
Abstract
Study Design
Retrospective review.
Objectives
To establish a cutoff value for hand grip strength and predict the favorable outcomes of adult spinal deformity surgery.
Summary of Background Data
Hand grip strength (HGS) has been suggested to predict surgical outcomes in various fields, including adult spinal deformity (ASD). However, to the best of our knowledge, no study has established a cutoff value for HGS in patients with ASD.
Methods
This study included 115 female patients who underwent reconstructive spinal surgery for ASD between September 2016 and September 2020. HGS was measured preoperatively. The Oswestry Disability Index (ODI), EuroQOL-5-dimension (EQ-5D), and visual analog scale (VAS) scores for back pain were all recorded both before and after surgery. Patients were dichotomized either into favorable or unfavorable outcome groups using an ODI cutoff score of 22 at 1 year after surgery. Multivariate logistic regression analysis was done to identify significant factors leading to favorable outcomes. A receiver operating characteristic (ROC) curve was drawn to define the cutoff value of HGS for favorable outcomes.
Results
Multivariate logistic regression analysis showed that HGS is significantly associated with favorable surgical outcomes in ASD (P = .031). The ROC curve suggested a cutoff value of 14.20 kg for HGS (area under the curve (AUC) = .678, P = .013) to predict favorable surgical outcomes in ASD. The surgical complications were not significantly affected by HGS.
Conclusion
The HGS of patients with ASD can be interpreted with a cutoff value of 14.20 kg. Patients with HGS above this cutoff value showed superior surgical outcomes at 1 year after surgery compared to those below this cutoff value.
Keywords
Introduction
Adult spinal deformity (ASD) and its treatment are two of the most important fields in the spine society. With various approaches to improve surgical techniques, 1 prognostic factors with the predictive ability for favorable surgical outcomes are among the topics of the deepest interest of spine surgeons.2,3 The hand grip strength (HGS), an indicator of voluntary muscle strength, is well known for its significance in assessing frail populations with sarcopenia.4-6 Findings in recent studies suggest that HGS measurement is a very simple yet useful tool to predict surgical outcomes, duration of hospital stay, and even mortality.2,5,7-10 Its use is not only limited to musculoskeletal problems, but it is also used in fields such as cardiothoracic surgery for malignancies. 9
An obstacle to interpreting the HGS values of patients with ASD is the lack of a known cutoff value to determine whether a certain HGS value is sufficiently high or inadequately low. HGS is greatly influenced by patient population characteristics, such as age, gender, and certain clinical conditions. 11 Certain cutoff values have been suggested for the diagnosis of sarcopenia;4,12-14 however, these values are based on normative data. Patients with ASD have low physical performance, weak muscle strength, and high disability in daily activities. 15 Therefore, this study aimed to determine an appropriate cutoff value for HGS and use it to predict the favorable surgical outcomes of patients with ASD.
Materials and Methods
Study Design and Patient Selection
This retrospective review was approved by the Institutional Review Board of our hospital (B-1607-409-101). Written informed consent was obtained from each participant before the commencement of the study. A total of 180 patients who underwent reconstructive spine surgery for ASD between September 2016 and September 2020 were screened. The inclusion criteria were as follows: (1) age >50 years; (2) female; (3) ASD diagnosis with a sagittal imbalance and treatment plan for corrective surgery, defined as a sagittal vertical axis (SVA) of >5 cm, pelvic tilt (PT) of >20°, or pelvic incidence (PI)–lumbar lordosis (LL) of >20° on lateral radiographs in a standing position; (4) subjective disability due to a stooping posture. The exclusion criteria were as follows: (1) thoracic and/or cervical myelopathy; (2) other musculoskeletal problems disabling walking activity; (3) syndromic or neuromuscular diseases; (4) serious general medical conditions such as sepsis or malignancy; (5) incomplete questionnaires on health-related quality of life and disability.
Measurement of HGS and Patient-Reported Outcomes
Hand grip strength is a routine preoperative examination for patients scheduled to undergo surgery at our department. HGS was measured in both hands using a dynamometer (GRIP-D5101; Takei, Niigata, Japan). The patients sat in a comfortable position, with their elbows extended, and squeezed the dynamometer with maximum strength. HGS was measured twice for both hands, with a short break in between. The best performance, regardless of hand dominance, was thus recorded.
Patient-reported outcomes (PRO), measured based on the Oswestry disability index (ODI score), EuroQOL-5 dimension (EQ-5D score), and visual analog scale (VAS score) for back pain, was examined before surgery and 3, 6, and 12 months after surgery.16,17 The validated ODI (Version 2.1a) is a self-report questionnaire for assessing back-related functional disability, comprising 10 items, each with 6 possible responses, and scores ranging from 0 to 5. The total score is the sum of the scores from the 10 items, which are then converted to a 0–100 scale. The EQ-5D is a five-dimensional classification system based on 5 health dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. 18 The EQ-5D measure can be interpreted as a continuous outcome scored from 0 to 1, with 1 indicating “full health” and 0 indicating “death”. A VAS was used to evaluate back pain based on a 10-cm line, indicating “no pain” and “most severe pain” at its opposite ends.
Surgical Procedures
All surgeries were performed by the lead author with expertise in spine surgery, with an individual but similar strategy for each patient. The Mizuho OSI modular table system was used for patient positioning with maximal LL. Then, a simple lateral radiograph was obtained to calculate the PI–LL mismatch. The surgical strategy of either multi-level posterior column osteotomies or pedicle subtraction osteotomy at L3 combined with additional posterior column osteotomy at other levels was chosen based on the PI–LL mismatch amount. The extent of the osteotomy (3-column osteotomy or posterior column osteotomy) was determined for proper correction of sagittal imbalance. In most cases, the uppermost instrumented vertebra (UIV) was T10 with variations, whereas the sacrum was generally the lowermost instrumented vertebra (LIV) with iliac screw insertion in most cases. Interbody fusion with a cage at lower lumbar levels, cantilevering of the rods, and compression between the screws were performed to aid deformity correction in the sagittal plane. Dual-rods at both sides with domino connectors were applied in most cases for stable fixation of long-level constructs and prevention of rod breakage.
Radiographic Measurements
Spinopelvic parameters, including the SVA, sacral slope (SS), PT, PI, and LL, were measured before and after surgery using biplanar stereo radiographic full-body imaging (EOS imaging, Paris, France). Proximal junctional kyphosis (PJK) was defined as (1) postoperative proximal junctional sagittal Cobb angle >10° and (2) a change in the proximal junctional sagittal Cobb angle from the preoperative measurement of >10°. The proximal junction is between the upper endplate of the vertebra 2 levels superjacent to the UIV and the lower endplate of the UIV. Proximal junctional failure (PJF) was defined as any of the following: UIV or UIV+1 fracture, disruption of the posterior osseo-ligamentous complex, pull-out of instrumentation, or neurological deficits.
Statistical Analysis
Continuous variables were compared using independent t-tests and are presented as mean ± standard deviation. Categorical variables were compared using the χ2 test. Patients were dichotomized into either favorable or unfavorable outcome groups. A favorable surgical outcome was defined as an ODI score of 22 or less, reflecting the level of well-being observed in healthy populations with no chronic lower back pain. 19 The odds ratio for every expected variable was calculated using univariate and multivariate logistic regression analyses to predict favorable surgical outcomes. Variables associated with favorable outcomes at P < .20 in the univariate analysis were entered into the multivariate analysis. A receiver operating characteristic (ROC) curve was drawn to select a cutoff value of significantly associated variables to predict favorable surgical outcomes. The AUC of .5, .5 –.6, .6 –.7, .7 –.8, .8 –.9, and >.9 indicates chance performance, bad predictive ability, sufficient predictive ability, good predictive ability, very good predictive ability, and excellent predictive ability, respectively. 20 The optimal cutoff value was set as the value that maximized the sum of sensitivity and specificity. All statistical analyses were performed using SPSS 26 (SPSS, Inc., Chicago, IL, USA). Statistical significance was set at P < .05.
Results
Patient Characteristics
This study included 180 patients who were screened between September 2016 and September 2020 for the study. Among these, 39 male patients were excluded because HGS is greatly influenced by sex. 11 Of the 26 patients further excluded, 7 patients had no preoperative HGS data, and 19 patients had incomplete data on PRO measures, including the ODI score, EQ-5D score, and VAS score for back pain. Finally, 115 patients were included as the study subjects.
Patient Characteristics of Total Study Population and After Dichotomization into Favorable or Unfavorable Surgical Outcome.
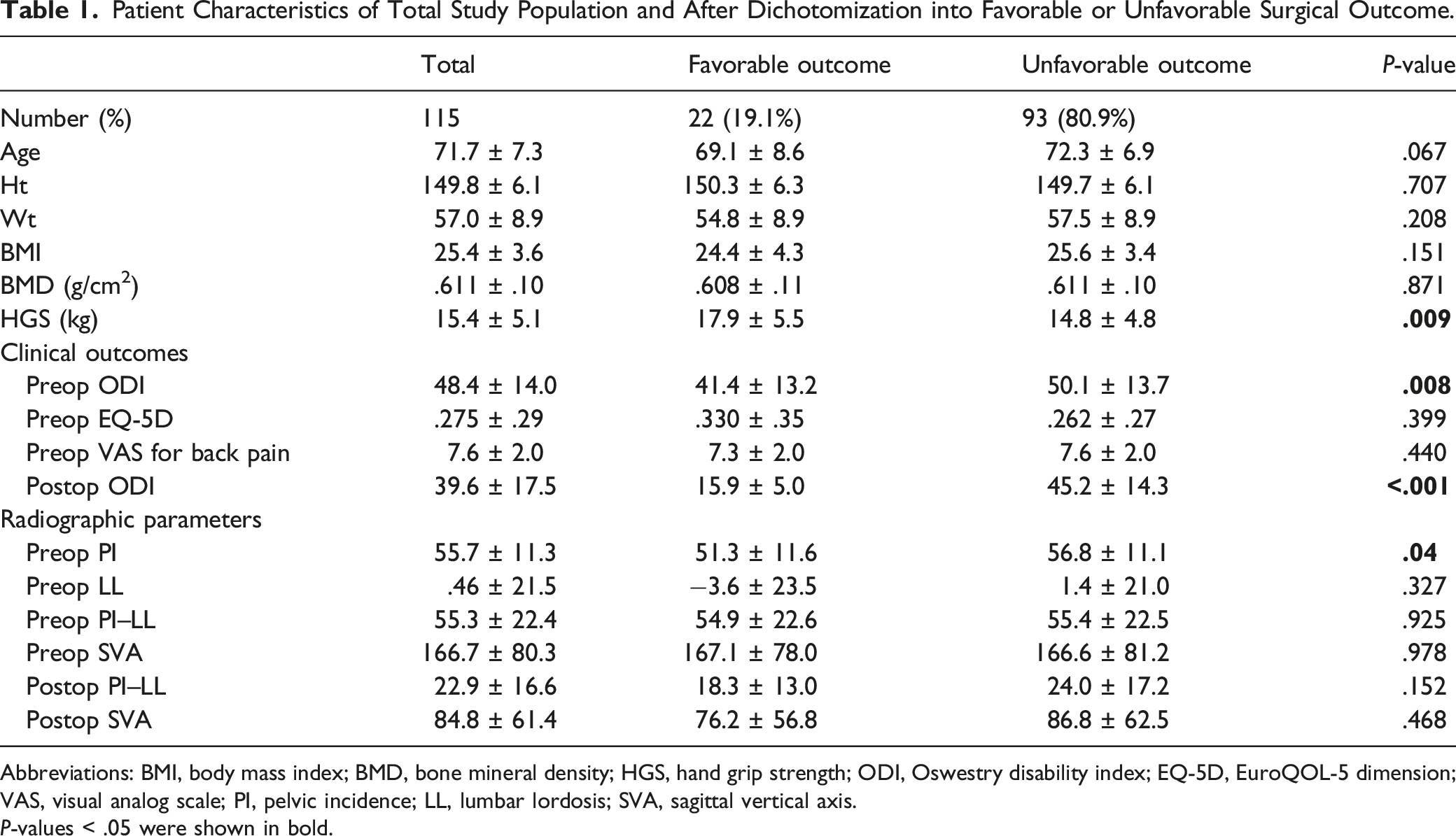
Abbreviations: BMI, body mass index; BMD, bone mineral density; HGS, hand grip strength; ODI, Oswestry disability index; EQ-5D, EuroQOL-5 dimension; VAS, visual analog scale; PI, pelvic incidence; LL, lumbar lordosis; SVA, sagittal vertical axis.
P-values < .05 were shown in bold.
Multivariate Analysis of the Predictors of Favorable Surgical Outcome
Multivariate Logistic Regression Analysis for Prediction of Favorable Surgical Outcome, Defined as Oswestry Disability Index Score of 22 or less at 1 year After Surgery.
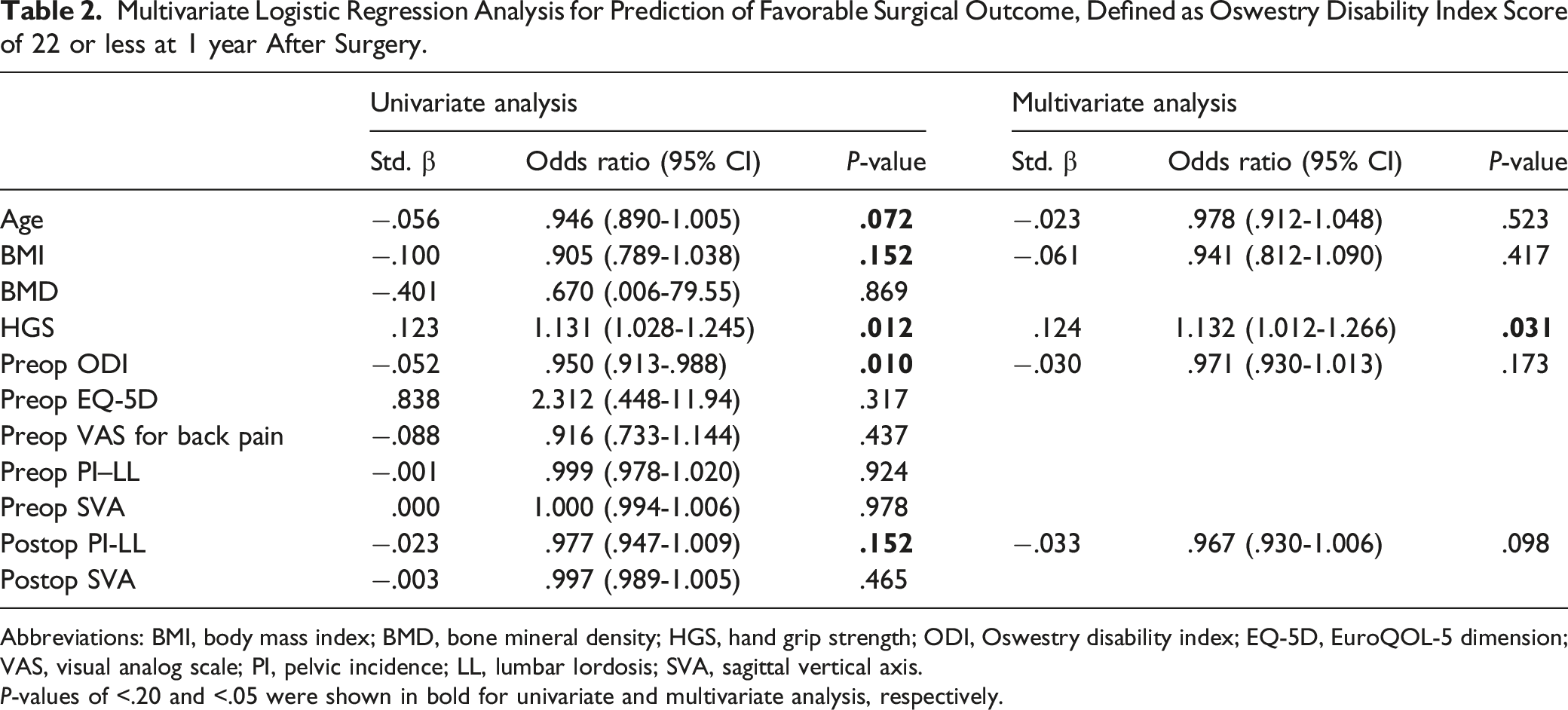
Abbreviations: BMI, body mass index; BMD, bone mineral density; HGS, hand grip strength; ODI, Oswestry disability index; EQ-5D, EuroQOL-5 dimension; VAS, visual analog scale; PI, pelvic incidence; LL, lumbar lordosis; SVA, sagittal vertical axis.
P-values of <.20 and <.05 were shown in bold for univariate and multivariate analysis, respectively.
Multivariate logistic regression analysis showed that HGS was most significantly associated with favorable surgical outcomes (odds ratio, 1.132; P = .031), whereas other factors did not show statistical significance (Table 2).
ROC Curve of HGS
An ROC curve was drawn to suggest a cutoff value for HGS to predict favorable surgical outcomes at 1 year after surgery (Figure 1). A cutoff value of 14.20 kg of HGS showed a sensitivity of .813 and a specificity of .500. The AUC was .678 (95% confidence interval, .539–.818), indicating “sufficient predictive ability” (P = .013).
20
Receiver operating characteristics (ROC) curve of hand grip strength to predict favorable surgical outcomes of patients with adult spinal deformity.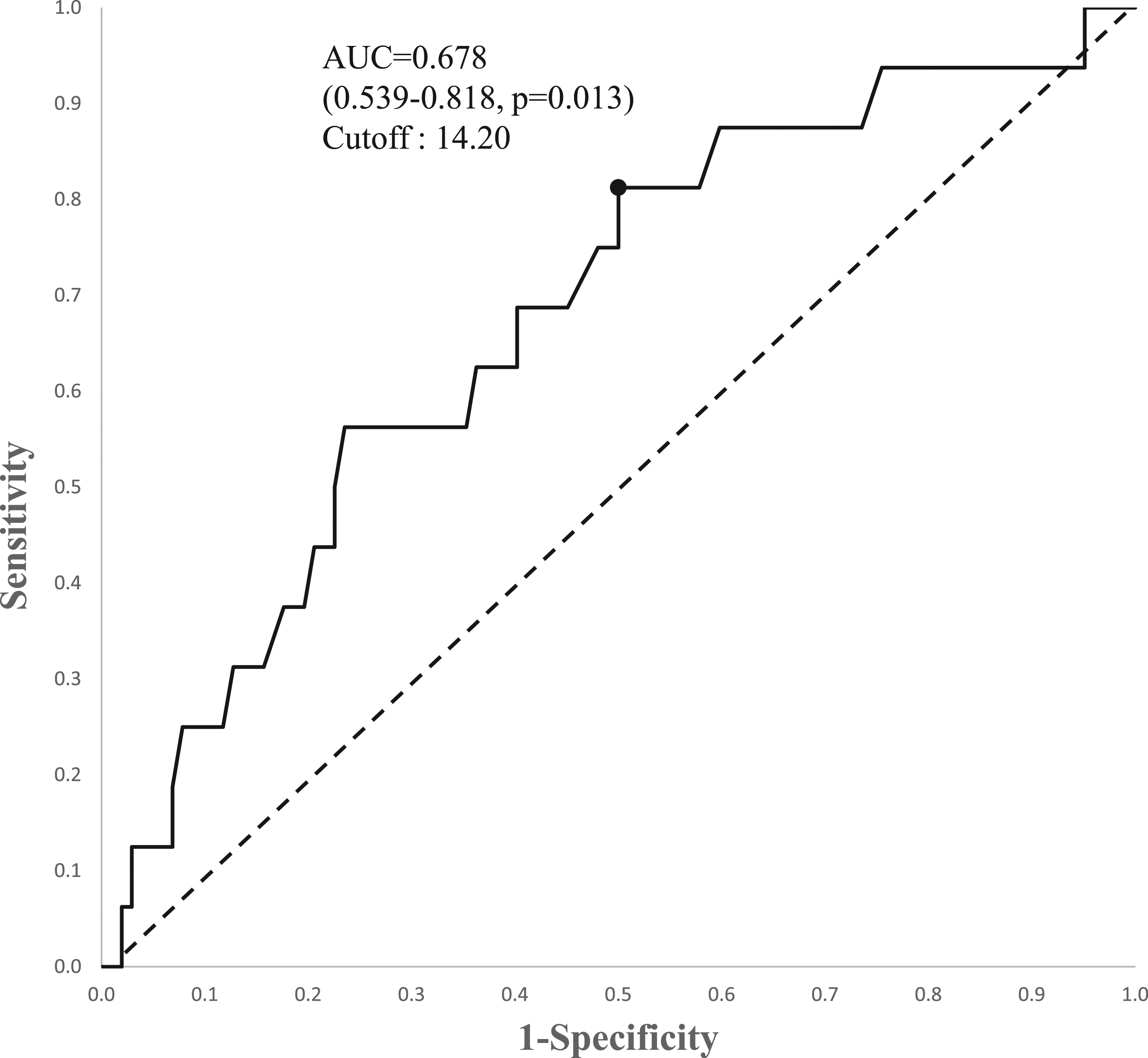
Post-Hoc Analysis
A post-hoc analysis was conducted by plotting the scatter diagram with the preoperative and postoperative ODI scores at 1 year after surgery on the 2 axes (Figure 2). Patients with HGS above the suggested cutoff value of 14.20 kg (Figure 1) were marked as filled dots, whereas those with HGS below the cutoff value were marked as empty dots. Three auxiliary lines were used to interpret the results. The bold horizontal line (“a”-line) represents the postoperative ODI score of 22; therefore, dots under the “a”-line represent those with favorable surgical outcomes. Twenty-two (19.1% of the total study population) patients were positioned under this line, and 18 patients had high HGS (27.3% of the high HGS group), whereas the remaining 4 patients had low HGS (8.2% of the low HGS group). A significantly larger proportion of patients in the high HGS group had a favorable outcome (P = .01). The straight diagonal line (“b”-line) represents those with the same x- and y-coordinates; therefore, those with improved ODI scores after surgery were marked below the “b”-line. The interrupted diagonal line (“c”-line) was drawn at 15 ODI score right to the “b”-line given that the minimum clinically important difference (MCID) of ODI score in patients with ASD is 15.
21
Therefore, dots under the “c”-line represent those with an ODI score improvement larger than that of the MCID after surgery. A total of 44 (38.3% of the total study population) patients met this criterion, of which 26 had high HGS (39.4% of the high HGS group), and 18 had low HGS (36.7% of the low HGS group). No significant differences were found between the proportions of patients with either high HGS or low HGS plotted under the “c”-line (P = .772). Post-hoc analysis comparing the preoperative and postoperative Oswestry disability index (ODI) scores using a scatter plot. “a”-line: ODI score of 22; “b”-line: postoperative ODI score same as preoperative ODI score; and “c”-line: improved postoperative ODI score by >15 points.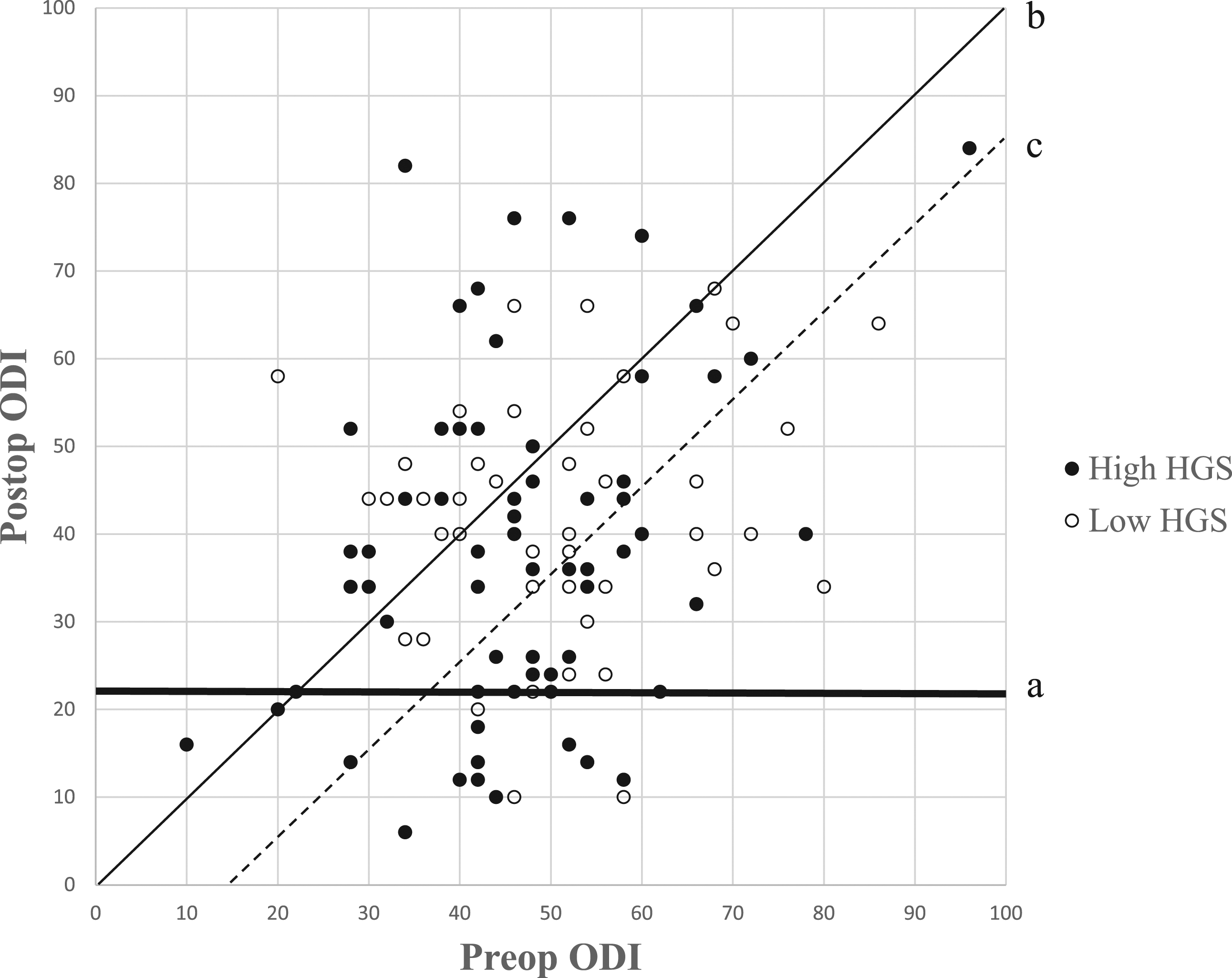
Medical and Surgical Complication Rates After Deformity Correction Displayed with Hand Grip Strength of Each Subgroups.
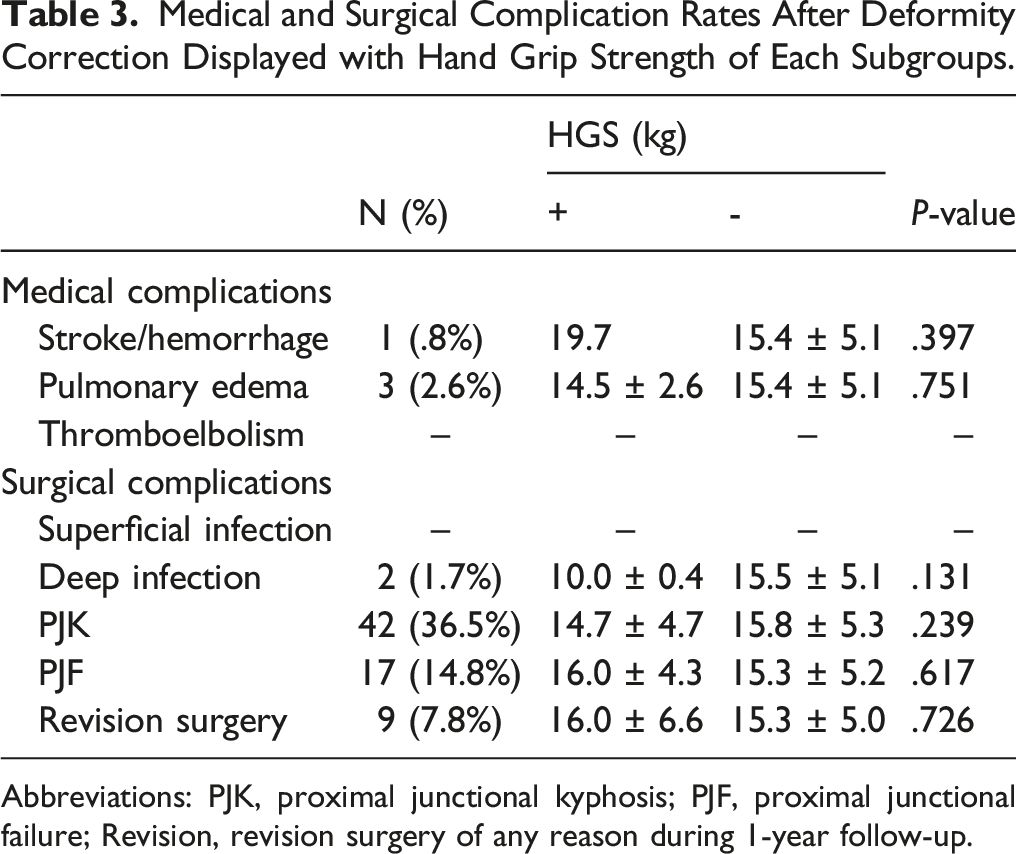
Abbreviations: PJK, proximal junctional kyphosis; PJF, proximal junctional failure; Revision, revision surgery of any reason during 1-year follow-up.
Discussion
Summary of Literature Advocating Grip Strength as Surgical Outcome Predictor.
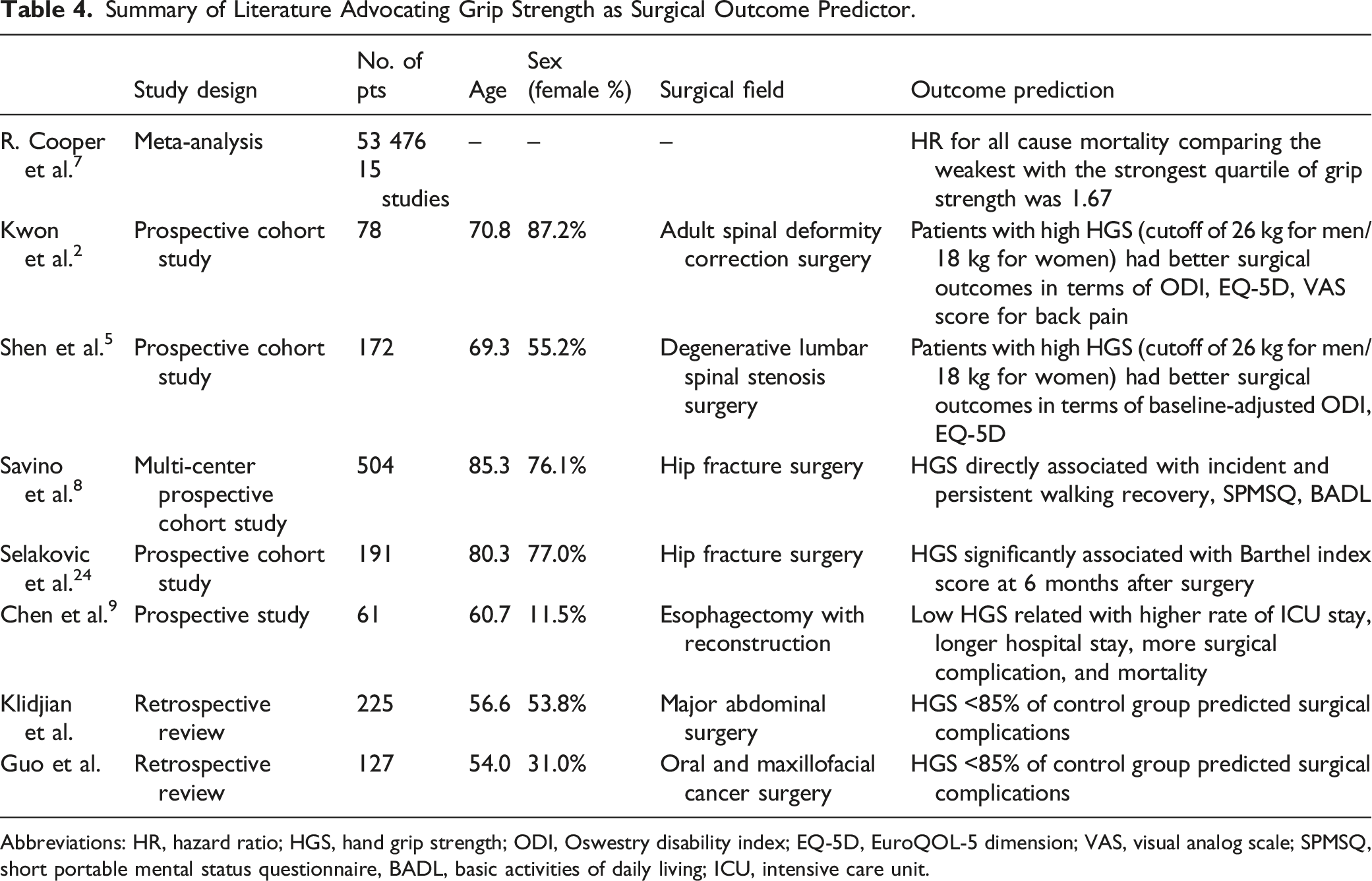
Abbreviations: HR, hazard ratio; HGS, hand grip strength; ODI, Oswestry disability index; EQ-5D, EuroQOL-5 dimension; VAS, visual analog scale; SPMSQ, short portable mental status questionnaire, BADL, basic activities of daily living; ICU, intensive care unit.
Hand grip strength is greatly influenced by patient population characteristics such as age, gender, and general medical condition.11,12 Therefore, a certain reference value is necessary for clinical application in a unique population of patients with ASD. The proposed HGS cutoff value (14.20 kg) in our study was lower than other known reference values used in the diagnosis of sarcopenia. The European Working Group on Sarcopenia in Older People first suggested a cutoff value of 20 kg for female patients in 2010 4 and changed it to 16 kg in their revised consensus in 2019. 13 The Asian Working Group for Sarcopenia set a cutoff value of 18 kg in 2014. 14 It is understandable because patients with ASD undergoing corrective surgery have a severe level of disability. A stooping posture resulting from back extensor muscle weakness and poor muscle coordination limits the daily activities of these patients. This lack of physical activity leads to a vicious cycle of muscle loss and accelerates the aging process. 23 Although data are not shown, we experimentally plotted other ROC curves by lowering the ODI cutoff value to 20 or 18 rather than 22 for favorable surgical outcomes. Then, the cutoff value of HGS to predict the respective level of postoperative ODI score increased to 16 or 18 kg. However, the number of patients meeting the stricter ODI score criteria decreased, diminishing its clinical usefulness.
The dichotomization of the surgical outcome was inevitable to plot an ROC curve and derive a cutoff value for HGS. We used an ODI reference value of “22 or less,” which was proposed by van Hooff et al, 19 indicating “achievement of an acceptable symptom state.” We categorized favorable or unfavorable surgical outcomes with this absolute value rather than a relative change, such as the MCID. The use of MCID has been suggested in the ODI scores of patients with ASD.21,24 Berven et al. 21 reported an MCID of 15 at the International Meeting for Advanced Spine Techniques, Scoliosis Research Society, 2005. Recently, Yoshida et al 24 proposed an MCID of 11. However, as per our experience, patients with ASD exhibit a wider range of preoperative ODI scores than those exhibited by patients with other disease entities, such as degenerative lumbar spinal stenosis or degenerative spondylolisthesis. 5 Thus, a certain amount of change in the ODI score may be sufficient for some patients but insufficient for others. In the post-hoc analysis (Figure 2), we found that the proportion of patients with high HGS was significantly higher in the patient group with ODI scores of 22 or less (below the “a”-line). In contrast, there was no such propensity; in the patients meeting the MCID of ODI score (below the “c”-line). From this point of view, the fact that only 20% of the present study population corresponded to “favorable outcome” suggests the need for further research on the absolute cutoff value of ODI in evaluating surgical outcomes in patients with ASD.
For proper interpretation of the current results, an aspect of the included patients’ characteristics must be considered. The current cohort includes elderly ASD patients with a mean age of 71.7 years. This is attributable to a narrow distribution of preoperative radiographic measures and symptom questionnaire scores compared to those of the HGS. Another critical point is that all surgeries were performed by a single surgeon at a single center. This resulted in relatively consistent values of postoperative PI–LL and postoperative SVA; in addition, there was no difference in postoperative radiographic parameters between the favorable and unfavorable outcomes. Therefore, a reasonable interpretation of the present study results would be that HGS could be a predictive factor of surgical outcomes only in case that a proper radiological goal was achieved after ASD surgery.
Other limitations: first, we confined the study subjects to female patients, and 39 males out of 180 screened patients (21.6%) were excluded. Similar to other reference values for HGS, the cutoff value for HGS in male patients with ASD should be suggested separately. However, due to female dominance in our ASD population, a larger sample size or multi-center study might be necessary. Second, some patients in the low HGS group had favorable surgical outcomes. These cases must be reviewed, as this can help achieve favorable surgical outcomes in this group.
In conclusion, the present study demonstrated that HGS is a predictor of favorable surgical outcomes in patients with ASD. A cutoff value of 14.20 kg can be used in patients with ASD to interpret the HGS as either high or low. Interpretation of the HGS with this cutoff value would aid in the shared decision-making process between the surgeon and the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.