
Abstract
Study Design
Retrospective cohort study.
Objectives
With steadily increasing implementation of far lateral approaches in spine surgery, surgeons can utilize the advantages of different approaches synergistically to ensure an optimal patient outcome. Our single institution study aimed to assess the complication rates of patients who underwent a lateral interbody fusion as the index procedure and additional anterior or posterior instrumentation as part of a planned staged surgical reconstruction effort.
Methods
This study was approved by our institutional review board (STUDY2021000113). We included 576 patients who received a lateral lumbar interbody fusion (LLIF) as the index procedure followed by transforaminal lumbar interbody fusion (TLIF), posterior lumbar interbody fusion (PLIF) or anterior lumbar interbody fusion (ALIF) between 2016 and 2020. Primary outcomes were complications identified during the initial inpatient stay, which were categorized into approach-related and secondary complications. Secondary outcomes tracked up to 6 years post-surgery.
Results
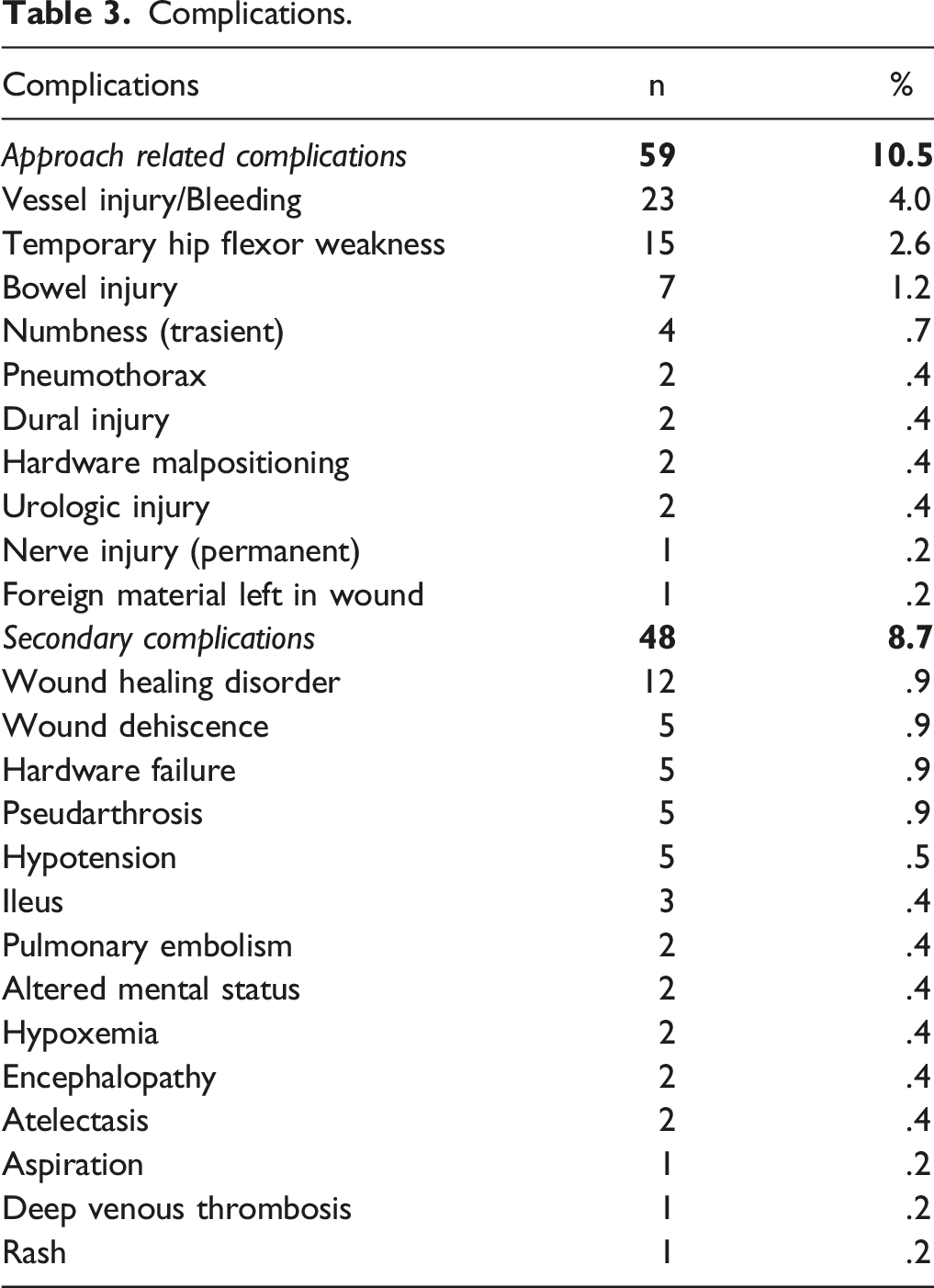
The overall complication rate was 19.2% (10.5% approach related, 8.7% secondary complications). Significant intraoperative hemorrhage (mean 659.3 mL vs 131.4 mL, P < .01) was the most common approach related complication with an incidence of 4%, followed by temporary hip flexor weakness in 2.6%. A permanent (femoral) nerve damage was verified in 1 patient. The most common secondary complication was impaired wound healing in 12 patients (2.1%). We identified a 7.1% (41 of 576 patients) rate of revision surgery, on average after 372 days (±34 days).
Conclusions
We recorded an overall complication rate of 19.2% for staged adult deformity corrective surgeries utilizing far lateral interbody fusions at several lumbar levels followed by a more comprehensive posterior surgical reconstruction.
Keywords
Introduction
Far lateral approaches to the thoracolumbar spine have rapidly become a popular addition to other interbody approach techniques over the last decade. Less invasive or so called ‘minimally invasive’ (MI) approach techniques in spine surgery have become popular due to reduced soft tissue dissection and potential for less surgical trauma in the management of patients with medical comorbidities. Pertinent to the development of less invasive anterior approaches far lateral access techniques that utilize the psoas major muscle structure as reference window can be summarized with the term ‘lateral lumbar interbody fusion’ (LLIF). LLIF consists of 2 subvariants ‘direct lumbar interbody fusion (DLIF, Medtronic SofamorDanek) and extreme lateral interbody fusion (XLIF; NuVasive, Inc., San Diego, CA); both are similar as to their trans-psoas access route but differ regarding specific surgical equipment.1,2 Touted advantages of such lateral fusion techniques include minimized tissue trauma, lower blood loss, and the preservation of the posterior ligamentous structural elements of the spine.3-5 Over time, however, a variety of specific complications have become increasingly commonly described for lateral approaches such as hip flexion and knee extension weakness as well as thigh and groin numbness, either through direct muscle trauma, lumbar plexus injury or a combination of both.1,2,6 To reduce specific transmuscular approach complications new antero-oblique surgical techniques such as anterior-to-psoas approach (ATP) and oblique lateral interbody fusion (OLIF) were introduced in 2012.7,8 Such less invasive anterior, anterolateral and far lateral approaches hope to reduce the soft tissue disruption, blood loss and other complication risks commonly associated with conventional posterior approaches.
9
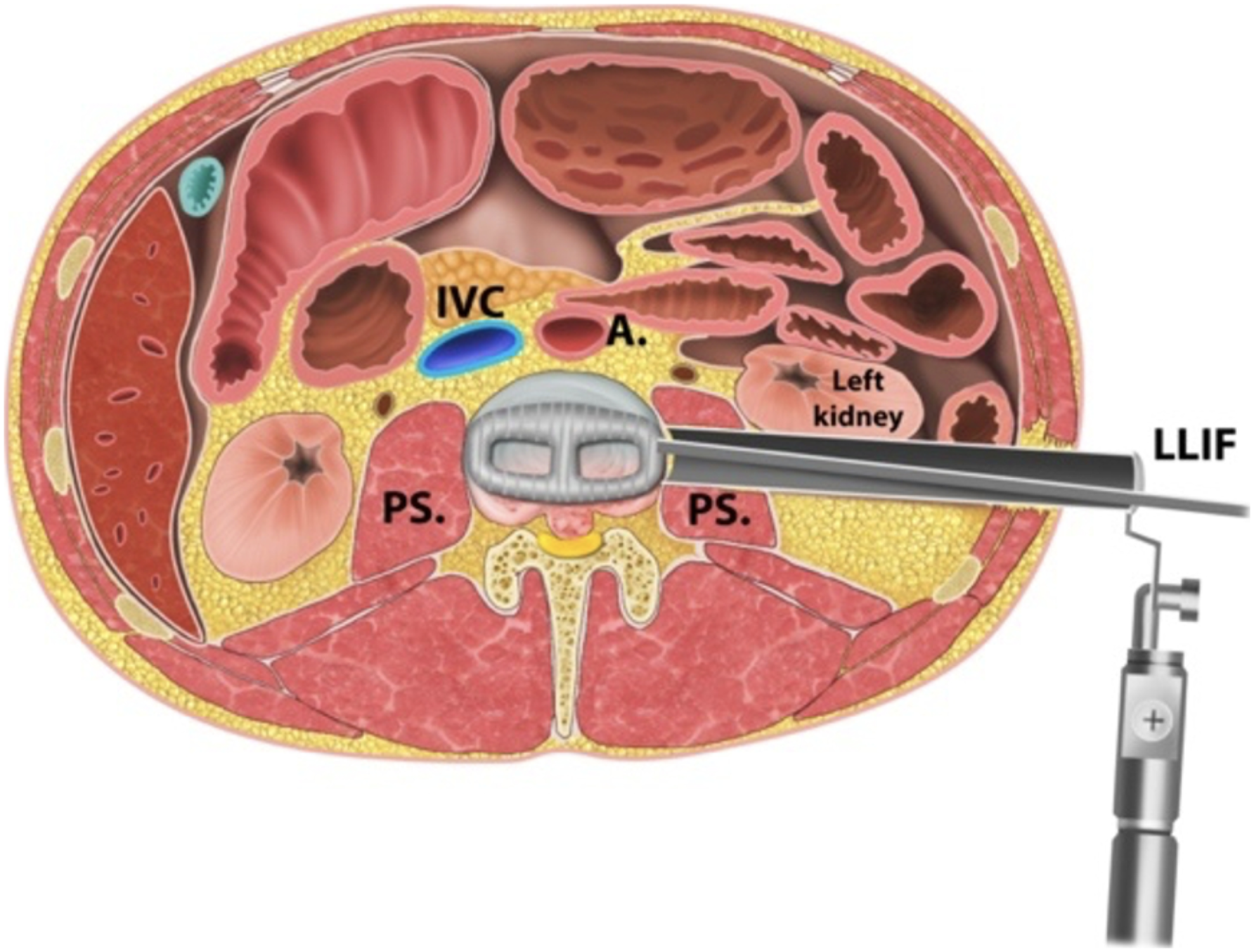
A summary graphic represents the various access trajectories for reconstructive procedures in the lumbar spine (Figures 1 and 2). Surgical approaches to the lumbar spine. Surgical approach for lateral lumbar interbody fusion (LLIF).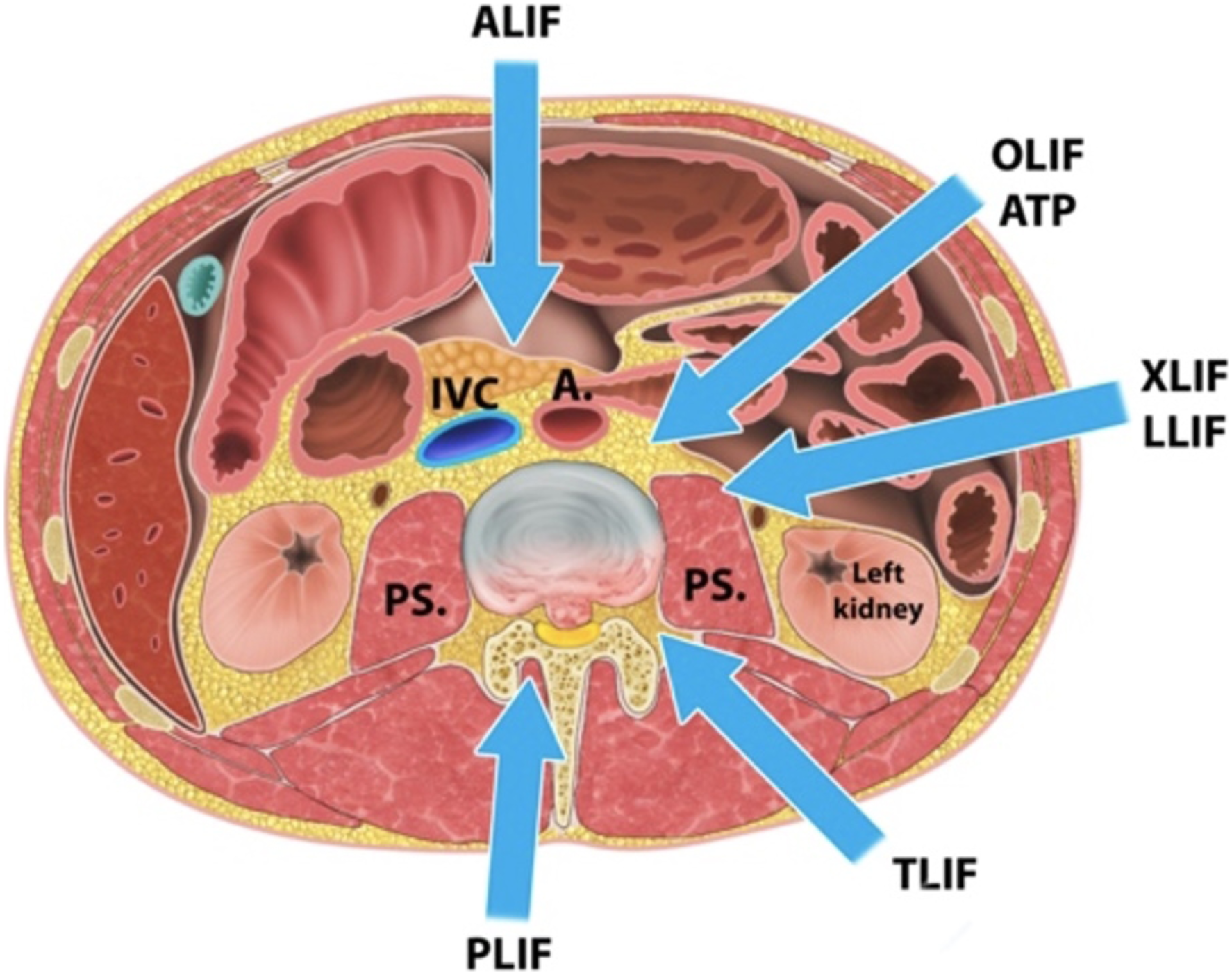
For certain complex conditions, such as major thoracolumbar deformities, advanced spondylotic disease and certain other spine conditions that encompass multiple levels of the thoracolumbar spine a combined use of lateral and posterior based surgeries might provide synergistic advantages towards an optimal patient outcome by emphasizing the strengths of either approach philosophy though a combined surgical care concept. Previously studies have emphasized reports on isolated approach specific complication and outcome rates. However, little is known regarding outcomes of patients who were treated with a planned combination of both techniques, consisting of a less invasive lateral fusion in combination with supplementary posterior neural decompression and instrumentation including a fusion procedure through a staged separate procedure.10-15 With this study we aimed to critically assess early and subacute complications as one of the outcome determinants from a routinely applied combination approach utilizing less invasive far lateral interbody arthrodesis first, followed by a more comprehensive posterior reconstruction procedure for thoracolumbar reconstruction surgery.
Materials and Methods
This study was carried out in accordance with the Declaration of Helsinki (as revised in 2013), and was approved by the institutional review board of Swedish Medical Center Seattle (STUDY2021000113). Based on the retrospective character of the study informed consent waiver was granted. Patients who received a LLIF between 2016 and 2020 followed by TLIF, PLIF, and ALIF were included. Patients who had previous operations on the spine and whose index procedure was not performed through a lateral approach were excluded. In addition to the epidemiological data (age, gender), the length of inpatient stay, total operating time of all procedures, blood loss, number of instrumented levels and quantitative use of expandable cages was recorded. The underlying diagnoses acting as the indications for surgery were grouped into categories. Preoperative comorbidities were recorded. Number of revision procedures, and the causes for revision were also recorded. The perioperative and postoperative complications that occurred during the inpatient stay were divided into 2 categories: approach-related, and secondary complications identified during the outpatient follow-up period. A group of 5 surgeons performed all the procedures using a highly consistent formalized surgical care program including consistent use of intraoperative neuromonitoring to aid and minimizing damage to motor nerves and roots of the lumbar plexus. Statistical analysis was performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA). Evaluation was carried out with descriptive statistics. For numerical data, means, standard deviations, medians, and quartiles were calculated depending on the distribution. Significance was determined at P < .05.
Results
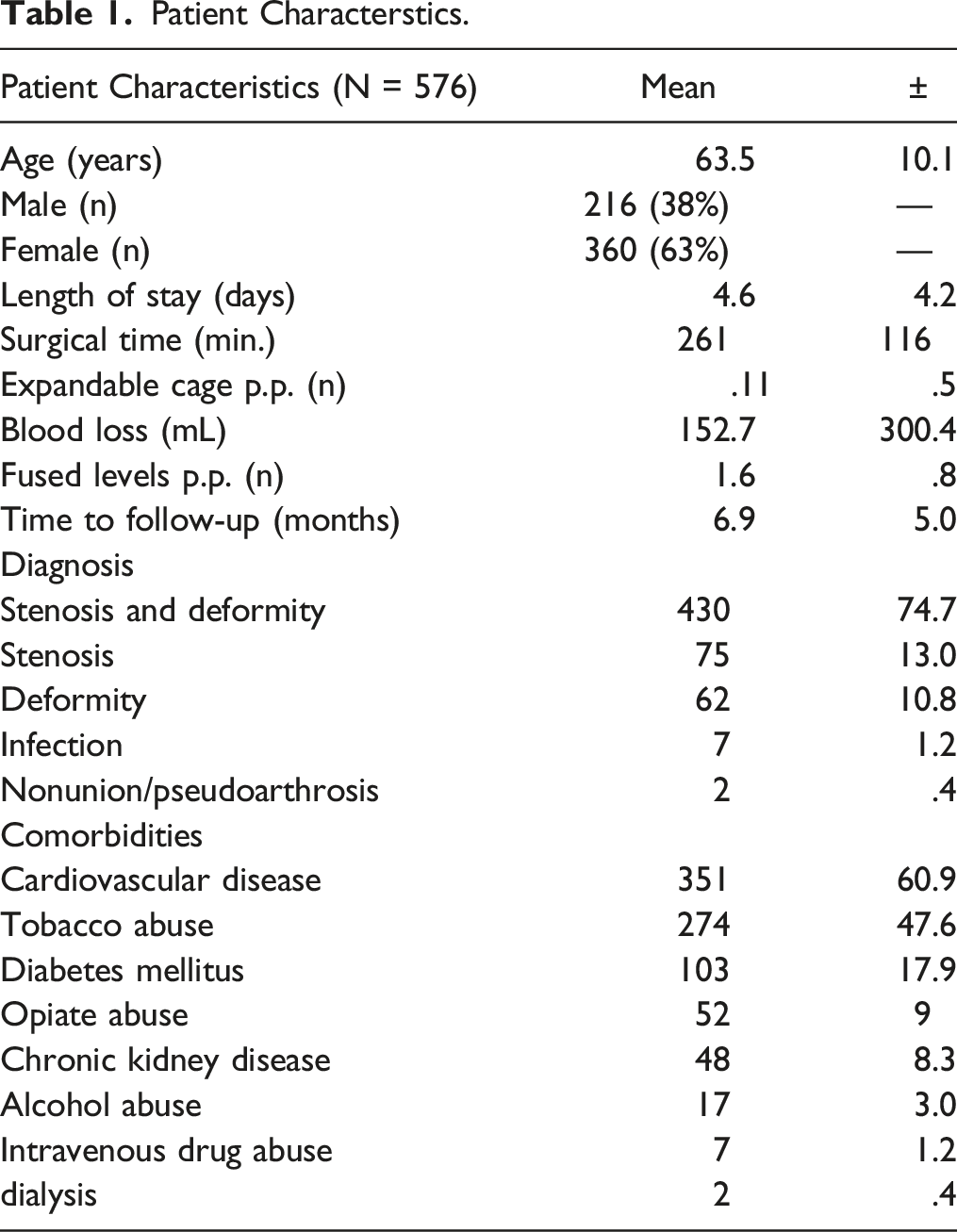
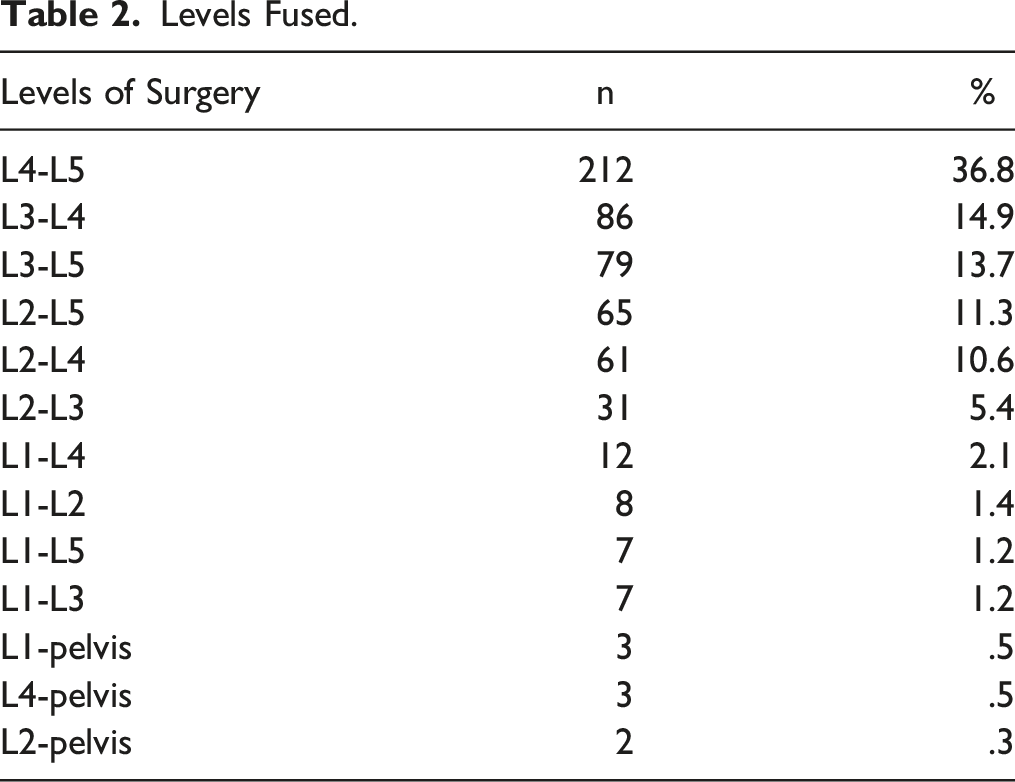
Five hundred and seventy-six patients (216 male (37,5%); 360 female (62,5%)) received a two-staged procedure. Of these, 546 patients (94.9%) received an XLIF as the index procedure, followed by a PLIF in 507 patients (92.9%), a TLIF in 31 patients (5.7%), and an ALIF in 8 patients (1.4%). Thirty patients (5.1%) received an OLIF as the index procedure followed by PLIF (27p.; 90%), and ALIF (3p.; 10%) (Figure 3). The average age at the time of surgery was 64 years (±10.1y). The mean length of hospital stay was 4.6 days (±4.2 days). Mean surgical time for both procedures combined was 261 minutes (±116 min). The clinical follow-up took place at an average of 7 months (±5 months) after the index surgery. Further results on patients' characteristics as well as comorbidities were summarized in Table 1, the exact distribution of instrumented levels was given in Table 2. Distribution of patients among the various approaches. Patient Characterstics. Levels Fused.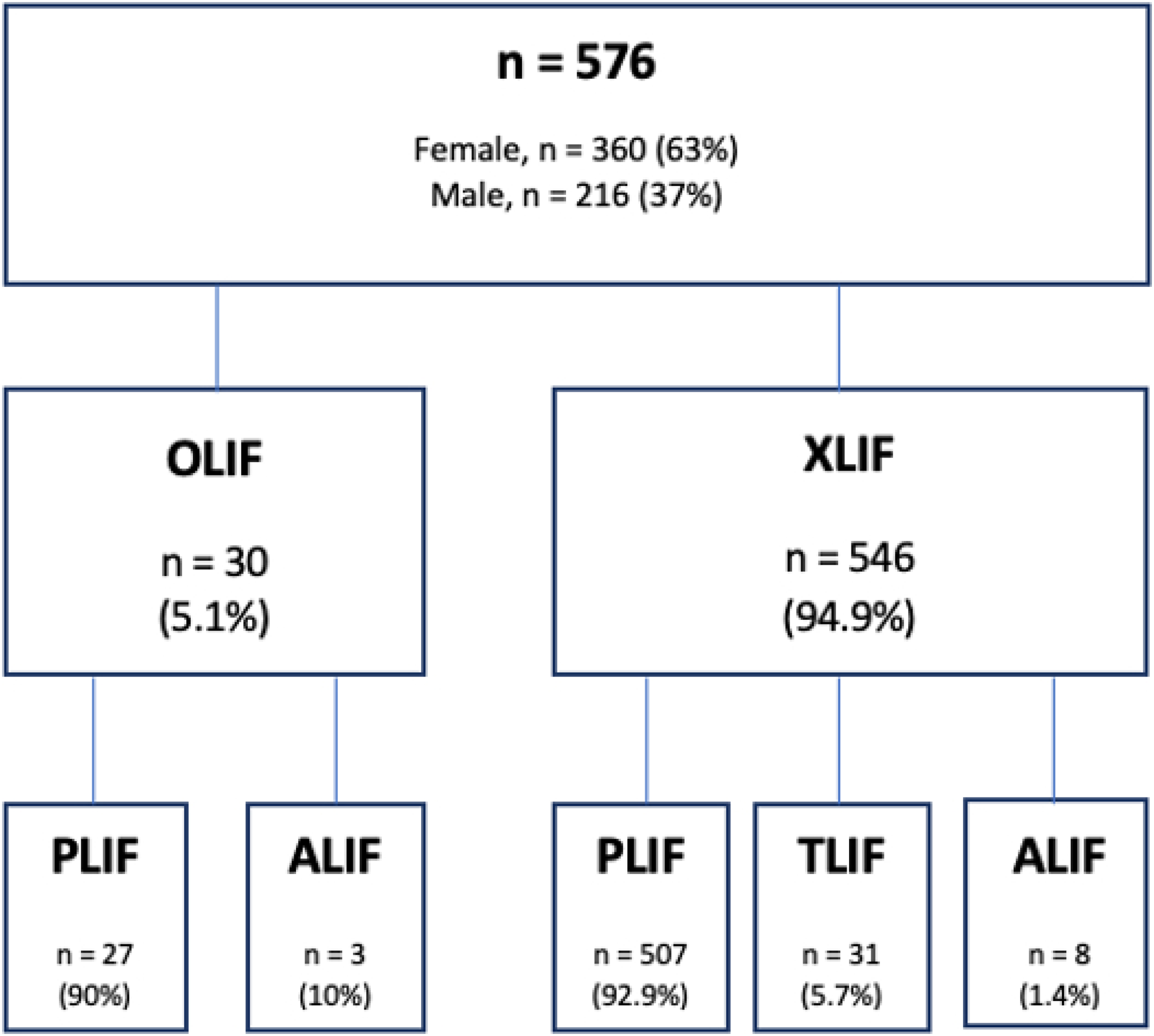
Complications
Complications.
The rate of revision surgery was 7.1%, with 41 of 576 patients necessitating a return to the operating room. The average time after which a revision was performed was 372 days (±34 days) following the index procedure. Thirty-seven patients underwent 1 revision, 3 patients underwent 2 revisions, and in 1 case (.2%) 3 revisions were necessary.
Discussion
For adult deformity surgery interbody instrumentation and fusion techniques applied in the thoracolumbar spine have become increasingly popular due to the perception of improving deformity correction and achieved long-term fusion rates. Traditional open approaches to the spine for interbody fusions are PLIF, TLIF first described by Harms and Rolinger in 1982, and ALIF. Anterior lumbar interbody fusion was first introduced in 1932, and carried out in 1933 using a tibial peg. Autografts were used until the 1970s, when the first studies with aluminum mesh cages were published. Refinements to the traditional larger open procedures in form of a MI- ALIF was then published in 1997 by Mayer.16-25 In comparison to the published complication rates of those fusions procedures we found no substantive differences to the complication rates we encountered with the staged combined far lateral and open posterior approach utilized in our large single institution case series.7,11,26-31 According to our data perioperative bleeding occurred with an incidence of 4% most frequently among approach-related complications and was rated as significant when it exceeded 500cc. In a systematic review, Walker et al. reported an incidence of significant perioperative bleeding of .4%-1.8% among 6481 patients from 59 studies after a trans-psoas or pre-psoas approach. 31 Silvester et al. described significant bleeding complications in 3 cases in their single institution study with 179 patients following an OLIF procedure. In their study, 2 cases were due to injuries to the external iliac vein and 1 case was a laceration of the iliolumbar vein, which is particularly at risk during anterolateral surgery to the L5/S1 level. 32
In our study, none of the patients with bleeding complications rated as ‘significant’ using our arbitrary 500cc threshold (659.3 mL vs 131.4 mL, P < .01), no clear injuries to large vessels were identified intra-operatively or post-operatively. Consistent with our findings Zeng et al., a single institution study, found a frequency of significant intraoperative bleeding of 4% in 91 patients following stand-alone OLIF, and 144 patients after OLIF with additional posterior pedicle screw fixation. They found no significant difference in this complication rate in between the 2 groups. 7 Temporary hip flexor weakness is another common complication of lateral approaches to the lumbar spine,29,33 and was recorded as clinically significant in 2.6% of the patients in our study. Temporary hip flexor weakness is an approach-specific complication that occurs almost exclusively in patients following a trans-psoas approach. This weakness, an almost expected sequela as result of blunt dissection and ensuing direct trauma to the psoas muscle and likely not a result of permanent nerve damage.10,15,28 In a systematic review by Epstein et al. the authors reported temporary weakness of the hip flexors in 1.2-3% of the cases, in 1453 patients who underwent OLIF procedures across 16 studies. 29 A systematic review by Salzmann et al. who analyzed the complication rates of 1874 patients from 20 studies following OLIF and 4607 patients from 20 studies following XLIF, found an incidence of temporary hip flexor weakness of 8.7% in the OLIF group, compared to 21.7% in the XLIF group. 27 In a prospective multicenter study, which analyzed 102 patients following XLIF of the levels L3/4 and L4/5, Tohmeh et al found a frequency of temporary hip flexor weakness in 27.5% of their patients. 34 However, other studies describe a temporary hip flexor weakness as a complication following dorsal approaches to the spine, whereby the surgeon did not directly encroach upon the psoas. In a systematic review of 42 studies including 4260 patients receiving LLIF conducted by Joseph et al., 9.4% of patients suffered temporary hip flexor weakness post-operatively. The authors also found an incidence of temporary hip flexor weakness in 2.2% of patients following MIS- TLIF. 11 This finding is interesting given that the psoas is innervated by the ventral branches of the spinal nerves at levels L1 to L4. A cadaveric anatomical study by Mahan et al. dissected 24 cadaver psoas muscles. They found that the direct muscle nerve branches from L2 and L3 could be found supplying the psoas in all specimens, while the efferents to the psoas from the L1 and L4 roots were subject to greater variability. In addition, this study was also able to show that the branches innervating the psoas muscle crossed the L3/4 disc space in the central zone in 45% of the cases. 35 It is therefore predictable that blunt manipulation of the psoas muscle in a far lateral approach can cause temporary hip flexor weakness. Temporary hip flexor weakness following MIS-TLIF is much less common and is likely caused by positional damage by irritation of the ventral ramus at the operated level. While all temporary hip flexor weaknesses in our data were completely resolved by the time of the patient’s last follow up during the period of f/u, Sadrameli et al. described the persistence of the symptoms in 9.1% of their patients after a follow up of 3 weeks following L4/5 LLIF. 30
The most feared complication in both lateral and conventional spinal surgery remains permanent iatrogenic nerve damage. In our data, this complication occurred in only 1 case (.2%) and was due to a femoral nerve damage following XLIF. This patient remained 3/5 strength in his quadriceps at their last follow up (7 months). Compared to the relevant literature, our rates of permanent femoral nerve damage were low. Permanent nerve damage was described in the above-mentioned systematic review by Joseph et al. in 1 percent the patients following MIS-TLIF, and in 2.5% of the patients following LLIF. 12 In contrast, a single institutional chart review by Mehren et al. analyzed 802 patients who underwent OLIF, and found neurological complications in 1.1% of their patients, but went on to state that all initial strength deficits regressed completely, and only 2 patients (out of 802) persisted to suffer from sensory deficits at time of last follow up. 36 It is therefore important to introduce a more precise categorization of neurological complications in future studies, which on the one hand distinguishes the etiology of the symptoms (e.g., manipulation of the psoas vs denervation regarding hip flexor weakness), as well as a rigorous standardized follow up.
In our study, the third most common approach-related complication was a bowel injury, which was reported in 7 cases (1.2%). Walker et al. found bowel injuries in 1.9% of patients with pre-psoas approaches, and in 1.3% of patient with trans-psoas approaches. Motasem et al. found an ileus in 7% of their patients after LLIF, compared to .5% in our data (5 patients). 37 In their systematic review Walker et al. also reported a urologic injury rate of 1.1% following pre-psoas approaches and no urologic injuries following trans-psoas approaches. 31 We did not encounter a single case of ureter or other urogenital injury. However, are aware of such injuries having occurred in our geographical area during our observation window at other institutions.
Our overall complication rate of 19.2% is comparable to complication rates previously reported in the literature. Zeng et al. reported a combined complication rate of 32% in 235 patients after OLIF stand alone or OLIF with supplementary pedicle screw fixation. They found a complication rate of 36% in the OLIF stand-alone group, and a complication rate of 30% in the OLIF plus pedicle screw fixation-group. 7 Yilmaz et al. found a total complication rate of 13.4% to 31.5% among 166 patients after a trans-psoas approach, depending on whether a corpectomy (31.5%) was performed or not. 3 In a systematic review, Walker et al. reported complication rates of .5% to 28% in both the pre-psoas group, which included 20 studies, and the trans-psoas group, which included 39 studies. 31 There exist some limitations that should be considered in the evaluation of the results of our investigation. First, the retrospective nature of this study could imply selection and other forms of intrinsic bias. Secondly, 95% of our procedures were trans-psoas approaches, with pre-psoas procedures and their complications being relatively under-represented, therefore limiting side-by-side comparisons. Due to the asymmetrical distribution of both groups, we refrained from determining P-values in order to make direct comparisons between XLIF and OLIF patients. Regarding the revision rate, the follow-up, which could be generated from the underlying data, is too short-sighted to make a final statement regarding the revision rate.
Conclusion
This retrospective review examined the complication rates in patients after lateral interbody fusion with supplementary instrumentation via a separate approach. The results indicated that complication rates (19.2%) remained in keeping compared to rates reported by other studies. Temporary hip flexor weakness remains the most common complication in lateral approaches, while wound healing disorders and increased perioperative blood loss seem to be more associated with dorsal instrumentation. Permanent femoral nerve damage is a rare complication of lateral approaches to the lumbar spine, and occurred in only 1 patient.
Footnotes
Authors' Contributions
Conceptualization: Oskouian Rod J, Chapman Jens R; Methodology: Frieler Sven, Tataryn Zachary; Formal analysis and investigation: Godolias Periklis, Charlot Kaarina, Tran Angela, Al-Awadi Hamzah; Writing - original draft preparation: Nunna Ravi, McBride Paul, Ghayoumi Pouriya; Writing - review and editing: Godolias Periklis, Gerstmeyer Julius; Ruetten Sebastian; Resources: Chapman Jens R, Oskouian Rod J; Supervision: Ruetten Sebastian, Chapman Jens R, Oskouian Rod J.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
We certify that all applicable institutional and governmental regulations concerning the ethical use of clinical data were followed during the course of this research according to the Declaration of Helsinki. This study (STUDY2021000113) was approved by the institutional review board at Swedish Medical Center Seattle. All methods were carried out in accordance with relevant guidelines and regulations.
Consent to Participate
All authors have given a written declaration of consent for publication of the data obtained in this study.
Availability of Data and Materials
The dataset used during the current study is available from the corresponding author on reasonable request.