
Abstract
Study Design:
Systematic review.
Objective:
Indirect decompression via lateral lumbar interbody fusion (LLIF) can ameliorate central and foraminal lumbar stenosis. In severe central stenosis, additional posterior direct decompression is utilized. The aim of this review is to synthesize existing literature on these 2 techniques and identify significant differences in outcomes between isolated indirect decompression via LLIF and combined indirect decompression supplemented with direct posterior decompression.
Methods:
A database search algorithm was utilized to query MEDLINE, COCHRANE, and EMBASE to identify literature reporting adult decompression study groups that involved an oblique or lateral fusion approach through September 2020. Improvement in outcomes measures and complication rates were pooled and tested for significance.
Results:
A total of 110 publications were assessed with 15 studies meeting inclusion criteria, including 557 patients and 1008 levels. Mean age was 63.1 years with BMI of 27.5 kg/m2. For the combined indirect and direct decompression cohort, lumbar lordosis (LL) increased 133.9%, from 22.8o to 48.7o, while the indirect decompression cohort LL increased 8.9%, from 41.9o to 45.5o. Difference in LL improvement between cohorts was insignificant (P > .05). Oswestry Disability Index (ODI) decreased from 36.5 to 19.4 in the combined indirect and direct decompression cohort, and from 44.4 to 23.1 in the indirect decompression cohort. ODI reduction was insignificant (P = .053).
Conclusions:
Prior studies of both indirect decompression as well as combined indirect and direct decompression of lumbar spine stenosis are limited by small samples, heterogeneous populations, and lack of direct comparisons. Both procedures result in improved function and pain postoperatively with direct decompression restoring more lordosis in patients with worse preoperative alignment.
Keywords
Introduction
Indirect decompression via minimally invasive lateral lumbar interbody fusion (LLIF) can be utilized to treat both foraminal stenosis and mild central stenosis secondary to various degenerative spinal pathologies.1-5 Although direct visualization of the dural sac or nerve roots is not performed in LLIF, neural elements are decompressed indirectly by increasing disc height, foraminal area, and central canal area after placement of an interbody cage. Iterations of LLIF, which have been patented and described in the literature, include direct lateral interbody fusion (DLIF, Medtronic Sofamore Danek, Minneapolis, Minnesota, USA) and extreme lateral interbody fusion (XLIF, NuVasive, Inc., San Diego, California, USA). 6 Oblique lumbar interbody fusion (OLIF) enables achievement of the same therapeutic aims of LLIF through use of a very similar surgical approach developed to obviate the need for psoas muscle dissection, thereby minimizing risk for both post-operative leg weakness and symptoms secondary to iatrogenic genitofemoral nerve injury. 7 Together, lateral and oblique spine fusion have grown in popularity by avoiding the drawbacks of anterior interbody lumbar fusion (ALIF), a procedure which requires a significantly larger surgical incision and great vessel mobilization to enable visualization of the vertebral bodies, while yielding improved clinical outcomes and good fusion rates.1-8
In cases of severe central stenosis, additional posterior direct decompression may be performed in conjunction with LLIF.9-11 Resection of posterior compressive structures such as bony osteophytes, facet joints, and ligamentum flavum cannot be performed via the lateral approach to the lumbar spine.12,13 Today, posterior decompression techniques may be performed using midline open, mini-open, or minimally invasive surgery (MIS) techniques. MIS posterior lumbar decompression utilizes a tubular retractor system to minimize dissection and destabilization of posterior midline structures such as the paraspinal musculature and stabilizing ligaments.1,2,14
The aim of this review is to analyze the existing literature and identify any significant differences in outcomes or complications between isolated indirect decompression from lateral interbody fusion and combined indirect decompression with additional direct posterior decompression surgery. As this type of analysis has not yet been performed, better understanding of the relative outcomes of indirect decompression and indirect decompression with additional direct posterior decompression may allow for an expansion of indications for isolated lateral interbody fusion as well as a better understanding for when additional posterior decompression is warranted.
Methods
Protocol
Methodological workflow for this review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes Protocols (PRISMA-P) approach. 15
Eligibility Criteria, Information Sources, and Search Strategy
A database search algorithm was utilized to individually query 3 databases (MEDLINE, COCHRANE, and EMBASE) and identify all relevant literature reporting decompression study groups that involved a lateral or oblique spinal fusion approach. The cutoff date for publications examined for inclusion was September 1, 2020. The database search algorithm utilized Boolean logic to search for literature which included the following terminology and their associated acronyms: “lateral lumbar interbody fusion,” “oblique lumbar interbody fusion,” “indirect decompression,” “direct decompression,” “posterior decompression,” “laminectomy,” and “laminotomy.” Excluded from the query results were all non-human, cadaveric, and non-English literature.
Study Selection
All publications assessed in this review were collected and managed using a systematic review platform (Covidence Software, Veritas Health Innovation, Melbourne, Australia, available at www.covidence.org). These publications were examined at the title and abstract level independently by 3 reviewers (AMS, KWM, KAS). Full manuscript review was conducted by 2 reviewers (MKM and AMS). Discordance of study inclusion recommendations between the independent reviewers were reviewed by the senior author (SI) who individually examined each disagreement and finalized the study inclusion list. Table 1 defines the full criteria used to screen the 110 publications considered in this review for inclusion and exclusion.
Review Inclusion/Exclusion Criteria.
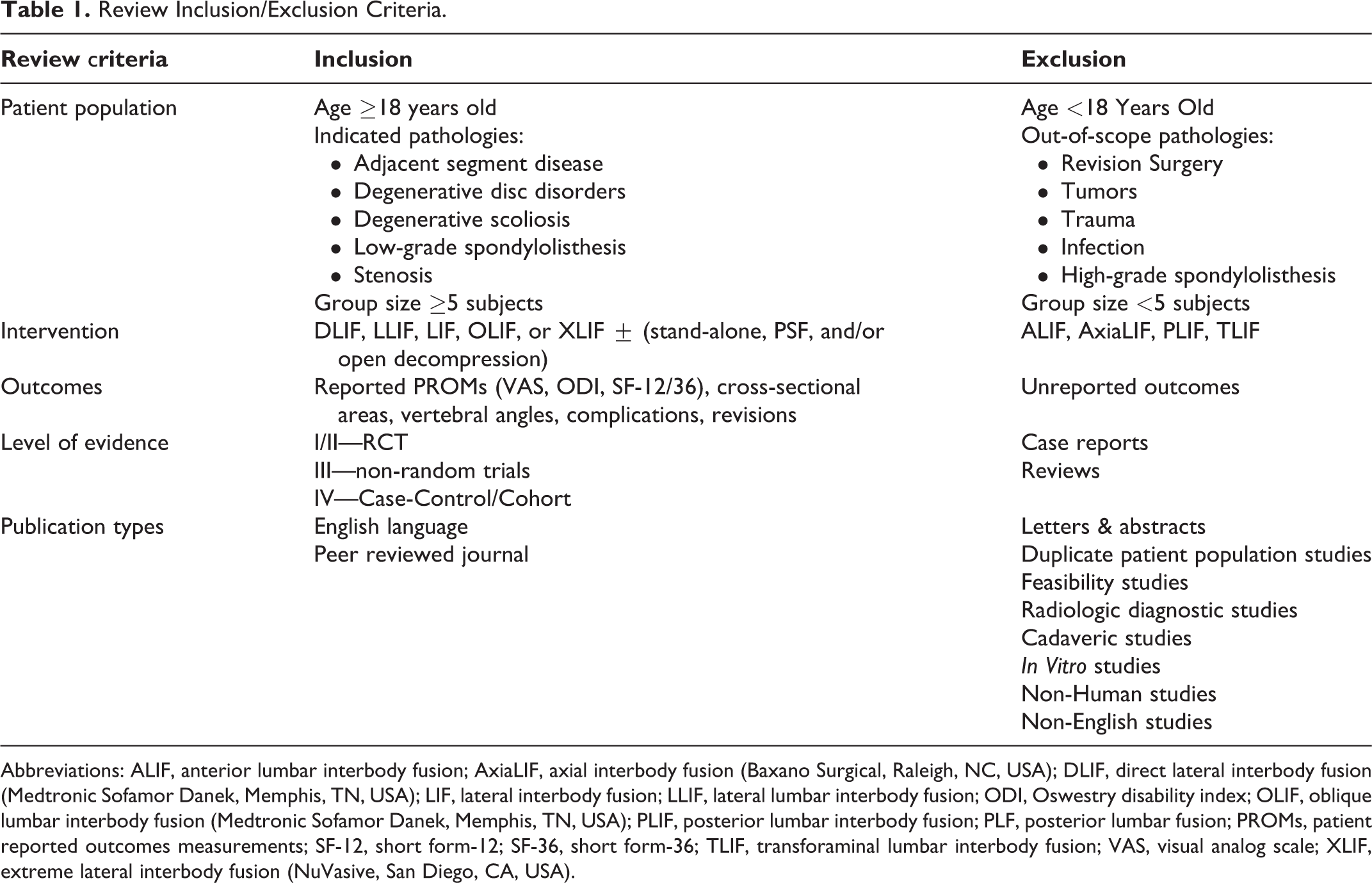
Abbreviations: ALIF, anterior lumbar interbody fusion; AxiaLIF, axial interbody fusion (Baxano Surgical, Raleigh, NC, USA); DLIF, direct lateral interbody fusion (Medtronic Sofamor Danek, Memphis, TN, USA); LIF, lateral interbody fusion; LLIF, lateral lumbar interbody fusion; ODI, Oswestry disability index; OLIF, oblique lumbar interbody fusion (Medtronic Sofamor Danek, Memphis, TN, USA); PLIF, posterior lumbar interbody fusion; PLF, posterior lumbar fusion; PROMs, patient reported outcomes measurements; SF-12, short form-12; SF-36, short form-36; TLIF, transforaminal lumbar interbody fusion; VAS, visual analog scale; XLIF, extreme lateral interbody fusion (NuVasive, San Diego, CA, USA).
Data Collection Process and Data Items
Each study group included in this review was assessed across 110 individually extracted data points. Data extracted from each study spanned the following categories: surgical approach, group size, levels, patient demographics, radiological assessment approach, as well as all reported surgical and clinical outcomes.
Risk of Bias Assessment
The Newcastle-Ottawa Scale (NOS) was utilized to assess the methodological quality of all publications included in this review. Several aspects were considered: subject selection (patient diagnoses and study population source), data comparability, radiological assessment approach (radiograph vs. advanced imaging), follow-up length (months), and loss-to-follow-up rate.
Summary Measures and Synthesis of Results
Statistical analysis involved examination of data for significant difference across 2 study cohorts (indirect and direct decompression) for the included study groups summarized in this review. Means reported in this review were pooled with weighting by group size. Meta-analysis was determined to not be feasible in this review because of relatively small sample sizes as well as a high degree of variability in outcomes assessment methodology across the included studies. Statistical difference was assessed using Student t tests (two-tail, unpaired, unequal variance assumed) with secondary post-hoc Tukey’s HSD testing for validation. Significance was assigned if P < .05. All data analysis was completed using Microsoft Excel 365 Version 2011 (Microsoft Corporation, Redmond, Washington, USA).
Results
A total of 79 publications were assessed for inclusion at the title and abstract level after excluding 31 duplicate publications (Figure 1). Overall, 15 studies satisfied the inclusion criteria after full review. With regard to study design, there were 10 retrospective studies, 5 prospective studies, and no randomized control trials. Three studies analyzed lateral interbody fusion combined with additional direct posterior decompression surgery (direct cohort) across 42 patients and 161 vertebral levels (Table 2). Mean subject age was 67.2 ± 5.8 years, 76.3% were female, and the mean follow-up period was 15.6 ± 7.6 months (range, 6.0-21.0 months). Fifteen studies analyzed isolated indirect decompression approach across 557 patients and 1008 vertebral levels with a mean fusion rate of 95.1% ± 4.5% (range, 89.2%-100.0%). Mean subject age was 63.1 ± 11.6 years, 59.2% were female, and the mean follow-up period was 17.6 ± 9.6 months (range, 6.0-34.8 months). There was a statistically significant difference in age (P < .01) and female to male ratio (P < .01) between cohorts.
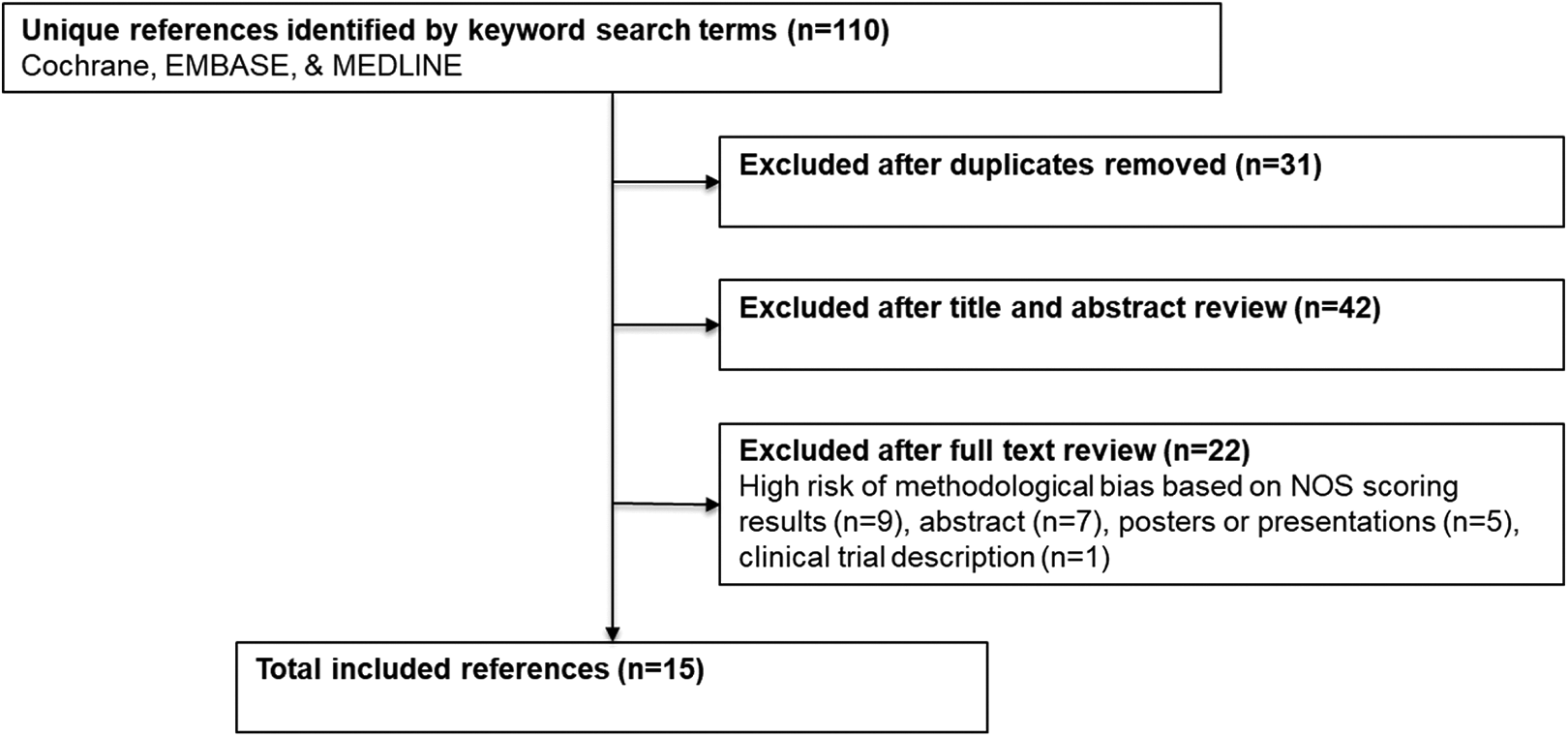
Workflow for identifying included references. The systematic review workflow utilized in this review closely followed the PRISMA-P best-practice recommendations.
Demographics of Included Studies.
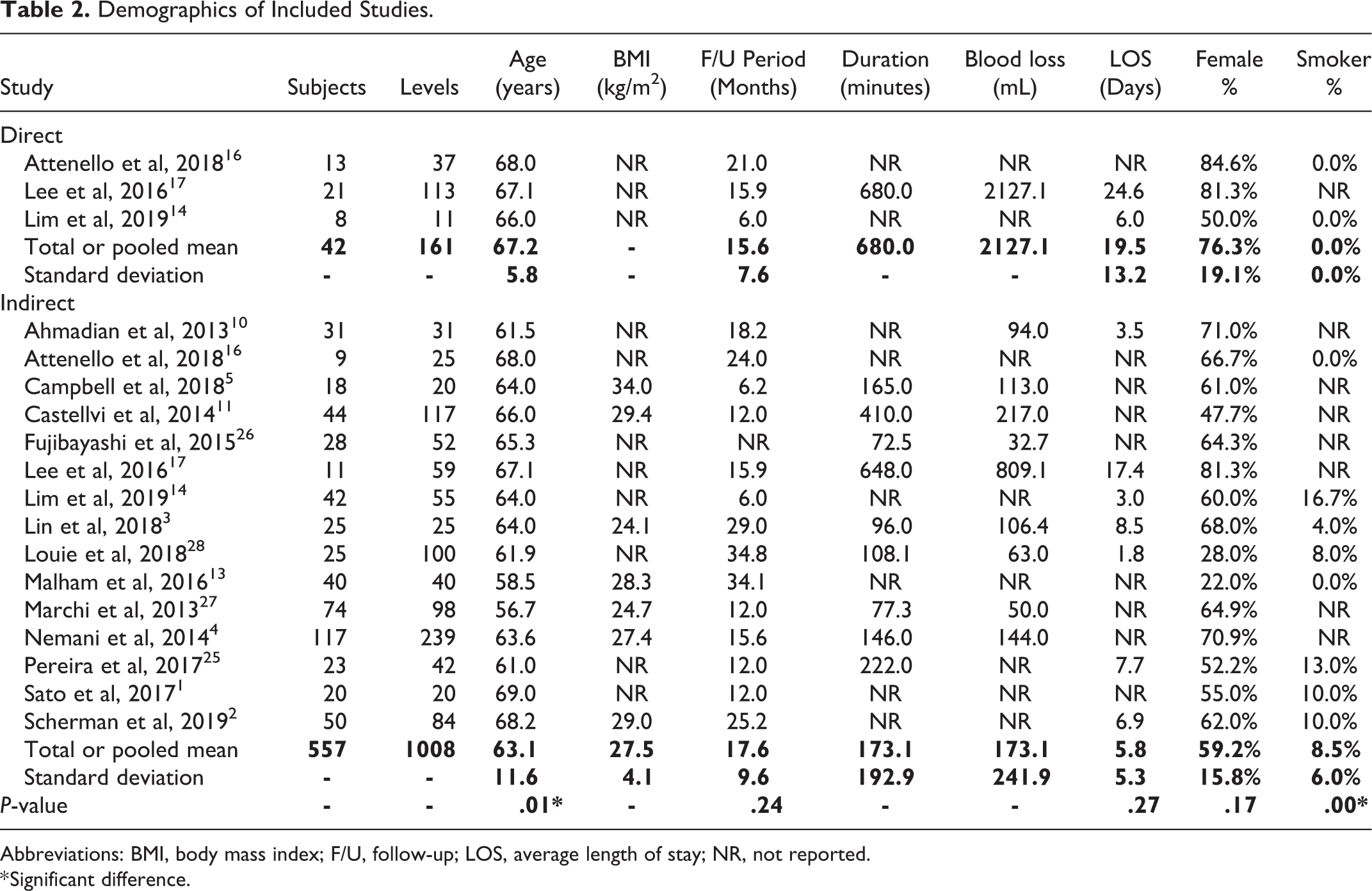
Abbreviations: BMI, body mass index; F/U, follow-up; LOS, average length of stay; NR, not reported.
* Significant difference.
Indication for surgical intervention and operative segment level varied across the included studies. For the direct decompression cohort, a diagnosis of adult degenerative scoliosis (ADS) was the primary indication in 86.4% of patients (Figure 2). For the indirect decompression cohort, stenosis was the most common diagnosis (36.1%), followed by spondylolisthesis (23.1%), degenerative disc disease (DDD, 20.6%), radiculopathy (12.4%), ADS (4.8%), and adjacent segment disorder (ASD, 2.2%). With respect to the indirect decompression cohort, the most commonly operated spinal segment level was L4-L5 (56.1%) followed by L3-L4 (27.2%), L2-L3 (12.6%), and L1-L2 (3.1%) (Figure 3). Publications reporting a combined direct and indirect decompression group did not report operative level data.
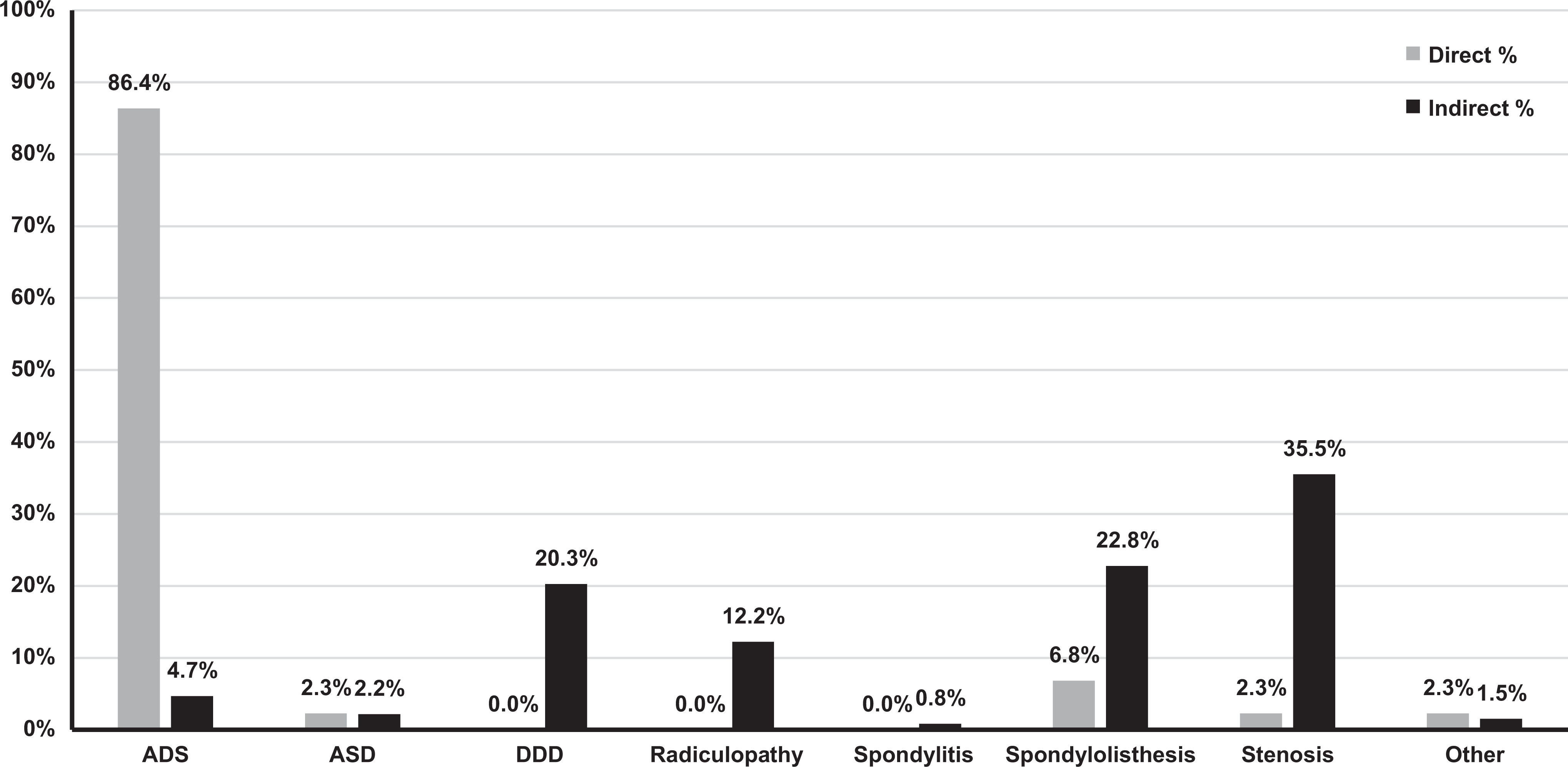
Percentage of cases by indication. ASD, adjacent segment disorder, ADS, adult degenerative scoliosis, DDD, degenerative disc disease. Indication of cases varied by decompression approach.
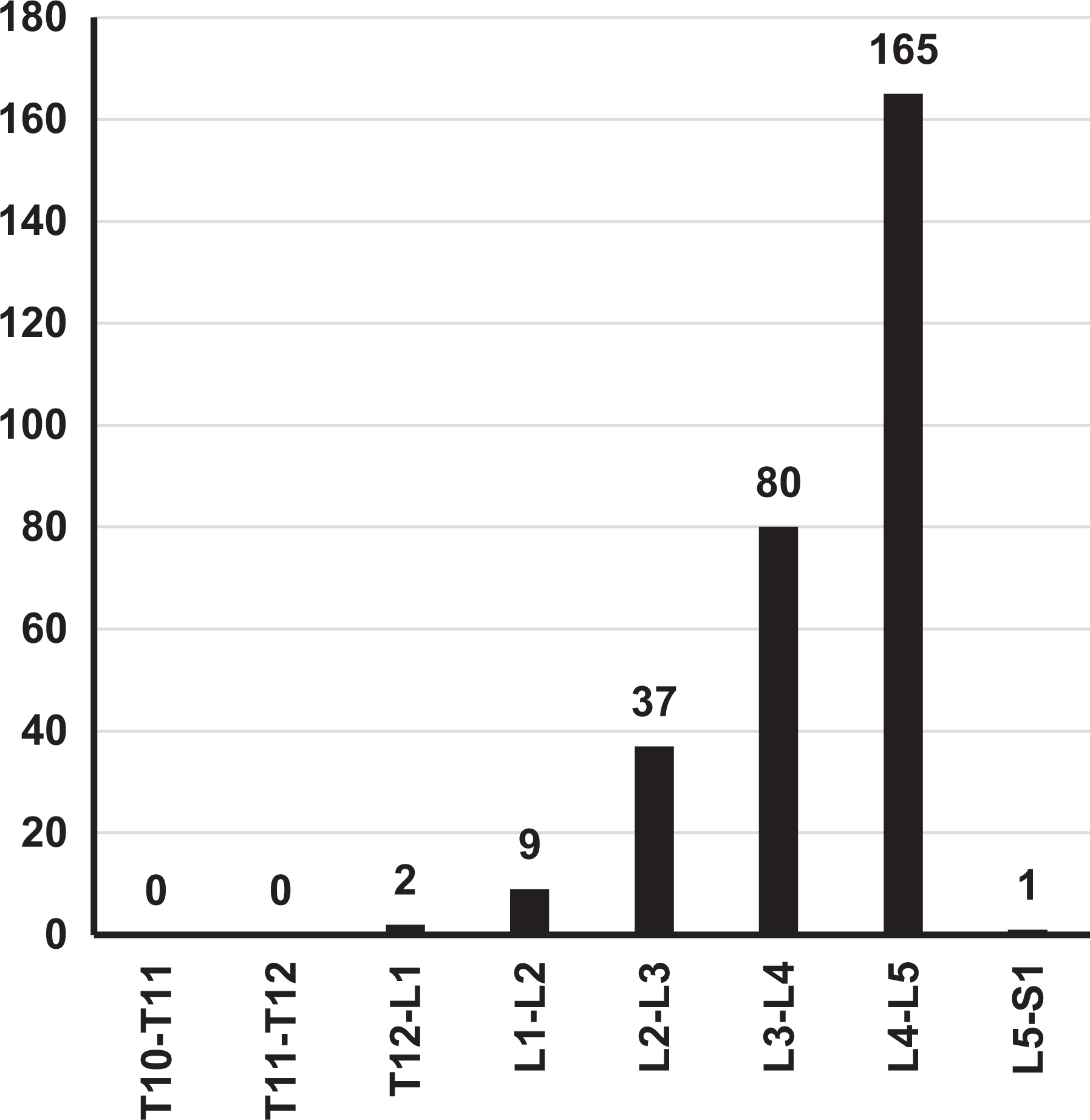
Indirect decompression operative spinal segment levels. Operative spinal segment levels were generally located in the lumbar spine, most frequently involving L4-L5.
Radiological outcomes of surgery were assessed utilizing radiographs in 11 out of 15 (73.3%) studies summarized by this review with the rest utilizing advanced imaging techniques (computed tomography [CT] or magnetic resonance imaging [MRI]). All 3 studies reporting direct decompression groups utilized radiographs.14,16,17 For the direct decompression cohort, lumbar lordosis (LL) increased by 133.9% from 22.8o to 48.7o (Table 3). For the indirect decompression cohort, LL increased by 8.9% from 41.9o to 45.5o. LL improvement difference between cohorts was insignificant (P > .05). Fusion rate was reported for only 1 of the 3 direct decompression groups (87.5%). 14 Pooled fusion rate reported for 9 indirect decompression groups was higher (95.1%); however, it was not possible to assess this difference for statistical significance.
Lumbar Lordosis Radiological Measurements Reported.
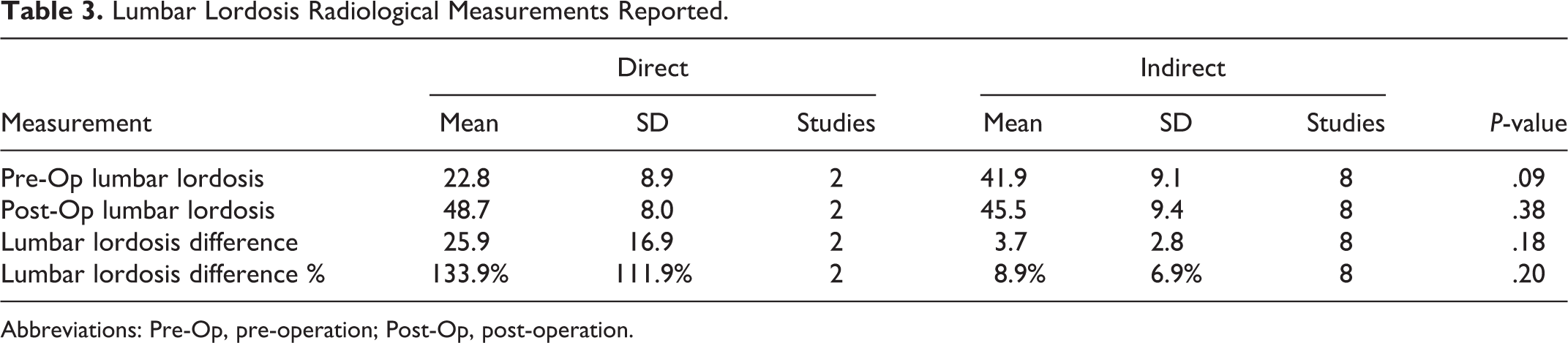
Abbreviations: Pre-Op, pre-operation; Post-Op, post-operation.
Patient reported outcome measures (PROMs) were reported using 10 individual scales across all 15 studies included in this review. The most consistently utilized PROM scales (≥2 studies) were considered for comparison across the indirect and direct decompression cohorts. Direct decompression Oswestry Disability Index (ODI) mean pre- and post-operative scoring decreased from 36.5 to 19.4 (Table 4). The indirect decompression ODI mean pre- and post-operative scoring decreased from 44.4 to 23.1. This difference in ODI improvement between groups was not statistically significant (P = .053). Mean decrease in Visual Analog Scale (VAS) back pain between pre- and post-operative scoring was 7.0 to 2.7 for the direct decompression cohort and 7.1 to 2.9 for the indirect decompression cohort This difference in VAS-back pain score improvement was also not statistically significant between groups (P = .46). VAS-leg pain reduction was from 4.9 to 2.3 for the direct decompression cohort and 6.8 to 2.2 for the indirect decompression cohort (P = .27).
Patient-Reported Outcomes Measures of Included Studies.
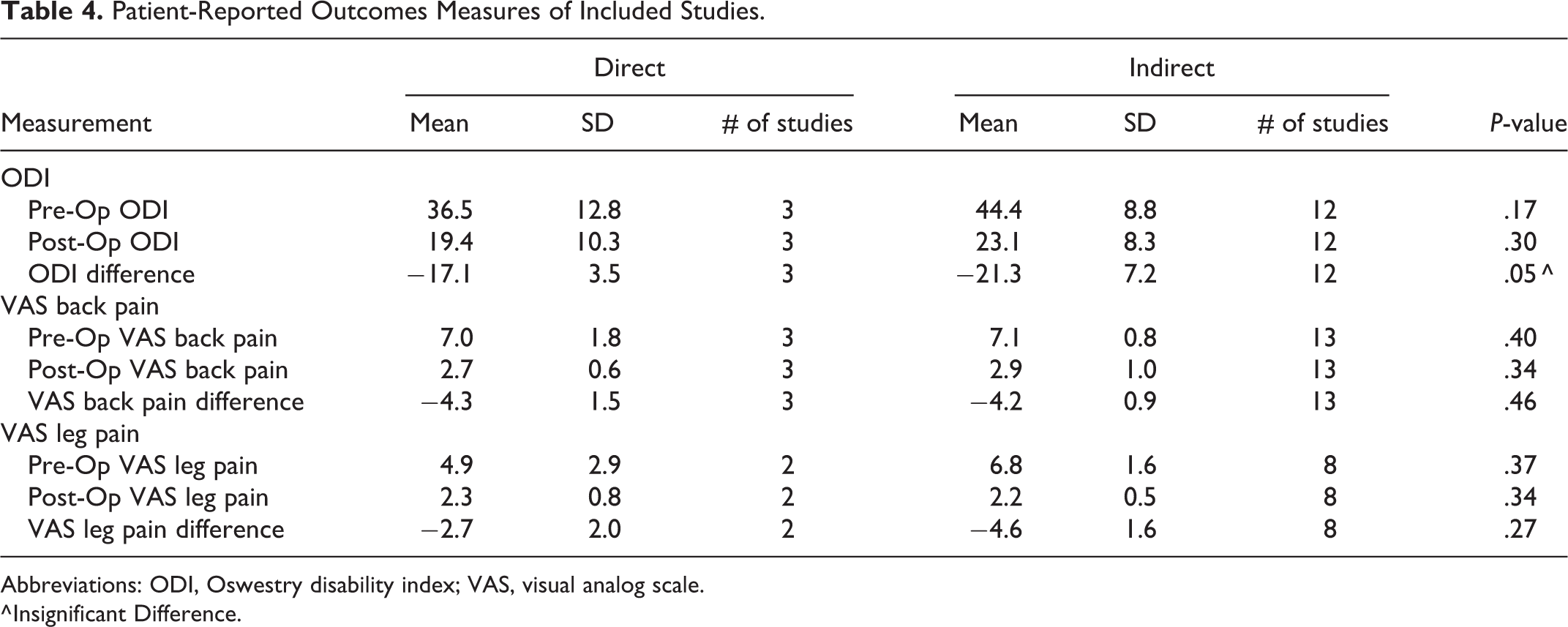
Abbreviations: ODI, Oswestry disability index; VAS, visual analog scale.
^ Insignificant Difference.
All-complications and revision rates varied across the direct and indirect decompression groups (Table 5). Direct decompression studies reported a mean all-complication rate of 16.7%. Indirect decompression studies reported a mean all-complication rate of 29.0%. Revision rate for direct decompression cases was 9.5% while the revision rate for indirect decompression cases was 8.1%. Relative to direct decompression, increased odds of all-complications and revision surgery after isolated indirect decompression were not statistically significant. Overall, the reported revision and all-complications rates in this systematic review are consistent with observed means across the spine fusion and decompression literature. 18
Post-Operative Clinical Indicators of Included Studies.

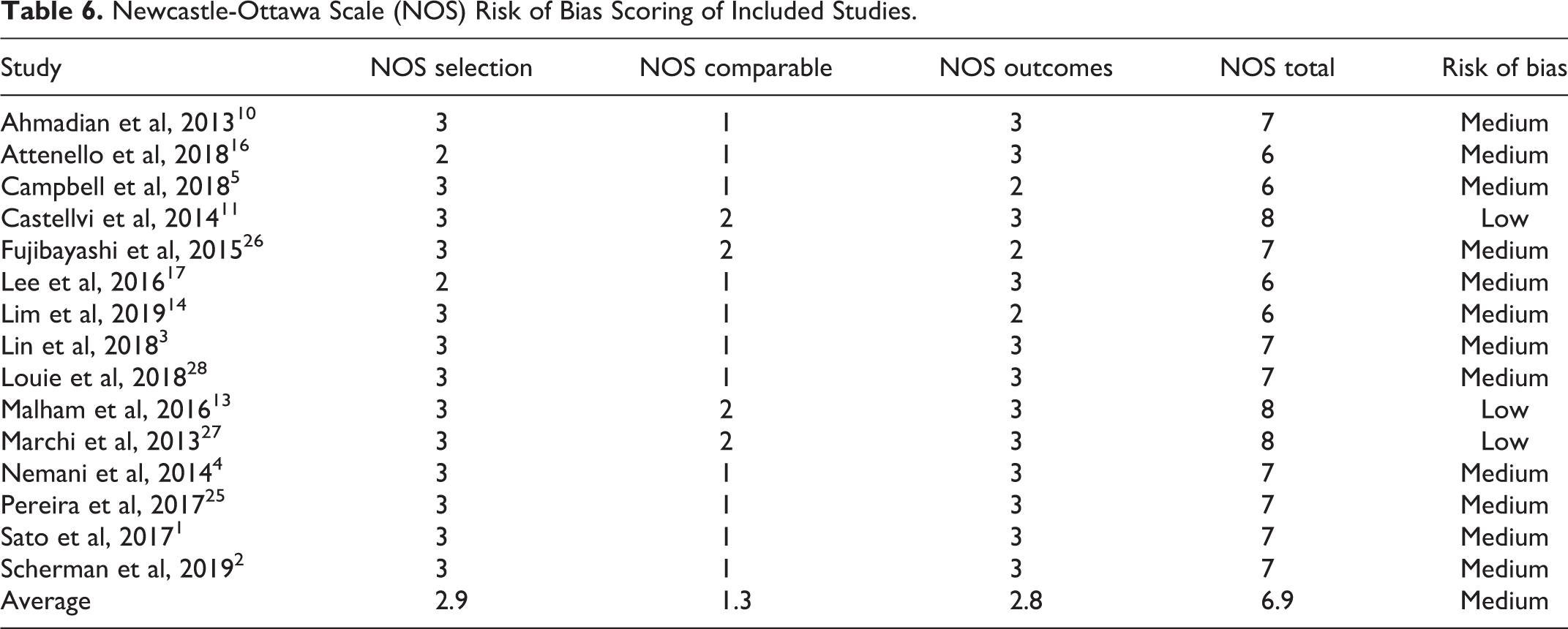
Twelve studies were assessed to have medium risk of bias due to methodological quality based on their NOS scores of 5, 6, or 7, with an average of 6.9 ± 0.5 out of 9.0 possible points (Table 6). The remaining 3 papers were assigned NOS scores of 8 or 9, with an average of 8.0 ± 0.0 out of 9.0 possible points, indicating low risk of methodological bias. Primary sources of bias identified during this assessment included study population selection, limited follow-up duration, and radiological evaluation approach. All included papers involved patients older on average relative to the patient demographics observed among all spine fusion surgery cases in the United States. 19 Radiological follow-up periods of less than 12 months typically required for bony fusion to occur, unreported fusion rate, unspecified graft approach, or limited patient demographic details were additional aspects that led to assignment of lower NOS scores. Overall, the studies included in this review have relatively limited risk of bias due to quality of approach.
Newcastle-Ottawa Scale (NOS) Risk of Bias Scoring of Included Studies.
Discussion
Prior studies of outcomes after lumbar indirect decompression via lateral interbody fusion with or without additional posterior direct decompression are limited by small sample sizes and heterogeneous patient populations. In addition, few studies directly compare these 2 techniques, with most studies reporting outcomes after either indirect or direct decompression procedures. Therefore, the current study aims to synthesize this existing literature via a systematic review. While significant differences in clinical and radiographic outcomes were not identified, both cohorts demonstrated improvements in patient reported outcome measures postoperatively. In addition, there was a notable trend toward a greater decrease in ODI with isolated indirect decompression and greater improvement in lumbar lordosis with additional direct posterior decompression.
Of the 15 studies included in this review, the most consistently comparable patient reported outcomes were ODI, VAS-leg pain, and VAS-back pain. Of those, statistically significant differences in improvement were not identified between the 2 cohorts. There was a trend toward greater improvement in ODI after isolated indirect decompression cohort (−21.3 vs. −17.1; P = .053). The limited number of patients in the current analysis likely limits the statistical power of this comparison. However, suggestion of a difference in functional outcomes between these procedures is novel, and the reason for this is unclear. While it may be assumed that patients requiring additional direct decompression have more severe preoperative stenosis and worse baseline function, this was not the case. In fact, patients undergoing additional direct posterior decompression actually had less preoperative disability compared with isolated indirect decompression patients, although this difference was not statistically significant. Another possible explanation is that posterior decompression results in additional approach-related pain and longer postoperative recovery. While studies of indirect decompression in isolation show good postoperative outcomes overall, it is often difficult to compare these studies with populations undergoing direct decompression due to differences in the underlying degenerative pathology being managed. However, it appears that in many cases, isolated indirect decompression is in indeed sufficient for treating lumbar degenerative pathology.
Interestingly, in terms of radiographic parameters, no significant differences were noted between indirect and direct decompression groups. While a greater increase in lumbar lordosis was seen in patients undergoing direct posterior decompression (+25.9
Overall, complication and revision rates were not statistically different between groups. However, there was a trend toward increased complications with isolated indirect decompression at 29.0% versus 16.7% for combined indirect and direct decompression (P = .06). As complications could only be assessed from 2 of the 3 studies of direct decompression, the true complications rates may be similar with a varied distribution of complication types. Higher rates of intraoperative nerve root injuries are seen with a posterior approach to the lumbar spine. In 1 systematic review of 6,669 MIS transforaminal lumbar interbody fusions (TLIF), the rate of postoperative radiculitis or neurological deficits was 5.9%. 20 While posterior dissection and nerve root manipulation for MIS TLIF is more extensive than for a posterior decompression, these risks are largely avoided with an isolated lateral approach. However, the lateral approach also introduces the possibility of different risks associated with spine-adjacent structures including the lumbar plexus and psoas muscle. In a series of 55 patients undergoing either MIS LLIF or TLIF, 31.0% of LLIF patients had postoperative hip flexion weakness compared with 0.0% of TLIF patients. 21
Similar reoperation rates were observed between cohorts. Lee et al demonstrated a 14.3% revision rate among 21 patients undergoing direct decompression. 17 This included 2 cases of epidural hematoma requiring evacuation as well as 1 deep infection requiring irrigation and debridement. There were no lateral approach-related complications with direct or indirect decompression cohorts. In addition, Lim et al demonstrated a 0.0% revision rate and 4.0% rate of intraoperative dural tear among patients undergoing direct decompression. 14 With patients undergoing indirect decompression, Marchi et al demonstrated a 13.5% revision rate, involving 10 of 74 patients, including 6 patients who experienced subsidence and 4 patients who had persistent post-operative stenosis. 27 Similarly, Louie et al demonstrated a 12.0% reoperation rate among patients undergoing indirect decompression involving 3 of 25 patients. 28 All 3 patients required subsequent posterior decompression and fusion for either persistent stenosis, graft subsidence, or new instability. As the risk of reoperation for inadequate decompression or refractory stenosis appears higher with isolated indirect decompression, this risk appears to be offset by increased reoperations for epidural hematoma and infections associated with utilization of a posterior approach.
Lee et al examined patients undergoing 3-, 4-, or 5-level interbody fusion with concomitant spinal stenosis and lumbar deformity. 17 In this cohort, patients undergoing open posterior decompression had worse preoperative kyphotic deformity with pre-operative lumbar lordosis of 18.0o versus 35.0o in their percutaneous fixation group. The additional facetectomies and osteotomies performed in these patients likely contributed to worse postoperative disability and pain. Interestingly, there were no significant differences in postoperative improvements in pain and function between patients with open posterior decompression and percutaneous posterior fixation.
Attenello et al similarly compared open decompression versus percutaneous fixation after LLIF in a population of patients with adult degenerative scoliosis. 16 However, they noted lack of significant difference between groups in terms of preoperative radiographic measures of deformity (lumbar lordosis, pelvic incidence minus lumbar lordosis [PI-LL], and coronal cobb angle). Nevertheless, each decision for posterior decompression versus percutaneous instrumentation was made independently by the treating surgeon based on clinical and radiographic factors. The authors found a significantly greater improvement in overall VAS pain score in the percutaneous group compared with the open posterior decompression group. However, no significant difference was noted when analyzing VAS-leg pain, VAS-back pain, or ODI (similar to the overall findings of this systematic review).
Finally, Lim et al studied a mixed population of patients with multiple degenerative diagnoses undergoing either isolated LLIF or LLIF with posterior decompression. 14 The most frequent diagnosis among isolated LLIF patients was degenerative spondylolisthesis, while the most common diagnosis among posterior decompression patients was degenerative scoliosis. The decision to proceed with isolated lateral lumbar fusion with or without additional posterior decompression was dependent on the presence of persistent neurogenic claudication pain or radicular leg pain, despite changes in posture or sitting. Both groups demonstrated significant improvements in all patient reported outcomes by final follow up, again without significant difference in improvement between the 2 groups (consistent with the overall findings of this review). The authors therefore concluded that their clinical criteria for offering posterior decompression of persistent pain despite dynamic posture were valid in this cohort.
Significant heterogeneity in the direct and indirect decompression cohort patient populations likely contributed to the lack of clear differences in outcomes between cohorts. For example, in adult spinal deformity populations, the need for posterior facetectomies and osteotomies to achieve deformity correction may supersede the need for additional posterior neural structure decompression. Traditionally, indirect decompression with LLIF has been utilized for restoration of disc and foraminal heights as well as decompression of foraminal stenosis. Recent studies have demonstrated positive clinical and radiographic outcomes with indirect decompression, even in the setting of severe central stenosis22-24 However, none of the comparative studies in the current review directly compare patients specifically with central stenosis. Both Lee et al and Attenello et al focus on deformity populations.16,17 Lim et al report that 45.2% of indirect decompression patients (n = 19) and 37.5% of direct decompression patients (n = 3) had severe central of lateral recess stenosis. 14 Therefore, future prospective study is necessary to elucidate the value of utilizing indirect versus direct decompression techniques specifically in the setting of symptomatic central lumbar stenosis.
There are a number of limitations to the current review that should be considered a priori. First, the majority of the included studies are observational and not comparative. None of these comparative studies were randomized controlled trials. Therefore, the overall quality and strength of studies included in this review was limited. Second, heterogeneity between direct and indirect decompression cohorts is likely. For example, cases managed with additional direct decompression were more likely to be in patients with severe lumbar stenosis. Similarly, patients undergoing indirect decompression may have had isolated foraminal stenosis or milder central stenosis which obviated the need for aggressive posterior surgical intervention. In general, patient diagnosis reporting did not delineate case severity in the reviewed studies. Next, only a limited set of studies included patients undergoing lateral fusion with additional direct posterior decompression. Alternative posterior fusion techniques, such as posterolateral fusion or transforaminal interbody fusion, are more likely to be utilized in cases when posterior decompression is deemed necessary. Finally, the most commonly reported patient outcome measures that could be compared between studies were ODI and VAS pain scores. Fusion rates, other radiological measurements, and global quality of life measures were either not assessed or reported inconsistently across studies. As a result, generalizability of our findings should be considered when determining the optimal course of treatment for individual patients. Nevertheless, the results of the current systematic review are both novel and useful.
In conclusion, the current review demonstrates that indirect lateral decompression without or combined with additional posterior decompression can be effective for treatment of lumbar spinal stenosis and other degenerative pathologies. While there are trends suggesting better functional improvements with indirect decompression as well as improved restoration of lumbar lordosis with additional posterior decompression, the heterogeneity of patients in these studies makes it difficult to complete all potential comparisons between cohorts. In addition, while the complication profiles of the 2 procedures differ, the revision rates are similar. Therefore, future prospective investigation is warranted to compare these 2 techniques in a controlled patient population, such as patients with moderate to severe central stenosis, with increased power. While both direct and indirect decompression are effective in specific patient populations, without this type of prospective comparison the ideal indications for an isolated indirect lateral decompression cannot be determined.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.