
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Selecting the last substantially touched vertebra (LSTV) or the lastly touched vertebra (LTV) as the lowest instrumented vertebra (LIV) has been shown to prevent distal adding-on (DA) in Lenke 1A and 2A curves or Lenke 1B and 1C curves, respectively. However, DA was still observed in our cohort even when fusing at or distal to STV or LTV when undergoing thoracic curve fusion (TCF). The purposes of this study are (1) to identify factors associated with the occurrence of DA when LIV for TCF is at or distal to LTV/LSTV, and (2) to demonstrate the effectiveness of LIV-index, defined as the summation of the proximity of LIV relative to neutral vertebra (NV) and stable vertebra (SV) as (LIV-NV) + (LIV-SV), in predicting postoperative DA.
Methods
A multicenter observational retrospective analysis was conducted on AIS patients who underwent TCF for major thoracic curves (MTCs, Lenke 1&2 curves). Subgroup analysis was performed between the DA and non-DA groups.
Results
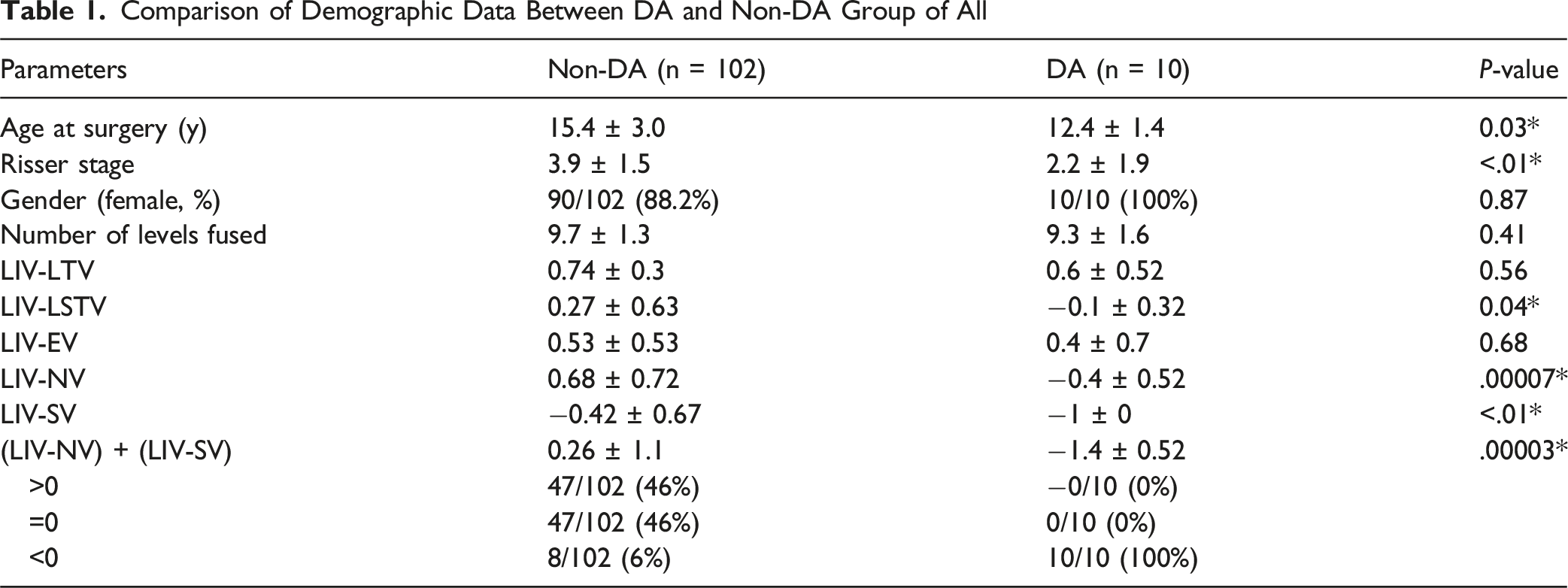
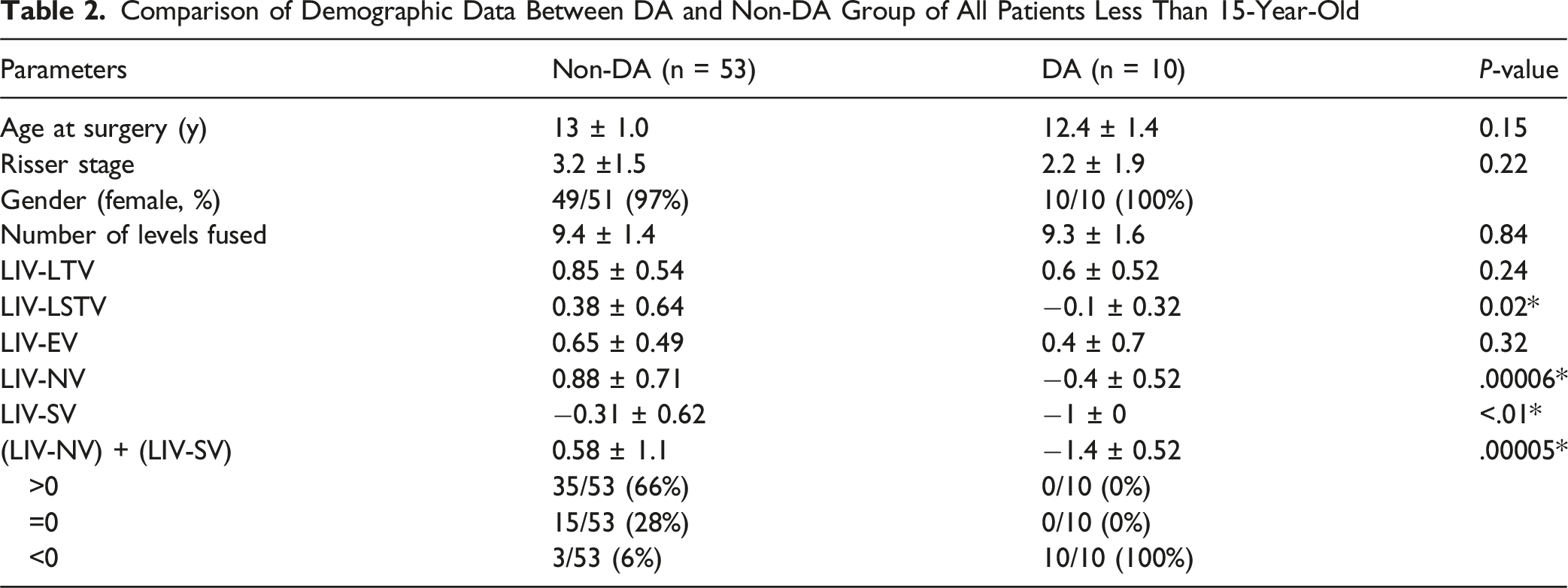
112 patients were included in the study with 10 patients presenting with DA during follow up. All patients in the DA group had an LIV-index < 0, indicating it a significant risk factor for DA (sensitivity = 100%, specificity = 92%, PPV = 55.5%, NPV = 100%, P < 0.001), especially for patients under 15-year-old (sensitivity = 100%, specificity = 94%, PPV = 77%, NPV = 100%, P < 0.001).
Conclusion
When fusing at or distal to LTV/LSTV in surgery for Lenke type 1 and 2 curves, the LIV-index can be used in clinical practice to prevent postoperative DA, particularly in younger patients.
Keywords
Introduction
The goals of surgical treatment for adolescent idiopathic scoliosis (AIS) are to achieve a 3-dimensional correction of the spinal deformity while optimizing spinal function and flexibility. Since 1958, selective thoracic fusion (STF) or thoracic curve fusion (TCF) has been an effective treatment option for correcting structural thoracic curves in AIS. This approach relies on the simultaneous correction of the unfused compensatory lumbar curves to achieve a balanced spine.1,2 However, inappropriate selection of lowest instrumented vertebra (LIV) may lead to the postoperative distal adding-on (DA) phenomenon, which is often associated with unsatisfactory clinical outcomes. 3
Selecting the last touching vertebra (LTV) or last substantially touched vertebra (LSTV) as the LIV has been shown to reduce the incidence of postoperative DA in Lenke 1A and 2A curves while selecting an LIV more cranial to the LTV is a recognized risk factor for postoperative DA in Lenke Type 1B and 1C curves.4-7 In fact, choosing the LTV as the LIV in patients with Lenke type 1 and 2 curves provides acceptable positioning of the LIV relative to the central sacral vertical line (CSVL) at long-term follow-up. 8 However, we still observed postoperative DA in Lenke type 1 and 2 curves treated with TCF, even when the LIV was at or distal to LTV or LSTV. Therefore, other factors related to LIV selection would also affect the occurrence of postoperative DA.
Neutral vertebra (NV) and stable vertebrae (SV) have also been reported as references for LIV selection in Lenke Type 1B and 1C curves.5,9 Recent systematic reviews and meta-analyses have demonstrated that multiple anatomical landmarks including the end vertebra (EV), neutral vertebra (NV), and stable vertebra (SV) all play important roles in LIV selection, with pooled odds ratios ranging from 2.43 to 4.52 for distal adding-on when LIV is placed proximal to these landmarks.10,11 It is intriguing to consider whether the proximity of the LIV relative to NV and SV also plays a role in determining the selection of LIV in addition to the concept of LTV or LSTV. The purposes of this study are (1) to identify factors related to the occurrence of postoperative DA when LIV for TCF is at or distal to LTV or LSTV, and (2) to demonstrate the effectiveness of the LIV-index, defined as the summation of the proximity of LIV relative to NV and SV, expressed as (LIV-NV) + (LIV-SV), in predicting postoperative DA.
Materials and Methods
This study was approved by the institutional review boards of the authors’ institutions (IRB number: 202105116RINA and 202100912B0). After approval by the institutional review board, a retrospective study of medical records and radiographs was performed on AIS patients who underwent thoracic curve fusion (TCF) with LIV at or above L1 and at or distal to LTV at two medical centers from January 2009 to July 2019. The inclusion criteria were as follows: age at surgery ≥ 10 years, Lenke classification as type 1 and 2 except type 1/2AR , and a minimum follow-up of 2 years with a complete set of radiographs. All surgeries were performed by one of the three experienced orthopedic surgeons with all pedicle screw constructs. Combination of hooks over the upper instrumented vertebra (UIV) was used only in a few selected cases. Clinical and radiographic measures were collected from medical records and erect standing anteroposterior radiographs of the whole spine taken before surgery, when able to stand independently after surgery, 1 year and 2 years postoperatively, and at the final follow-up. Categorical variables included Lenke classification, Risser stage, lumbar modifier, location of the LIV, LTV, LSTV, NV and SV and LIV-index, which represents the summation of the proximity of LIV relative to NV and SV in level as (LIV-NV) + (LIV-SV) and a more positive value refers to LIV located more distally. Radiographic measurements were collected, including the proximal and main thoracic (PT&MT) Cobb angle, thoracolumbar/lumbar (TL/L) Cobb angle, T5-T12 kyphosis, T12-S1 lordosis, sagittal balance, and coronal balance, as well as the apical translation of thoracic curves (TCs) and lumbar curves (LCs). The measurement was performed by two independent examiners. DA was defined as a more than 5° increase in the angulation of the superior end-plate of LIV+1 to the inferior endplate of LIV or more than 5 mm in deviation from the CSVL of the LIV+1.12,13 Mann-Whitney U test and Chi-square test were used for the subgroup analysis between groups of DA and non-DA patients. For diagnostic accuracy measures (sensitivity, specificity, positive predictive value, and negative predictive value), exact binomial confidence intervals were calculated using the Clopper-Pearson method, and the P-value for the diagnostic test performance was derived using Fisher’s exact test. 14 The data were analyzed using SPSS 20.0 statistical software (SPSS Inc., Chicago, IL) and statistical significance was defined as a P value less than 0.05.
Results
Comparison of Demographic Data Between DA and Non-DA Group of All
Comparison of Demographic Data Between DA and Non-DA Group of All Patients Less Than 15-Year-Old
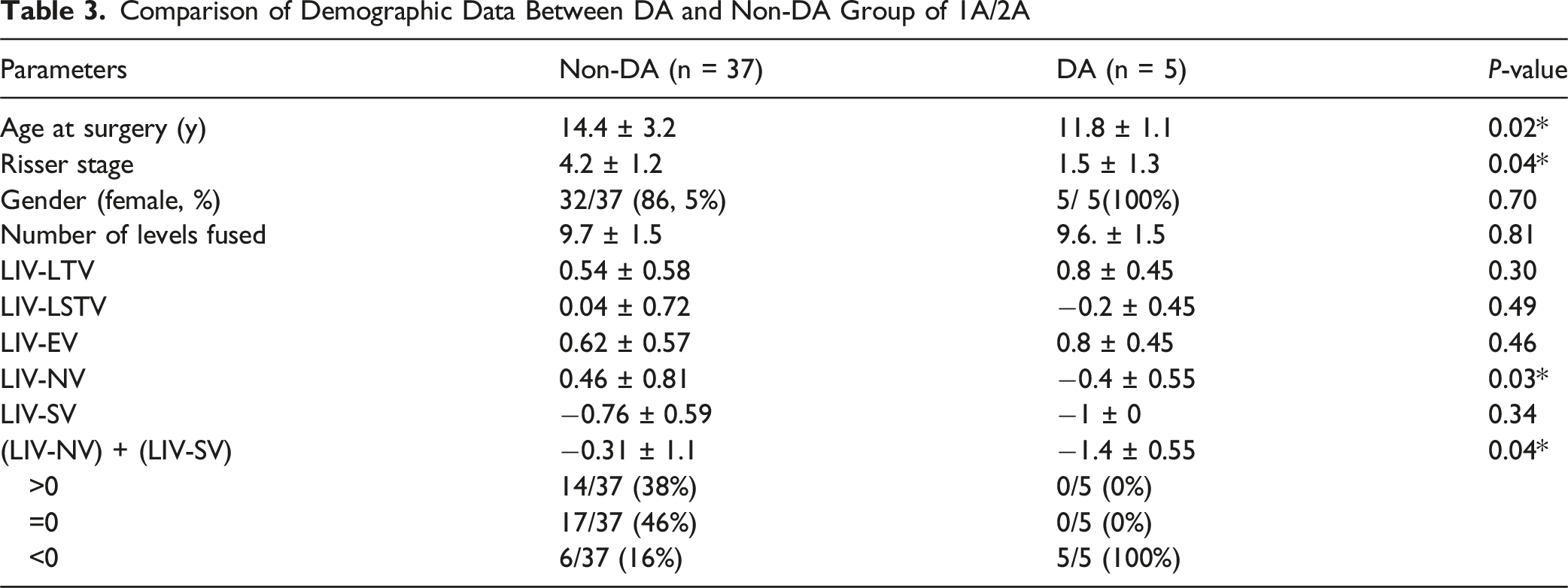
Comparison of Demographic Data Between DA and Non-DA Group of 1A/2A
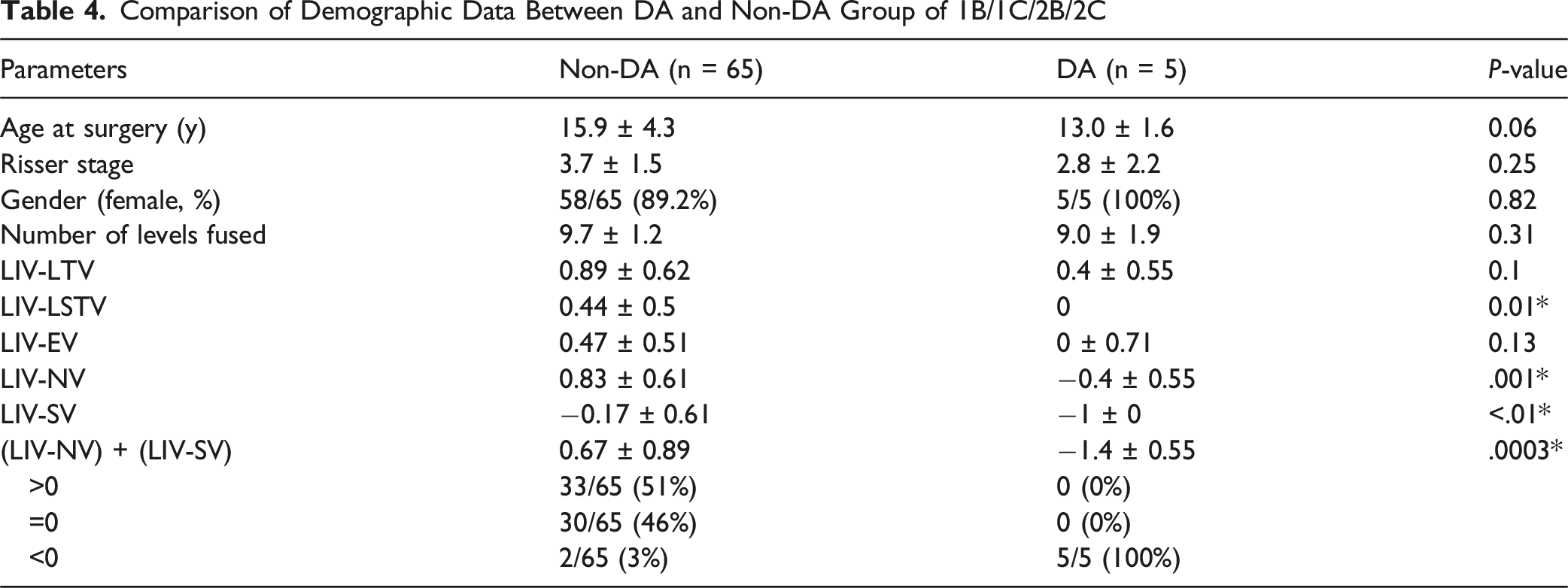
Comparison of Demographic Data Between DA and Non-DA Group of 1B/1C/2B/2C
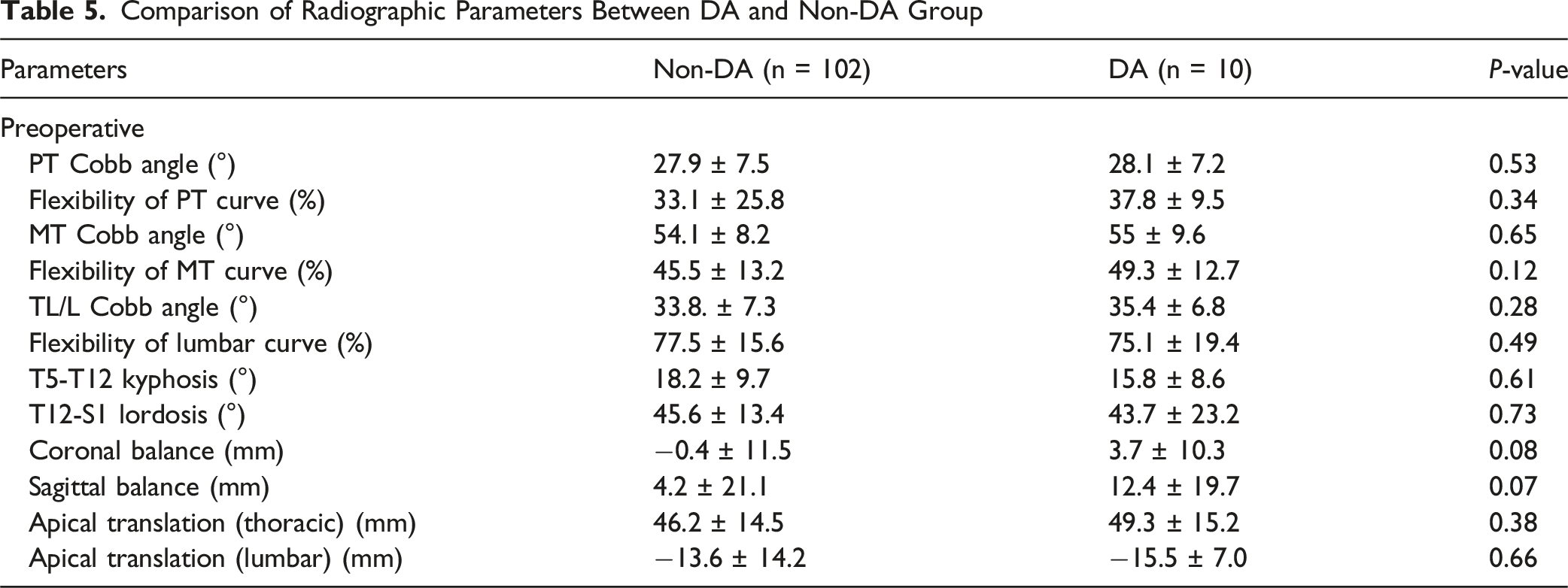
Comparison of Radiographic Parameters Between DA and Non-DA Group
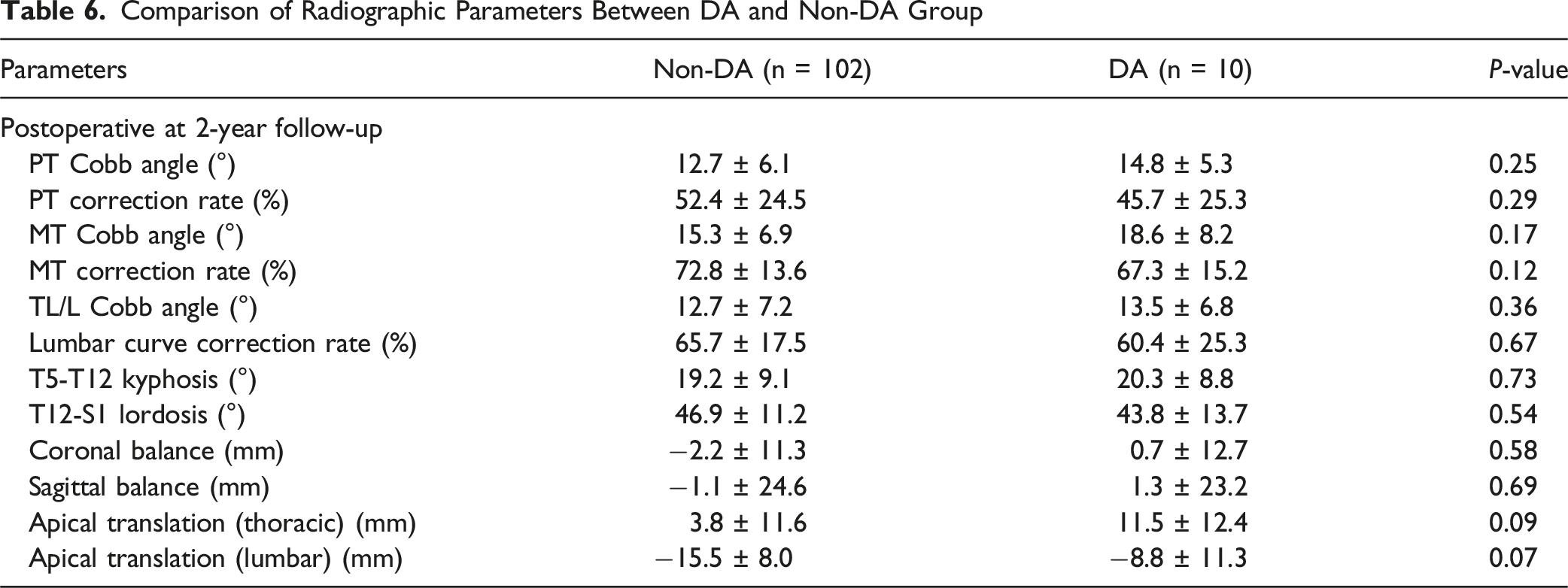
Comparison of Radiographic Parameters Between DA and Non-DA Group
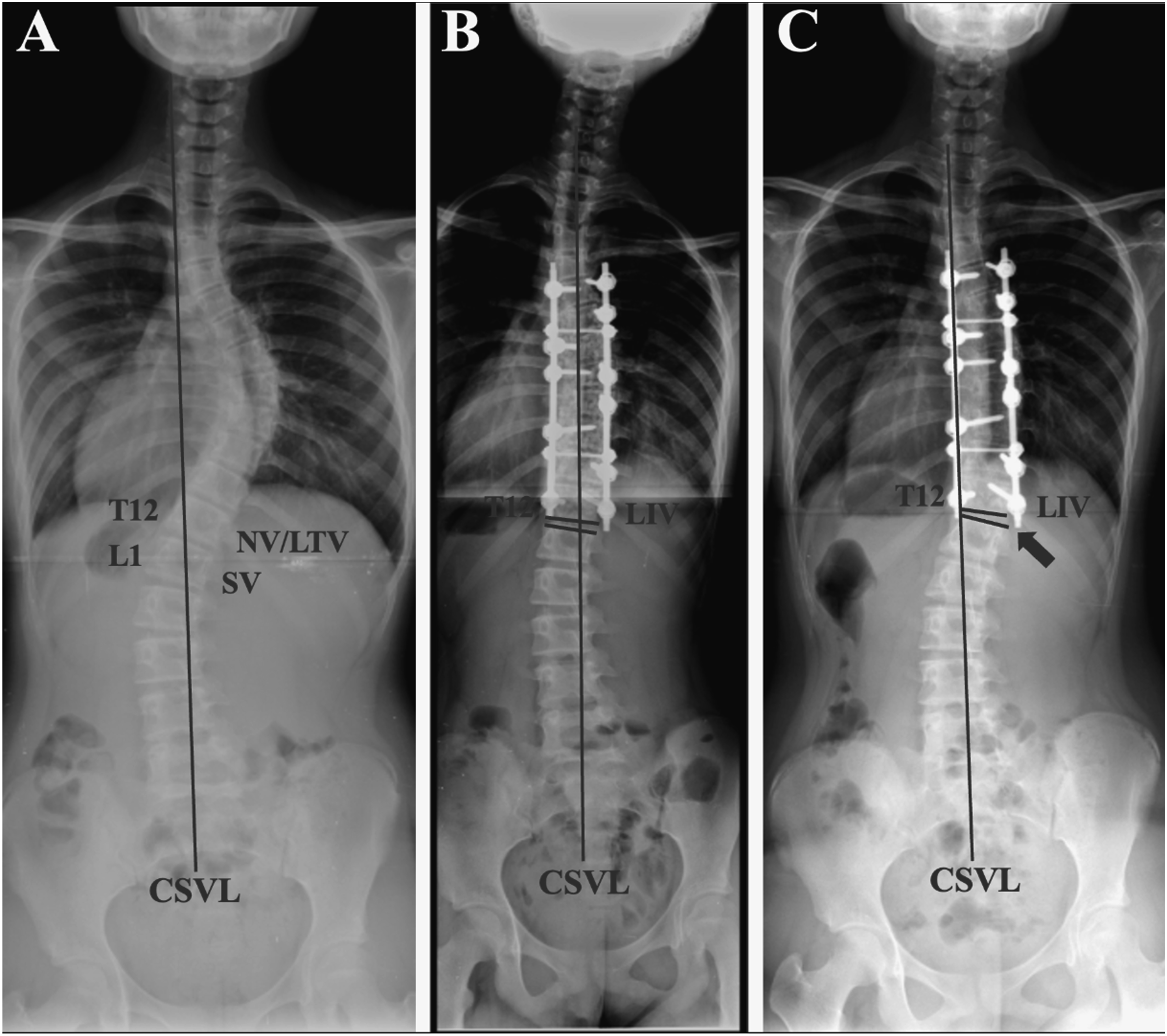
(A) Preoperative and (B) Immediately Postoperative Erect Standing Whole-Spine Radiographs of a 13- Year-Old Girl With Lenke 1BN Curve. The Levels of LIV, LTV, LSTV, NV, and SV Corresponded to T12, T12, T12, T12, L1, Respectively. The LIV-Index for This Patient Was Calculated as (LIV-NV) + (LIV-SV) = 0 + (−1) = −1 (C) Distal Adding-on Phenomenon Was Observed 2 Years After Surgery, as Indicated by the Arrow
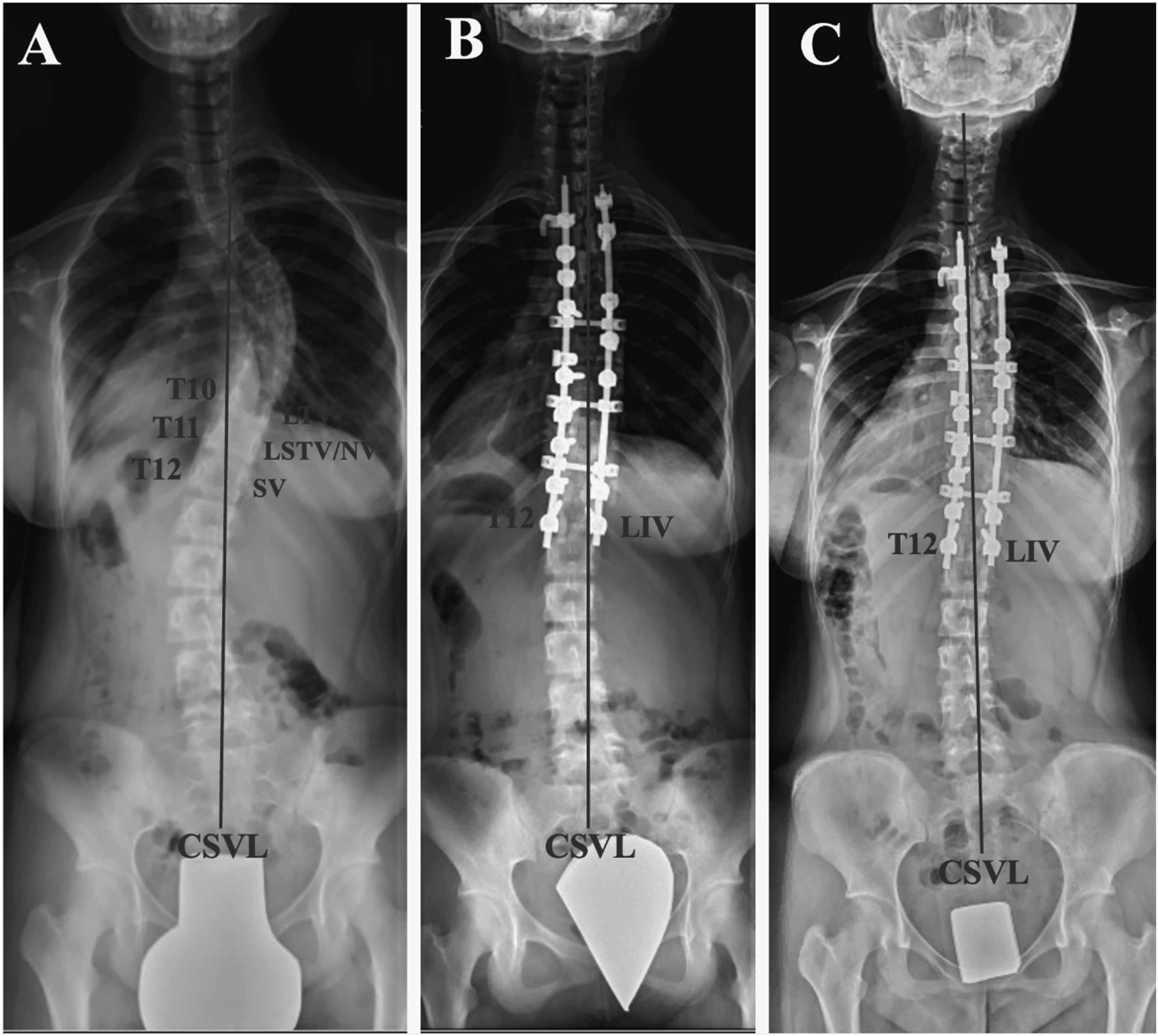
(A) Preoperative and (B) Immediately Postoperative Erect Standing Whole-Spine Radiographs of a 14- Year-Old Girl With Lenke 1BN Curve. The Level of LIV, LTV, LSTV, NV, and SV Corresponded to T12, T10, T11, T11, T12, Respectively. The LIV-Index for This Patient Was Calculated as (LIV-NV) + (LIV-SV) = 1 + 0 = 1 (C) Distal Adding-on Phenomenon Was Not Observed 2 Years After Surgery
Discussions
Several guidelines for determining the LIV in AIS surgery have been proposed and have evolved alongside advances in spinal implants. Cho et al recently introduced the concept of LTV for selecting LIV, based on a study of 195 patients with Lenke 1A curves. 12 They discovered that fusing down to LTV could reduce the incidence of postoperative DA. Matsumoto et al. found that positioning LIV more cranial than LTV was significantly associated with DA in a study of Lenke 1A patients. 6 Cao et al. reported that placing LIV at or distal to LTV might prevent postoperative DA in Lenke 2A curves. 4 Additionally, Qin et al further differentiated LSTV from Radiographic measurements were collected LTV and recommended using LSTV as the LIV to avoid DA in Lenke 1A patients. 7
Conversely, selecting the LIV for Lenke Type 1B and 1C curves remains a subject of debate, with few specific studies available. One study evaluating 46 patients with Lenke Type 1B and 1C curves identified having the LIV at or cranial to LTV as a significant risk factor for postoperative DA. 5 Another study involving 69 patients with Lenke Type 1B or 1C curves found that intraoperative disc angulation below LIV exceeding 3° was associated with postoperative DA. 9 Additionally, using the LTV as the LIV for Lenke type 1 and 2 curves, as well as for various lumbar modifiers, yielded acceptable outcomes with a minimum 5-year follow-up. 8
While the current LIV-index combines coronal balance (SV) and axial rotation (NV), the exclusion of the EV—which defines the anatomical end of the primary curve—may underestimate mechanical implications at the LIV. Previous studies have demonstrated that the difference between LIV and EV is a significant risk factor for adding-on, with univariate analysis showing that the relationship between LIV and EV levels affects postoperative outcomes. 4 Although LIV-EV was not statistically significant in our cohort, this may be due to our specific inclusion criteria requiring LIV at or distal to LTV/LSTV. In future studies, a “three-axis” index incorporating EV alongside NV and SV may offer better comprehensiveness by accounting for the complete anatomical definition of the curve boundaries. Recent comparative studies of nine different LIV selection criteria have shown that incorporating multiple anatomical landmarks can improve prediction accuracy, with some criteria achieving adding-on incidences as low as 5.9% 11
While the present study focuses on coronal plane parameters for determining LIV, sagittal alignment—especially the presence of thoracolumbar junctional kyphosis (TLK)—can significantly influence postoperative stability. Our previous cohort focusing on postoperative distal junctional kyphosis (DJK) in AIS patients after TCF and the following meta-analyses performed by Jia et al that included the cohort have demonstrated that postoperative thoracic kyphosis ≥25° and thoracolumbar kyphosis ≥10° are related to distal junctional kyphosis (DJK), with LIV placement above the sagittal stable vertebra showing a 13.2% rate of DJK compared to 0.8% when LIV is placed at or below the sagittal stable vertebra.18,19 In cases with TLJ kyphosis, stopping instrumentation at a kyphotic LIV (eg, T12 or L1) may predispose to junctional failure. Previous recommendations suggest that sagittal kyphosis at the thoracolumbar junction (T10-L2) should be less than 20° and a lordotic disc angle below the LIV is important to prevent distal junctional kyphosis. 1 Despite our beholding concept that the progression of coronal plane is independent of sagittal alignment once the sagittal stability is achieved, future versions of the LIV-index should consider integrating sagittal modifiers, potentially incorporating the relationship between LIV and the sagittal stable vertebra (SSV) to provide a more comprehensive three-dimensional assessment of fusion level selection
A major concern lies in the inclusion of skeletally immature patients—particularly those with low Risser stages—for selective thoracic fusion. The literature consistently demonstrates that skeletal immaturity is a significant risk factor for distal adding-on and junctional complications, with peak curve progression occurring at Tanner stage 2-3 just after the onset of the pubertal growth spurt. 17 Studies have shown that male sex, skeletal immaturity (low Risser stage), and undercorrection are associated with higher rates of coronal decompensation, with some series reporting up to 50% of patients with Risser 4-5 staging at the time of selective fusion.20,21 The appropriateness of TCF in skeletally immature patients should be critically evaluated, as the higher risk of DA and junctional failure in this population may confound the predictive value of any LIV selection criteria. The literature suggests that closure of the triradiate cartilage is important to prevent adding-on and distal junctional problems, and skeletal maturity as determined by the triradiate cartilage is one of the best predictors of successful outcomes after selective fusion.1,22 However, our findings suggest that the LIV-index may serve as a valuable tool precisely in these high-risk younger patients where traditional anatomical landmarks may be insufficient. While skeletal immaturity is a recognized risk factor for DA, our sub-analysis in patients under 15 years demonstrated that the LIV-index maintained strong predictive ability even when the difference in Risser stage became non-significant (P = 0.22). This suggests that the LIV-index provides predictive value beyond skeletal maturity alone, potentially through its incorporation of specific anatomical relationships that remain relevant regardless of growth potential. Actually, given the fact that majority of patients under 15 years in our cohort didn’t develop DA (53/63 = 84.1%) and the high specificity of LIV-index (94%), the LIV-index exactly serves as a valuable supplemental tool precisely in these younger patients where traditional anatomical landmarks may be insufficient. The index may be identifying biomechanical vulnerability patterns that are independnt of yet complementary to, skeletal maturity assessment
Despite findings suggesting that selecting LTV or LSTV as the LIV can reduce the incidence of postoperative DA, previous studies indicate that 50% to 74% of patients with an LIV proximal to LSTV achieved favorable outcomes without DA (negative predictive value, NPV, 26%-50%) at final follow up. However, the current study revealed that the LIV-index could be more effective than LTV or LSTV for selecting LIV, offering better discrimination as a risk factor for postoperative DA, particularly for patients with major thoracic curves (MTCs, Lenke 1&2 curves) of various lumbar modifiers (NPV 55.5%), especially in those younger than 15 years old (NPV 77%).
The selection of LIV at either LTV or LSTV is primarily guided by considerations of curvature in the coronal plan. However, unsatisfactory outcomes have still been observed when LIV for posterior spinal fusion in AIS is positioned at a rotated vertebra. 23 In Cho et al's study, patients with postoperative DA were fused 1.6 levels proximal to the NV, while those without DA had LIV only 0.9 levels proximal to the NV (P = 0.023). This finding suggests that selecting the LIV at neutral or slightly rotated vertebra is associated with a lower likelihood of postoperative DA. 12
Similarly, Qin et al identified greater vertebral rotation at one level proximal to the LSTV (LSTV-1) as an additional risk factor for DA when LSTV-1 was chosen as the LIV. 7 Sarwahi et al proposed that selecting a minimally rotated LTV (Nash-Moe grade 0/1) as the LIV can reduce the number of fusion levels without compromising radiographic outcomes. 24
Recent studies have shown that the relative position of LIV to NV (LIV-NV) and to SV (LIV-SV) are strongly associated with postoperative DA and may be more reliable indicators than the relative position of LIV to LTV (LIV-LTV).5,9 This insight prompted us to combine LIV-NV and LIV-SV into a single criterion, the LIV-index, to predict postoperative DA. In the current study, the LIV-index demonstrated excellent discrimination, with a sensitivity of 100%, specificity of 92%, PPV of 55.5%, and NPV of 100% (P < 0.0001).
In the current study, the overall incidence of postoperative DA was 8.9%, significantly lower compared to the approximately 20% incidence reported in previous studies where some patients had LIV proximal to LTV.5,9,25 This finding reaffirms that fusing at or distal to LTV can reduce the likelihood of postoperative DA.
Additionally, all patients with postoperative DA in the current study were younger than 15 years old and lower Risser stage at the time of surgery. This finding aligns with previous literature indicating that skeletal maturity is associated with postoperative DA. 16 In comparison to a cohort study that identified factors related to the progression of residual lumbar curves in AIS patients receiving TCF, 26 the age difference between the non-progression and the progression group in that study was more significant than the difference observed between the DA and the non-DA group in the current study.
When specially focusing on patients under 15 years old, despite the difference in Risser stage becoming non-significant, the LIV-index continued to demonstrate strong predictive ability for postoperative DA (sensitivity = 100%, specificity = 94%, PPV = 77%, NPV = 100%, P < 0.0001). This suggests that the LIV-index could serve as a valuable supplement to LTV or LSTV for LIV selection, particularly for avoiding postoperative DA in younger AIS patients.
The current study has several limitations, including a small sample size, a non-randomized design that may reduce statistical power, and potential biases. Additionally, due to ongoing debates regarding the best method for choosing LIV, pre-operative plain films may not have been optimally taken for the purpose of LIV selection. Some researchers advocate for alternative imaging techniques, such as traction X-ray under general anesthesia (TrUGA), prone X-rays, or supine X-rays, rather than the conventional upright radiograph method.24,27,28 The exclusion of EV from our current LIV-index may limit its comprehensiveness, and future studies should investigate a three-dimensional index incorporating sagittal parameters. Additionally, the study’s focus on patients with LIV at or distal to LTV/LSTV may have created a selection bias that could affect the generalizability of our findings to all AIS patients undergoing selective thoracic fusion. Despite these limitations, the current study is the first to introduce the LIV-index, which integrates the concepts of coronal balance (LIV-SV) and vertebral column rotation (LIV-NV). The LIV-index shows promise for application in Lenke type 1 and 2 curves with different lumbar modifiers.
Conclusions
When fusing at or distal to LTV/LSTV in the surgical treatment of Lenke type 1 and 2 curves, the LIV-index—defined as the sum of coronal balance (LIV-SV) and vertebral column rotation (LIV-NV)—can be utilized in clinical practice to guide LIV selection and help prevent postoperative DA, particularly in younger and skeletally immature patients. In the current study, no postoperative DA occurred when the LIV-index was ≥ 0. Specifically, postoperative DA can be avoided if LIV is chosen at LTV/LSTV when NV is proximal to LTV/LSTV. Conversely, if NV is at or distal to LTV/LSTV, it is advisable to consider placing LIV distal to LTV/LSTV or even at SV to minimize the risk of postoperative DA.
Footnotes
Authors’ Note
I-Hsin Chen is currently affiliated with: Department of Orthopedics, National Taiwan University College of Medicine and National Taiwan University Hospital, Taipei, Taiwan; Department of Orthopedics, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan; and Graduate Institute of Biomedical Engineering, National Taiwan University, Taipei, Taiwan. Po-Yao Wang is currently affiliated with: Department of Orthopedics, National Taiwan University College of Medicine and National Taiwan University Hospital, Taipei, Taiwan; Department of Orthopedics, Taipei Medical University Hospital, Taipei, Taiwan; and Department of Orthopedics, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: None of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of any aspect of this work. None of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submission of this work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. No author has had any other relationships, or has engaged in any other activities, that could be perceived to influence or have the potential to influence what is written in this work.