbness all improved after surgery, indicating successful pain relief for most patients. However, postoperative improvement in low back pain and leg numbness was not statistically significant in the non-beneficial group. This finding emphasizes the importance of understanding factors contributing to treatment success and tailoring interventions to address individual patient needs. Furthermore, we observed that improvements in leg pain and walking ability appeared to be more significant determinants of a good outcome than lumbar functioning or low back pain improvement in this study. While lumbar functioning and improvement in low back pain are essential aspects of treatment evaluation, alleviating leg pain and improving walking ability may impact overall patient satisfaction and perceived treatment success. Moreover, the influence of preoperative SVA on alignment and satisfaction was notable. Patients with high preoperative SVA had low treatment satisfaction. This may also affect walking ability, but unfortunately, it is challenging to determine if this result is due to pain or whether a large SVA affected walking ability.
The potential reasons for these differences warrant further investigation and could be the focus of future research. For example, the resolution of leg pain and improved walking ability directly impact a patient’s ability to engage in daily activities and enhance their overall quality of life. Additionally, the interaction between leg pain and walking ability may be crucial in determining patients’ perceived functional improvement and satisfaction with the surgical outcome.
One of the limitations of our study is its retrospective design, which may introduce potential selection bias and confounding factors. As we utilized pre-existing data, unaccounted variables could have influenced our results. Our study lacks a comprehensive assessment of bone fusion using CT scans in all cases. The inability to evaluate the impact of cage subsidence on bone fusion in certain cases and the challenge of categorizing patients with multi-level LLIF surgeries regarding fusion status limited our ability to explore this critical aspect of our research fully. Additionally, it is important to address potential bias in our study.
One potential source of bias lies in evaluating canal dimension improvements, which the study authors conducted. While we attempted to minimize bias through standardized assessment methods, the lack of an independent reviewer for this aspect may have introduced some subjectivity into the measurements.
Another limitation is the relatively small sample size utilized in our study. This may restrict the generalizability of our findings to a broader population. A larger cohort would provide increased statistical power and enhance the external validity of our results. To address these limitations and improve the quality of future research, we would like to consider prospective study designs with larger cohorts to obtain more robust evidence. Additionally, conducting long-term follow-up assessments would be valuable for evaluating the durability of treatment outcomes and addressing potential confounding factors or biases.
Despite these limitations, our study provides valuable insights into the effectiveness of LLIF and the use of JOABPEQ as a PROM for assessing indirect decompression. The significant improvements in specific domains of JOABPEQ, such as lumbar function, walking ability, social life function, and mental health, suggest that enhancing these aspects during treatment and postoperative care could lead to better patient-reported outcomes and satisfaction.
For future research, investigations into patient-reported outcomes beyond one year post-surgery and multi-center collaborations could further strengthen the evidence base and enhance the generalizability of our findings. Additionally, exploring the influence of various patient factors, such as age, comorbidities, and preoperative pain levels, on treatment outcomes and QOL could provide a more comprehensive understanding of the DLSS management process.
Conclusions
In conclusion, our study demonstrates that indirect decompression using LLIF is an effective treatment option for patients with DS and concurrent DLSS, significantly improving patient-reported outcomes and radiographic measures. This study represents the first comprehensive evaluation of the JOABPEQ across each domain following indirect decompression using LLIF. Employing the JOABPEQ as a PROM comprehensively assesses the success of the treatment and patient satisfaction. Furthermore, focusing on social life function and mental health domains could further enhance patient-reported outcomes.
Footnotes
Author’s Note
This study, including any part of it, does not have any prior or duplicate submissions or publications elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.