
Abstract
Study Design:
A retrospective, comparative study.
Objective:
To determine the radiological behavior of the lumbar curve in selective fusions in premenarchal girls with adolescent idiopathic scoliosis (Lenke 1 B/C).
Methods:
A retrospective, comparative study was conducted. Selective fusion was performed in 21 patients younger than 18 years. The patients were divided into 2 groups: group A, after menarche (n = 12) and group B, before menarche (n = 9). Angles (preoperative, and at 1 and 2 years postoperatively) of the fused thoracic curves and the corresponding lumbar curves were measured and compared. For statistical analysis, the t test was used with a significance level of P < .05.
Results:
Mean preoperative angle value of the proximal/main thoracic curve was 61° in group A and 57° in group B (P = .44), and 21° and 20°, respectively, in the first year postoperatively (P = .61). Mean preoperative angle value of the lumbar curve was 43° in group A and 42° in group B (P = .87), while at 1 year after surgery, this curve was 19° in both groups (P = 0.91), and at 2 years postoperatively, the curve was 16° in group A and 17° in group B (P = .75).
Conclusions:
Over a 2-year follow-up, we did not find significant radiological differences in lumbar curves between patients who underwent surgery before and after menarche.
Introduction
Selective thoracic fusion is a surgical option for patients with adolescent idiopathic scoliosis (AIS) aimed to achieve a limited spinal arthrodesis trying to preserve as many mobile segments as possible. Nevertheless, it is important to consider the risk of loss of correction and progression of the unfused lumbar curve, especially in skeletally immature patients. 1,2 The aim of the classification system for AIS by Lenke was to establish treatment guidelines defining curve types according to region, magnitude, flexibility, sagittal profile, and the relationship of the apex of the lumbar curve to the center sacral vertical line. 1
Skeletal development is a complex and multifactorial phenomenon. Different clinical and radiological indicators of skeletal development have been described, such as chronological age, Tanner stage, and menarche, as well as Risser classification, Sanders stage, and status of the triradiate cartilage. Menarche, although a late event, is objectively evaluable and generally recognized by the patient.
Menarche is the culmination of a series of physiological and anatomical processes of puberty, occurring after hypothalamic-pituitary-gonadal axis reactivation and gonadotropin-releasing hormone secretion. 2 -4
Skeletal maturity is a relevant aspect to consider in the management of patients with AIS for prognostic and therapeutic purposes. 4,5
The aim of this study was to determine the radiological behavior of the fractional lumbar curve in selective fusions in premenarchal girls with AIS (Lenke 1 B/C).
Material and Methods
A retrospective, cross-sectional, and comparative study was conducted evaluating a total of 21 female patients who underwent surgery for AIS between October 2012 and March 2016. The inclusion criteria were Lenke 1 curves, lumbar modifier B or C, angle value of the curve >40°, selective fusion, fixation with pedicle screws, and at least 2 years of postoperative follow-up. The exclusion criteria were anterior approach, pseudarthrosis, and implant failure.
The patients were divided into 2 groups: The first group included 12 patients who were postmenarche and the second group included 9 patients who were premenarche at the time of surgery. Pre- and postoperative (immediate, first year, and second year) radiological evaluation consisted of standing anteroposterior and lateral radiographs of the full spine to assess lateral curvature using the Cobb method. The lower limit of instrumentation was established mainly based on 2 radiologic features: the neutral vertebra and the most proximal instrumented vertebra dissected by the central sacral vertical line.
Demographic, clinical, and radiologic parameters prior to surgical treatment are detailed in Table 1. In both groups, pre- and postoperative angle values of both the main thoracic curve and the fractional lumbar curve were analyzed and compared.
Preoperative, demographic, clinical and radiologic features.
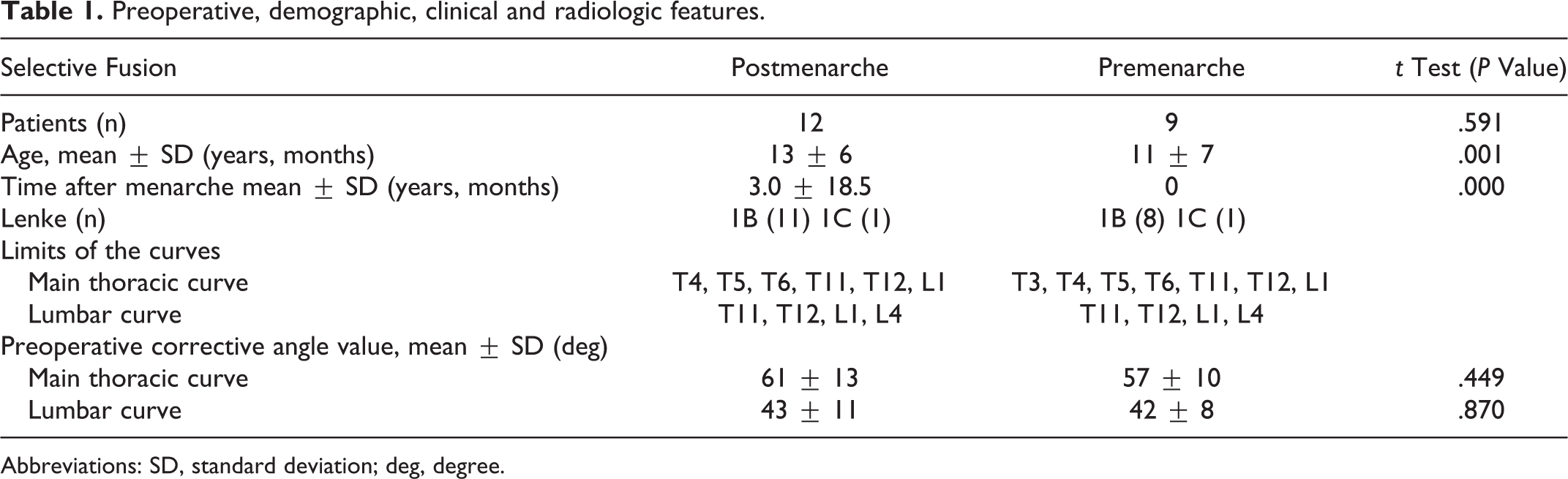
Abbreviations: SD, standard deviation; deg, degree.
Statistical analysis was performed using the t test and P < .05 was considered statistically significant. The SPSS 18 program was used for all statistical analysis.
The study was approved by the hospital institutional review board and because of the retrospective observational nature of the study, the institutional review board waived the informed consent.
Results
Mean age of the patients in the premenarche group was 12 years 1 month, compared with 13 years 8 months of those in the postmenarche group (P = .001), with a reported mean postmenarche time of 3 years at surgery in the latter group. All patients in the premenarche group had their first menstruation before the follow-up was completed.
The most common curve type (Lenke) was 1B in both groups. In the postmenarche group, the mean preoperative angle of the main thoracic curve was 61° (range, 41° to 87°), whereas the angle in the premenarche group was 57° (range, 42° to 70°) (P = .449).
One year after surgery, the mean angle of the main thoracic curve were 20°(range, 9° to 41°) and 21° (range, 12° to 31°) in the post- and premenarche groups, respectively (Table 2). The percentage of correction was 67% in the former, and 63% in the latter group, without statistically significant differences (P = .617).
Preoperative and Postoperative radiological parameters.
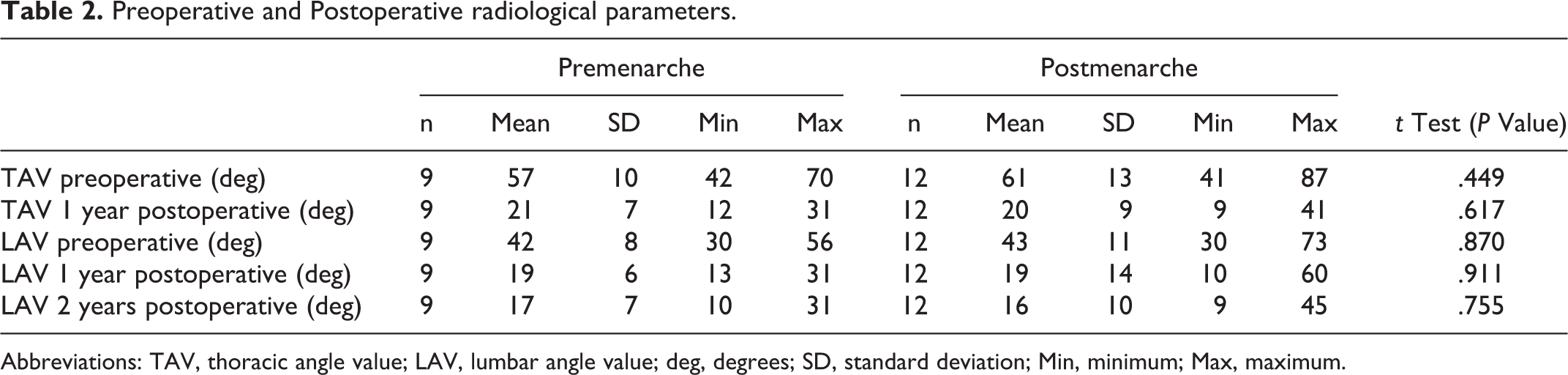
Abbreviations: TAV, thoracic angle value; LAV, lumbar angle value; deg, degrees; SD, standard deviation; Min, minimum; Max, maximum.
As regards outcome of the fractional lumbar curve, in the postmenarche group, the mean angle value was 43° (range, 30° to 73°) preoperatively, 24° (range, 15° to 65°) immediately postoperative, 19° (range, 10° to 60°) at 1 year postoperatively, and 16° (range, 9° to 45°) at 2 years postoperatively, while in the pre-menarche group fractional lumbar curve angle values were 42° (range, 30° to 56°), 22° (range,17° to 36°), 19° (range, 13° to 31°), and 17° (range, 10° to 31°), respectively (Figure 1).
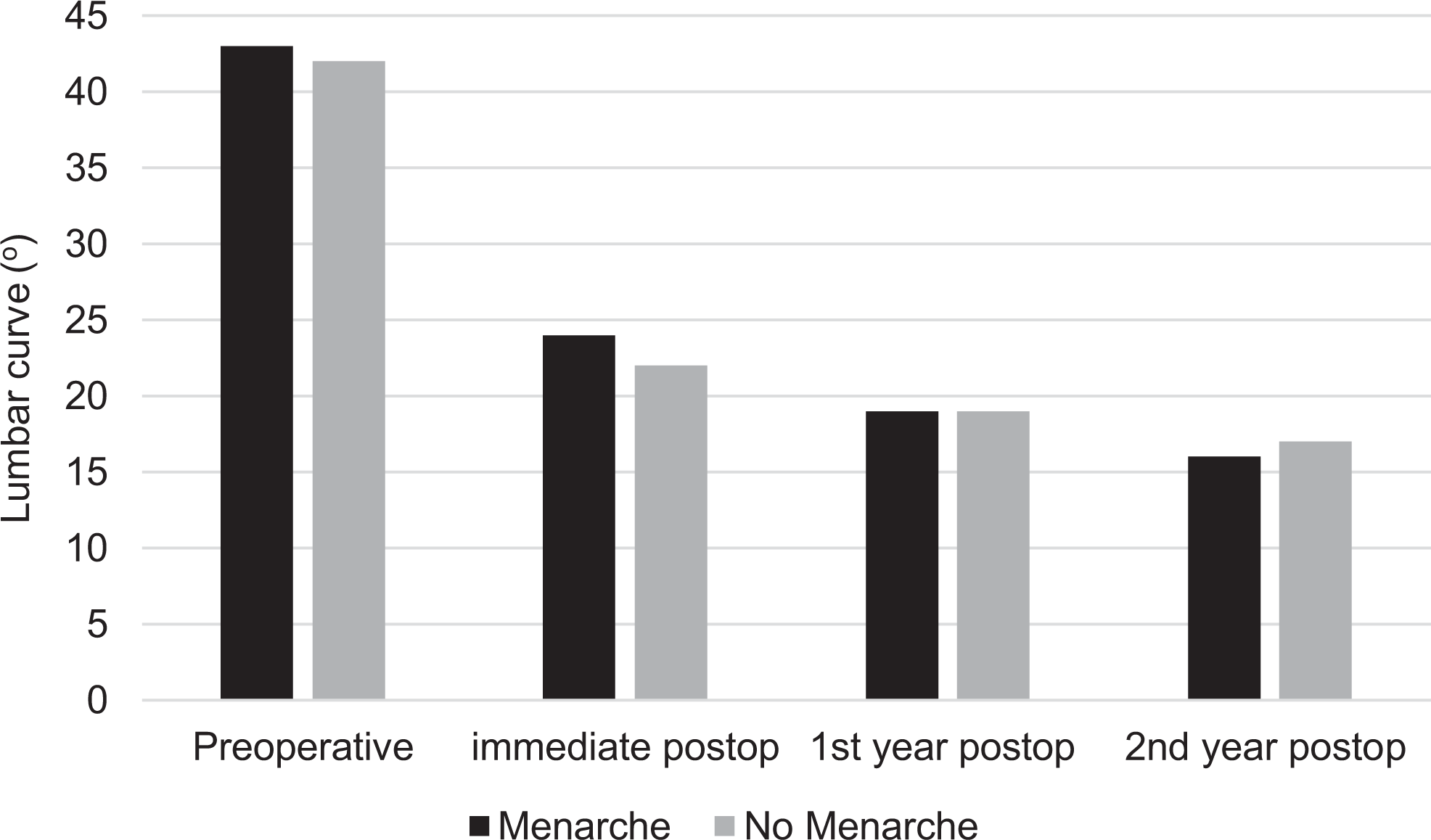
Lumbar curve evolution.
At 1 year postoperatively, mean lumbar curve correction was 55% (P = .911).
Between the first and the second year of follow-up, the behavior of the fractional lumbar curve did not show significant differences between both groups (P = .755) (Table 2).
Discussion
In 2001, Lenke et al 6 developed a treatment-directed classification system for AIS aimed to avoid curve progression, achieve global spinal balance with good coronal and sagittal alignment, and preserve as many mobile segments as possible.
Multiple clinical and radiological factors associated with skeletal maturation have been analyzed as risk factors for curve progression in patients with AIS. Growth velocity and skeletal age, with different measurement methods, are objective markers of pubertal maturation; however, menarche, although one of the late signs of skeletal maturity, is an event clearly identifiable by the patient and generally discussed during the medical interview, is still one of the most commonly used parameters in daily clinical practice. 3,4,6,7 Considering this paradigm, in our series this aspect of skeletal maturation was evaluated in relation to the progress of the lumbar curve in patients with AIS who underwent selective thoracic fusion.
Postoperative correction of the main thoracic curve after selective fusion is a factor analyzed in different series. In 16 patients (68%, Risser sign 4-5) with a mean preoperative angle value of 63°, Studer et al 8 obtained a postoperative decrease of 20 degrees without significant loss of correction at the 2-year follow-up. Edwards et al 9 reported a loss of correction of >10° after a mean follow-up of 5 years in 46% of skeletally immature patients (Risser 0-2). In our series, analyzing the main thoracic curve and considering menarche as a parameter for skeletal maturity, preoperative angle values and correction percentages were similar to those reported in the literature, and no significant differences were found regarding loss of correction of the fused curve at 1 year of follow-up.
At 2 years of follow-up, Sponseller et al 10 found a spontaneous loss of correction of the nonfused lumbar curve of 17° in patients with open triradiate cartilage, compared with 9° in those with closed triradiate cartilage and Risser stage 3-4.
In a series by Lenke et al 11 evaluating 44 patients who underwent selective thoracic fusion (Lenke type 1-2 C), among other factors, the evolution of the lumbar curve in relation to the skeletal maturity of the patients was analyzed. Of the patients considered to be immature (Risser 0-1), 26% had a >10° increase of the lumbar curve at a mean follow-up of 5 years. Of the skeletally mature patients (Risser 3-4), only 6% had a similar increase during the same time of follow-up. 11
In our series, the majority of patients had a lumbar type C modifier; however, both groups showed a spontaneous correction of the curve with angle values that were similar to the first year of follow-up. At the end of follow-up, the premenarche group showed less reduction, although not statistically significant, in the curve parameters. It is important to emphasize that all the girls in the premenarche group had their first menstruation before the follow-up period was completed.
Limitations of our study are the lack of sagittal plane analysis, the retrospective nature and small sample size, and the time of follow-up, considering that the subjects were patients in the process of skeletal development. Nevertheless, regarding this latter aspect, beyond the difference in age, the remaining variables showed to be homogeneous when comparing both study populations.
Conclusion
Selective fusion remains the treatment of choice in the majority of patients with Lenke type 1 curves, even in those who are skeletally immature. Menarche does not seem to be a strong predictive factor for the radiologic outcome of the lumbar curve, mainly at the mid-term follow-up, to be used in the surgical timing and strategy planning in patients with AIS.
To determine the behavior of the lumbar curve beyond 2 years, more evidence reflected in long-term studies is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.