
Abstract
Study Design:
A retrospective cohort study.
Objective:
To investigate the factors contributing to the development of postoperative distal junctional kyphosis (DJK) in adolescent idiopathic scoliosis (AIS) patients who underwent posterior spinal fusion (PSF) with lowest instrumented vertebrae (LIV) at or above L1.
Methods:
Patients with Lenke type 1 or 2 curves who underwent PSF with LIV at or above L1 with a minimum follow-up of 2 years were evaluated. The primary outcome measure was the occurrence of postoperative DJK. Radiographic parameters of sagittal alignment and inclusion/exclusion of sagittal stable vertebra (SSV) in PSF were analyzed to determine their associations with the occurrence of postoperative DJK.
Results:
Overall, 122 patients (mean age: 15.1 ± 3.2 years) were included. The overall incidence of postoperative DJK was 6.6%. DJK was observed in 19.0% (8/42) of patients whose SSV was not included in PSF and not in patients with SSV included in PSF (n = 80). In the SSV-excluded group, univariate analysis found two significant risk factors for DJK: postoperative thoracic kyphosis (TK, T5-12) and postoperative thoracolumbar kyphosis (TLK, T11-L2). The ROC curve revealed that postoperative TK ≥ 25° and TLK ≥ 10° best predicted the occurrence of postoperative DJK in the SSV-excluded group. The incidence was significantly higher in cases with postoperative TK ≥ 25° or TLK ≥ 10° (7/13 = 53.8%) than in those with postoperative TK < 25° and TLK < 10° (1/29 = 3.4%).
Conclusions:
The current study revealed that postoperative TK ≥ 25° or postoperative TLK ≥ 10° with SSV excluded from PSF were related to DJK after PSF for Lenke type 1 and type 2 AIS. When the SSV is intended to be spared from PSF to save more motion segments, TK and TLK should be carefully evaluated and attained in a lesser magnitude (TK < 25°, TLK < 10°) after surgery.
Keywords
Introduction
Selective thoracic fusion (STF) has been performed in adolescent idiopathic scoliosis (AIS) patients who have a primary main thoracic curve with a compensatory lumbar curve. 1 STF limits fusion segments and allows preservation of more motion segments in the lumbar spine.2,3 However, preserving flexibility through the lumbar spine may increase the potential risk of developing an imbalance below the STF in either the coronal or sagittal planes.4-8
Distal junctional kyphosis (DJK) indicates an increase in kyphosis at the adjacent segment distal to the lowest instrumented vertebra (LIV) of the spinal fusion. DJK can lead to pain, imbalance, poor cosmesis, and degenerative disc disease due to increased mechanical stress on the adjacent segments.9,10 Although postoperative DJK has been repeatedly described in the literature, there are only a few studies have investigated the risk factors and predictive radiographic parameters of this postoperative sagittal decompensation.10,11
The concept of sagittal stable vertebrae (SSV) has been employed to select the LIV in posterior spinal fusion (PSF) for thoracic hyperkyphosis. 12 Yang et al. utilized this SSV concept to STF for AIS and demonstrated that choosing LIV at or below the SSV could prevent postoperative DJK. 13 However, in their study, only 17% of patients whose SSV was not included in the STF developed DJK. DJK did not develop in a large proportion of patients whose STF did not include the SSV. Therefore, there might be other factors related to the occurrence of DJK when SSV was not included in PSF. The purpose of this study was to further investigate possible contributing factors to the development of postoperative DJK in Lenke type 1 and 2 AIS patients who underwent PSF with LIV at or above L1.
Materials and Methods
This study was approved by the institutional review board at the institution of the corresponding author (IRB number: 202006002RINB). After approval by the Institutional Review Board, a retrospective study of medical charts and radiographs was conducted for AIS patients who underwent PSF at 2 tertiary hospitals from January 2009 to July 2017. The inclusion criteria were: patients’ age at surgery ≥ 10 years, Lenke type 1 or 2 curve, the LIV at L1 or above, and a minimum follow-up of 2 years with a complete set of radiographs. The LIV was selected according to Lenke’s recommendation as the most cephalad vertebra in the thoracolumbar/lumbar region that was at least touched by the central sacral vertebral line (CSVL) on an upright coronal radiograph. 14 Clinical and radiographic measures of the spinal deformity were collected from medical charts as well as erect standing anteroposterior and lateral radiographs of the whole spine taken before surgery, within 3 weeks after surgery, and at final follow-up.
Radiographic measurements were performed digitally on Picture Archive and Communication System (PACS) images. Coronal measures included the Cobb angles of the main thoracic curve. Sagittal measures included thoracic kyphosis (TK, upper endplate of T5 to lower endplate of T12), thoracolumbar kyphosis (TLK, upper endplate of T11 to lower endplate of L2), lumbar lordosis (LL, lower endplate of T12 to upper endplate of S1), sacral slope (SS), distal junctional angle (DJA, sagittal disc angle between LIV and LIV+1, LIV+1: the vertebra just distal to the LIV), focal kyphosis at LIV-LIV+1 (angle between the upper endplate of LIV and the lower endplate of LIV+1). Global sagittal alignment was measured using the sagittal vertical axis (SVA). The number of fused vertebrae, implant density (number of pedicle screws and hook/number of fused vertebrae), and Risser stage were also calculated. Distal junctional kyphosis (DJK) was defined as either focal kyphosis at LIV-LIV+1 ≥ 10° 10 or ≥ 5° of kyphotic change in sagittal disc angle between LIV and LIV+1 during follow-up after surgery. 15
Inclusion of the SSV in PSF for thoracic hyperkyphosis12,16 and in STF for AIS 13 has been considered as a factor preventing postoperative DJK. SSV was defined as the vertebral level at which 50% of the vertebral body was in front of the posterior sacral vertical line (PSVL) on an erect standing lateral radiograph (Figure 1 and 2). The relationship between inclusion/exclusion of SSV in the PSF and occurrence of postoperative DJK was also investigated in this study.
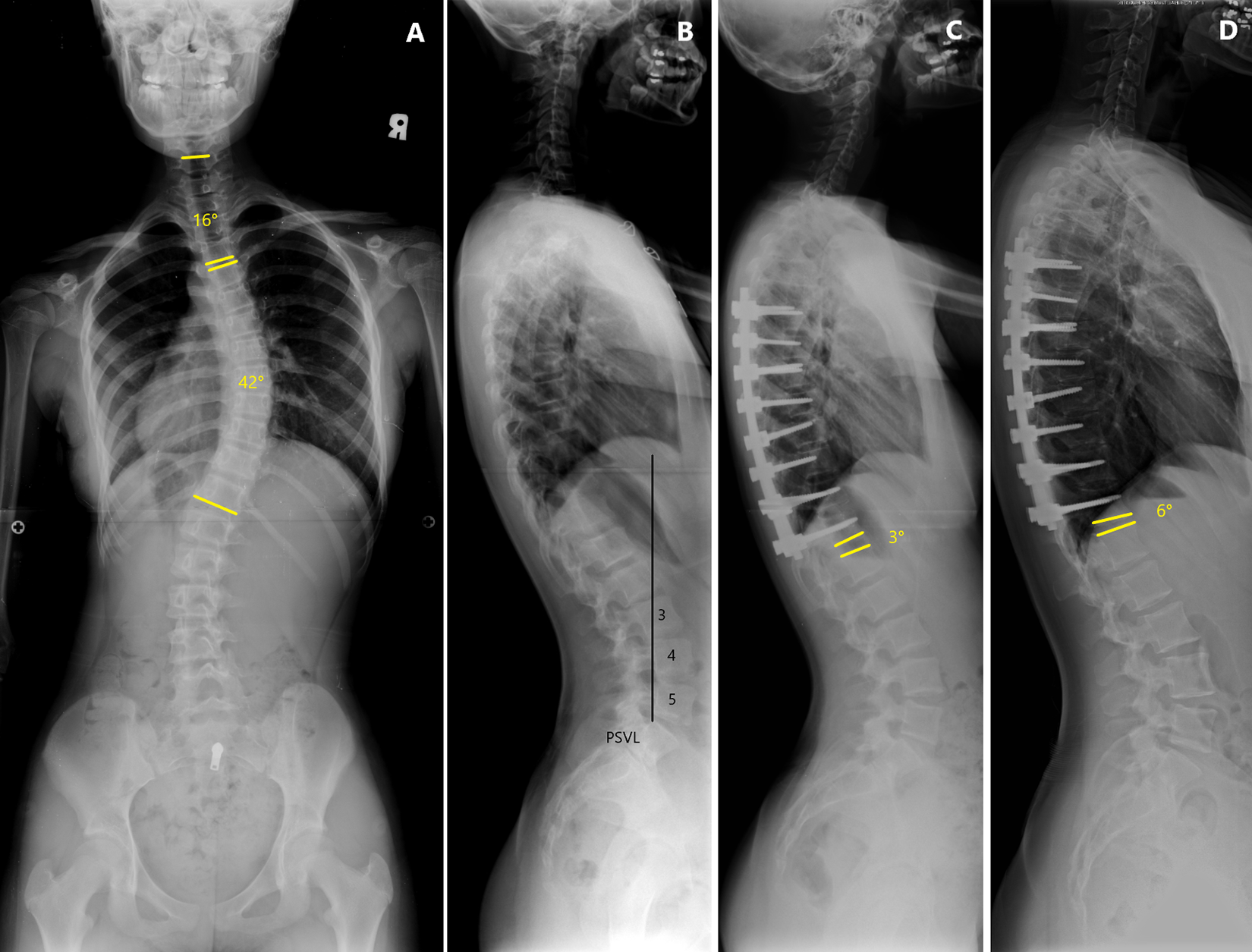
Erect standing whole-spine radiographs of a 10-year-old female patient with AIS. (A) Preoperative posteroanterior radiograph showing a main thoracic curve of 42°. (B) The lateral radiograph demonstrated utilization of the posterior vertical line (PSVL) to determine the sagittal stable vertebra (SSV) as the level at which 50% of the vertebral body was in front of the posterior sacral vertical line, which is L3 in this case. (C) Postoperative lateral radiograph demonstrating a 25° thoracic kyphosis (TK, T5-12), a 15° thoracolumbar kyphosis (TLK, T11-L2), and a 3° lordosis of the sagittal disc angle. Note that the surgeon chose the lowest instrumented vertebra (LIV) as T12, two level above sagittal stable vertebra (SSV), in this case. (D) The lateral radiograph taken 4 years after surgery demonstrated a 6° kyphosis of sagittal disc angle. 9° of kyphotic change in the sagittal disc angle below the LIV developed during follow-up, which met the criteria for postoperative distal junction kyphosis (DJK) in our study.
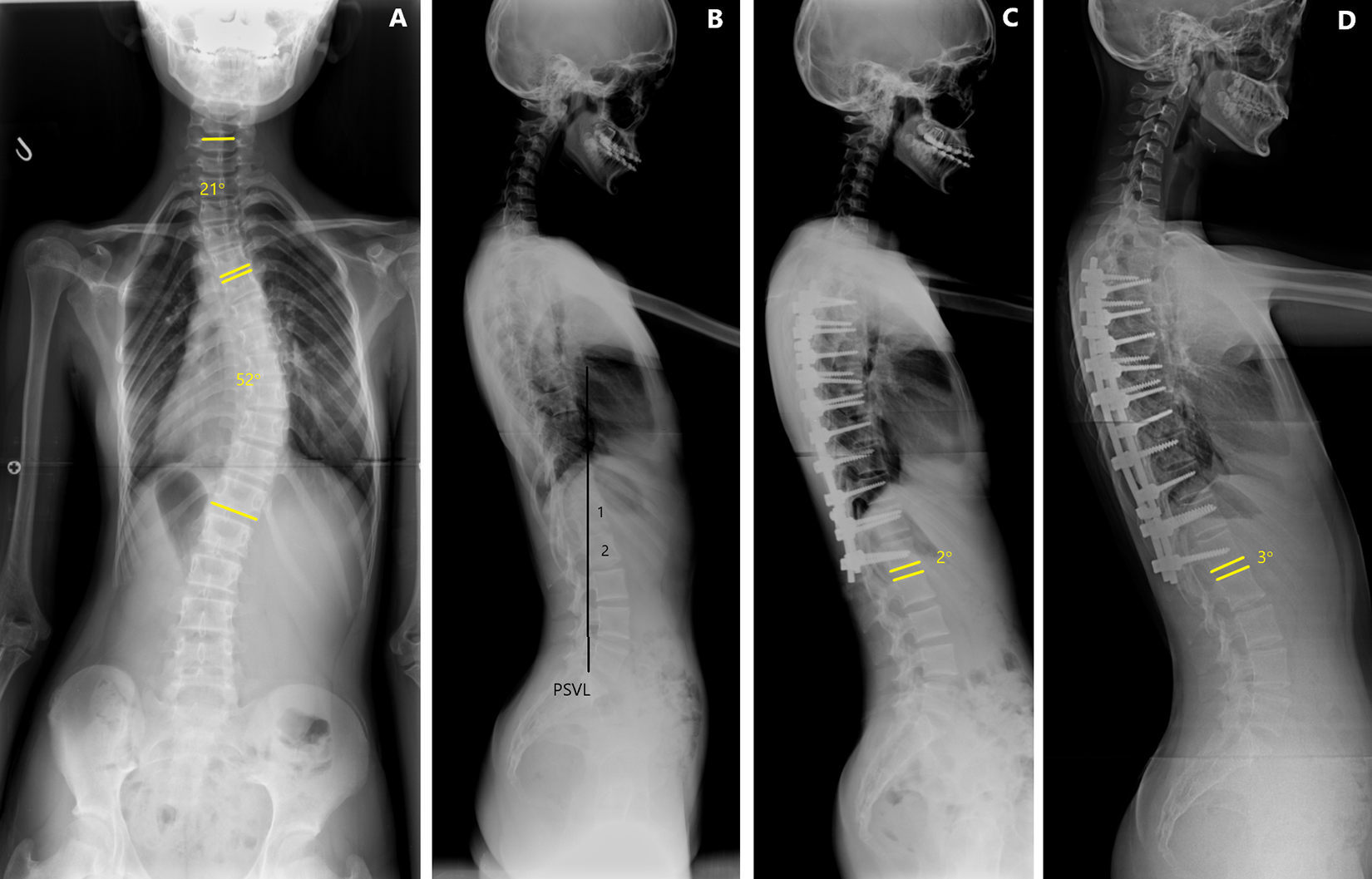
Erect standing whole-spine radiographs of a 15-year-old female patient with AIS. (A) Preoperative posteroanterior radiograph showing a main thoracic curve of 52°. (B) The lateral radiograph demonstrated that sagittal stable vertebra (SSV) was L1 in this case. (C) Postoperative lateral radiograph demonstrating a 2° lordosis of the sagittal disc angle. Note that the surgeon chose the lowest instrumented vertebra (LIV) as L1, at the same level as SSV. (D) The lateral radiograph taken 4 years after surgery demonstrated a 3° lordosis of sagittal disc angle. There was no distal junctional kyphosis in this case.
Statistical Analysis
Distributions of variables are given as means, standard deviations, and ranges. For the analysis between the 2 groups, a Mann-Whitney U test was used for continuous measures. Fisher’s exact test and the chi-square test were used for categorical data analysis. Receiver operating characteristic (ROC) curve analysis was used to determine the optimal cutoff value of the occurrence of DJK. A P-value of < .05 was considered statistically significant.
Results
A total of 122 patients (101 female and 21 male) met the criteria and were included in this study. Their mean age at the time of surgery was 15.1 ± 3.2 (range 10 – 25) years and Risser stage was 3.7 ± 1.4 (range 0 – 5). According to the AIS classification by Lenke et al., 17 there were 94 patients (77.0%) with type 1 (main thoracic) curve and 28 (23.0%) with type 2 (double thoracic) curve. The numbers of patients with lumbar modifiers A, B, and C were 60, 45, and 17, respectively. There were 89 patients with normal thoracic kyphosis (T5-12 kyphosis 10 – 40°), 2 with hyperkyphosis (> 40°), and 31 with hypokyphosis (< 10°). The mean number of vertebrae fused was 9.4 ± 1.3 (range 6 – 13). The average magnitude of the main thoracic curve was 53.4° ± 10.0° (range 40° – 86°) preoperatively and 20.2 ± 6.0° (range 7° – 45°) postoperatively with a correction rate of 62.2% ± 9.2% (range 41.5% – 86.5%).
The overall incidence of postoperative DJK was 6.6% (8/122) in the current study. Among 80 patients with SSV included in the PSF (SSV-included group), there were no cases with postoperative DJK. In cases in which the PSF did not include the SSV (SSV-excluded group), the incidence of postoperative DJK was 19.0% (8/42). The occurrence rate of postoperative DJK was significantly higher for patients in the SSV-excluded group than in the SSV-included group (P = 0.0001). A comparison of demographic data between the SSV-included group and the SSV-excluded group is shown in Table 1. There was no significant difference between the 2 groups with respect to sex, age at surgery, Risser stage at surgery, number of levels fused, implant density, Lenke type, and lumbar modifier. Noticeably, the mean level of the LIV was more caudal in the SSV-included group (12.4 ± 0.6; T11-L1) than in the SSV-excluded group (12.1 ± 0.6; T10-L1).
Comparison of Demographic Data between the SSV-Included Group and the SSV-Excluded Group.
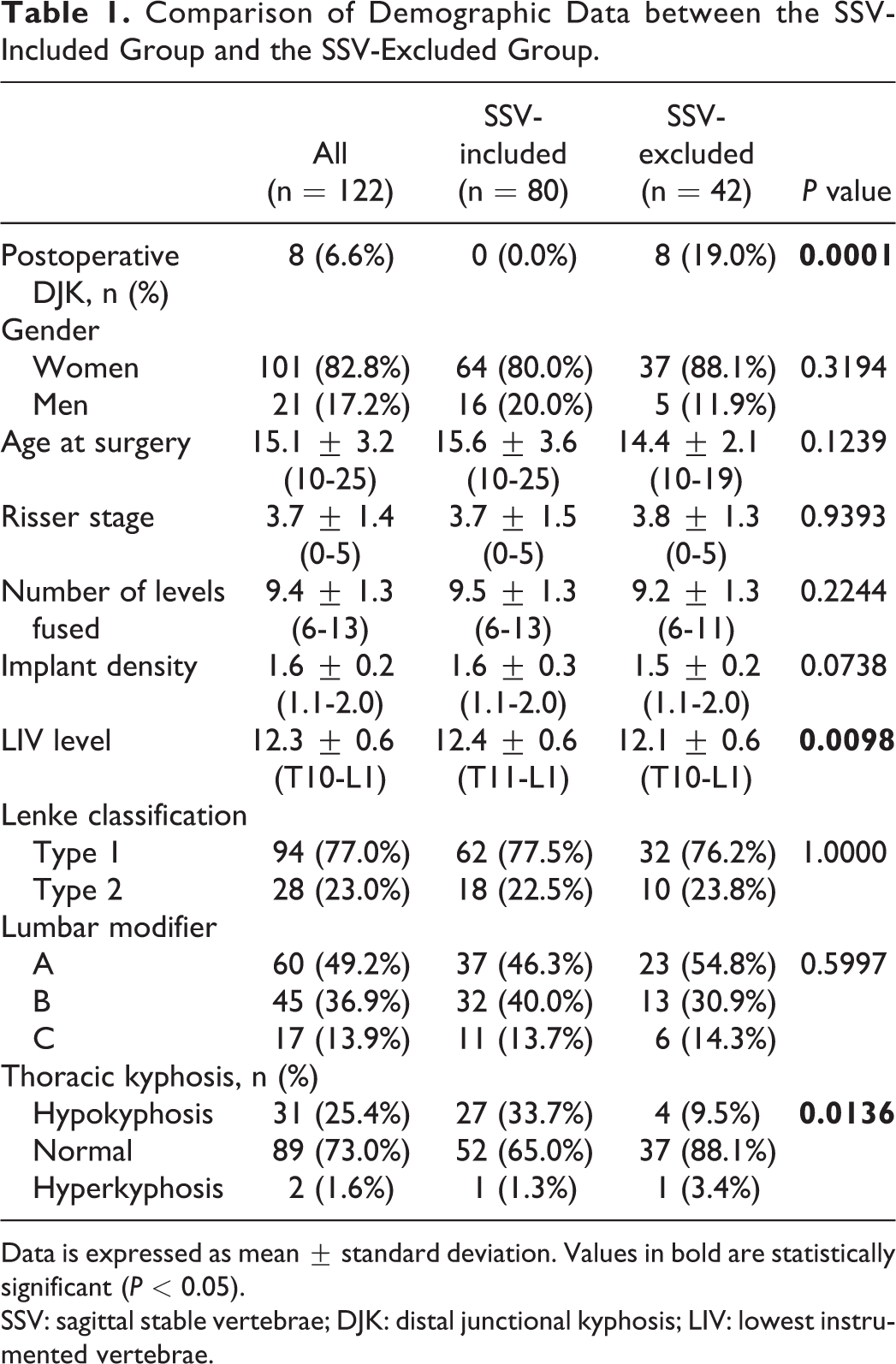
Data is expressed as mean ± standard deviation. Values in bold are statistically significant (P < 0.05).
SSV: sagittal stable vertebrae; DJK: distal junctional kyphosis; LIV: lowest instrumented vertebrae.
To investigate the risk factors, the patients in the SSV-excluded group were further allocated into the DJK and n-DJK groups according to the occurrence of postoperative DJK (Figure 3). Comparisons of demographic data, radiographic characteristics and measures between the 2 groups are shown in Table 2 and Table 3. There was no significant difference in demographic data and radiographic measures between the 2 groups, except for TK and TLK, which were larger in the DJK group before and immediately after PSF. However, only the immediate postoperative values of TK and TLK reached statistical significance between the 2 groups. The distribution according to the patients’ TK and TLK immediately after PSF is shown in Figure 4. ROC analysis showed that an immediate postoperative TK ≥ 25° (Figure 5, 95% confidence interval 0.669 – 0.920, P = 0.0018, area under curve 0.818) and TLK ≥ 10° (Figure 6, 95% confidence interval 0.605 – 0.879, P = 0.0376, area under curve 0.761) would best predict the occurrence of postoperative DJK in the SSV-excluded group. The occurrence rate of postoperative DJK was significantly higher in patients with immediate postoperative TK ≥ 25° (60.0%, 6/10) than in those with TK < 25° (6.3%, 2/32, P = 0.0009). The occurrence rate of postoperative DJK was significantly higher in patients with immediate postoperative TLK ≥ 10° (62.5%, 5/8) than in those with TLK < 10° (8.8%, 3/34, P = 0.0014). When the SSV was not included in the PSF, the incidence of postoperative DJK was significantly lower if both immediate postoperative TK was < 25° and TLK < 10° (1/29 = 3.4% vs 7/13 = 53.8%; P = 0.0004).
Demographics and Characteristics of n-DJK and DJK Subgroups In SSV-Excluded Group.
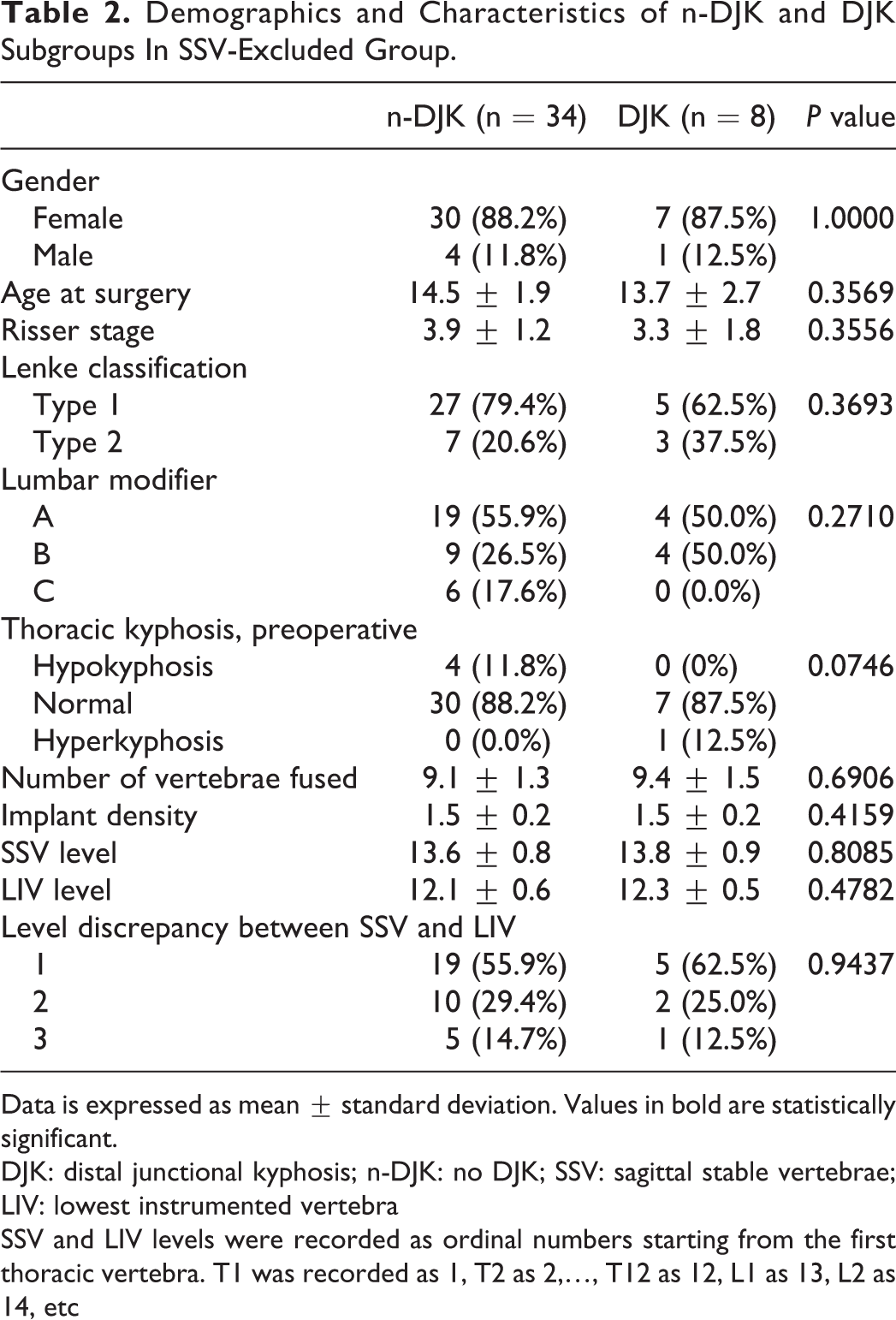
Data is expressed as mean ± standard deviation. Values in bold are statistically significant.
DJK: distal junctional kyphosis; n-DJK: no DJK; SSV: sagittal stable vertebrae; LIV: lowest instrumented vertebra
SSV and LIV levels were recorded as ordinal numbers starting from the first thoracic vertebra. T1 was recorded as 1, T2 as 2,…, T12 as 12, L1 as 13, L2 as 14, etc
Preoperative and Immediate Postoperative Radiographic Measures of n-DJK and DJK Subgroups in SSV-Excluded Group.
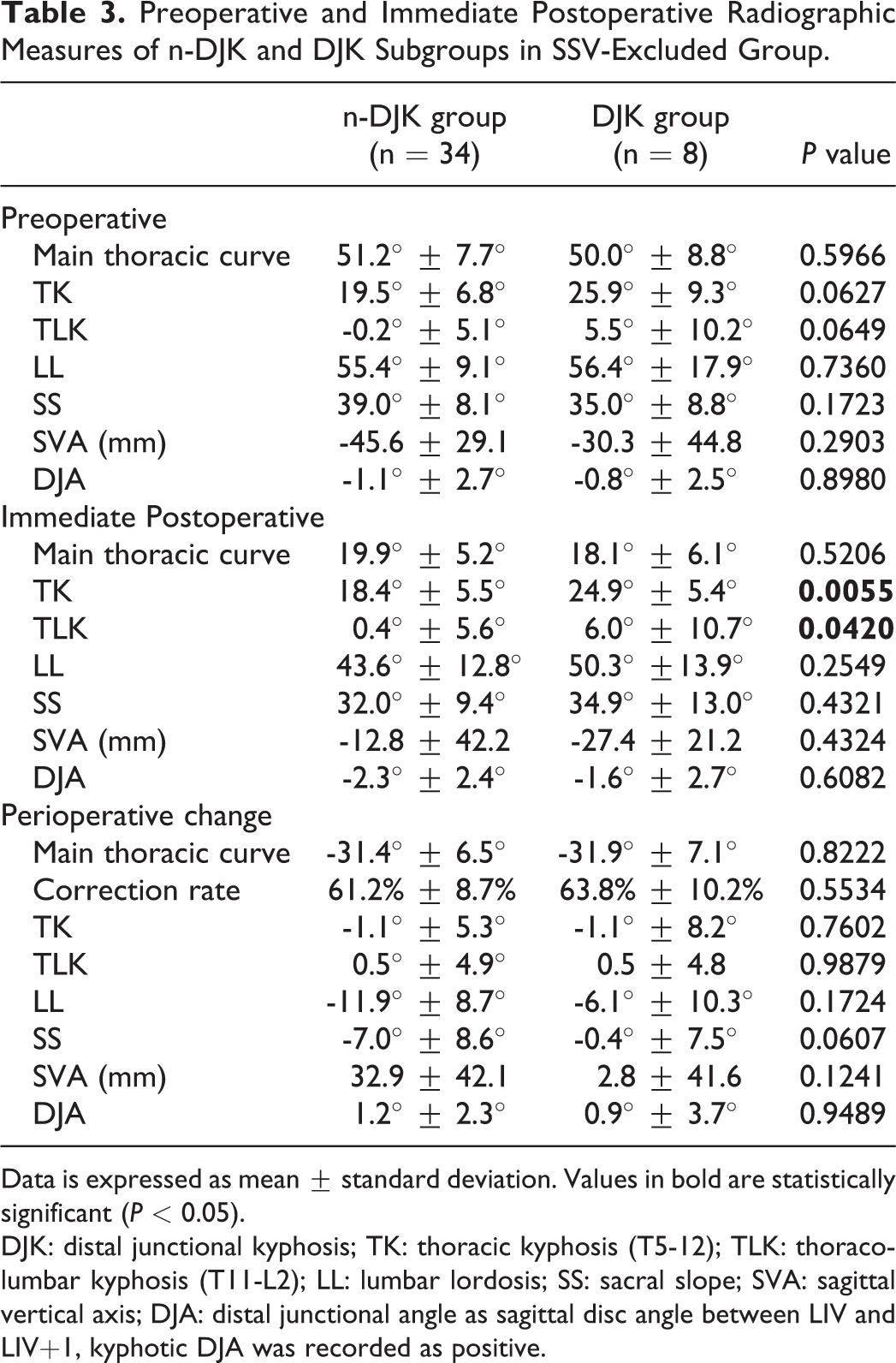
Data is expressed as mean ± standard deviation. Values in bold are statistically significant (P < 0.05).
DJK: distal junctional kyphosis; TK: thoracic kyphosis (T5-12); TLK: thoracolumbar kyphosis (T11-L2); LL: lumbar lordosis; SS: sacral slope; SVA: sagittal vertical axis; DJA: distal junctional angle as sagittal disc angle between LIV and LIV+1, kyphotic DJA was recorded as positive.
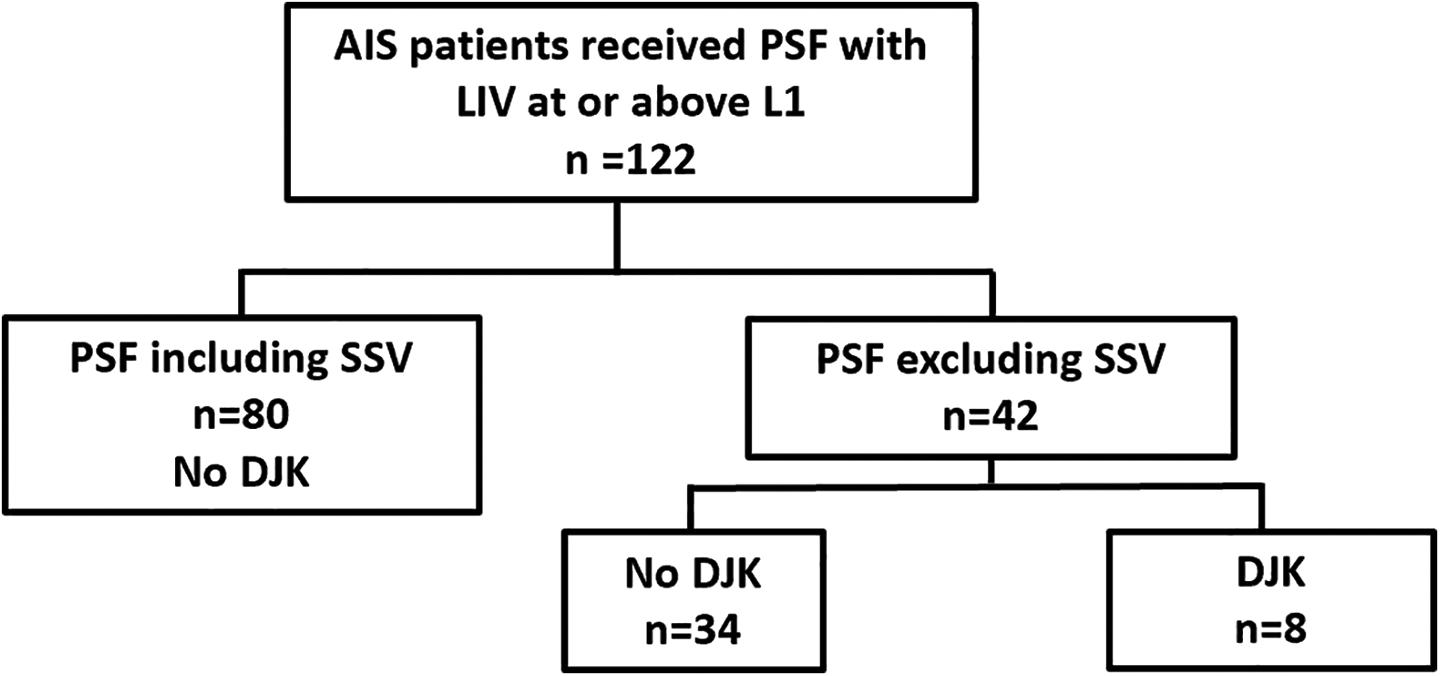
Flow chart of all patients receiving posterior spinal fusion (PSF) with lowest instrumented vertebrae (LIV) at or above L1 with inclusion or exclusion of sagittal stable vertebrae (SSV) and the occurrence of distal junctional kyphosis (DJK).
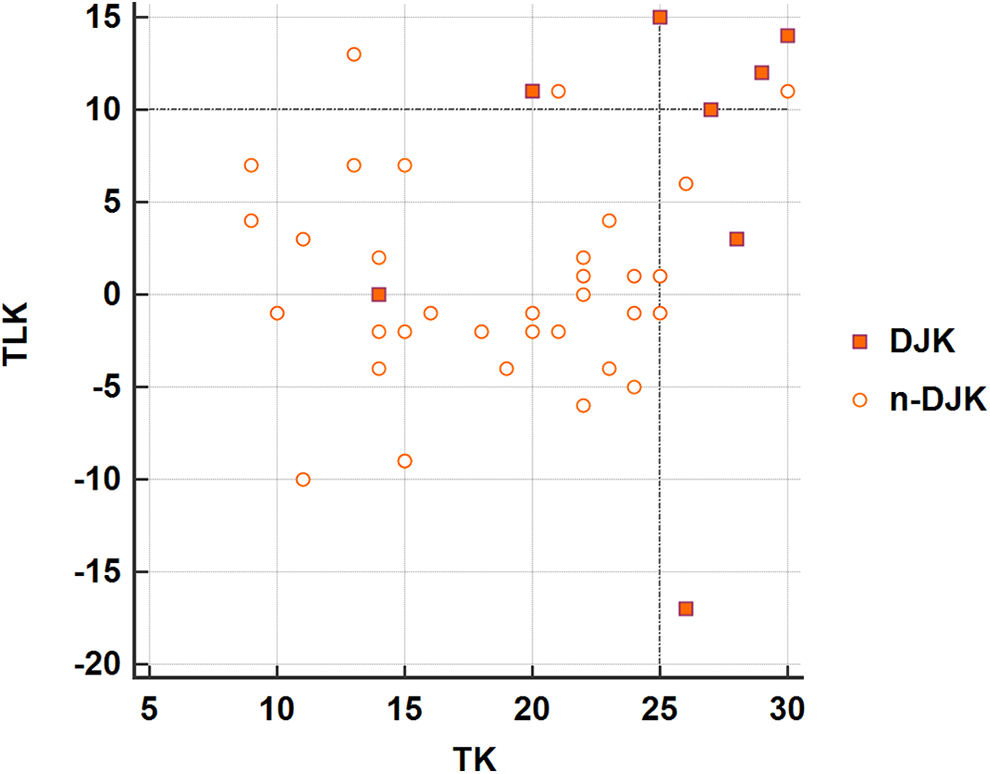
The distribution of postoperative thoracic kyphosis (TK) and postoperative thoracolumbar kyphosis (TLK) in each patient. The occurrence rate of postoperative DJK was significantly lower in patients with postoperative TK < 25° and TLK < 10° (1/29 = 3.4%) than in those with postoperative TK ≥ 25° or postoperative TLK ≥ 10° (7/13 = 53.8%).
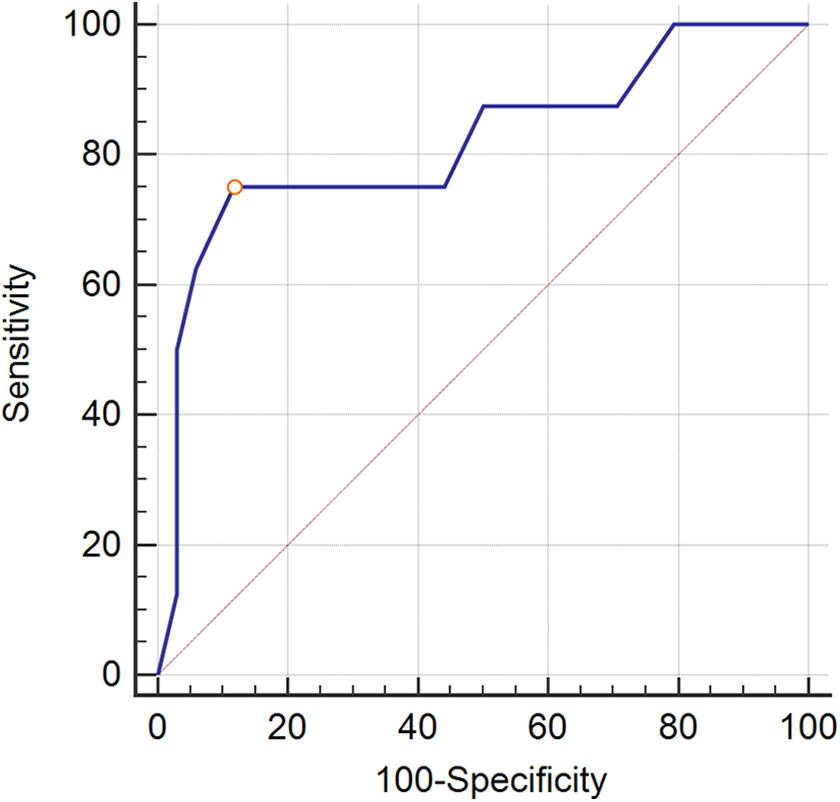
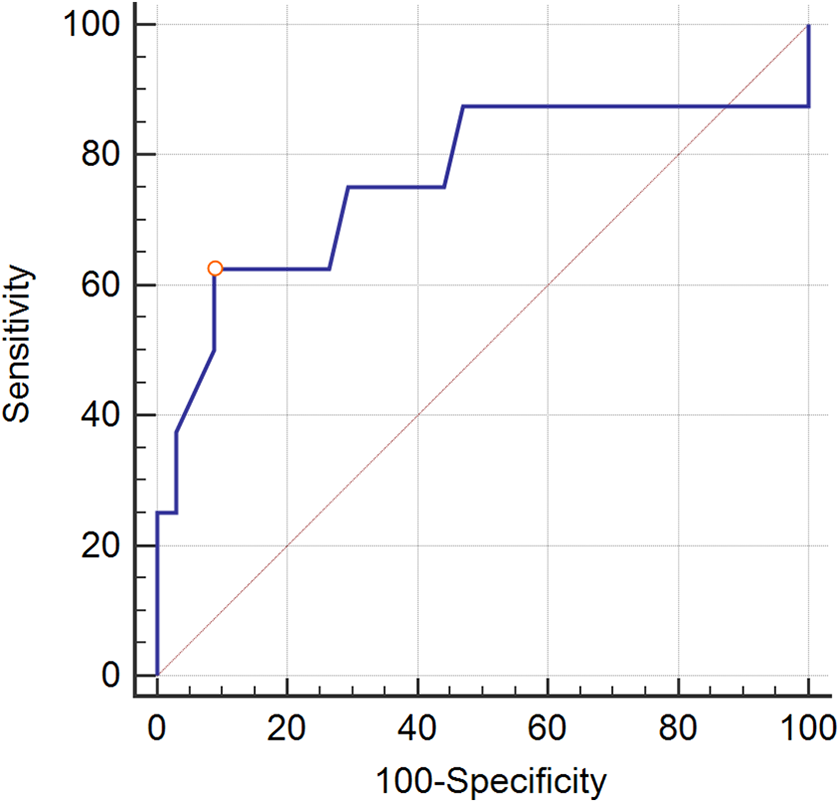
The receiver operating characteristic (ROC) curve of postoperative TK angle for predicting the distal junctional kyphosis (DJK). The area under the curve (AUC) was 0.818 (P = 0.0018). The cutoff value was 25°.
The receiver operating characteristic (ROC) curve of postoperative TLK angle for predicting the distal junctional kyphosis (DJK). The area under the curve (AUC) was 0.761 (P = 0.0376). The cutoff value was set at 10°.
Discussion
Although mild kyphosis at the thoracolumbar junction after PSF is usually well tolerated and compensated to maintain sagittal balance during young adulthood,9,18 the long-term radiographic effects and clinical impacts of DJK as AIS patients age and their compensatory capacity decreases are presently unclear and warrant further investigation. To prevent the occurrence and subsequent influences, the risk factors of postoperative DJK should be identified and well managed during surgery.
There have been many debates on selecting the LIV for PSF to achieve a balance between the benefit of preserving lower lumbar motion and the risk of imbalance below the LIV.4,7,8,19-23 Previously, determination of the LIV mainly focused on parameters on the coronal plane. The importance of radiographic parameters on the sagittal plane has received more attention in recent years. It has been proposed that inclusion of the SSV in the PSF for thoracic hyperkyphosis and Scheuermann’s disease may prevent postoperative DJK.12,16,24 Yang et al. applied the SSV concept to the prevention of postoperative DJK in AIS patients. In their study, no DJK (0/69) developed when the LIV was at or below the SSV, whereas the rate of DJK was 17.4% (8/46) when the SSV was not included in the STF. 13 In the current study, the occurrence rate of DJK was 19.0% (8/42) when the LIV was at or below the SSV and no patients (0/80) had DJK when SSV was included in PSF with LIV at or above L1. The occurrence rates of postoperative DJK were similar in both studies.
As both studies showed that the occurrence rate of postoperative DJK was less than 20% in the SSV-excluded group, there should be other factors contributing to this sagittal decompensation distal adjacent to the LIV. To our knowledge, no study has discussed the detailed risks of postoperative DJK when the SSV was not included in the PSF. In order to investigate other potential risks in the SSV-excluded group, a subgroup analysis was conducted and revealed that postoperative TK and postoperative TLK were more kyphotic in the DJK group. Preoperative TK and preoperative TLK were also more kyphotic in the DJK group but the differences were not statistically significant between the 2 groups. Furthermore, postoperative TK ≥ 25° and postoperative TLK ≥ 10° were found to be highly correlated to the occurrence of postoperative DJK in the SSV-excluded group.
Kyphosis ≥ 20° at the thoracolumbar junction has been considered as a structural curve and has been proposed to be included in the spinal fusion in order to prevent a postoperative distal decompensation. 17 Preoperative TLK < 10° has been proposed as a radiographic criterion for STF to treat Lenke types 1C and 2C AIS curves. 2 In the current study, no patient had preoperative TLK more than 20° and preoperative TLK ≥ 10° was not demonstrated as a risk factor for postoperative DJK when PSF did not include SSV. The postoperative DJK may occur even in lumbar modifier A or B if the TLK exceeded 10° on the occasion when the PSF did not include the SSV. According to the findings in the current study, TLK should be kept or reduced to a lesser extent if the PSF intends to exclude the SSV to save more motion segments. Otherwise, SSV should be included in the PSF to prevent postoperative DJK.
Patients with thoracic AIS are typically hypokyphotic at the thoracic spine compared to the same aged population without scoliosis.25,26 PSF for thoracic AIS would alter sagittal profiles of the spine with reestablishment of TK and reciprocal changes in unfused segments.25-28 It has been emphasized that preservation or restoration of TK is important to prevent resultant loss of LL and possible flatback syndrome subsequently.25,26 A critical value of thoracic kyphosis has even been proposed to prevent sagittal plane deterioration after STF for thoracic AIS. 29 However, the current study revealed a higher occurrence rate of postoperative DJK in patients whose PSF did not include the SSV, and the TK (T5-12) exceeded 25°. To save more motion segments with the exclusion of SSV from the PSF, the TK should be carefully tailored to produce a good sagittal alignment profile whilst preventing increased risks of postoperative DJK.
For Lenke 1 and 2 AIS, inclusion of SSV in the PSF could substantially prevent postoperative DJK in the current and previous studies. When the SSV-excluded fusion construct is considered, production of a sagittal profile with postoperative TK < 25° and TLK < 10° is important to reduce the risk of postoperative DJK. If TK ≥ 25° or TLK ≥ 10° was noted after PSF with LIV at or above L1, the development of postoperative DJK may be noted in about 50% of patients.
The results of the study should be interpreted with the following limitations. First, this study was limited by its retrospective nature and randomization of treatment was not allowed. Second, the multicenter design allowed us to recruit many more patients into the study; however, differences in operative technique and experience level among the surgeons may play a role in the results.
Conclusion
Although shorter fusion for AIS could preserve more motion segments, adequate levels should be contained in the spinal fusion procedure to prevent decompensation. The current study revealed that postoperative TK ≥ 25° or postoperative TLK ≥ 10° were factors of DJK occurrence if PSF did not include the SSV when LIV was at or above L1. When the SSV is intended to be excluded from the PSF to preserve more motion segments, TK and TLK should be carefully evaluated and attained in a lesser magnitude (TK < 25°, TLK < 10°) after surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.