
Abstract
Study Design
Systematic Review and Meta-analysis
Objectives
This systematic review and meta-analysis is aimed to assess effectiveness, safety, clinical, functional and radiological outcome of either combined anteroposterior or posterior-only approach in the surgical management of active tubercular disease of paediatric thoracolumbar spine.
Methods
A systematic literature search through PubMed, Scopus, Web of Science and Cochrane Library database was performed. Data extraction was undertaken following methodological quality assessment.
Results
9 out of the 182 publications identified, were included for analysis. A total of 247 patients were analysed. Two amongst the 9 studies were retrospective comparative studies evaluating posterior approach with combined anteroposterior approach and were considered for comparative meta-analysis. Blood loss and duration of surgery was significantly higher in the anteroposterior group, as compared to the posterior-only group. There was no significant difference between the 2 groups in terms of post-operative kyphosis angles, final kyphosis angles, number of complications, functional outcome and spinal fusion time. However, all the included studies were non-randomised and retrospective. Only 2 of them had a control group with a high heterogeneity amongst these 2 studies.
Conclusion
The inference from the studies included in this review suggests that equivalent results can be achieved with posterior-only approach for thoracolumbar tuberculosis in children as compared to anteroposterior approach, with much lower complexity, reduced blood loss and shorter surgical time. However, due to the high risk of bias and considerable heterogeneity among the studies included, we cannot conclude whether one approach is better than the other.
Keywords
Introduction
Spinal tuberculosis (TB) accounts for approximately half of the cases of osteo-articular TB. 1 The WHO global TB report of 2020 has estimated the incidence of TB for 2019 to be 10 million cases worldwide. Out of these, approximately 12% of the affected population is of children. 2 The prevalence of spinal TB is around 4.5% of all childhood TB. 3 The incidence of spinal tuberculosis is increasing due to the expanding use of immunosuppressants and biological therapies, the emergence of drug-resistant bacterial strains and immigration of people from disease prevalent zones. Anti-Tubercular drugs are effective in the management of uncomplicated spinal TB in children. However, it has been suggested that due to a tendency to undergo morphological changes, dorsolumbar (DL) region is more prone for progression of kyphotic deformity in children. 4 Furthermore, DL vertebrae itself are at risk for buckling collapse in children. Children afflicted with TB of the DL spine exhibit an increase in deformity not only during the active phase of the disease, but also during the quiescent phase until skeletal maturity. 5
Development of severe kyphosis is commoner complication in children with spinal TB than in adults. Severe kyphosis occurs approximately in 5% of patients with spinal TB. 6 Kyphosis is not only a cosmetic deformity but can also trigger psychological issues, cardiorespiratory problems and late onset paraplegia. 7 The progression of kyphosis following the healing of the tubercular lesion and the physiological growth in children can be difficult to manage. 8 Surgical management of spinal TB in paediatric population plays an important role in patients with spinal instability, neurological deficits, symptomatic abscess formation and spinal deformity. 9 It has been shown that the surgical intervention can assist in achieving spinal stability, facilitate neurological recovery and allow deformity correction. Currently, limited information is available to interpret the effects of surgical approach (anteroposterior vs posterior-only) on the safety, clinical, functional and radiological outcome including evaluation of complications, in paediatric patients with tuberculosis of DL spine. Till date, there is insufficient evidence to decide which is a better surgical approach to treat active tubercular disease of DL spine in paediatric age group.
This systematic review and meta-analysis compares the 2 widely used surgical approaches viz. combined anteroposterior and posterior-only approach in the management of paediatric thoracolumbar TB with respect to post-operative Cobb’s angle, Cobb’s angle at final follow-up, functional outcome, operative time, blood loss, fusion time and complications.
Materials and Methods
Protocol and Registration
The protocol for this systematic review was registered on PROSPERO on 4th June 2021 (registration number: CRD42021238888; title: Surgical Management of Paediatric Thoracolumbar Tuberculosis: A Systematic Review and Meta-analysis).
Eligibility Criteria
We included the all studies (both prospective and retrospective) evaluating patients under 18 years of age with active tuberculosis of the thoracolumbar spine with or without kyphosis. Only those studies which described at least 5 or more patients and who underwent surgery for thoracolumbar spinal tuberculosis by either combined anteroposterior or posterior-only approach with a minimum follow-up of 24 months of each patient were included.
Studies that comprised of patients with healed tuberculosis of spine with or without kyphosis, studies which included patients with active tuberculosis of cervical spine, review articles, letters to the editors and case reports were excluded. We also excluded all duplicated studies, studies with unreliable, missing or overlapping data, abstract-only papers and those without a full-text.
Information Sources, Literature Search and Study Identification
Search Strategy.
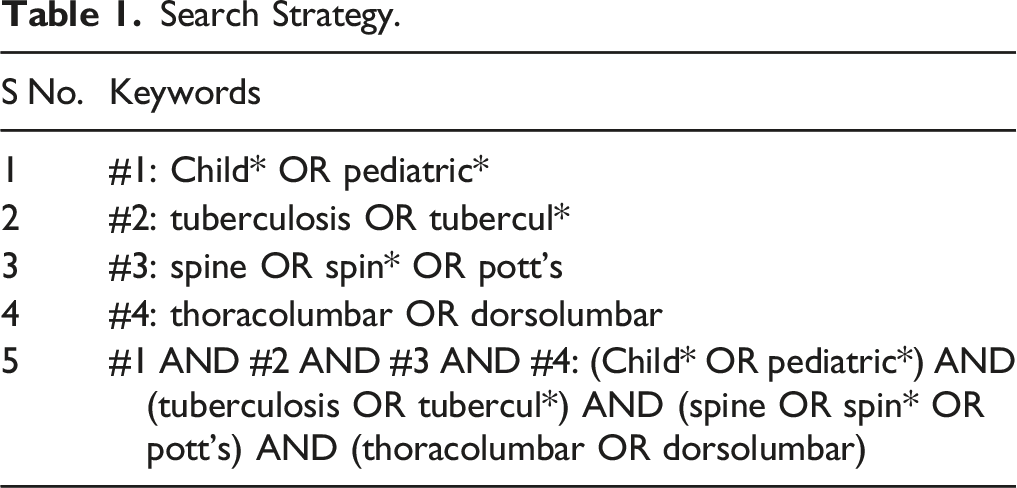
Data Extraction
Two authors (MKP and GU) individually performed the searches, screened the titles and/or abstracts, and assessed them. The full texts of potentially eligible studies were independently assessed. Any disagreement was resolved by mutual discussion and consultation with the senior author (VJ). The second round of screening was done by reviewing the full-text articles of the selected studies. Quality assessment of studies comparing posterior approach with anterior and posterior approach was performed using the Newcastle–Ottawa Scale. Data was then extracted from the studies selected for inclusion.
Statistical Analysis
A narrative synthesis of the findings from the included studies is presented. The descriptive data regarding patient characteristics available from all studies was summarized in tabulated form. Median (range) or Mean (Standard deviation) was used to summarize the data for continuous variables (as reported) and frequency/percentage was used for categorical variables. Age, sex, surgical duration, post-operative Cobb’s angle, Cobb’s angle at final follow-up, functional outcome, operative time, blood loss, spinal fusion time and complications were all recorded in surgically treated pediatric patients with tuberculosis of the thoracolumbar spine.
Heterogeneity between the studies in effect measures was assessed using the chi square and I2 statistics. We pooled the data using a random-effects meta-analysis (Der Simonian and Laird method) or a fixed effect meta-analysis, as appropriate (a fixed-effect model was used if I2 < 40% and a random-effects model was applied if I2 > 40%).10,11 Suitable forest plots were generated. Proportional meta-analysis was performed on data from case series, as appropriate. A two-sided P value< .05 was regarded as statistically significant.
Results
Literature Search and Screening
The PRISMA flowchart has been presented in Figure 1. The preliminary search yielded 66 articles on PubMed, 83 on Scopus (All Fields) and 33 on Web of Science. No extra papers were found in the Cochrane library (All Text). After screening duplicates and excluding unrelated articles based on the title, 24 papers were considered for assessment of full texts and finally 9 papers, published between year 2010 and 2019 were considered for this systematic review. There were 2 retrospective comparative studies comparing posterior approach with combined anteroposterior approach for paediatric thoracolumbar tuberculosis, therefore, they were considered for comparative meta-analysis. Rest of the 7 studies included in the review were case series, out of which 4 series were on posterior approach. PRISMA flow diagram.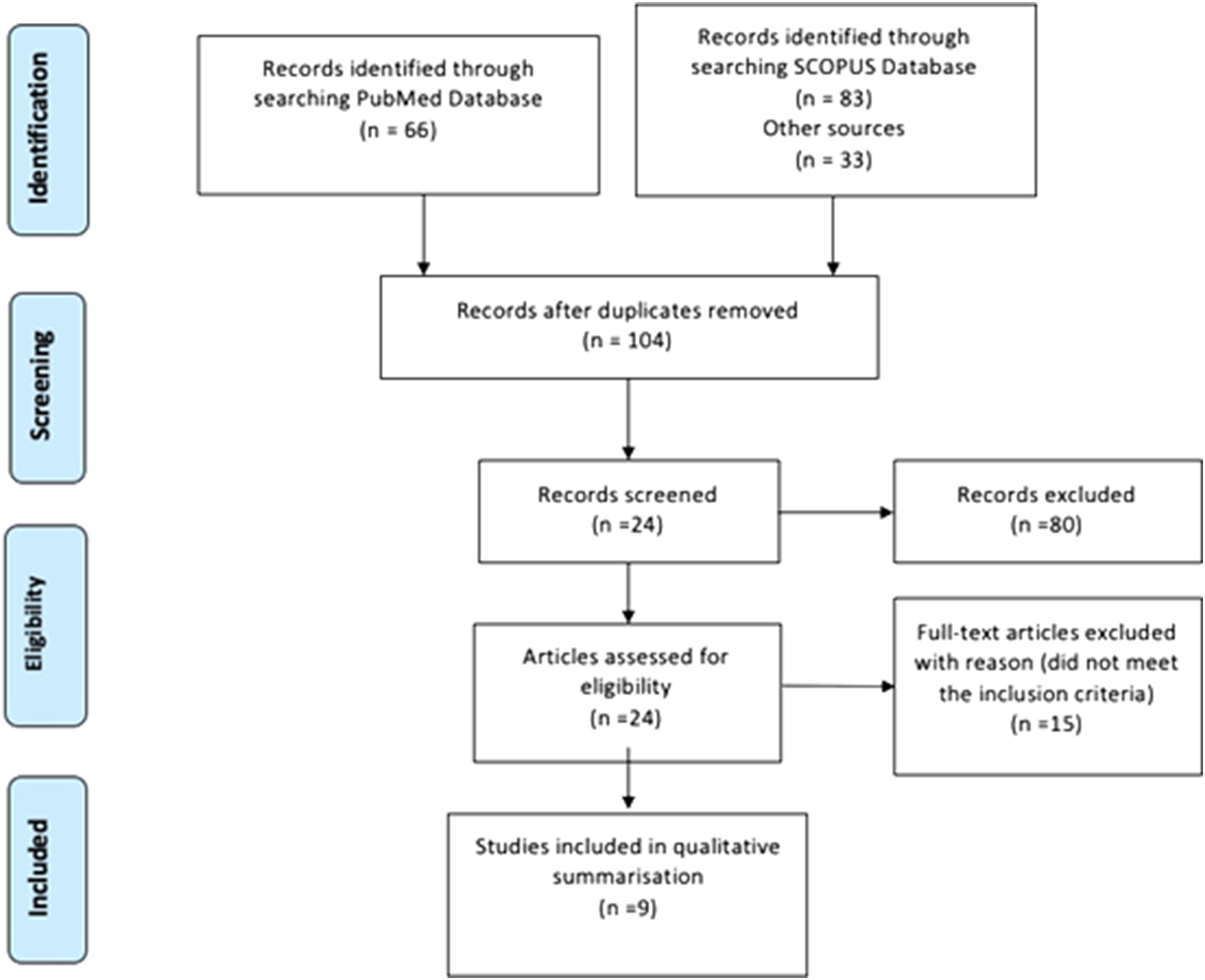
Characteristics of the Studies
Summary of Studies Included in the Systematic Review.
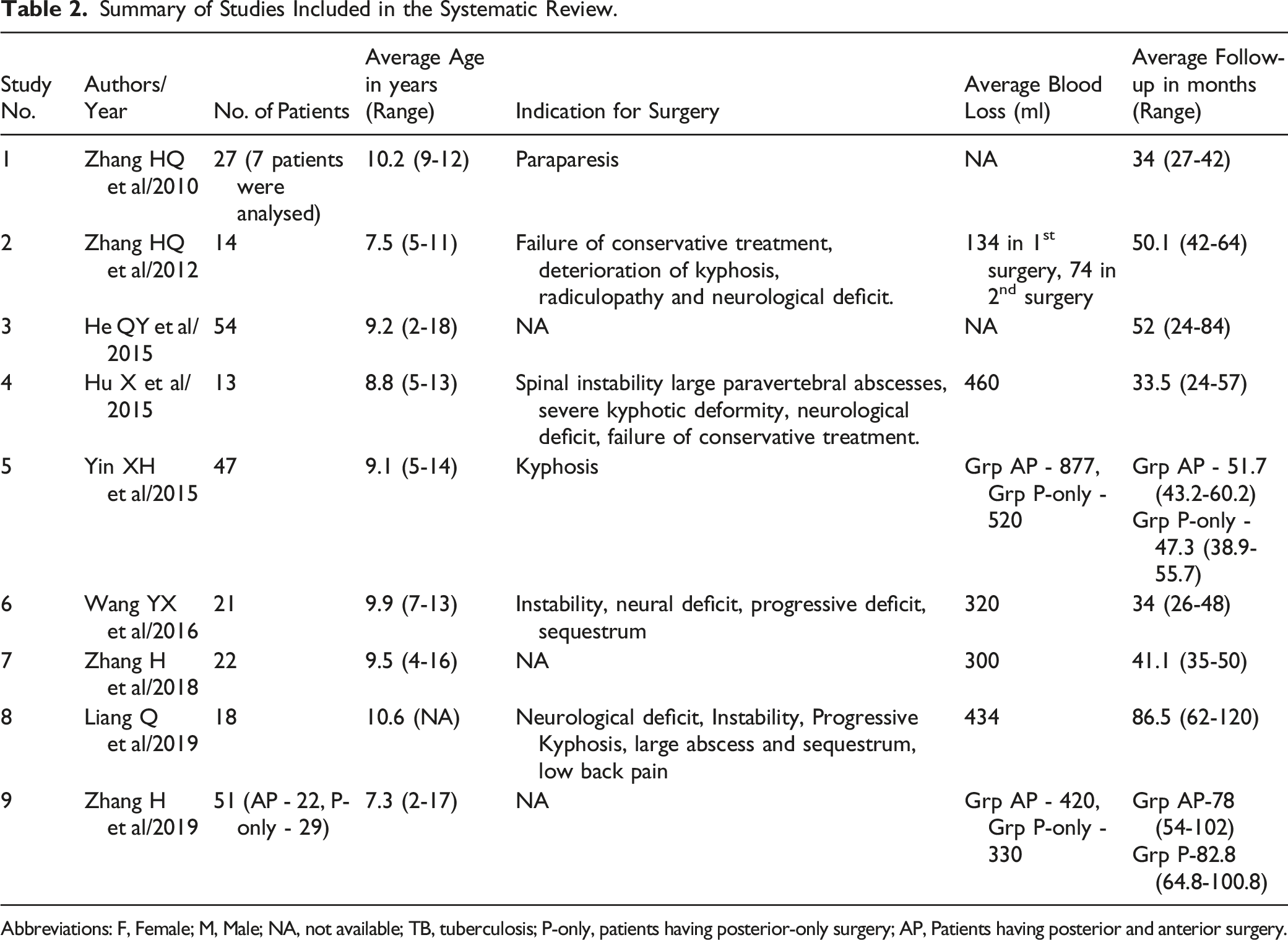
Abbreviations: F, Female; M, Male; NA, not available; TB, tuberculosis; P-only, patients having posterior-only surgery; AP, Patients having posterior and anterior surgery.
Summary of Published Studies Included in the Systematic Review form 2010 to 2019.
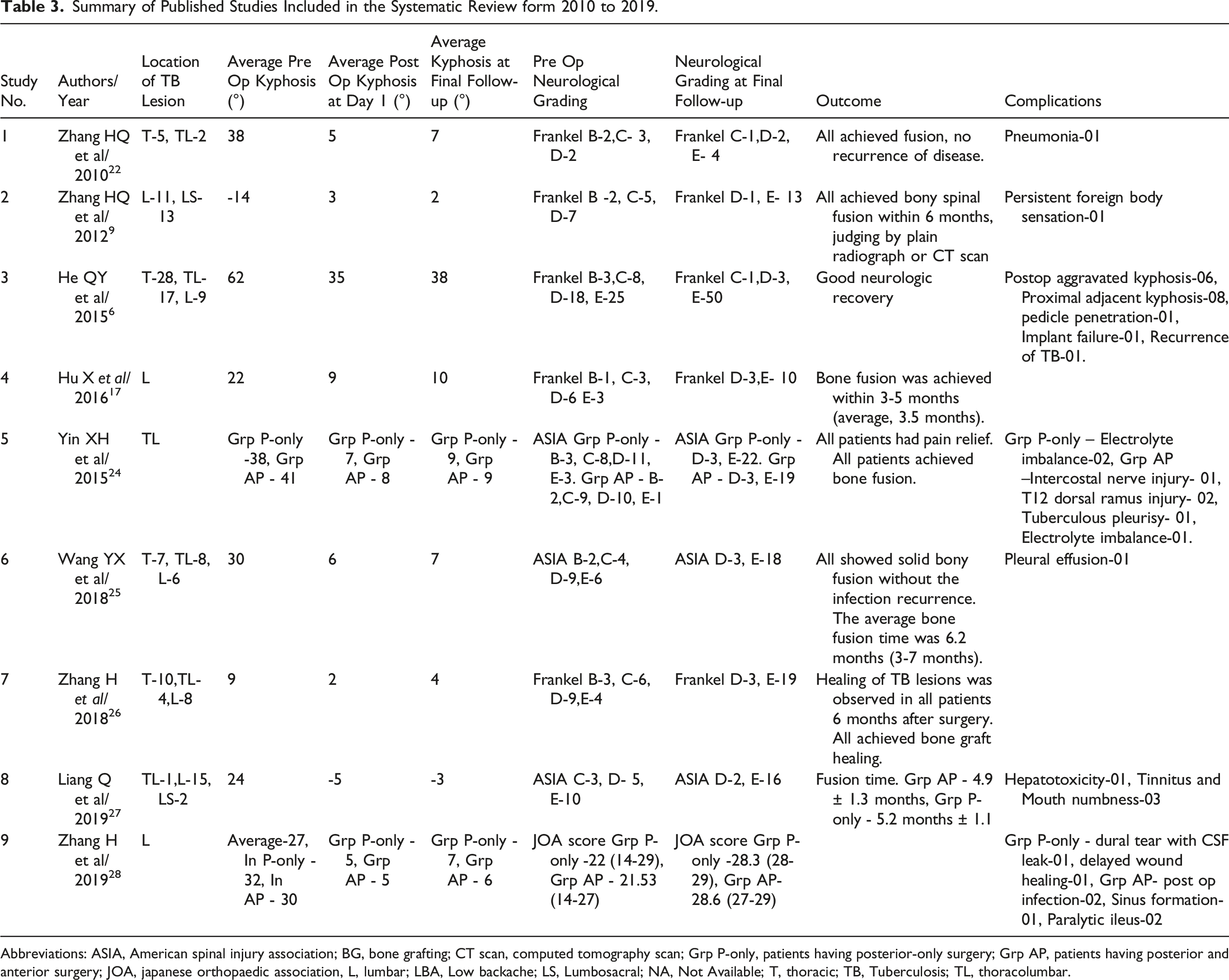
Abbreviations: ASIA, American spinal injury association; BG, bone grafting; CT scan, computed tomography scan; Grp P-only, patients having posterior-only surgery; Grp AP, patients having posterior and anterior surgery; JOA, japanese orthopaedic association, L, lumbar; LBA, Low backache; LS, Lumbosacral; NA, Not Available; T, thoracic; TB, Tuberculosis; TL, thoracolumbar.
Pooled Analysis
Pooled analysis was done from 4 studies reporting data on patients treated with anterior + posterior approach and 5 studies reporting data on posterior-only approach, as available in the published articles. a) Post-operative kyphosis
Average post-operative Kyphosis was 3.2° in anteroposterior approach with confidence interval (CI) [-1.3, 7.6]. Average post-operative kyphosis was 6.4° in posterior approach with CI [5.1, 7.7]. b) Kyphosis at final follow-up
Average kyphosis at final follow-up was 3.5° in anteroposterior approach with CI [ -1.7, 8.7]. Average kyphosis at final follow-up was 7.4° in posterior approach with CI [ 6.1, 8.7]. c) Complications
We found a total of 10 reported complications out of 86 cases undergoing anterior and posterior surgery. We observed a pooled rate of .101; 95% CI [.038, .164] and the heterogeneity for this was low (I2 = 0%). Amongst the cases undergoing the posterior-only surgery, we found a total of 7 reported complications out of 95 cases We observed a pooled rate of .066; 95% CI [.017, .115] and the heterogeneity for this was low (I2 = 0%).
Data for blood loss, operative time and time to achieve fusion could not be pooled because of heterogeneous and inadequate data.
Results of Meta-Analysis of the Two Primary Studies Comparing Anterior and Posterior Approach With Posterior Only Approach
a) Blood loss: Blood loss was significantly higher in the anterior + posterior group, as compared to posterior-only group (Mean difference 310.30 mL; 95% CI 279.21 mL, 341.40 mL; test of overall effect: z = 19.56, p <.001) However, there was a considerable heterogeneity among both the studies (I2 = 100%, p < .001), so random effects model was employed. b) Surgical duration: Operative time was significantly higher in the anterior + posterior group, as compared to posterior-only group in the metanalysis of 2 studies (Mean difference 110.69 minutes; 95% CI 91.63 minutes, 129.74 minutes; test of overall effect: z = 11.28, p <.001) However, there was a considerable heterogeneity among both the studies (I2 = 97%, p < .001), so random effects model was employed. c) Post-operative kyphosis angles: This was compared between the 2 groups on the post-operative radiographs in the 2 studies and did not show a significant difference (Mean difference .7°; 95% CI -.0°, 1.5°; test of overall effect: z = 1.90; p = .06, Chi square=.54, I2 was 0%, p= .46 so fixed effects model was used) d) Kyphosis angles at final follow-up: This was compared between the 2 groups on the follow-up radiographs in the 2 studies and showed a significant difference (Mean difference .7°; 95% CI .03°, 1.5°; test of overall effect: z = 2.04, p = .04; Chi square=.81 I2 was 0%, p= .37 so fixed effects model was used) f) Number of Complications: The rate of complications like infections, chest complications, deep vein thrombosis, dural tear and cerebrospinal fluid leak was compared between the 2 groups in the 2 studies and the number of complications was found to be higher in the anterior + posterior group (total 10 complications) vs posterior-only group (total 5 complications) with an Mantel Haenszel Odds ratio (MH-OR) of 2.90 (95% CI .91, 9.26; Z=1.80, p= .07, Chi square=.06, I2 = 0% so fixed effects model was used) but the difference did not achieve significance. g) Functional outcome(Oswestry Disability Index): ODI score at final follow-up did not show a significant difference, with MD - .05 months, 95% CI [-.32, 1.43](Z = .08, p = .94, Chi square=4.58, I2 = 78% so random effects model was used). h) Time to fusion: Fusion time did not show a significant difference (Mean difference .33; 95% CI -.22, .88; test of overall effect: z = 1.18; p = .24. However, there was a considerable heterogeneity (Chi square= 10.15%, I2 = 90%, p = .001), so random effects model was used.
Assessment of Risk of Bias
The overall risk of bias was assessed as low (the total score was 7 for the article by Yin XH et al and 8 for the article by Zhang H et al as per the Newcastle and Ottawa scale for the 2 retrospective comparative studies.24,28
Discussion
Location of Lesion/Segments Involved
This systematic review has included studies undertaken amongst paediatric TB spine patients with thoracolumbar and lumbar spine involvement only. Rajasekaran has claimed that location of the lesion is an important factor for severity of kyphosis at the time of clinical presentation. 7 Maximum kyphosis is found in patients with thoracic lesions during the active phase of disease. The author has postulated that this could be due to the additive effect of normal thoracic kyphosis. However, tendency of vertebral collapse decreases in the healed phase probably due to the support by rib cage. This is manifested by clinical improvement of the kyphosis angle during healed phase. On the other hand, a poorer prognosis is seen in lesions of thoracolumbar spine as evident by an increase in kyphosis angle during the active phase and subsequent smaller improvement during the healed phase. Kyphosis in children may even progress during healed phase due to longitudinal and appositional growth along with the differential development of anterior and posterior vertebral elements. 12
The risk factors for the development of severe kyphosis are-
He QY et al have stated that in patients less than 18 years old with spinal TB, there is a likelihood of involvement of more spinal segments. 6 This is attributed to the arrangement of vascular and lymph channels in the annulus fibrosus and the end plate cartilage. Loose-fitting attachment of the prevertebral fascia and periosteum to the vertebral body has also been highlighted as another possibility. 15 Out of the 4 studies in which the patients underwent surgery with posterior-only approach, there was statistically significant improvement of kyphosis at final follow-up, noticed in 3 studies, whilst no data was available in 1 study. Of the studies in which surgery was undertaken with an anteroposterior approach, only 1 study showed statistically significant improvement of kyphosis at final follow-up while 1 study did not comment on kyphosis.
Neurological Status
Studies in this systematic review have utilised either Frankel or ASIA grading system, or the JOA scoring system of assessing the neurological function. Pre-operatively, 11 patients had Frankel Grade B, 25 had grade C, 42 patients had grade D and 32 patients had grade E neurological function which improved following surgery. At final follow-up, 2 patients had grade C, 12 patients had grade D and 96 patients had grade E function. Similarly, patients whose function was classified as per ASIA grading system or the JOA score also improved after surgery. The improvement in neurological function was seen in patients with anteroposterior as well as posterior-only surgical approach.
Surgical Method/Approach
In majority of the cases of TB spine, the involvement is paradiscal; so, the anterior debridement has obvious advantages. Anterior debridement without fusion has been assessed by Medical Research Council (MRC). These studies were performed at Hong Kong and Bulawayo institutions. 16 Nonetheless, the results of these studies have not shown any long-term benefit of anterior debridement + chemotherapy as compared to chemotherapy alone. Anterior approach offers better exposure, complete debridement and ability to achieve anterior fusion. However, anterior approach in lower lumbar spine does have an increased risk of neurovascular injury. Anterior fusion technique, alone also has reported to have the risk of increased kyphosis angle in the follow-up period, particularly if there is involvement of multiple segments. 17
Combining both anterior and posterior debridement with fusion in single or 2 stages may offer the advantage of decreasing the incidence of kyphosis in follow-up period. Disadvantages of combined approach either in single or 2 stage includes increased cost, longer stay and more incidence of post-operative complications. 17 However, it is possible to achieve most of these objectives with a posterior-only approach, with relatively lower complexity and morbidity (as anterior disease can also be addressed using costo-transversectomy, trans facet approach, transpedicular approach or lateral extracavitatory approach) on case-to-case basis. Consequently, these approaches are now becoming popular to address anterior disease from the back. It is possible to insert bone graft/cage anteriorly by a posterior approach. Posterior approach is also easier to learn with a flatter learning curve. It may obviate the need of a cardio-thoracic or general surgeon as most orthopaedic or spine surgeons are conversant with the same. In the past, posterior approach was advocated mostly for cases with posterior spinal disease and spinal tumour syndrome. With changing times, posterior approach has now become an appropriate choice to address most cases of paediatric thoracolumbar spinal tuberculosis.
Studies have shown that use of implants in Spinal TB surgery is safe. Oga M et al evaluated the adherence properties of Mycobacterium tuberculosis (M tuberculosis) to stainless steel and found out that M tuberculosis is less adhesive and produces less biofilm than pyogenic bacteria. They concluded that instrumentation surgery is safe in spinal TB when combined with debridement and Anti-Tubercular Therapy (ATT). 18 Benli I et al reported that Titanium anterior implants are similarly safe to apply in Pott’s spine. 19 Huang QS et al (2009) aimed to verify the importance of early reconstruction of spinal instability. They performed anterior decompression with autologous bone grafting and posterior instrumentation. They reported that anterior approach was required for good visualisation of the diseased spinal cord. Early mobilisation and prevention of kyphosis was attributed to posterior instrumentation. 20
ATT is effective but may not be able to prevent paraplegia and kyphosis on its own. Erturer E et al concluded that the 360° spinal fusion method is beneficial in patients with the involvement of 2 or more vertebral levels and accompanied by moderate or severe kyphosis. 360° spinal fusion method achieves complete kyphosis correction, allows efficient stabilization, early mobilization and is effective in maintenance of the accomplished correction. Titanium mesh cage filled with spongious chip allograft was used at anterior corpectomy site. The authors found out that use of titanium mesh had no negative effects on infection and also it provided anterior support with respect to mechanical stability. 21
Zhang HQ (2010) et al performed single-stage posterior transpedicular screw fixation and anterior debridement with fusion especially in children with active Pott’s disease and poor health. They have demonstrated it to be a safe and effective method in achieving spinal decompression with immediate and sufficient stabilization of kyphosis correction in such patients. The authors have also highlighted the advantage of posterior instrumentation in achieving sufficient kyphosis correction, avoiding exposure of tuberculosis foci posteriorly, ability to provide three-column spinal fusion to prevent imbalanced spinal growth of children and long-term maintenance of correction. Thus it appears the application of posterior instrumentation in children aged less than 5 years is safe and achievable. The authors have recommended delayed removal of implants to accomplish developmental, physical milestones. The study also concludes that duration of anaesthesia and surgical time were not associated with increased morbidity. 22
Zhang HQ (2012) et al performed 2 stage surgery for spinal TB. In first stage, they performed posterior pedicle instrumentation with distraction of the anterior column. After an average gap of 2 weeks, second stage surgery was undertaken which included anterior column debridement and use of allografts. The authors have advocated that posterior instrumentation done in first stage has the advantage of restoring spinal alignment, maintains vertebral height, allows indirect decompression of spinal cord and provides anterior space for the application of allograft in second stage surgery. Anterior bone grafting has the added advantage of prevention of progression of kyphosis. 23 A mild kyphosis can be effectively corrected by anterior approach alone. However, for a kyphosis angle of more than 30° with or without multiple-level involvement, a combined anterior and posterior approach is probably more effective
Yin XH et al compared the posterior-only approach with anterior–posterior approach in DL spine TB in children. They have concluded blood loss, surgical time and hospital stay was reduced perceptibly in patients who underwent posterior-only surgical approach. 24 Wang YX et al performed single-stage debridement, interbody grafting, posterior instrumentation and posterior fusion of DL spine TB and achieved good results. 25 Zhang H et al (2018) performed focus debridement, posterior instrumentation and anterior fusion using titanium mesh cages filled with combined autograft and allograft during the posterior-only approach in 22 children. Authors have claimed solid fusion in all patients with significant clinical improvement in kyphosis correction and neurological status. 26 Liang Q et al used combined anterior and posterior approach in lumbar TB and performed posterior instrumentation, posterolateral grafting, anterior debridement and strut grafting in 18 children and claimed it to be safe and effective method. 27 Zhang H et al compared posterior with postero-anterior approach in 51 children with lumbar TB and concluded that in experienced hands, posterior-only approach provides a satisfactory outcome. 28
Bone Grafting
Both autograft and allograft have been used in the assessed studies. Application of either graft materials have their own merits and demerits. As autografts, ribs are readily available from local site (they may be removed as a part of approach) and have been shown to be a better source of BMPs (Bone morphogenic protein) compared to iliac crest and fibula. 29 Autografts also have the advantage of immunocompatibility with no risk of disease transfer providing higher chances of bone fusion. However, disadvantages of autograft include donor site morbidity, blood loss, limited availability in children and questionable structural support.30-32 Apart from this, there is also risk of graft fracture, slippage or absorption. Allografts on the other hand, may not be easily available and has the potential for disease transmission along with a slower rate of achieving fusion. Nevertheless, use of freeze-dried allograft reduces this risk of disease transmission. 33
This review, however, is not without limitations. First, there is a void in the literature with regard to good quality comparative studies comparing the posterior + anterior approach with posterior-only approach (no randomised controlled trials or prospective cohort studies). Among the 9 studies included, all were retrospective, none of them were randomized and only 2 of them had a control group. Furthermore, there was high heterogeneity among the 2 studies included in the meta-analysis. Therefore, the results drawn from these studies alone or when aggregated in a meta-analysis; are at high risk of bias.
Conclusion
The evidence from the studies included in this meta-analysis (although with the limitation of high heterogeneity among the studies) suggests that equivalent results can be achieved with posterior-only approach for thoracolumbar tuberculosis in children as compared to anteroposterior approach, with much lower complexity, lesser blood loss and shorter surgical time. However, due to the high risk of bias and considerable heterogeneity among the studies included in this meta-analysis (which includes only retrospective studies with small numbers and non-randomized allocation), we cannot conclude whether one approach is better than the other. Larger high-quality randomised controlled prospective studies are needed in the future to further confirm these findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.