
Abstract
Study Design
Retrospective Exact Matched case-control study
Objectives
Surgical treatment delay in AIS due to family preferences is common. This study aims to quantify the increase in risks as the Cobb angle increases and provide a Quantifiable Risk Reference Table that can be utilized for counseling.
Methodology
AIS patients were divided into 3 groups: Group A: Cobb angle 50–60°, Group 61–70°, and Group CFinal ≥80°. Each patient in Group CFinal who had curve progression were then traced-back-in-time (TBIT) to review the clinical data at earlier presentations at 50–60° (C1), and 61–70° (C2). Patient demographics, radiological, operative, and outcomes data were compared between Group A vs C1 and Group B vs Group C2.
Results
A total of 614 AIS surgeries were reviewed. Utilizing the EM technique, a total of 302 AIS patients were recruited. There were 147, 111, 31, and 32 patients matched in Groups A, B, C1, and C2, respectively. C2 Final patients had 34% curve pattern change, 23.2% higher incidence of requiring two surgeries, and 17.3% increase in complications. There was a statistically significant increase of 2.4 spinal levels fused, 12% increase in implant density, 35% increase in operative time, 97% increase in intra-operative blood loss, 10% loss of scoliosis correction, 40% longer hospitalization stay, and 36% increase in costs for patients who had curve progression.
Conclusion
This study is the first to use a homogenously matched AIS cohort to provide a Quantifiable Risk Reference Table. The Risk Table provides essential knowledge for treating physicians when counseling AIS patients.
Keywords
Introduction
The management strategy of Adolescent Idiopathic Scoliosis (AIS) depends on the curve magnitude, rate of progression, and patients’ skeletal maturity. As the curve progresses, this may lead to issues of increased deformity, back pain, negative psychosocial effects, cardiovascular dysfunction, and potentially increased risk of mortality.1-5 However, surgeons are often faced with patients and their family members who want to avoid or defer surgery. These AIS patients are often asymptomatic, with no complaints of back pain, disability, and no cardiopulmonary dysfunction. They often do not see the need for surgery or appreciate the potential risks of increased complications and outcomes should the scoliotic curve progresses. The vast majority of these patients may decide to delay surgery due to family preferences, such as to avoid interfering with school examinations. 6 Other reasons for delaying surgery may range from wanting to explore treatment alternatives or are afraid of post-operative complications.7,8
Multiple studies have demonstrated that patients with curve progression will result in more complex surgeries and increased complications.6,9-12 These studies were unable to quantify the exact amount of increase in risks and outcomes correlated to the curve progression and subsequent increased surgical complexity. To the best of the authors’ knowledge, there are no studies in the literature that demonstrates a quantifiable increase in risks as the Cobb angle increases in near homogenously matched comparative cohorts. In this study, we aimed to provide a table with a set of quantifiable risk references that can be utilized during the consultation to counsel the patient and family members should they choose to defer AIS surgery at a Cobb angle of 50° and above.
Methodology
A retrospective Exact Matched (EM) case-control study conducted in a single university hospital was performed. All consecutive patients who met the inclusion criteria were analyzed. All AIS patients with Cobb angle ≥ 50° who underwent primary surgery from 2012 to 2019 were included. Patients who had previous spinal surgeries, neuromuscular, syndromic, or congenital scoliosis were excluded.
At the time of surgery, the Cobb angle of individual patients was analyzed. They were divided into 3 groups: Group A: Patients with Cobb angle of the structural curve between 50 and 60°, Group B of 61 and 70°, and Group CFinal of 80° and above. Group A and B represent AIS patients who underwent surgery when it was initially suggested (non-progressed group). Group CFinal represents AIS patients who, despite initial refusal eventually underwent surgery after their curves have progressed to 80° or above (progressed group) (Figure 1). Flowchart of matching. C1 and C2 refer to the same individual patient, but at different distinct time points when the patient was offered surgery but declined. All patients were matched using Exact Matching (EM).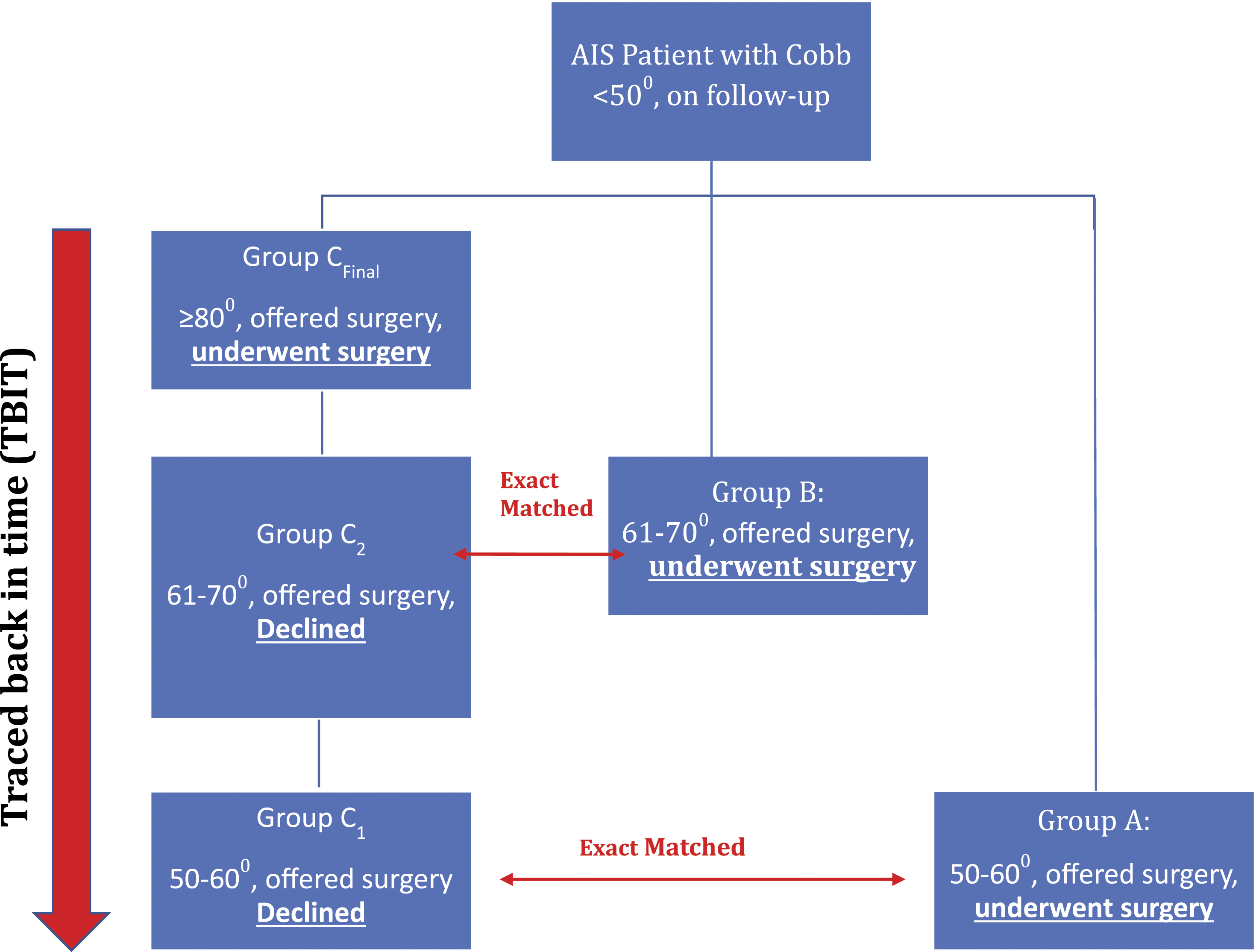
Each patient in group CFinal who had curve progression with the main structural curve of 80° and above was traced-back-in-time (TBIT) to review his or her clinical data at earlier presentations, when the main structural curve was at 50–60° (C1), and 61–70° (C2). C1 and C2 refer to the same individual patient (C1 Final, C2 Final), but at past distinct time points when the patient was first offered surgery but declined. The progressed, non-operative TBIT C1 and C2 patients were then used to match AIS patients who had undergone surgery without progression, to create the comparative cohorts as Group A and Group B. Figure 2 shows a patient who had curve progression. This particular patient had a curve change from Lenke 1 to Lenke 3, and subsequently Lenke 4. The patient was exact matched to patients in Group A and Group B (Figure 2). Patient demographics, radiological, operative, and outcomes data were compared between Group A vs C1 and Group B vs Group C2. Scoliosis Research Society 22 r (SRS-22r) score, Visual Analog Score (VAS), EQ5D, Short Form-36 Physical (SF-36 PCS), and Mental component score (SF-36 MCS) were analyzed. X-rays showing a patient with curve progression from Lenke 1 to Lenke 4.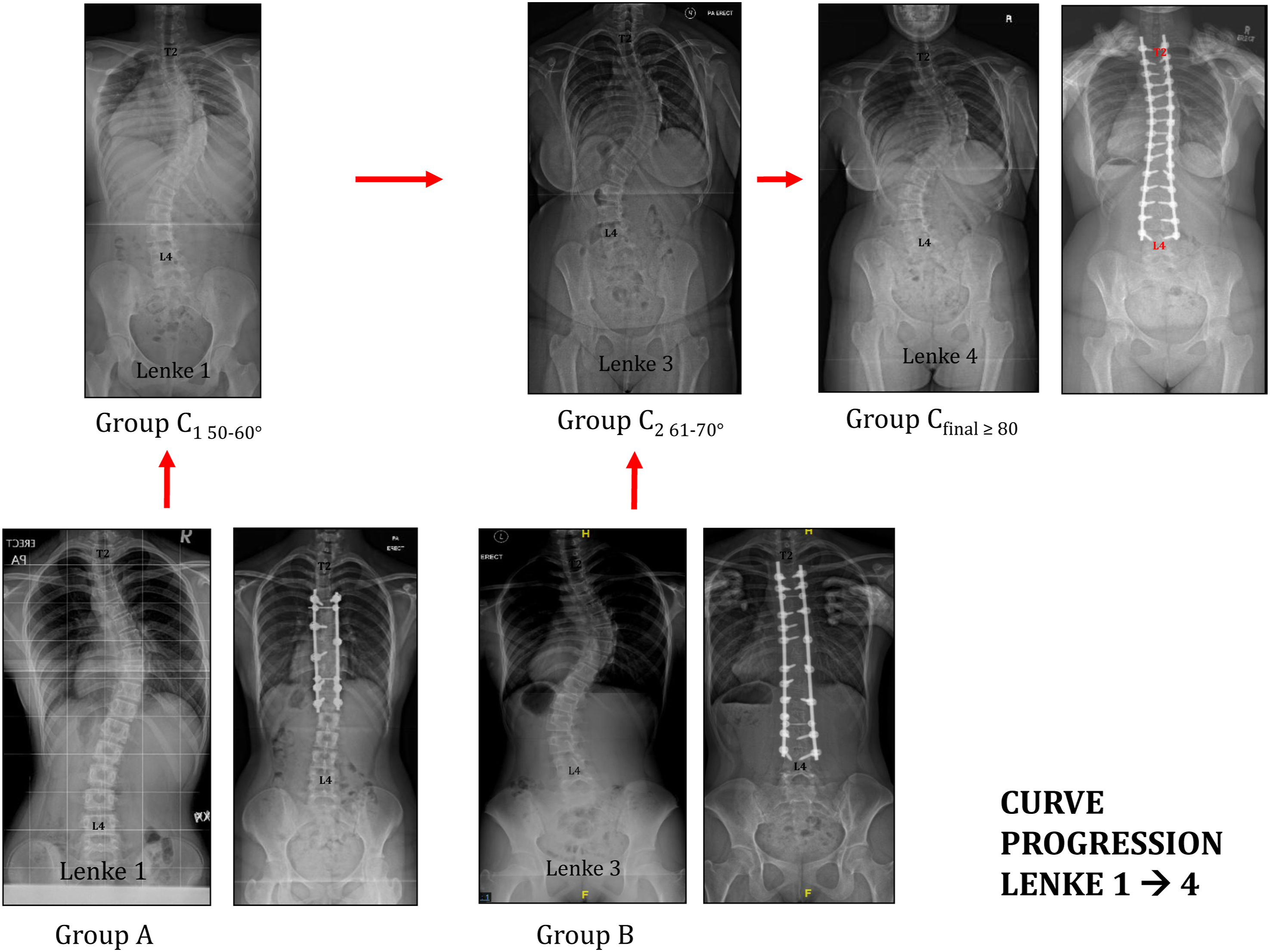
Informed Consent
As this was a retrospective study, informed consent was not required from the patients. Approval was obtained from the local Institutional Review Board (Approval: 2015/00576).
Cohort Matching
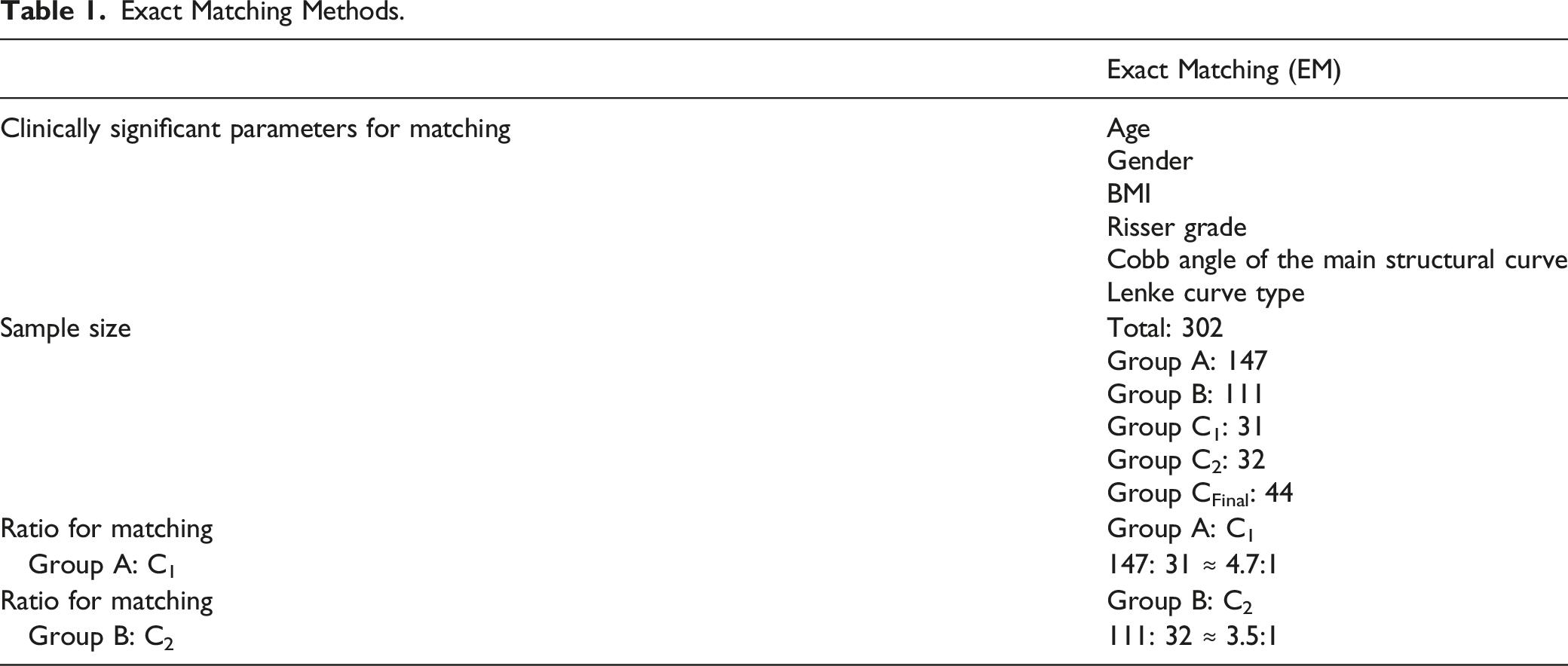
Exact Matching Methods.
Results
A total of 614 AIS surgeries were reviewed. 46 patients who had main structural curves of Cobb angle ≥ 80° were identified. 504 (82.1%) patients were females. The average age of the patient at the time of surgery was 14.2 ± 2.1 years old, BMI 19.0 ± 3.8 kg/m2. The most common Risser grade was grade 4 (29.8%), and grade 5 (23.8%). The most common Lenke curve pattern was type 1 (35.4%) and Lenke type II (25.3%). The mean pre-operative Cobb angle was 56.9 ± 6.6°.
Demographics of Patients Using Exact Matching Technique.
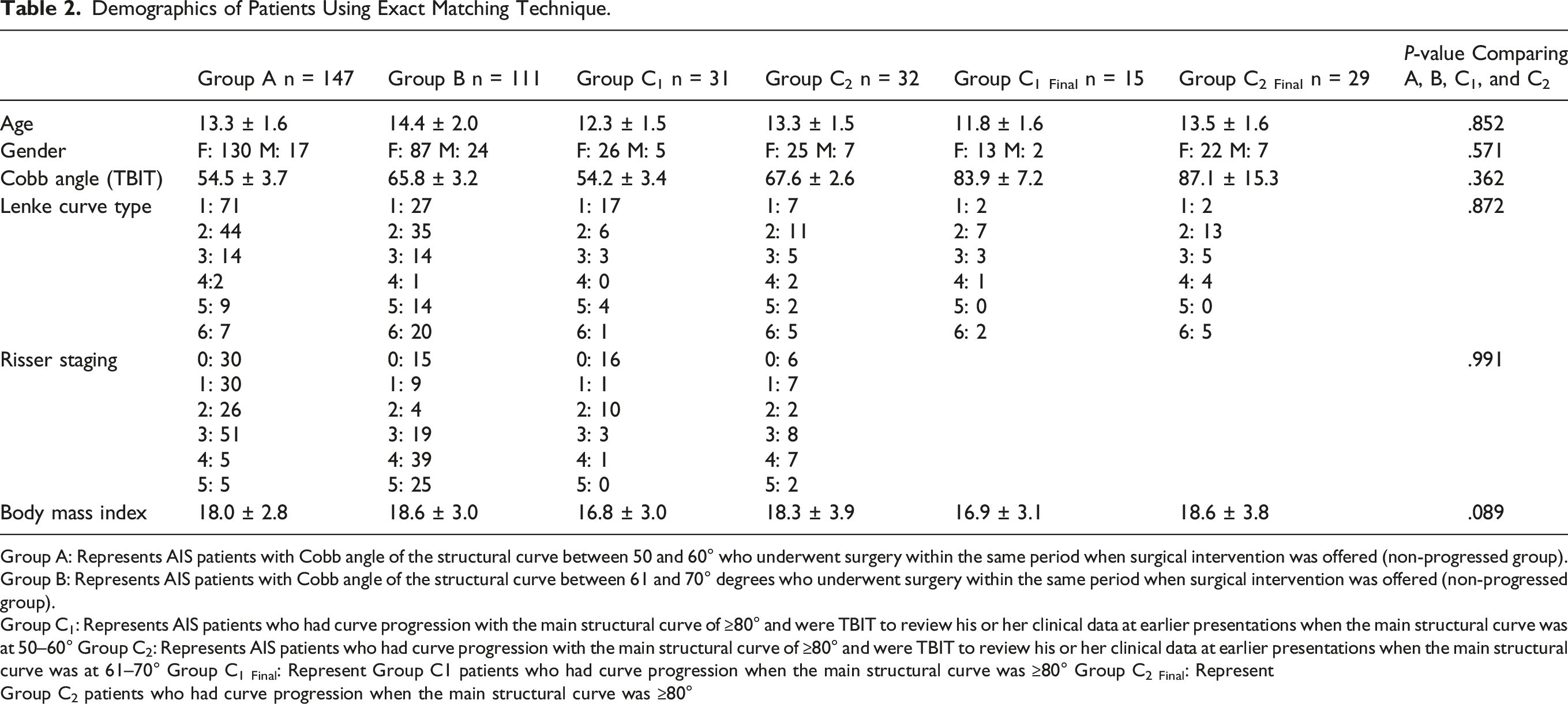
Group A: Represents AIS patients with Cobb angle of the structural curve between 50 and 60° who underwent surgery within the same period when surgical intervention was offered (non-progressed group).
Group B: Represents AIS patients with Cobb angle of the structural curve between 61 and 70° degrees who underwent surgery within the same period when surgical intervention was offered (non-progressed group).
Group C1: Represents AIS patients who had curve progression with the main structural curve of ≥80° and were TBIT to review his or her clinical data at earlier presentations when the main structural curve was at 50–60° Group C2: Represents AIS patients who had curve progression with the main structural curve of ≥80° and were TBIT to review his or her clinical data at earlier presentations when the main structural curve was at 61–70° Group C1 Final: Represent Group C1 patients who had curve progression when the main structural curve was ≥80° Group C2 Final: Represent
Group C2 patients who had curve progression when the main structural curve was ≥80°
A total of 147 patients were included in Group A to match the patients in Group C1. 130 (88.4%) patients were females, and the average age at the time of surgery was 13.3 ± 1.6 years old. The mean pre-operative Cobb angle was 54.5 ± 3.7°, and the mean BMI was 18.0 ± 2.8 kg/m2. The most common pre-operative Risser grade was grade 3 (34.7%), and the most common Lenke curve type was type I (48.3%), and type II (29.9%). The EM ratio was 147: 31 (Group A: Group C1) (Table 1 and 2).
Similarly, a total of 111 patients were matched and recruited in Group B. 87 (78.4%) were females, and the average age at the time of surgery was 14.4 ± 2.0 years old. The mean pre-operative Cobb angle was 65.8 ± 3.2°, and the mean BMI was 18.6 ± 3.0 kg/m2. The most common pre-operative Risser grade was grade 4 (35.1%), and the most common Lenke curve type was type II (31.5%) and type I (24.3%). The EM ratio was 111: 32 (Group B: Group C2) (Table 1 and 2).
Change in Curve Pattern
A total of 24 (38.1%) CFinal patients experienced curve pattern changes at their eventual surgery. In Group C1 Final, 11 (35.5%) patients were noted to have a Lenke curve pattern change from type 1 to type 2.1 patient (3.2%) had curve type change from type 5 to 6, and 1 patient (3.2%) had curve type change from 6 to type 4 at their eventual surgery. A total of 41.9% of C1 Final patients whose initial Cobb angle was 50–60° but had their scoliosis progressed to Cobb angle ≥80° experienced curve pattern changes.
In Group C2 Final, 2 patients (6.3%) were noted to have a Lenke curve type change from type 1 to type 2, 2 patients (6.3%) from type 1 to type 3, 4 patients (12.5%) from type 5 to type 6, 1 patient (3.2%) from type 5 to type 3, and 2 patients (6.3%) from type 3 to type 4 at their eventual surgery (Table 2). A total of 34.4% of C2 Final patients whose initial Cobb angle was 61–70° but had their scoliosis progressed to Cobb angle ≥ 80° experienced curve pattern changes.
Fusion Levels, Number of Screws, and Implant Density
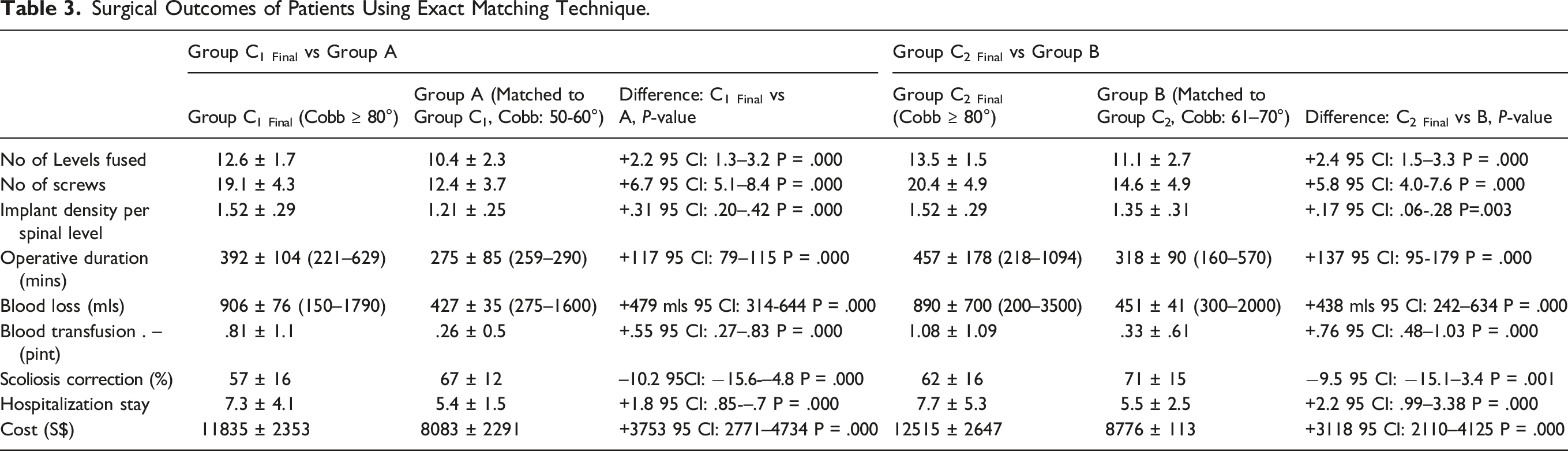
Surgical Outcomes of Patients Using Exact Matching Technique.
Risk Quantification Reference Table for Progressed AIS Surgery.
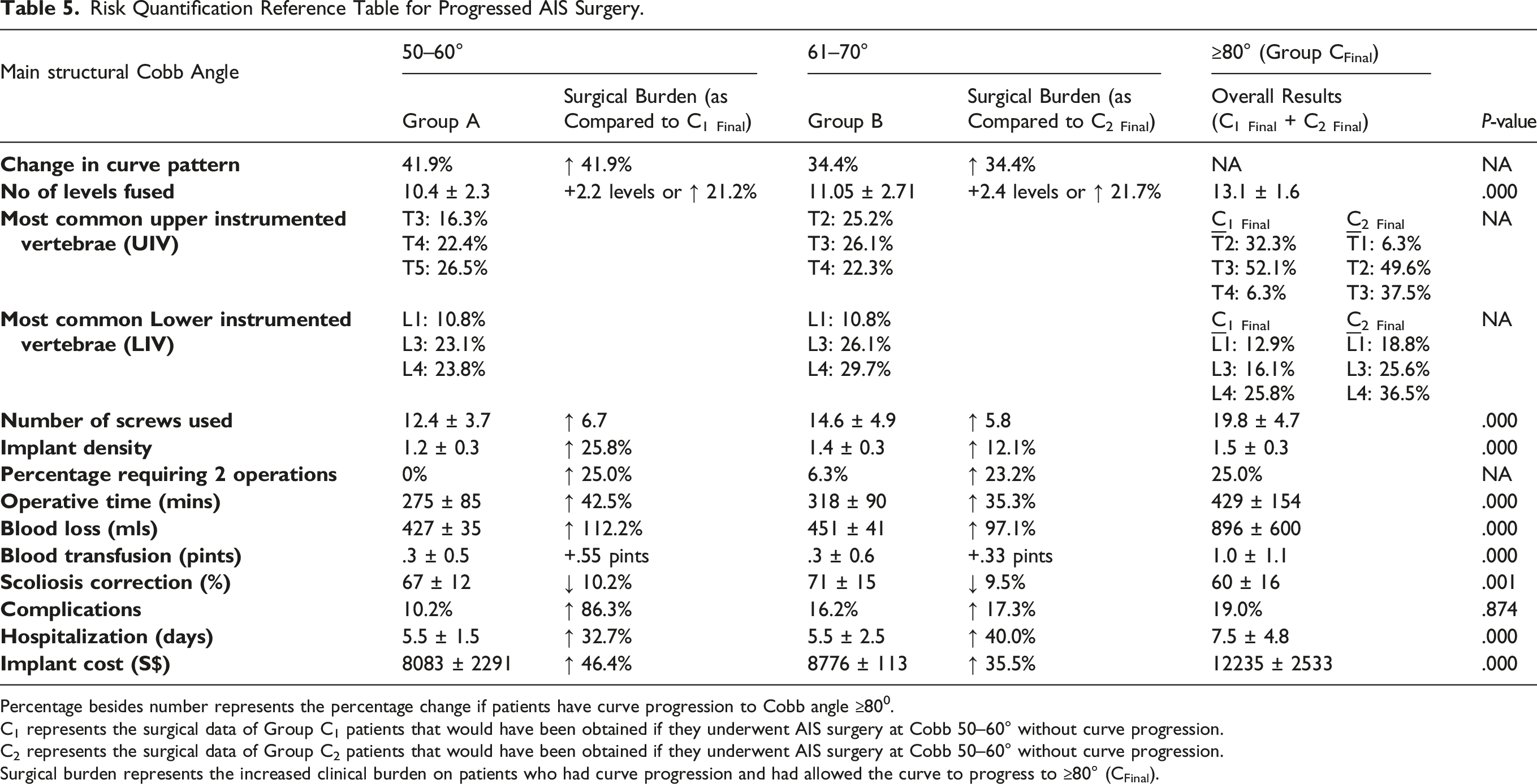
Percentage besides number represents the percentage change if patients have curve progression to Cobb angle ≥800.
C1 represents the surgical data of Group C1 patients that would have been obtained if they underwent AIS surgery at Cobb 50–60° without curve progression.
C2 represents the surgical data of Group C2 patients that would have been obtained if they underwent AIS surgery at Cobb 50–60° without curve progression.
Surgical burden represents the increased clinical burden on patients who had curve progression and had allowed the curve to progress to ≥80° (CFinal).
Patients who chose to defer surgery from AIS curves at 61–70° and had subsequent curve progression to ≥ 80° would have an additional 2.4 spinal levels fused in their AIS surgeries (95% CI: 1.5–3.3, P-value = .000), an increase of 5.8 pedicle screws used (95% CI: 4.0–7.6, P-value = .000) and a mean increase in mean implant density by .17 implant per spinal level (95% CI: .06–.28, P-value = .003), or a 12.1% increase in implants used (Table 3,5).
Operative Time, Intra-operative Blood Loss, and Blood Transfusion
Patients who chose to defer surgery from AIS curves at 50–60° and had curve progression to ≥ 80° would have an increase of mean surgical duration by 117 minutes (95% CI: 79–115, P-value = .000) or 42.5% increase in operation time. In addition, these patients would have an additional 479 mls of intra-operative blood loss (95% CI: 314–644, P-value = .000), approximately a 112% increase, requiring an extra .55 pints of blood transfusion post-operatively (95% CI: .27–.83, P-value = .000) (Table 3,5). There was a 25.0% increased risk of these C1 Final patients requiring 2 surgeries if their curve progressed (Table 3,5).
Patients who chose to defer surgery from AIS curves at 61–70° and subsequently had curve progression to ≥ 80° would have an increase of mean surgical duration by 137 minutes (95% CI: 95–179, P-value = .000) or 33.6%. There was an additional 438 mls of intra-operative blood loss (95% CI: 241.5–634, P-value = .000), approximately a 99% increase, requiring an extra .76 pints of blood transfusion post-operatively (95% CI: .48–1.03, P-value = .000) (Table 3,5). There was a 23.2% increased risk of these C2 Final patients requiring 2 surgeries if their curve progressed (Table 3,5).
Complications
A higher overall complication rate was noted in Group CFinal (progressed group) but this was not statistically significantly different when compared to Group A and B group (non-progressed surgery group) (19.0% vs 12.8%, P-value = .874). In patients with a smaller curve from Group A and B, 15 patients had respiratory complications. There were 6 gastrointestinal-related, 3 wound-related, 2 transient neurological, and 1 broken screw complication found. 2 patients required revision surgeries. There were no mortality or patients who were paralyzed. In patients with curve ≥ 80° (Group CFinal), 5 patients had respiratory complications. There were 2 gastrointestinal-related, 3 wound-related, and 1 transient neurological complication. 2 patients had revision surgeries. There were no mortality or neurological deficits (Table 3,5).
Outcome Scores
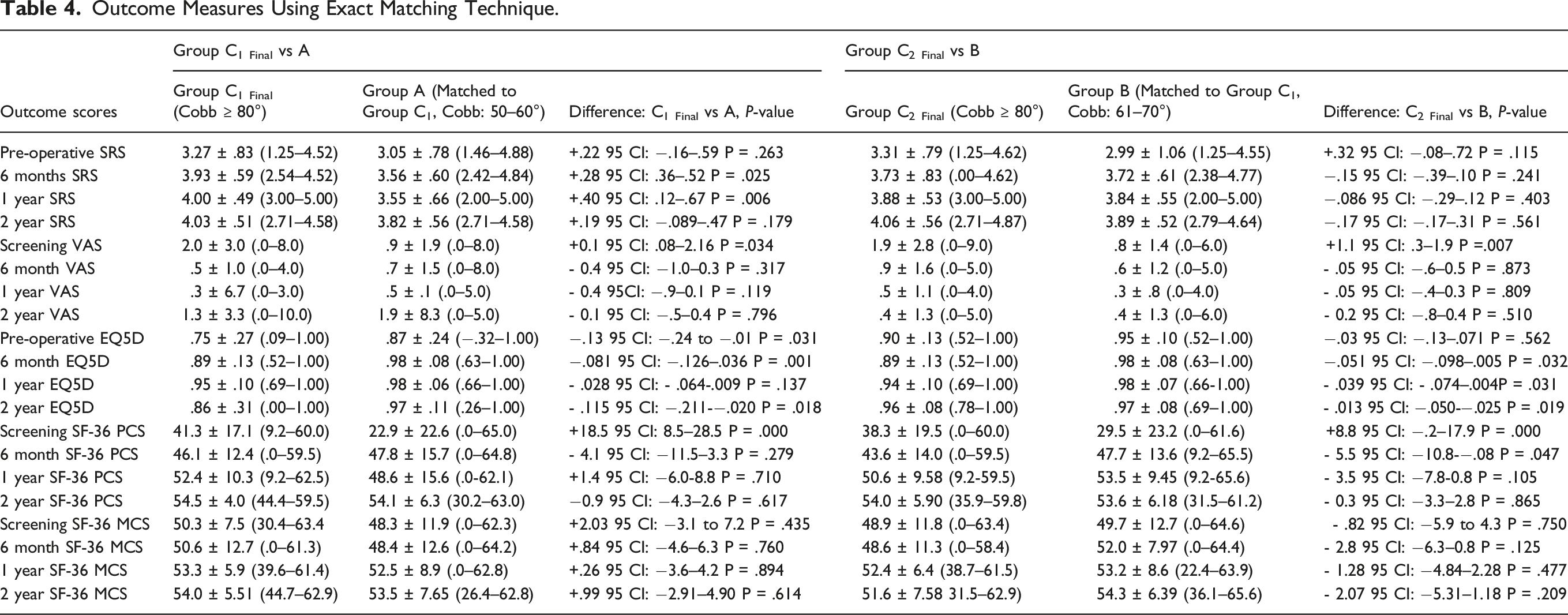
Outcome Measures Using Exact Matching Technique.
Hospitalization Stay and Implant Cost
Patients who chose to defer surgery from AIS curve at 50–60° and had subsequently curve progressed to ≥ 80° would have an increase in mean hospitalization stay of 1.8 days (95% CI: .845–2.717, P-value = .000) and an additional implant cost of S$3753 (95% CI: 2771–4734, P-value = .000) or 46.4% increase (Table 3,5).
Patients who chose to defer surgery from AIS curve at 61–70° and subsequently had progression to ≥ 80° would have an increase of mean hospitalization stay of 2.2 days (95% CI: .990–3.380, P-value = .000) and an additional implant cost of S$3118 (95% CI: 2110–4125, P-value = .000) or 35.5% increase (Table 3,5).
Discussion
A common clinical scenario which many spine surgeons face is that after offering surgical intervention to the AIS patient, the patient or family members will often decline or opt to defer the surgery. The AIS patient and family members perceive that the asymptomatic spinal curvature to be benign and can be left alone, even at Cobb angle of 50° and above. However, in the Iowa Study with 50-year long-term prospective follow-up, Weinstein et al reported that AIS patients with thoracic curves of ≥ 50° will likely continue to progress, while curves < 30° are usually stable.2,4,14 Many authors had reported that patients with scoliotic curves which progressed to 80° and above would have a more difficult scoliosis corrective surgery and were expected to have increased post-operative complications.11,15-17 In this study, we aimed to provide a Risk Quantification Reference Table for progressed AIS surgery to guide physicians’ patient counseling process (Table 5).
As the Cobb angle of the AIS structural curve progresses and increases in magnitude, the once flexible compensatory curve will also increase in magnitude and stiffness. The increased rigidity of the compensatory curve further changes the scoliosis curve pattern as AIS progresses.18,19 In a study of 35 patients, Yang et al estimated that delay in surgery in immature AIS patients with >40° curves led to 34% of patients having curve pattern changes according to the Lenke classification. These patients with curve progression and curve pattern changes had increased spinal levels fused in their AIS surgeries. 9 In the current study, using the Exacting Matching technique, a total of 24 (38.1%) patients had curve changes. In Group C1 Final (patients who presented at 50–60°), 13 (41.9%) patients underwent curve changes. 12 (92.3%) of them changed from a single structural curve pattern to a double structural curve pattern, while 1 (7.7%) of them changed from double curve pattern to triple curve pattern. In Group C2 Final (patients who presented at 61–70°), 11 patients (34.4%) patients underwent curve changes. 8 (72.7%) of them changed from a single structural curve pattern to a double structural curve pattern, while 3 (27.3%) of them changed from double curve pattern to a triple curve pattern. Our study showed that a higher percentage of curve pattern changes were noted in AIS patients who had curve progression from Cobb angle 50 to 60° than that of a curve from 60 to 70°. This represents a window of opportunity to alter the natural history of the scoliosis progression if this information was told to the patients and family members, to change their mind of not delaying surgical intervention at 50–60°.
When the flexible curve compensatory curves become structural curves, this would lead to a downstream effect of increased spinal fusion levels, operative time, and intra-operative blood loss. 10 The Group C Final patients who curve progression from an initial scoliotic curve of 50–60° would have an increased risk of additional levels of spinal fusion, more pedicle screws, and an increase in operative time, and increased blood requiring post-operative blood transfusion. Due to the increase in AIS curve magnitude and stiffness, these C1 Final patients had 25.0% higher incidence of requiring 2 operations for the corrections of scoliosis, often involving anterior and posterior spinal approaches.
In contrast to the C1 Final patients, as their scoliosis progresses, only the UIV appears to propagate more proximally when compared to C2 Final patients, who as their curve progresses, both UIV will propagate more proximally and LIV propagate more distally. The most common UIV noted in C2 Final patients who had deferred and finally had surgery was T2 (49.6%), T3 (37.5%) with 6.3% at T1, whereas the most common LIV was at L4 (36.5%), L3 (25.6%) with 3.1% at L5. In a study of 378 female AIS patients, Grabala et al. reported that AIS patients who were fused to L3 or L4 had an 8% higher incidence of lower back pain. When the LIV was moved more distally, the risk of requiring a Cesarean section during childbirth was increased to 55%. 20 Bartie et al. reported that 75% post-operative AIS patients experienced back pain, with higher intensity of pain experienced by patients who were fused to L4. 21 As the LIV moved more caudally, range of motion and fingertip-to-floor distance were also significantly restricted. 22 Hence, the knowledge of a potential need for more proximal UIV and distal LIV requirements would be an important point in the counseling of AIS patients and family members should they decide to defer the surgery.
Another important outcome consideration in patients and family counseling for AIS surgery would be the degree of Cobb angle correction, the length of hospitalization stay, functional outcome, and surgical costing. In this study, the CFinal patients with curves progressing to 80° and beyond had almost 1 liter of intra-operative blood loss, which was twice as much as what they would have lost should the patient choose to have surgery performed at a smaller Cobb angle without delay. In addition, the final scoliosis correction was reduced from 70% correction in Group A and B patients to 60% in Group CFinal patients. Hospitalization stay was prolonged from less than one week in the Group A and B patients to more than one-week hospitalization stay in the Group CFinal patients.
One of the limitations of the current study is its retrospective nature and its cohorts matching methodology. Although the EM technique increases the chance of excluding patients who do not match and reduces the sample size, it ensures that the matching population is near homogenous and provides the most accurate matched cohort study that, to the best of the authors’ knowledge, is lacking in the reported AIS literature. While there may be variations of surgical techniques and clinical practices in AIS surgeries from one country to another, the current study reported data is in line with what was published in the literature, and hence our risk reference table is likely of clinical relevance.10,23-25 Lastly, as this was an exact matched study based on retrospective data, some of the patients from Group A and B may not have curve progression.
In conclusion, using the EM technique, we found that AIS patients who chose to defer surgery at 50–60° or 60–70° and subsequently progressed to ≥ 80°, would have an estimated 41.9% or 34.4% curve pattern change, a statistically significant increased number of spinal levels fused by 2.2 or 2.4 spinal levels, 26% or 12% increase in implant density required, 42.5% or 35% increased operative time, 110% or 99% additional intra-operative blood loss, 37% or 35% longer hospitalization stay, and 51% or 39% increased costs, respectively. There was an overall 10% loss of scoliosis correction, a more proximal UIV, and more distal LIV, and a 25% higher incidence of 2 surgeries required in patients who deferred AIS surgery. There was a trend toward a higher complication rate, although this was not statistically significant (86% or 17%, respectively). The authors believe that the current study results can be translated into important knowledge which is essential for any treating physicians when counseling the AIS patients and their parents who want to delay AIS surgery when the scoliosis Cobb angle reaches 50° or beyond. The Risk Quantification Reference Table for progressed AIS surgery (Table 5) provided in this study may transform care and give better value for both the AIS patients and the health system, should the AIS patient be persuaded to have the AIS surgery without delay and avoid the costly consequences of scoliosis progression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.