
Abstract
Study Design:
Systematic review.
Objectives:
(1) What are the surgical indications? Have they changed over time since the year 2000? (2) What is the current surgical approaches of choice? Have they changed over time since the year 2000? Do they vary by geographical region? (3) What are the most common outcome measures following surgery?
Methods:
Electronic databases and reference lists of key articles were searched from database inception from January 1, 2000 to December 31, 2016 to identify studies specifically evaluating surgical indications, current surgical approaches, and outcome measures for spinal tuberculosis.
Results:
Six randomized controlled trials were identified from our search (1 excluded: no surgical arm identified after review) Neurological deficit, instability and deformity were common indications identified. Surgical approach included predominantly anterior for cervical spine and posterior for thoracic and lumbar spine. Combined approach was preferred in pediatric cases. Degree of deformity correction, neurological outcomes, and fusion formed the main bases of assessing surgical outcomes.
Conclusions:
Majority of the current literature is from South Asia. The presence of neurological compromise, deformity, and instability were the primary criteria for surgical intervention. The preferred approach varied with the anatomical region of the spine in adults. Outcome measures predominantly involved deformity correction, neurological deficit, and fusion.
Introduction
Tuberculosis (TB) affecting the human bones and joints has a long historical background. 1 –3 It is estimated that 2 million people suffer from spinal TB. 4 In endemic areas, it is the most common form of infective spondylodiscitis. The presentation of the disease is variable and bears a strong influence based on the pathogen, stage of the disease, drug sensitivity, and geographical region. With the rise of multidrug resistance TB, the pattern of presentation and treatment has changed to become even more complex. Early identification of the pathogen (biopsy) and initiation of chemotherapeutic medicines prevent many of the severe deformities; surgical intervention is still widely considered and practiced. While the surgical indications broadly include progressive neurological deficit, progressive deformity, instability, pain, and uncertain diagnosis, there is dearth of literature and consensus on the surgical indications, type of surgery, and the outcome. 5 There are also regional differences and individual surgeon preferences as far as surgical strategy is concerned that may influence the outcome and disease morbidity. The aims of this study are to evaluate the current trends of surgical intervention in Pott’s disease treatment, identify regional differences in the surgical management, and identify indication for surgical treatment of the disease.
Key Questions
Among patients with spinal TB,
What are the surgical indications? Have they changed over time since the year 2000? What is the current surgical approaches of choice? Have they changed over time since the year 2000? Do they vary by geographical region? What are the most common outcome measures following surgery?
Materials and Methods
Study Design
Overview and bibliometric study.
Information Sources and Search
PubMed, from January 1, 2000 to December 31, 2016. Search strategy can be found in the supplemental material.
Rationale and Eligibility Criteria
Key Question 1. We sought indications for surgery by examining the inclusion and exclusion criteria for all randomized controlled trials (RCTs) of surgery for spinal TB since the year 2000. We judged that enrollment criteria for a surgical trial would represent the current thought on indications for surgery. Key Question 2. We searched for all publications reporting primary data on patients receiving surgery for spinal TB since the year 2000. Key Question 3. All systematic reviews with a meta-analysis were obtained that evaluated surgery for spinal TB since the year 2000, and the outcomes measures were recorded.
Data Extraction
Data was extracted independently by 2 investigators (CF, JRD) and compared. Discrepancies were resolved by consensus. The following data items were recorded:
For Key Question 1—Study citation, country where study was conducted (or country of primary author), spine segment treated, the intervention and control procedure, inclusion and exclusion criteria. For Key Question 2—year of study, surgery type (anterior, posterior, combined), country where study was conducted (or country of primary author), age (adult or children). For this key question, data from the study abstract were reviewed and the full text was only consulted when information from the abstract was inadequate or unclear. For Key Question 3—study citation, outcomes assessed, and spine segment treated.
Analysis and synthesis of results was performed by qualitative synthesis and descriptive statistics.
Results
Study Selection and Characteristics
Key Question 1. Six randomized controlled trials were identified from our search. We excluded 1 after full-text review for lack of a surgical arm, and we retained 5.
6
–10
Key Question 2. We identified 503 studies from our search strategy and retained 287 meeting our prestated criteria; 266 in adults and 21 in children. Key Question 3. Sixteen systematic reviews were identified; 5 reported a meta-analysis and were retained.
11
–15
Results of the publication selection are illustrated in Figure 1. Citations of all studies included and those excluded at full text can be found in the supplemental material.
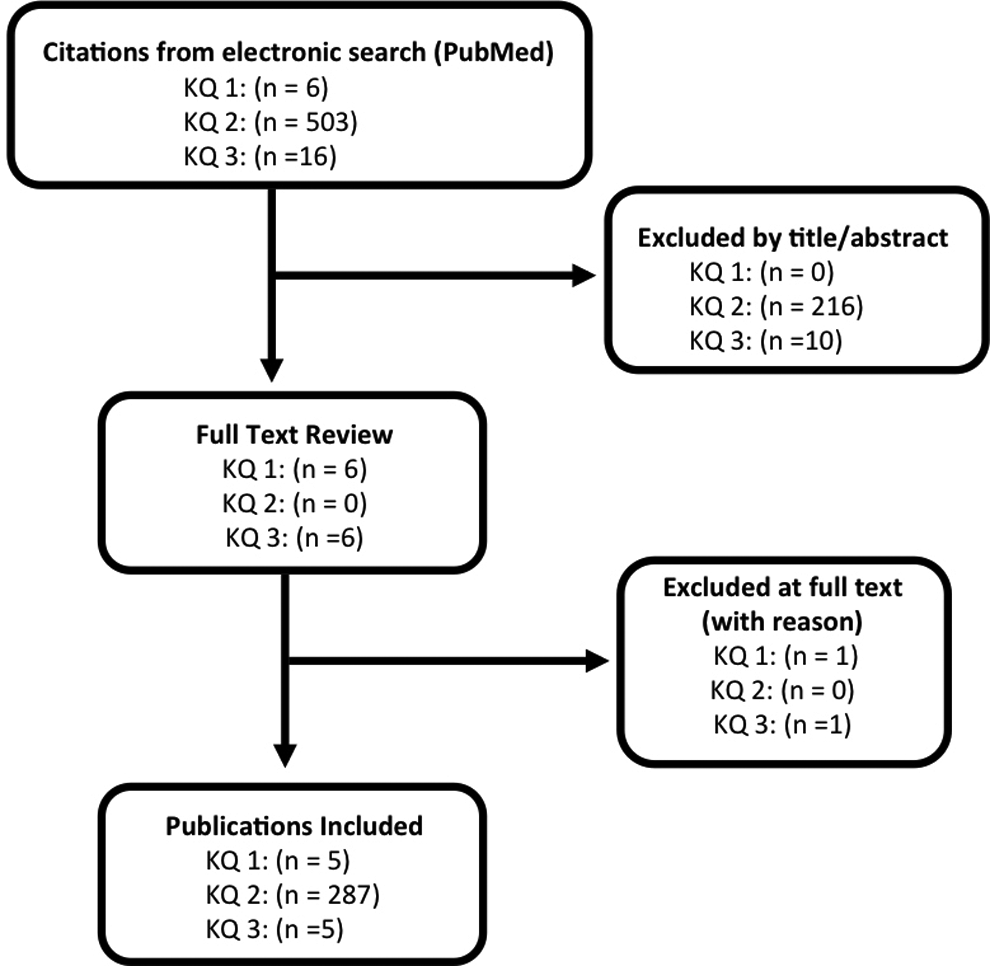
Flow diagram showing results of literature search and study selection. KQ, key question.
Key Question 1. What are the surgical indications? Have they changed over time since the year 2000? Surgical indications for spinal TB as described in RCTs are poorly delineated and inconsistent (Table 1).
Cervical spinal TB. The inclusion criteria for entering the only cervical RCT included cervical myeloradiculopathy, persistent neck pain, difficulty swallowing, and upper extremity weakness.
9
Upper thoracic spinal TB. From a single RCT, ineffective control with anti-TB drugs AND one of the following: larger sequestrum formation, or sinus formation, or larger abscess, or vertebral collapse, or progressive kyphosis, or neurologic deficit.
7
Thoracic, lumbar spinal TB. One RCT required all of the following: Frankel grading D and E, severe back pain, larger sequestrum formation and significant spinal instability.
8
Lumbar spinal TB. One RCT required only a lumbar compression fracture to be eligible for surgery.
10
Lumbosacral spinal TB. One or more of the following were required for surgery in a single RCT of lumbosacral TB: Spinal cord or nerve root compression causing dysfunction, spinal instability or kyphosis, large abscess, bony cavity, dead bone, sinus tract, resistance to drug therapy.
6
There is a lack of evidence to determine whether indications for spinal TB surgery have changed since 2000.
Inclusion and Exclusion Criteria in Randomized Controlled Trials of Surgical Intervention for Spinal Tuberculosis.
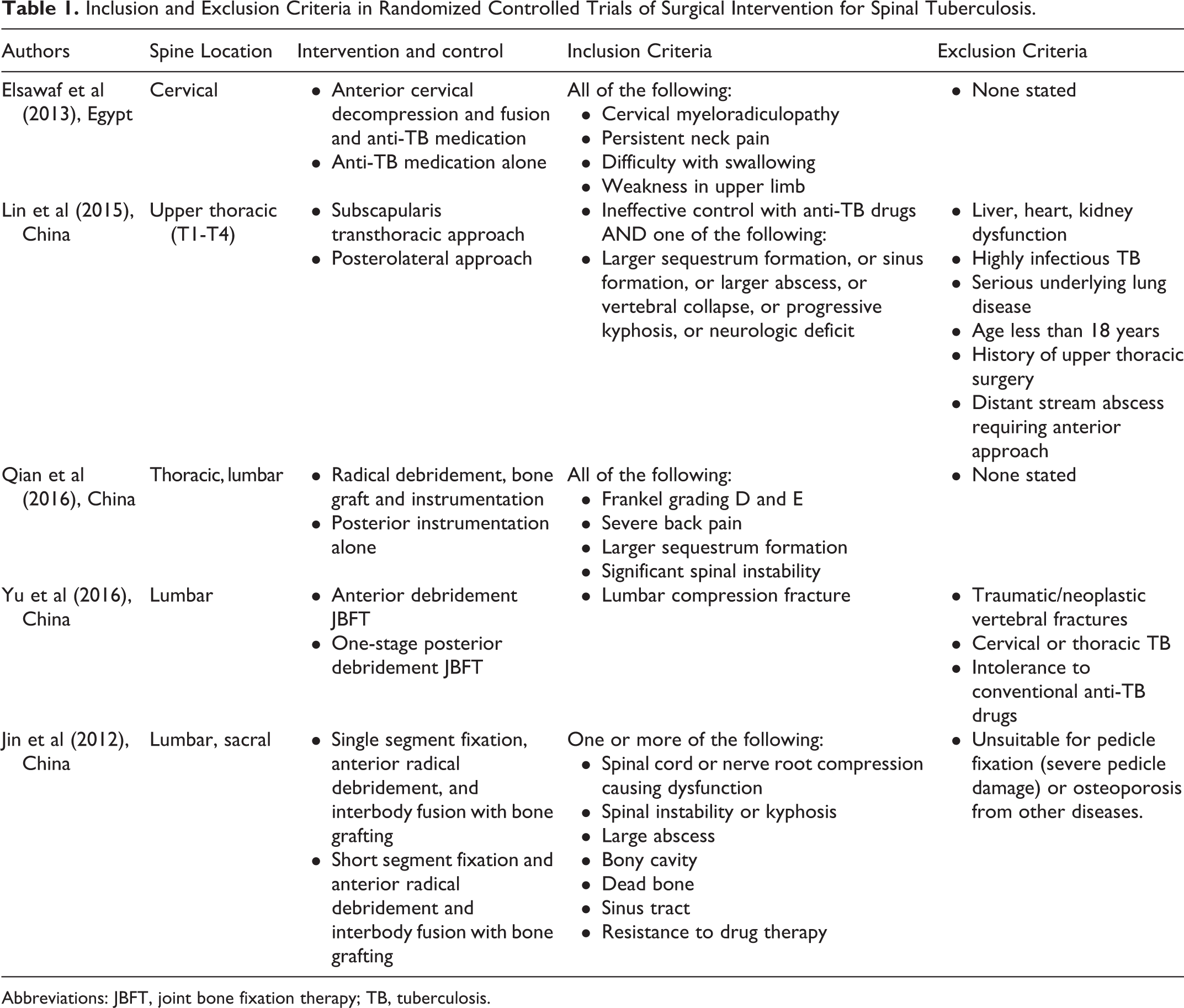
Abbreviations: JBFT, joint bone fixation therapy; TB, tuberculosis.
Key Question 2. What is the current surgical approaches of choice? Have they changed over time since the year 2000? Do they vary by geographical region? Published studies from 2000 to 2016 report anterior and posterior approaches in similar frequency, with half as many studies reporting a combined approach (Figure 2). Twenty-three percent of studies describe some patients receiving one approach and others receiving a different approach. Among surgical studies of adults with spinal TB, publications reporting on patients receiving the posterior approach have risen from the least reported approach in the early 2000s to the most frequently reported approach in the past 4 years (Figure 3). Among surgical studies of children with spinal TB, the anterior and combined approaches remain the most frequently published (Figure 4). The majority of surgical studies in spinal TB arise from China, followed by India, Turkey, and Korea (Figure 5).
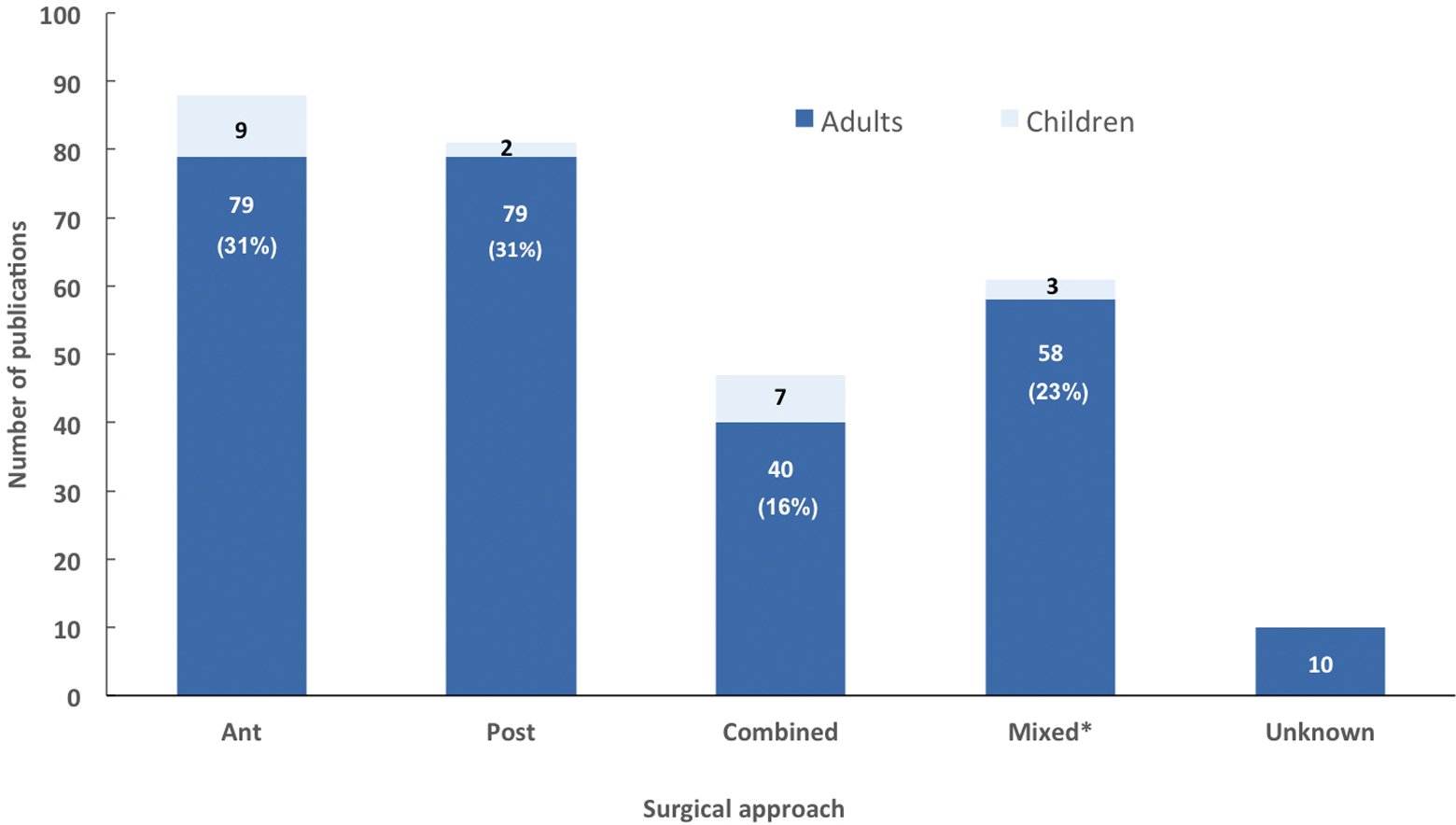
The number of publications of surgery in spinal tuberculosis, stratified by surgical approach, 2000-2016.
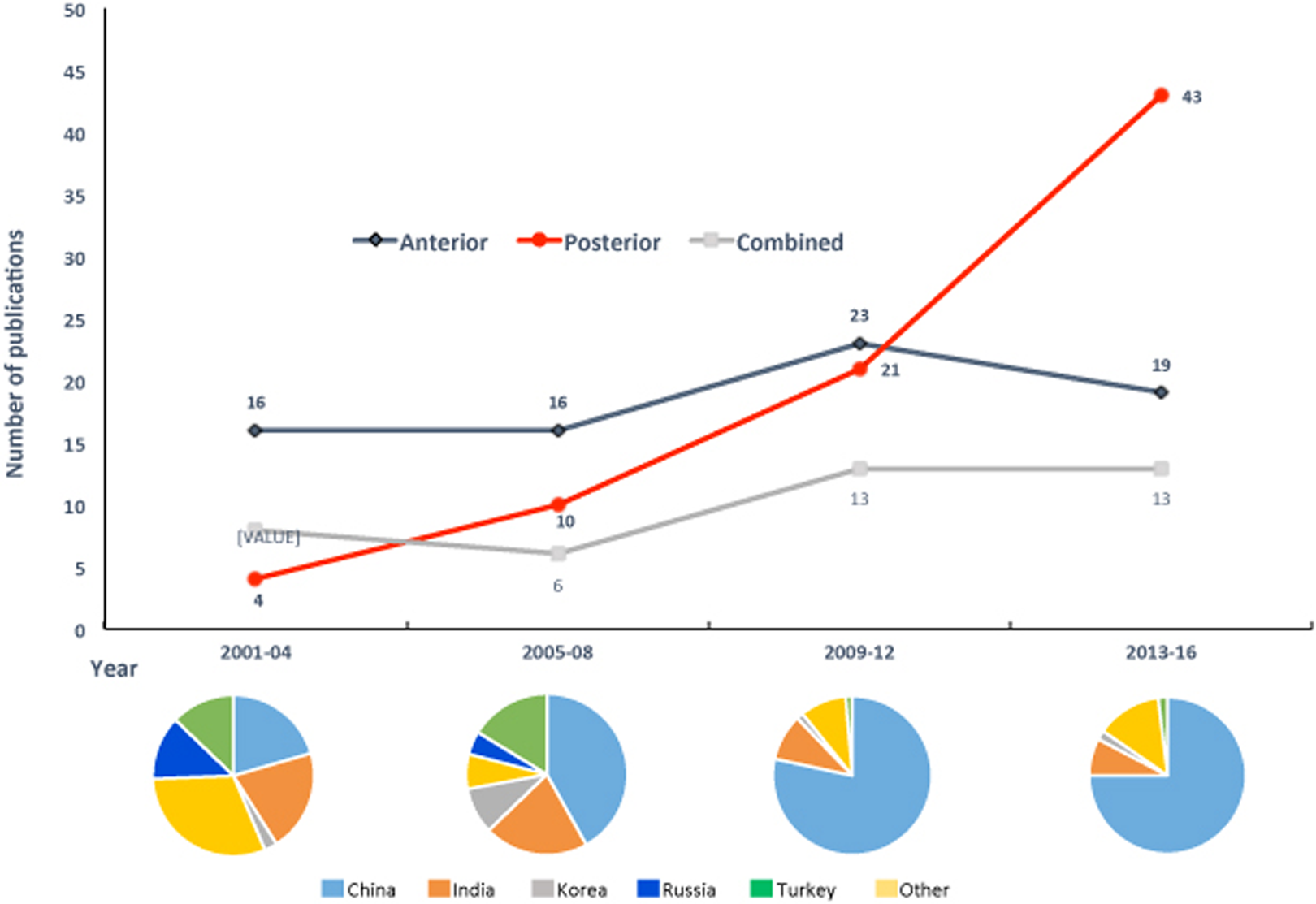
The change in the number of publications of surgery in adult spinal tuberculosis, stratified by surgical approach, 2001-2016.
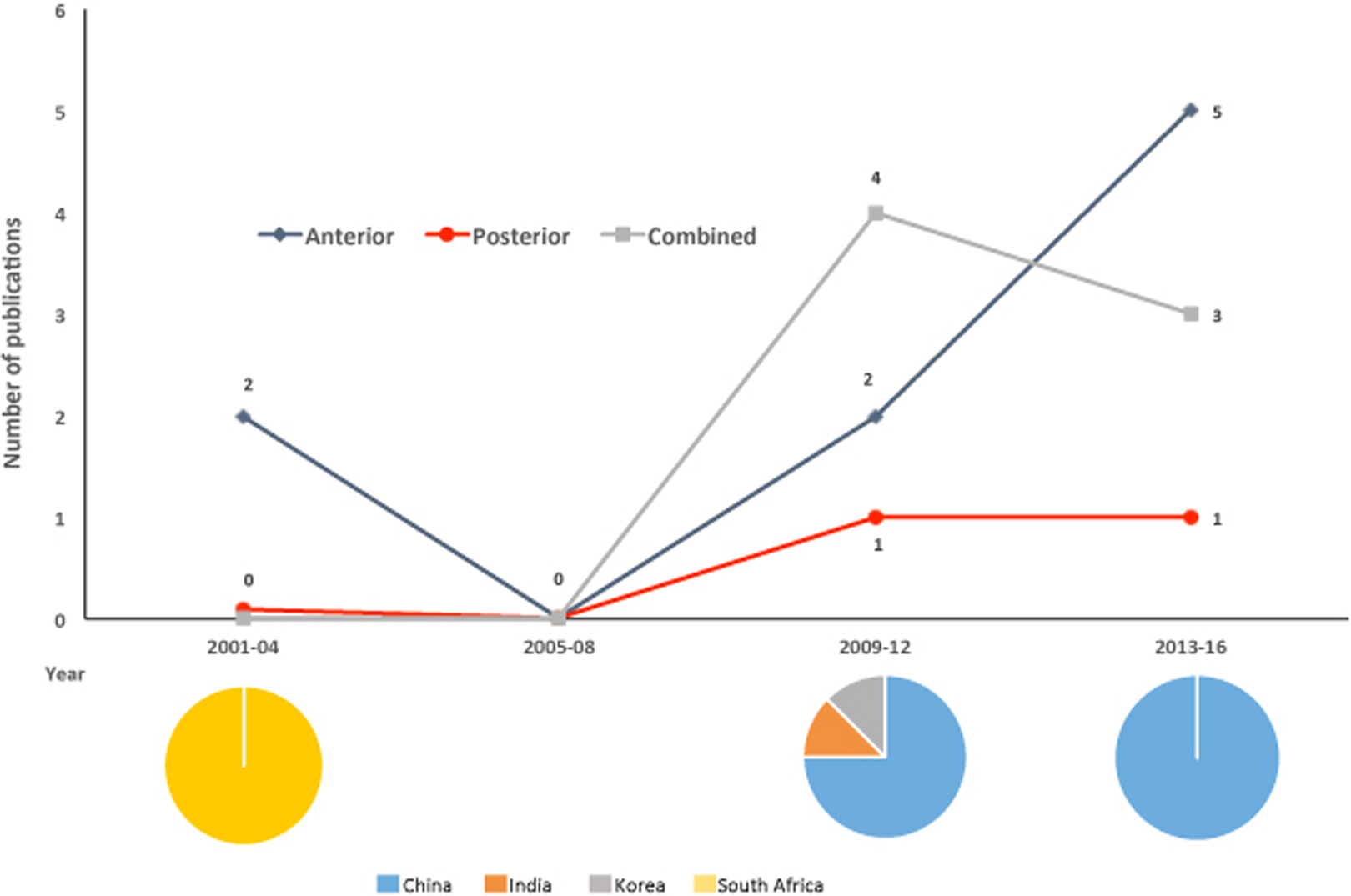
The change in the number of publications of surgery in pediatric spinal tuberculosis, stratified by surgical approach, 2001-2016.
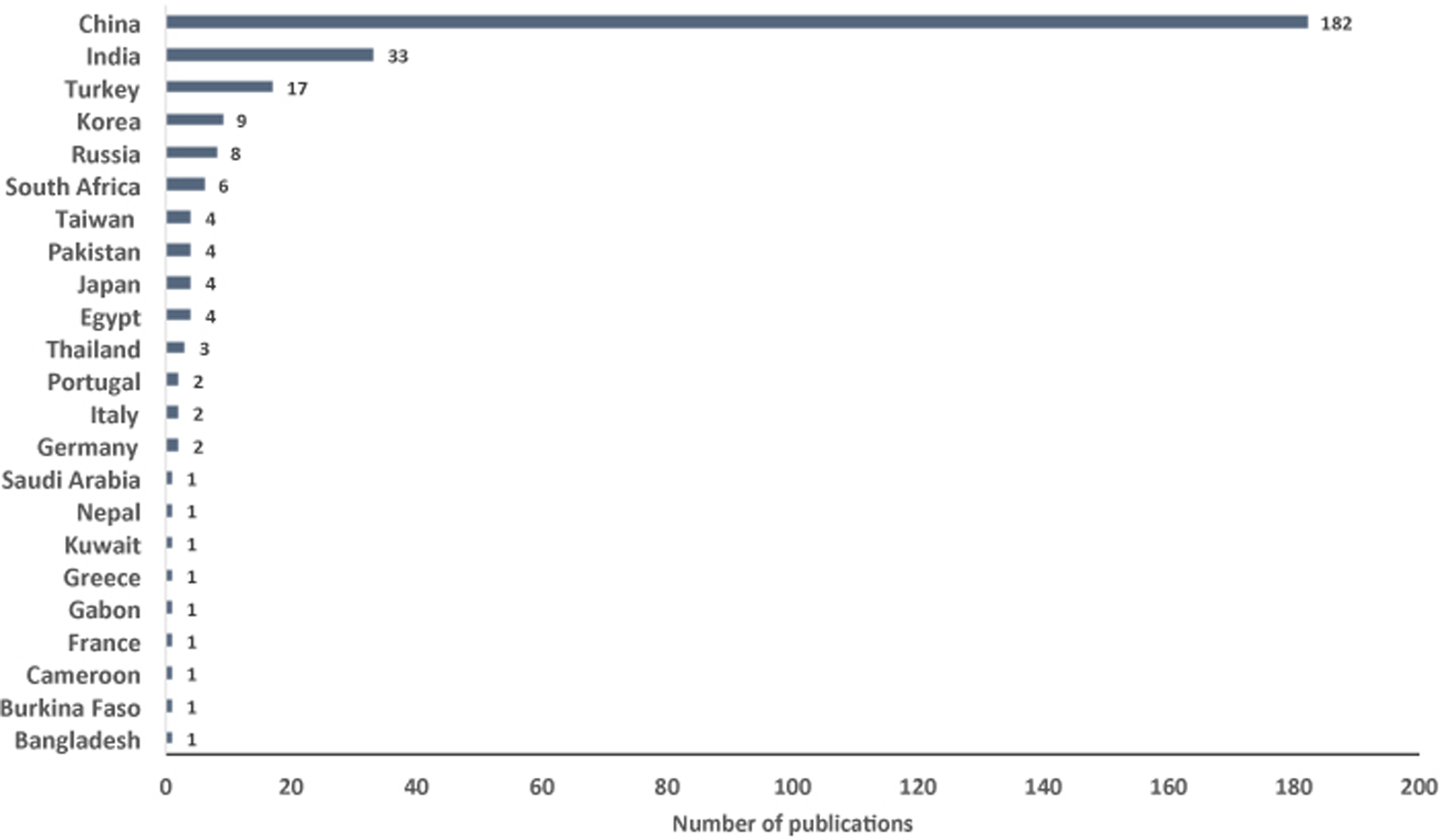
The number of publications of surgery in spinal tuberculosis, stratified by country originating the study, 2000-2016.
Key Question 3. What are the most common outcome measures following surgery?
Correction of angle/deformity, neurological deficit, bony fusion were the most frequently reported outcomes in published systematic reviews of surgery in spinal TB (Table 2).
11
–16
Loss of correction, operation time, blood loss, and hospital stay were also frequently recorded. Only 2 systematic reviews reported on return to activity level.
Outcomes Assessed in Systematic Reviews of Surgical Interventions for Spinal Tuberculosis.
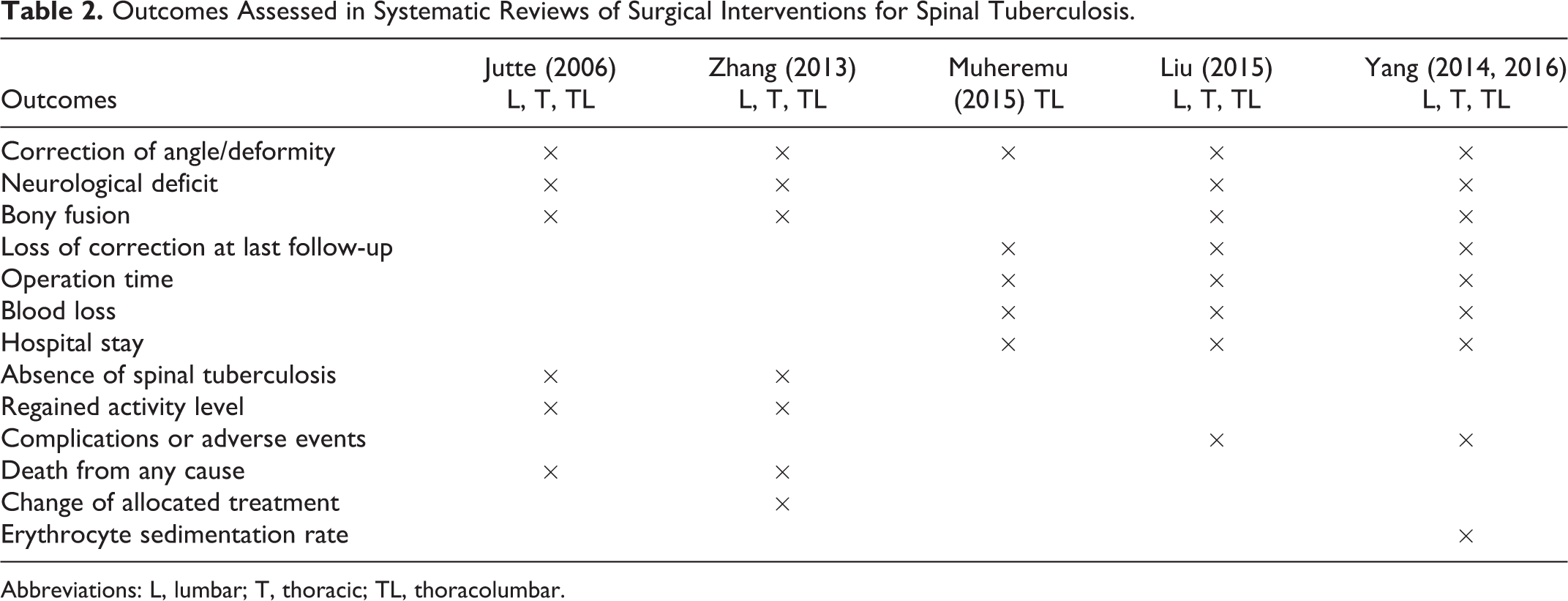
Abbreviations: L, lumbar; T, thoracic; TL, thoracolumbar.
Illustrative Case
A 45-year-old woman of Asian origin presented with inability to walk independently that progressively worsened over past 3 weeks before presentation. She also complained of gradually worsening dull mid-back pain over a period of 2 months. She had control over her bowel and bladder function. On neurological examination, she had 2/5 power in bilateral hip flexor, 3/5 power in bilateral knee extension and ankle dorsiflexion, and 3/5 power in long toe extensors (ASIA impairment scale, AIS C). Abdominal reflex was absent and deep tendon reflexes in the lower extremities were exaggerated (patella, 4+; ankle, 3+; bilateral ankle clonus, 10 beats sustained). She had a sensory level at around T10. She denied any constitutional symptoms. Her laboratory values revealed the following: hemoglobin, 9.3 g%; white blood cells, 6700/μL (4000-11 000); erythrocyte sedimentation rate, 62 mm/h; and C-reactive protein 8.2mg/dL (0-3).
Magnetic resonance imaging scan of the thoracic spine revealed a lesion involving T8-9 disc space with an epidural component that was significantly compressing the spinal cord with a prevertebral collection (Figure 6). A computed tomography (CT) scan of the region showed lytic destruction of the T8 and T9 vertebral bodies (Figure 7) with more than 50% body destruction.
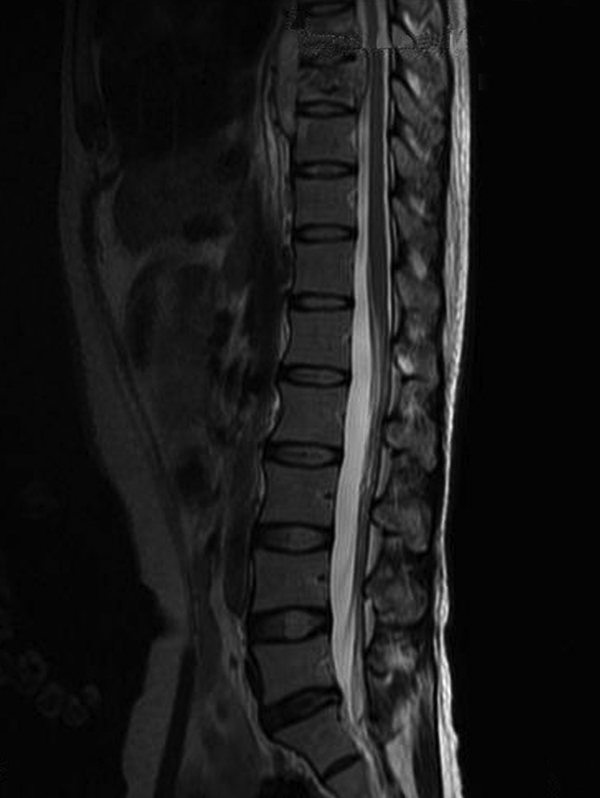
Magnetic resonance image (T2-weighted) showing T8-9 spondylodiskitis with epidural collection and significant spinal canal compromise.

Computed tomography scan sagittal image showing lytic destruction of the T8-9 vertebral bodies.
A transpedicular CT-based biopsy was done, which revealed presence of acid fast bacilli on Ziehl-Neelsen staining thus confirming the diagnosis of a tuberculous spondylo-diskitis. Culture and antibiotic sensitivity was pending. Her chest CT did not suggest any active TB lesion in the lungs and screening of the remaining spine was negative.
Considering the neurological decline, surgical intervention was considered. She underwent a 2-stage surgery. Stage 1 involved posterior stabilization from T5 to T12 along with T8-9 laminectomy and bilateral transpedicular decompression of the anterior epidural collection. At surgery, there was presence of thick granulation tissue that was found to envelop the spinal cord and bilateral T8 nerve roots. The granulation tissue layer was gently peeled off the neural structures. Stage-2 surgery involved anterior left-sided transthoracic approach with T8-9 vertebrectomy and anterior column support with a structural allograft and supplement fixation with pedicle screws in the vertebral body. The postoperative radiographs are shown in Figure 8.
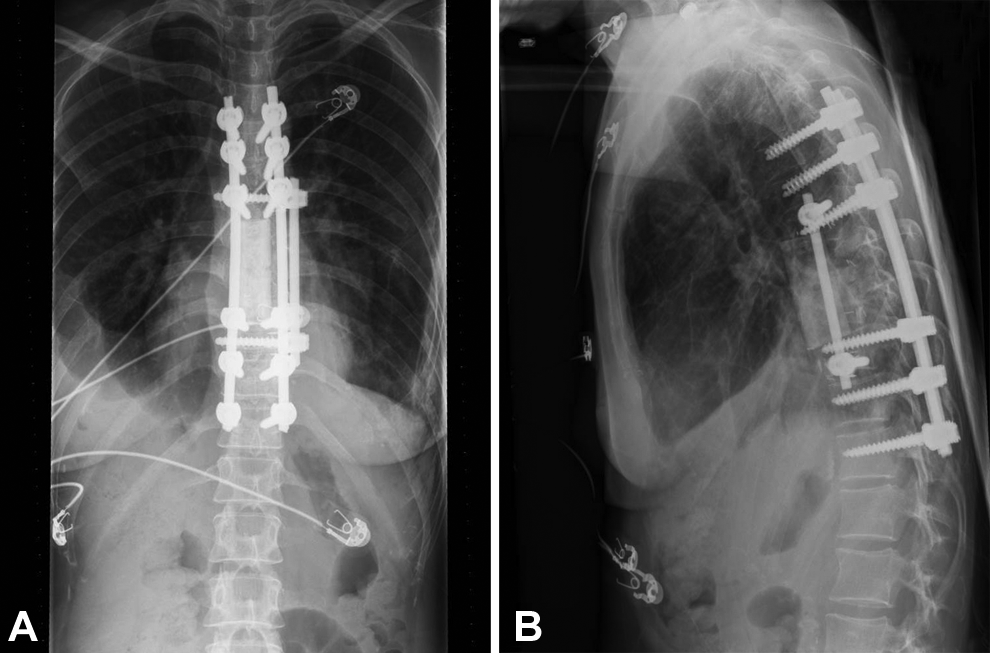
(a) One-year postoperative anteroposterior radiograph showing stable hardware position. (b) Lateral radiograph showing anteriorly placed structural allograft with healing of the lesion.
She was started on 4-drug anti-tuberculous chemotherapy regimen. The culture came out positive for Mycobacterium tuberculosis bacilli and the organism was sensitive to primary drugs.
The patient had a rapid recovery of the neurological status and she was independently ambulatory at 6 weeks and regained complete motor recovery at 3 months (AIS: E). Anti-TB medication was continued till 1 year with close monitoring of her clinical condition and laboratory values.
Discussion
The majority of the cases of spinal TB are seen in Southeast Asia and Africa, 17 and most of the recent literature we identified comes from that region.
While conservative treatment with anti-tuberculous drugs, including chemotherapy is standard therapy, the role of surgical intervention remains less clear. There are no clearly defined indications for surgery. The Medical Research Council (MRC) defined “favorable outcome” as absence of an abscess or sinus, which is radiological silent, with no neurological impairment. 18,19 The guideline did not include deformity in the “favorable outcome” measures. However, in our review of randomized controlled trials of surgical intervention in spinal TB, the presence of neurological compromise, deformity, and instability were the primary criteria for surgical intervention, irrespective of the anatomical area of the spine affected. Resistance to treatment, large abscess, and sequestrum formation were also found to be reasons for surgical intervention.
Neurological decline and deformity are the most feared complications of spondylodiscitis. 20 Neurological deficit can occur in 20% to 40% of cases in endemic and underdeveloped regions. 21 The average vertebral column collapse with conservative treatment alone is 15° and in 3% to 5% cases it could be severe up to 60° in severe cases. 19,22 –24
The anterior surgical approach was more commonly used in the cervical and cervicothoracic spine among our included studies, while the posterior approach was more commonly used in the remaining spinal column, particularly in studies published in the past 5 years. In the cervical spine, surgeons are well versed with the anterior approach, which allows for direct decompression and rigid structural stabilization. In the thoracic and lumbar spine, the availably of better posterior-based implants and widespread knowledge of safe surgical techniques to achieve circumferential decompression and stabilization may influence its widespread use. 25 –27
TB in pediatric spine in some scenarios tends to develop significant instability and “buckling effect.” 28 The combined approach was used frequently in children. This approach not only allows for deformity correction but also allows to save levels in surgery and prevent crank shaft phenomena in growing spine.
In our review, measurement of deformity correction was the most commonly described outcome measure followed by neurological deficit and identification of fusion.
In spite of the volume of surgical literature available on Pott’s disease, patient-related functional and quality of life outcomes were rarely reported in the large surgical literature reviewed. Going forward it may be of interest to see how the quality of life is being altered with surgical intervention in tuberculosis of spine.
Our review has several limitations. First, there are limited data sources for surgical indications. Second, we used an indirect measure of preferences for surgical approach based on the number of publications. Third, studies typically report on cases seen 3 to8 years prior to publication date, and therefore, the most recent surgical approaches are not necessarily represented here.
Conclusion
Majority of the current literature is from South Asia. The presence of neurological compromise, deformity and instability were the primary criteria for surgical intervention. In general, the anterior approach in the cervical and cervicothoracic spine and posterior approach in the thoracic and lumbar spine are the preferred approach for adult cases. Deformity correction, neurological deficit, and fusion are among the most commonly used treatment outcome measures following a surgical intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.