
Abstract
Study Design
Retrospective study.
Objectives
We investigated the effect of corridor width on the postoperative outcomes of patients who underwent the OLIF procedure.
Methods
Patients who underwent OLIF surgery, which included L4-5, between 2015 and 2021 were retrospectively studied. The patients were divided into three groups by the width of the corridor: not more than 10 mm, between 10 and 20 mm, and 20 mm or more. We compared clinical and radiographic outcomes and complications between these groups.
Results
A total of 81 patients were included. There were no significant differences in VAS leg and back pain scores, ODI scores, or complications between each group. The radiographic findings, including cage position, anterior and posterior disc height, segmental Cobb angle, and foraminal height, also showed no significant differences between each group. The only radiographic finding that showed a significant difference between each group was the angle of the cage. We found significantly less degree of angle in the wider than 20 mm group when compared to the other two groups. (P-value = .01). There was no recorded incidence of major vascular complications.
Conclusions
The width of oblique corridor does not affect clinical outcomes, complications, or radiographic findings, including position of the cage, anterior and posterior disc height, segmental angle, and foraminal height after OLIF procedure, including L4-5 level. Thus, the OLIF procedure can be performed safely even in patients with limited oblique corridors, especially at L4-5.
Keywords
Introduction
Oblique lateral interbody fusion (OLIF) is a minimally invasive spine surgery that has the advantages of lower blood loss, fewer complications, and a shorter return to work time. This procedure also had the benefit of reducing morbidity and mortality compared with traditional open spinal surgery. OLIF is useful to treat many spinal diseases, especially lumbar degenerative diseases and adult spinal deformity. 1 This procedure utilizes the anterolateral retroperitoneal approach to get access to the oblique surgical corridor, which is bounded by the medial edge of the psoas muscle and the great vessels. 2 Several studies reported promising clinical and radiographic outcomes and few complications after the OLIF procedure.3,4 However, controversies still exist regarding the appropriate-width of the corridor for performing the OLIF procedure safely.
The width of the corridor varies for each person. Some patients may not have any corridors. 5 Ng et al 6 reported that 25% of the patients did not have an accessible oblique corridor due to obstruction by major vessels or high-riding psoas muscle. For interbody cage placement in OLIF, a corridor’s width of at least 18 millimeters (mm) is usually required, along with the width of a frequently used cage. 7 Wang et al reported that the narrow oblique corridor was associated with a higher risk of major vascular injury when an OLIF procedure was performed. 1 Thus, some patients, particularly those with narrow corridors, might not be a good candidate for performing the OLIF procedure.
The purpose of this article was to study the effect of the oblique corridor’s width on patients’ clinical and radiographic outcomes after performing the OLIF procedure and to determine whether the narrow corridor is safe for performing the OLIF or not.
Materials and Methods
A single-center retrospective review of patients who underwent OLIF surgery from 2015 until 2021 was conducted. This study was approved by the Ethics Committee of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (IRB No. 0900/64). Informed consent was waived for this study. The inclusion criteria were the patients who underwent an OLIF procedure at least one level, including L4-5. The exclusion criteria were the patients who underwent more than five levels of spinal surgery and did not have complete clinical and radiographic outcome data. The patients who had prior lumbar spine or abdominal surgeries were also excluded.
The clinical outcomes, including the Oswestry Disability Index (ODI) and the visual analog scale (VAS) for back and leg pain, were collected at the preoperative period, 1-month, and 1-year after the operation.
The perioperative complications that were recorded and analyzed included anterior thigh pain, transient psoas muscle weakness, lumbar sympathetic chain injury, bowel ileus, infected surgical site, contralateral nerve injury, retroperitoneal hematoma, urinary retention, ureteric injury, and major vessel injury.
The radiographic measurements were performed by two orthopedic surgeons (PC, TT). The measured parameters included the anterior disc height (ADH), posterior disc height (PDH), segmental angle (SA), and foraminal height (FH) on lumbosacral lateral radiographs Figure 1. The anterior disc height (ADH) was the distance between the anterior upper endplate of L5 and the anterior lower endplate of the L4 vertebral body. The posterior disc height (PDH) was the distance between the posterior upper endplate of L5 and the anterior lower endplate of the L4 vertebral body. The segmental angle (SA) was the Cobb angle between the upper endplate of the L4 vertebral body and the lower endplate of the L5 vertebral body. The foraminal height (FH) was the distance between the lower edge of the L4 pedicle and the superior edge of the L5 pedicle. The position of the cage (POC) was categorized into 3 positions depending on the location of the center of the cage and in the intervertebral disc area. The POC was defined as 1, 2, or 3 if the center of the cage is in the anterior one-third, middle one-third, or posterior one-third of the disc space, respectively. The (A) preoperative and (B) postoperative segmental angle (SA), anterior disc height (ADH), posterior disc height (PDH), foraminal height (FH), and position of cage (POC) were measured on the lateral radiographs. (C) The psoas muscle cross-sectional area (PA) was measured on the postoperative axial T2-weighted MRI. (D) The angle of the cage (AOC) was measured on the postoperative axial T2-weighted MRI.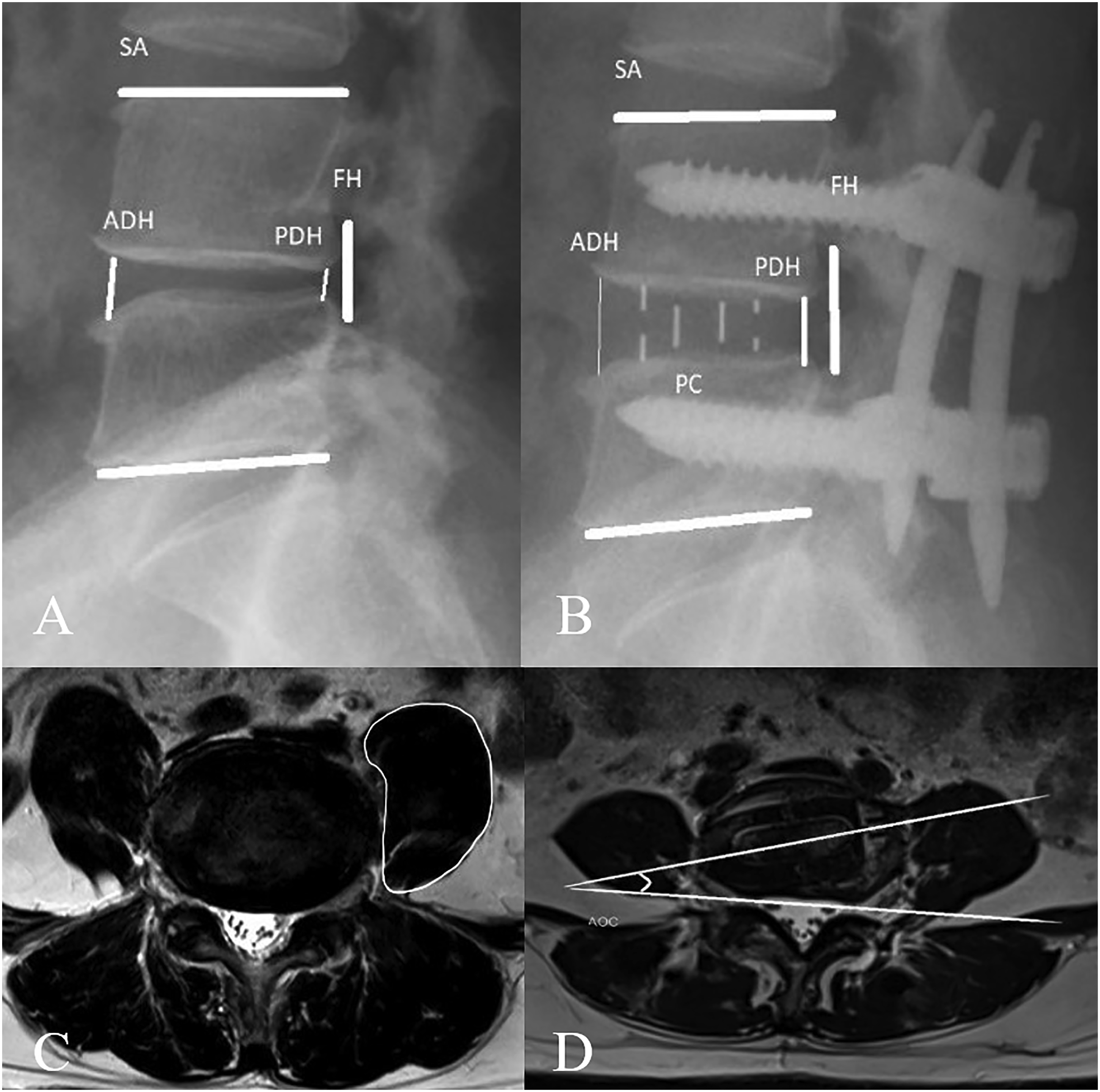
The preoperative axial T2-weighted magnetic resonance image (MRI) at the L4-5 mid-disc level was used to evaluate the pre-psoas surgical corridor, which is defined as the area between the medial edge of the psoas muscle and the aorta, or left common iliac artery, and the psoas muscle cross-sectional area (PA). The corridor was measured and divided into 3 groups: group 1 (<1 centimeter [cm]), group 2 (1-2 cm), and group 3 (>2 cm) Figure 2. The MRI was also used to evaluate the psoas muscle cross-sectional area (PA) and angle of the cage (AOC) (Figure 1). The corridor’s width was categorized into three groups (Gr.): (A) Gr.1 < 1 cm, (B) Gr. 1-2 cm, and (C) Gr.3 > 2 cm.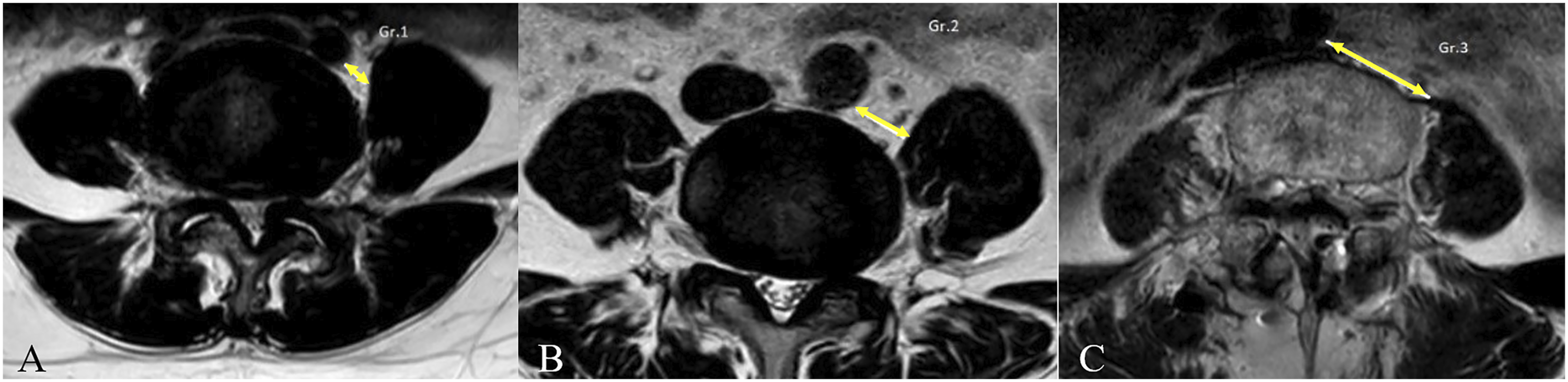
The clinical outcomes, radiographic outcomes, and complications were then compared between each group of patients.
Surgical Technique
After general anesthesia was done, the patient was positioned in the right lateral decubitus position. The targeted intervertebral disc levels were checked using the C-arm fluoroscope, and skin marking was done. A skin incision was made along the anterolateral part of the abdomen, corresponding to the skin marking of the targeted disc. The external oblique, internal oblique, and transverse abdominis muscles were bluntly dissected layer by layer to access the retroperitoneal space. The operated intervertebral disc was identified and prepared for the discectomy. In cases where the patient had no or a narrow surgical corridor, the sponge and retractor were used to retract the psoas muscle posteriorly in order to create a working space between the great vessel and the psoas muscle (Figure 3). The self-retaining tubular retractors were then applied to the created corridor before disc space preparation. After discectomy and endplate preparation were done, the appropriate-size cage filled with demineralized bone matrix (DBM; GRAFTON®, Medtronic, Minneapolis, MN, USA) was inserted in the disc space. Finally, the percutaneous posterior fixation with percutaneous pedicle screws and rods was done. Oblique surgical corridor (A) before and (B) after psoas muscle retraction.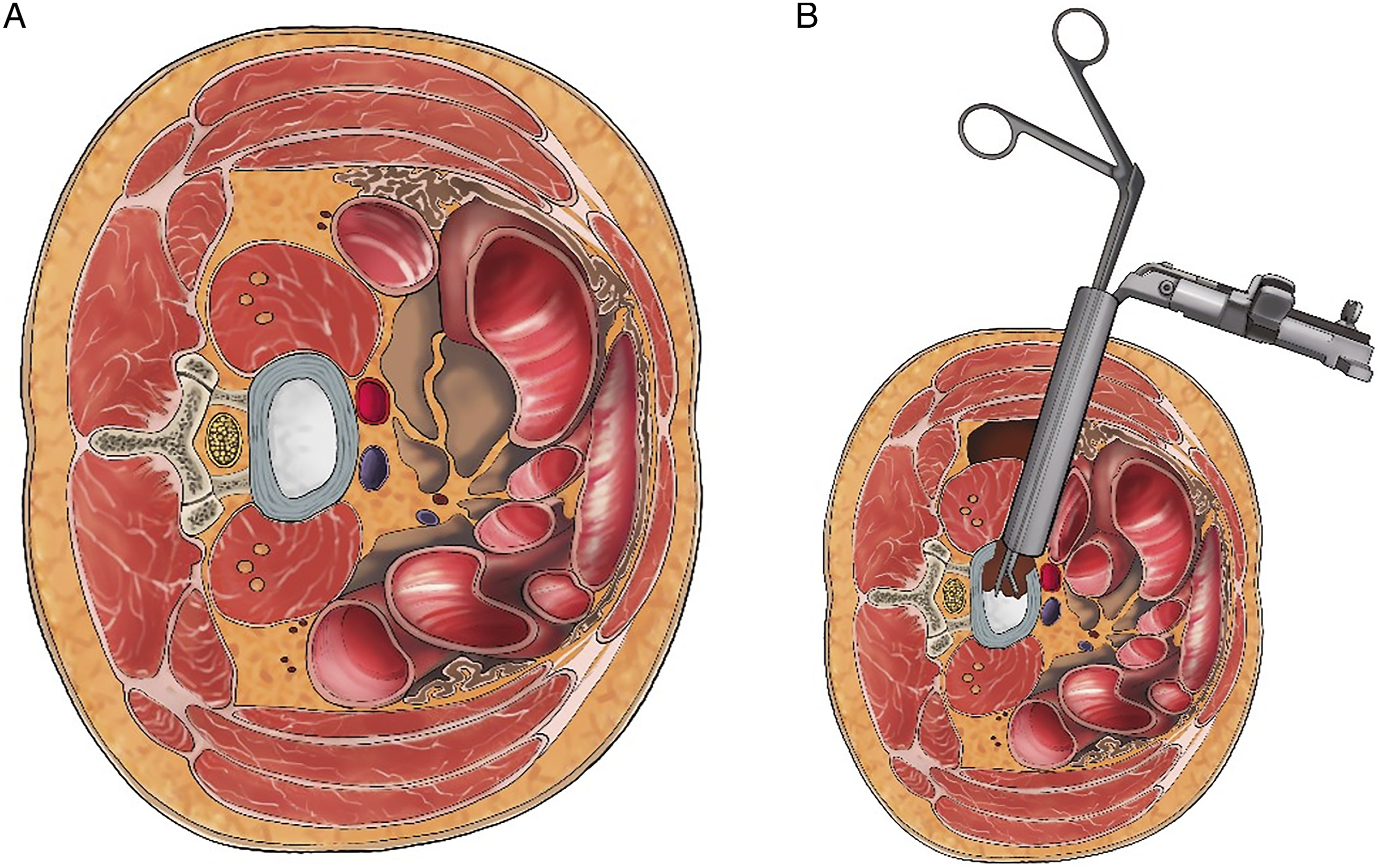
Statistical Analyses
The demographic data was analyzed using descriptive statistics, in which the continuous data was presented as mean with standard deviation (SD) or median with interquartile range (IQR), and the categorical data was presented as numbers and percentages. Differences in width between each corridor group were compared using Fisher’s exact test, and ANOVA with post-hoc comparison, or Kruskal-Wallis test with Dunn’s post-hoc comparison as appropriate. The effectiveness of the operation was compared using a paired t-test and Repeated Measure ANOVA. The intra- and inter-rater reliability analyses were done by using the intraclass correlation coefficient (ICC). Statistical analyses were conducted using STATA version 15 (StataCorp. 2017. Stata Statistical Software Release 15. StataCorp LLC, College Station, TX.). A two-tailed P-value <.05 was considered statistically significant.
Results
Demographic Data.
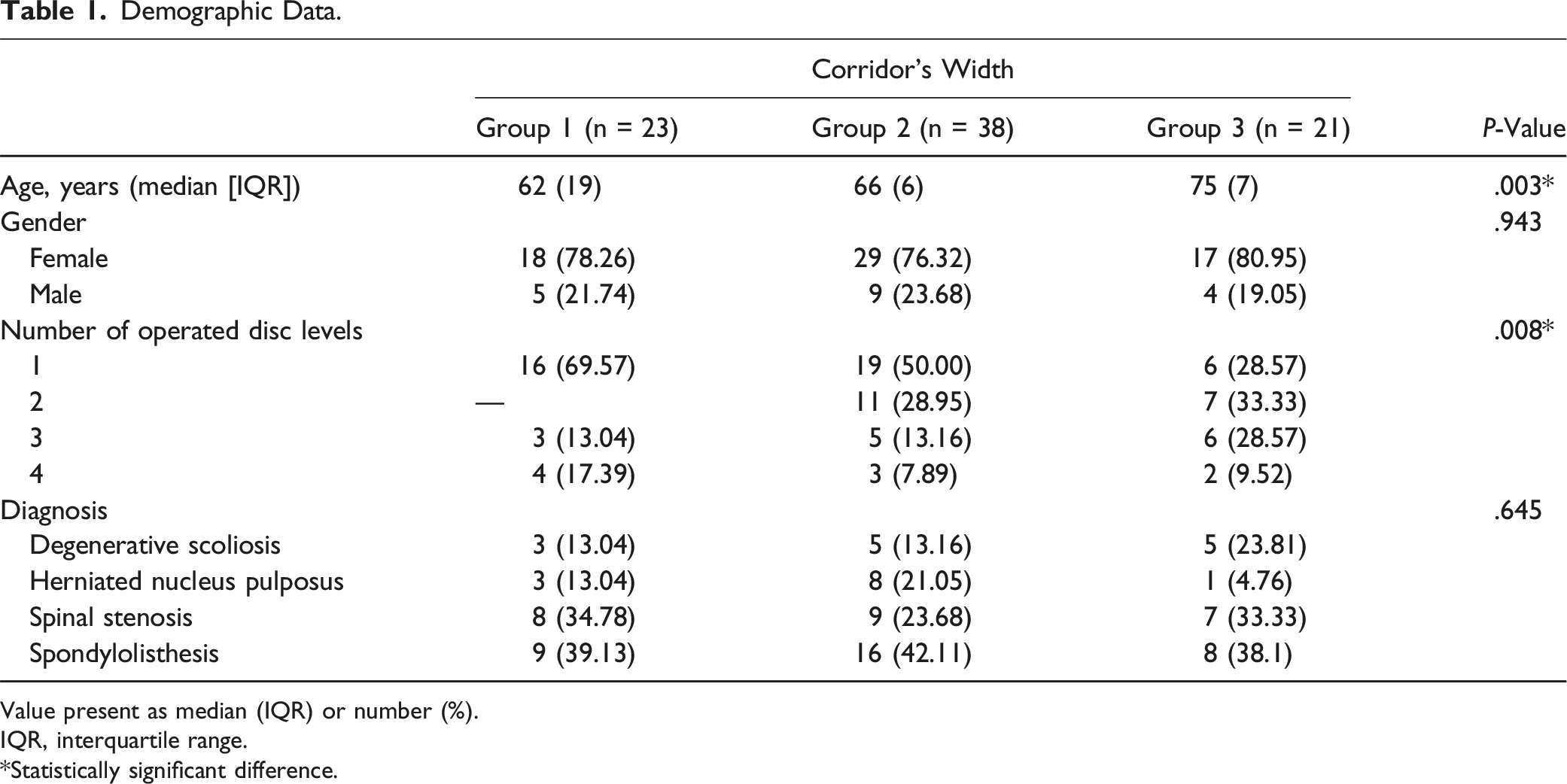
Value present as median (IQR) or number (%).
IQR, interquartile range.
*Statistically significant difference.
Clinical Outcomes.
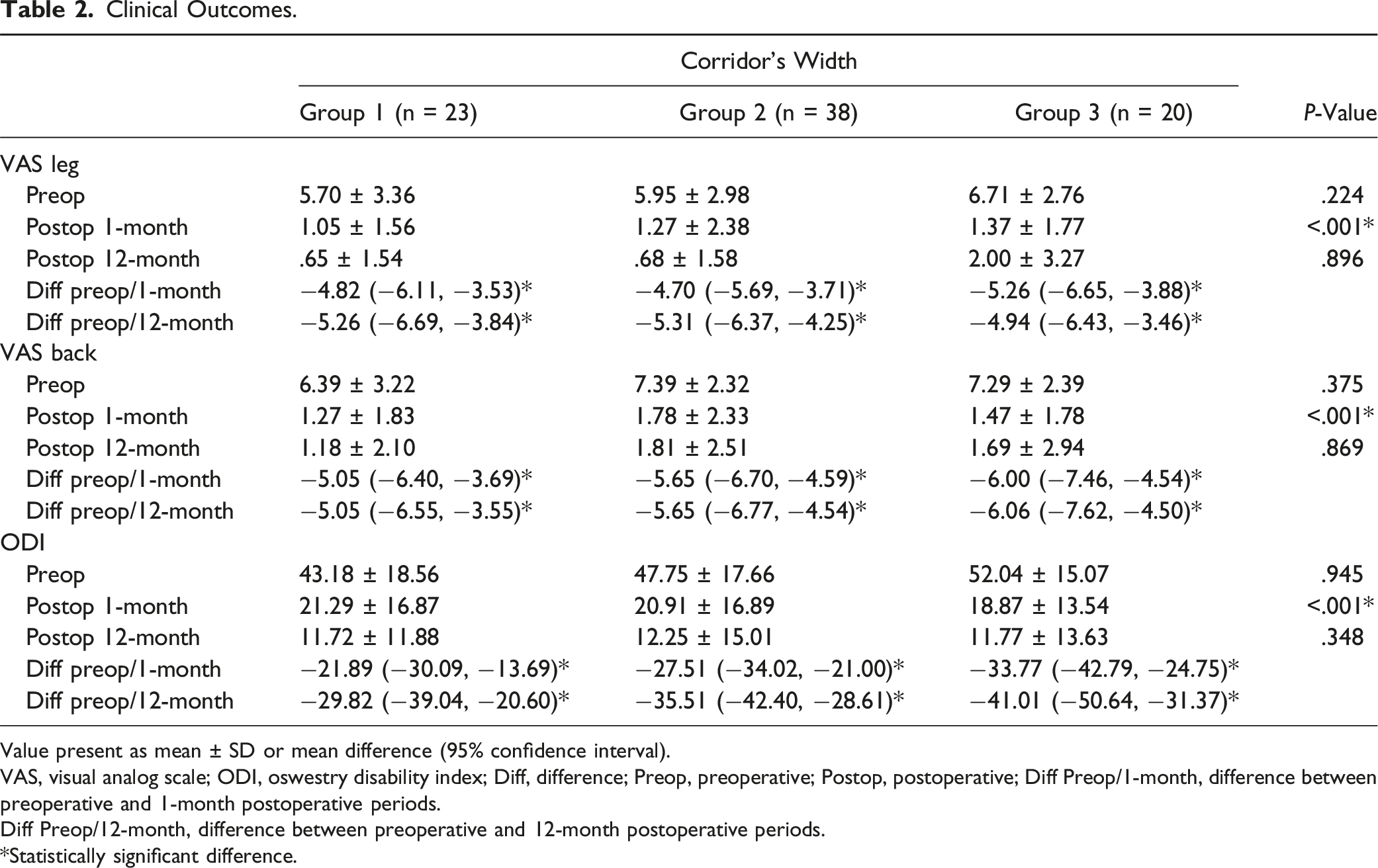
Value present as mean ± SD or mean difference (95% confidence interval).
VAS, visual analog scale; ODI, oswestry disability index; Diff, difference; Preop, preoperative; Postop, postoperative; Diff Preop/1-month, difference between preoperative and 1-month postoperative periods.
Diff Preop/12-month, difference between preoperative and 12-month postoperative periods.
*Statistically significant difference.
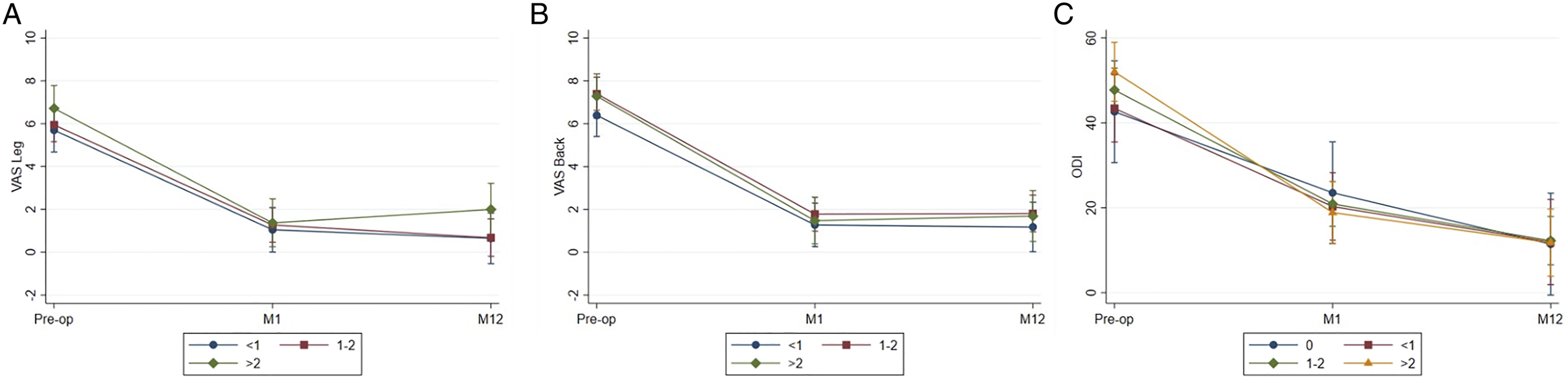
VAS (A) leg and (B) back pain scores, and (C) ODI scores comparison between preoperative, 1-month, and 12-month post-operation.
Complications.
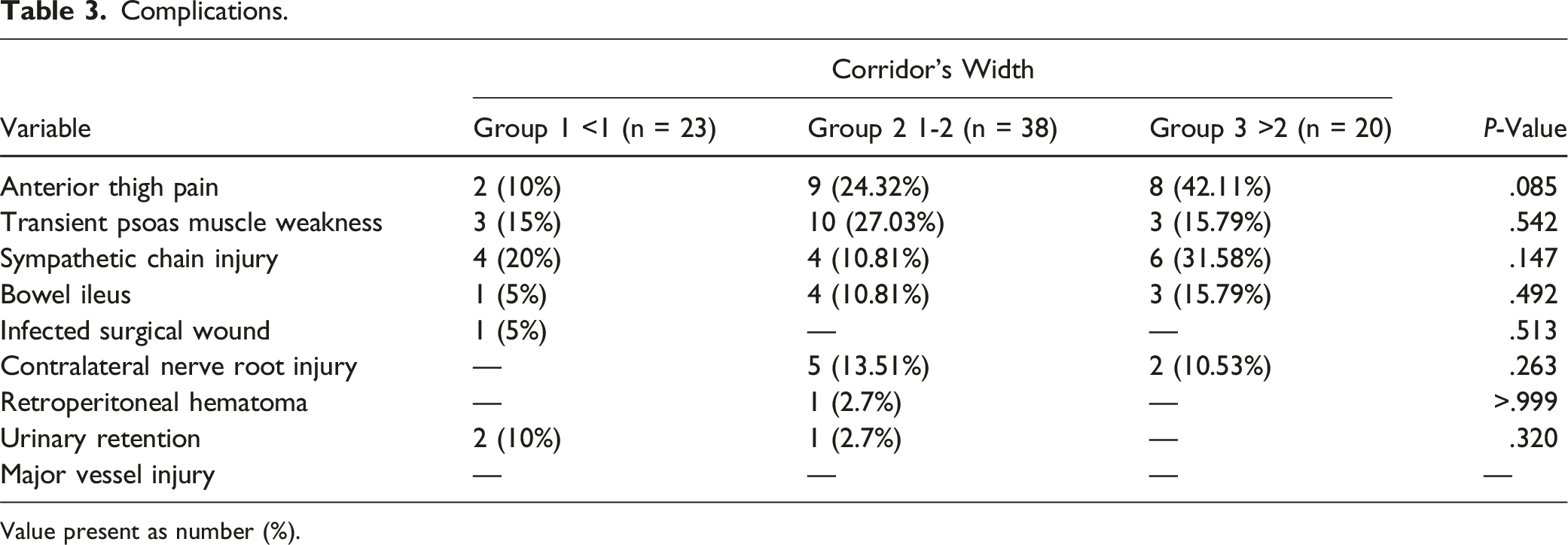
Value present as number (%).
Radiographic Outcomes.
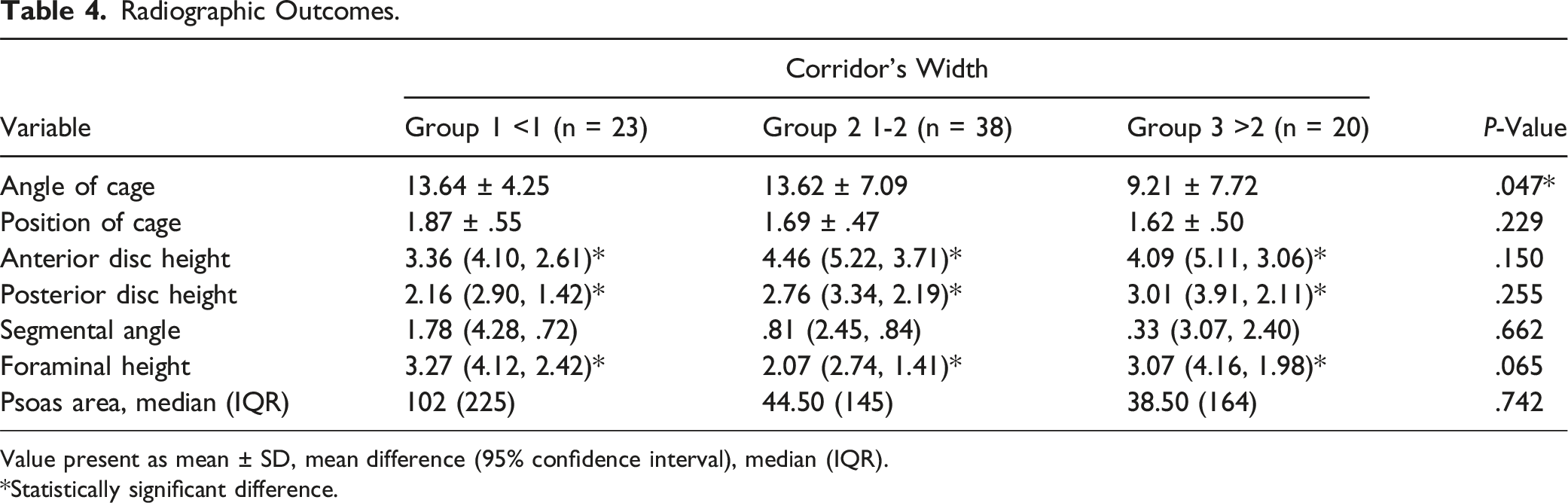
Value present as mean ± SD, mean difference (95% confidence interval), median (IQR).
*Statistically significant difference.
Discussion
In this study, the authors found that the clinical outcomes, including the VAS score for back and leg pain and the ODI score of the patients who underwent the OLIF procedure, which included L4-5 level, improved significantly in all groups of the corridor’s width at 1- and 12-month postoperative follow-up. The clinical results of this study were in accordance with several studies that reported improvements in clinical outcomes after the OLIF procedure. Abbasi et al 8 performed 303 OLIF procedures on a total of 568 spinal levels. At the 1-year follow-up, pain scores improved from 8.6 ± 1.3 to 4.1 ± 3.0, and the ODI score improved from 56.6 ± 15.3% to 38.6 ± 21.4%. Another retrospective study by Abbasi et al 9 reported significant improvement in pain scores and functional outcome scores after performing the OLIF in patients diagnosed with lumbar degenerative diseases.
In addition, we found comparable complication rates in all 3 groups of the corridor’s width. No major vascular injury was found in any group. The complication rates of this study were in line with various studies. Zeng et al 10 reported overall 32.34% complication rates in 235 patients, including approach-related complications such as vascular injury, psoas muscle hematoma, and psoas muscle weakness. A previous study conducted by Li et al 11 reported that intraoperative major vessel injuries occurred at .9%. These vascular structures are mostly injured due to forceful traction during the approach to the oblique corridor area and disc space. The prevalence of these complications ranged from zero to 52.9%. Another common complication of the OLIF procedure is anterior thigh symptoms. Cheng et al 12 reported in a study of 79 patients and found that 9 patients (11.4%) had ipsilateral transient psoas weakness, 2 patients (2.5%) had ipsilateral transient quadriceps weakness, and 17 patients (21.5%) had groin or thigh numbness and pain.
In theory, the narrow or no-corridor group required more dissection in the corridor and more psoas muscle retraction to gain adequate exposure to the targeted intervertebral disc. However, we found similar rates of anterior thigh pain, transient psoas muscle weakness, and lumbar sympathetic chain injury, regardless of the corridor width. In addition, our study showed that the patients with a narrow or no corridor (<1 cm)-countably 23 out of 81 patients (28%)-could undergo an OLIF procedure at L4-5. None of the patients in this group was abandoned or changed the procedure during the operation. This means that performing the OLIF procedure is fairly safe, even for patients who have a narrow or no oblique corridor. Moreover, a meticulous dissection of soft tissue around the oblique corridor and gentle retraction of the psoas muscle played essential roles in limiting the approach-related complications. This study demonstrated a contrast result to some previous studies. Ng et al 6 reported that 25% of the patients had no corridor for accessing the L4-5 level due to obstruction of vessels and should be contraindicated for performing the OLIF procedure. Virk et al 13 described that the presence of major vascular structures obscuring the surgical field on the preoperative evaluation should be a contraindication to performing the lateral lumbar interbody fusion.
Concerning the radiographic outcomes, the studied parameters, including position of the cage, differences in anterior and posterior disc height, foraminal height, segmental angle, and psoas muscle cross-sectional area between the preoperative and postoperative periods, were not significantly different between the three groups. The improvement in ADH, PDH, FH, and segmental angle of this study was in accordance with several studies.7,14 The angle of the cage was the only radiographic parameter that showed significantly different results between these three groups, in which group 3 had a smaller angle than the other two groups. Since the wider corridor offers more working space and requires less psoas muscle retraction, the surgeon can insert the cage in an orthogonal trajectory more comfortably compared with the narrow corridor.
The limitations of this study were that it was retrospective in nature and had a small sample size. The patients’ clinical outcomes had been followed up to only 1 year after the operation. The authors studied the corridor’s width only at L4-5 level. In addition, we did not study the impact of psoas muscle volume and the regional deformity on the radiographic measurements.
Conclusions
The oblique corridor’s width does not affect the clinical outcomes, complications, or radiographic findings, including the position of the cage, anterior and posterior disc height, segmental angle, and foraminal height after the L4-5 included OLIF procedure. Only the angle of the cage was affected by the size of the corridor. Thus, the OLIF procedure can be performed safely even in patients with narrow or no oblique corridor.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.