
Abstract
Study Design:
Retrospective.
Purpose:
To evaluate the relationship between shoulder/ neck imbalance with distal adding-on phenomenon and to identify other risk factors in Lenke 1 and 2 (non-AR curves) adolescent idiopathic scoliosis (AIS) patients.
Methods:
100 Lenke 1 and 2 AIS patients with lowest instrumented vertebra (LIV) cephalad to or at L1 were recruited. Medial shoulder/ neck balance was represented by T1-tilt and cervical axis (CA). Lateral shoulder balance was represented by clavicle angle (Cla-A) and radiographic shoulder height (RSH). Distal adding-on phenomenon was diagnosed when there was disc wedging below LIV of >5o at final follow-up. Predictive factors and odds ratio were derived using univariate and multivariate logistic regression analysis.
Results:
Mean age of this cohort was 15.9 ± 4.4 years. Mean follow-up duration was 30.9 ± 9.6 months. Distal adding-on phenomenon occurred in 19 patients (19.0%). Only Risser grade, preoperative CA and final follow-up lumbar Cobb angle were the independent factors. A positive preoperative CA deviation increased the odds of distal adding-on by 5.4 times (95% CI 1.34-21.51, P = 0.018). The mean immediate postoperative T1-tilt, CA, RSH and Cla-A were comparable between the group with distal adding-on and the group without.
Conclusion:
Distal adding-on phenomenon occurred in 19.0% of patients. Preoperative “Cervical Axis” was an important factor and it increased the risk of distal adding-on by 5.4 times. Other significant predictive factors were Risser grade and lumbar Cobb angle at final follow-up. Immediate postoperative shoulder or neck imbalance was not a significant factor for postoperative distal adding-on phenomenon.
Keywords
Introduction
Distal adding-on phenomenon was among the common postoperative complications following posterior spinal fusion (PSF) in adolescent idiopathic scoliosis (AIS). Despite having various recommendations on the selection of lowest instrumented vertebra (LIV) in PSF for major thoracic curves, the incidence of adding-on phenomenon was still reported to be as high as 51.1%. 1 Many studies had investigated the factors in relation to this phenomenon. Selection of LIV proximal to the substantial touch vertebra (STV) 2-4 was one of the most crucial factors in addition to lower Risser grade 1-3,5-8 and younger age.1,7-9 Other related factors were open triradiate cartilage,5,10-12 lumbar C modifier curves, 5 preoperative LIV horizontal (LIV-H) angle, 13 preoperative LIV-H mismatch with lumbosacral takeoff (LSTO) angle, 13 fusion mass shift of more than 18 mm, 14 postoperative residual lumbar curve, 15 postoperative residual apical translation of main thoracic (MT) curve, 16 rotation of the lumbar vertebra 17 and flexibility of compensatory lumbar hemicurve. 10
In addition to the above factors, adding-on phenomenon was also believed to be a compensatory mechanism for postoperative shoulder imbalance (PSI).18,19 A multicenter study by Cao et al. reported that radiographic shoulder height (RSH) was positively correlated to change in angulation of first disc below LIV, and negatively correlated with the deviation change of LIV+1. However, the association was weak. 18 Lee and his colleagues noted the correlation between distal adding-on and PSI, but the relationship was not statistically significant. 19
Therefore, the aim of this study was to further elucidate the relationship between preoperative as well as immediate postoperative neck and shoulder balance with distal adding-on phenomenon at final follow-up and to identify the predictive factors related to it.
Methods
Study Design
This retrospective study was performed in a single academic institution from 2013 to 2016. All Lenke 1 and 2 AIS patients (non-AR) who underwent PSF with a minimum follow-up of 2 years were recruited. Lenke 1 and 2 curves were classified into AR/ AL depending on the tilt of the L4 vertebra as described by Miyanji et al. 20 Only patients with non-AR curves were included. In this cohort, the LIV chosen was at the last substantially touched vertebra (LSTV) by central sacral vertical line (CSVL). 7 Exclusion criteria were age <10 or >30, incomplete data, revision or anterior surgery and non-idiopathic scoliosis. The objectives of this study were 1) to evaluate the relationship between preoperative and immediate postoperative neck, medial shoulder and lateral shoulder imbalance with distal adding-on phenomenon at final follow-up, and 2) to determine the predictive factors associated with distal adding-on in those patients. Ethical approval was obtained from University Malaya Medical Centre Medical Ethic Committee (MREC ID NO: 2 018 119-6873) and patients’ consent was acquired for publication purpose.
Sample Size Calculation
Sample size was calculated using G*Power version 3.1.9.2 based on the systematic review and meta-analysis by Yang et al. 1 The primary outcome was prevalence of distal adding-on among AIS patients. Their study showed an overall 14.0% pooled prevalence of distal adding-on. Alpha (α) of 0.05 and power (1-β) of 0.80 were selected. The sample size calculated was 47. This study recruited 100 patients.
Definition
Below were the definitions of key radiographic parameters in this study: Distal adding-on phenomenon: An increase of >5° in the angulation of the first disc below the instrumentation and/or distalization of the end vertebrae.
7
Cervical axis (CA): An angle between the longitudinal axis of cervical spine (a line connecting the center of C2 odontoid process and center of C7 spinous process) with the vertical plane (in degree).
21
We classified it into positive (≥1°) and negative (≤0°). T1-tilt: An angle between the upper end-plate of T1 vertebra with the horizontal plane (in degree).
22
We classified it into positive (≥1°) and negative (≤0°). Clavicle angle (Cla-A): An angle (in degree) that is subtended between a horizontal reference line which is drawn perpendicular to the lateral edge of the radiograph and touches the most cephalad portion of the elevated clavicle and a line which touches the most cephalad aspect of both the right and left clavicle.
23
We classified it into positive (≥1°) and negative (≤0°). Radiographic shoulder height (RSH): The difference between the level of soft tissue shadow above the acromioclavicular joint at both ends and the horizontal line (in millimeters).
22
We classified it into positive (≥1°) and negative (≤0°).
Flexibility of curve:
Correction rate (CR) of curve:
Side bending correction index (SBCI):
Radiographic Measurements
Anteroposterior and lateral plain radiographs were taken preoperatively, immediate postoperatively and at final follow-up. For this study, we only measured the preoperative, immediate postoperative and final follow-up radiographs. Immediate postoperative radiographs were performed between 6 weeks to 3 months postoperative period. Preoperatively, supine side bending (SSB) radiographs were performed, incorporating the bending of the cervical spine (cervical supine side bending, CSSB radiographs) to assess the maximum flexibility of the proximal thoracic (PT). 24 Radiographic parameters that were analyzed were Risser grade, upper instrumented vertebra (UIV) level, LIV level, Cobb angle, T1-tilt angle, CA, Cla-A, RSH, UIV tilt angle, and first disc space tilt angle below LIV. The Cobb angle for PT, MT and lumbar (L) were measured in both standing and side bending films. The CR or correction index as well as flexibility were calculated using formulas shown above. All radiological measurements were done by a single surgeon using digital software (Centricity PACS, version 5.0, GE Healthcare, Chicago, IL, USA).
Surgical Strategy
All patients underwent PSF using pedicle screws and rods construct with alternate level pedicle screw placement. Correction maneuvers consisted of rod translation and direct vertebral derotation techniques. Radical facetectomies were performed to increase spinal flexibility prior to correction as well as to assist the fusion process. Autogenous bone graft obtained from the spinous processes, laminae, facet joints and transverse processes were processed and distributed over the fusion bed to augment the fusion process. LIV selected was the last substantially touched vertebrae by the CSVL.2-4,7 Therefore, level of LIV was not analyzed as a factor in this study. The UIV in Lenke 1 curves were T3, T4, or T5 when the right shoulder was high or when the shoulder was balanced. Fusion to T2 was performed when the left shoulder was high. In Lenke 2 curves, the UIV were T1 or T2 when the left shoulder was high and T3 when it was level or the right shoulder was high. The optimal UIV tilt angle was calculated from the CSSB radiographs preoperatively. 25
Statistical Analysis
Continuous variables were analyzed with independent sample t-test. Categorical variables were analyzed with Chi-squared test. Pearson correlation test was used to assess the relationship between immediate postoperative shoulder parameters with distal adding-on using surrogate parameter which was the first disc space tilt angle below LIV. Binary logistic regression analysis was used to establish the predictive factors related to distal adding-on phenomenon. The test involved both univariate and multivariate analyses. Variables selection were done based on the recommendation by Bursac et al. 25 Univariate logistic regression was performed for all variables initially. Variables with P < 0.25 and clinically relevant were selected for multivariate analysis. 26 The multivariate logistic regression was analyzed using backward selection method based on likelihood ratio. Odd ratios (OR) were calculated to illustrate the risk. OR ≥1 indicated the outcome event is more likely to happen and OR < 1 indicated the investigating factor is less likely to experience the outcome event. All data was analyzed using Statistical Package for the Social Sciences version 25 (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). P-value of less than 0.05 was considered statistically significant.
Results
The patients’ demographic profile was illustrated in Table 1. Majority of patients had Lenke 1 curves (75.0%). Preoperative radiological parameters that were noted to be statistically significant between the Lenke groups were; Cobb angle measured from PT, MT, L, PT SB, and MT SB. The mean T1-tilt in Lenke 1 was −3.3 ± 5.7° compared to 2.6 ± 5.5° in Lenke 2 (P < 0.001). Age, gender, Risser grade and follow-up duration were not statistically significant.
Demographic of patients (n = 100).
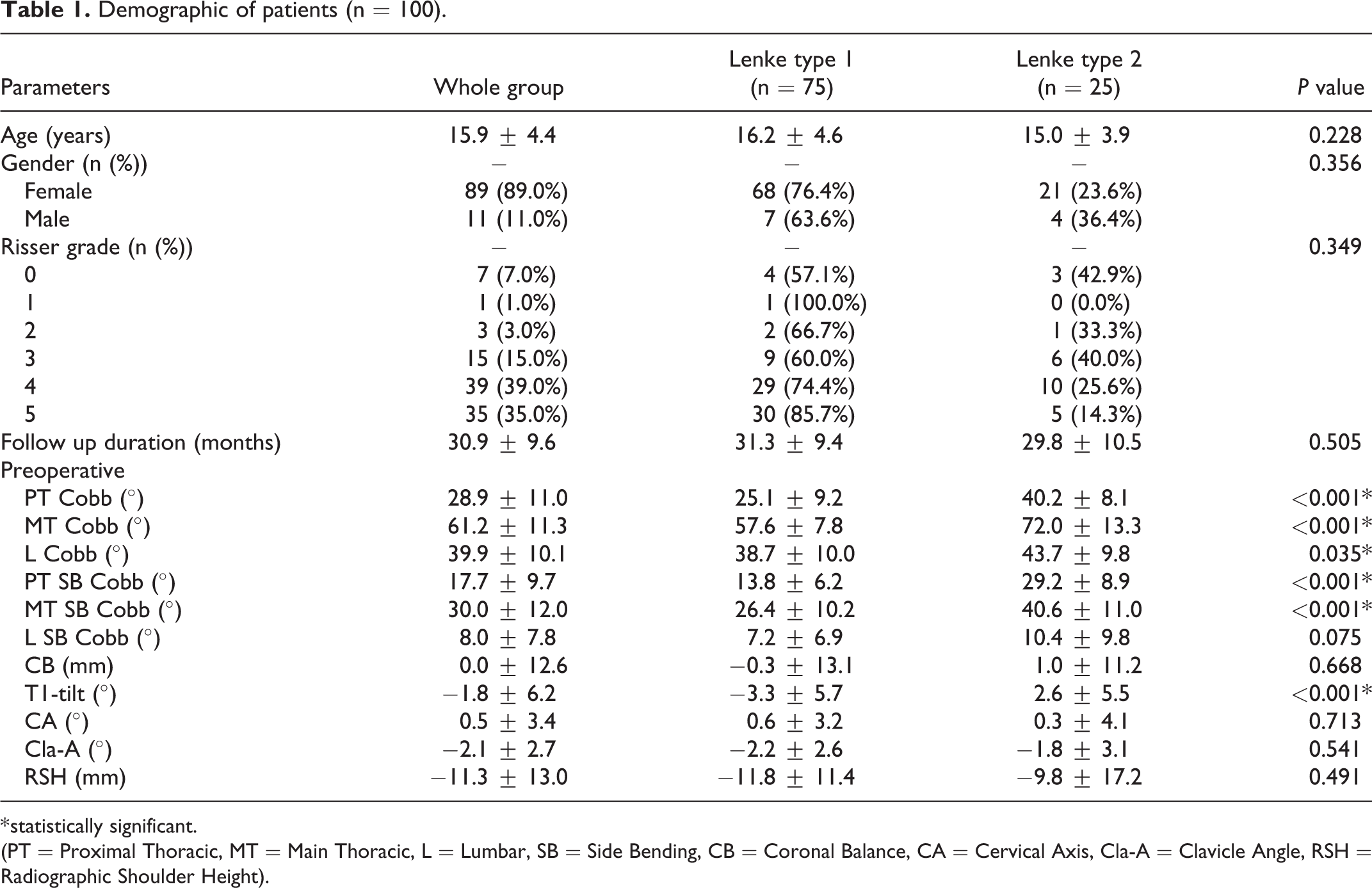
* statistically significant.
(PT = Proximal Thoracic, MT = Main Thoracic, L = Lumbar, SB = Side Bending, CB = Coronal Balance, CA = Cervical Axis, Cla-A = Clavicle Angle, RSH = Radiographic Shoulder Height).
Postoperative radiological parameters were illustrated in Table 2. PT Cobb, MT Cobb, L Cobb, T1-tilt, MT and L CR were statistically significant (P < 0.05). Lenke 2 had greater mean T1-tilt (5.5 ± 3.6°) than Lenke 1 with a significant P-value of 0.001. Both CA and Cla-A had greater mean value in Lenke 1 patients. There were no significant differences between Lenke 1 and 2 concerning PT CR, CA, Cla-A and RSH. The RSH was about the same between 2 groups of patients.
Postoperative Radiological Measurements of Patients (n = 100).
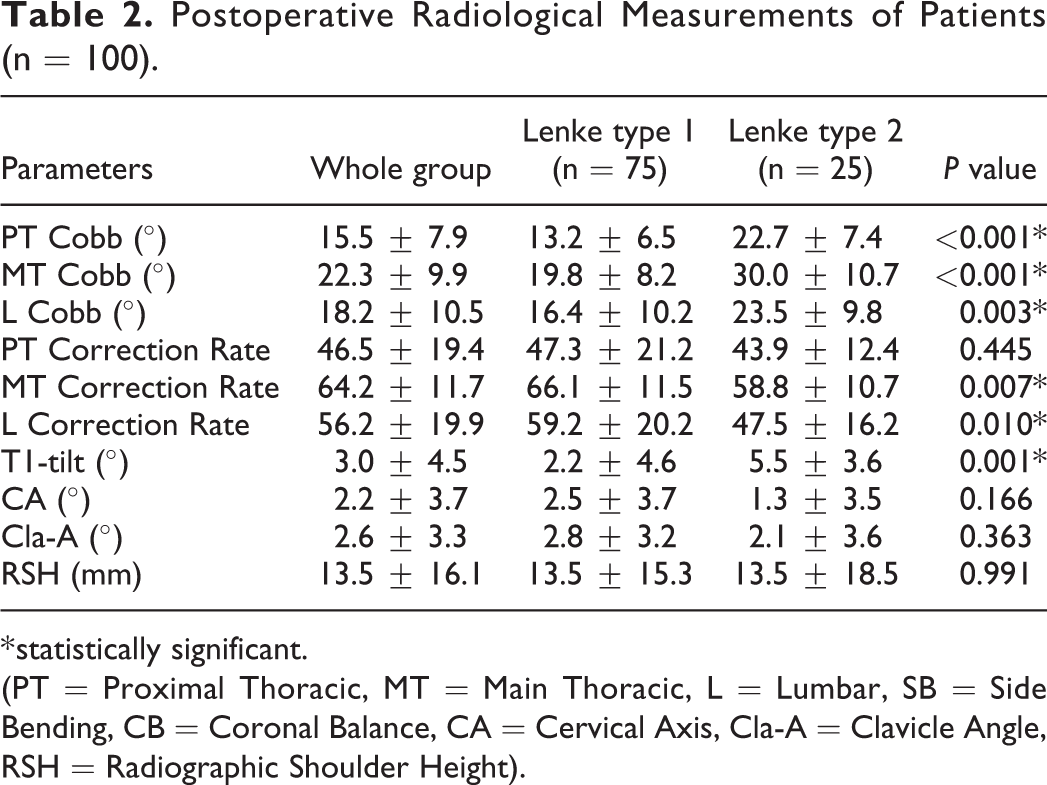
* statistically significant.
(PT = Proximal Thoracic, MT = Main Thoracic, L = Lumbar, SB = Side Bending, CB = Coronal Balance, CA = Cervical Axis, Cla-A = Clavicle Angle, RSH = Radiographic Shoulder Height).
Predictive Factors for Distal Adding-On Phenomenon
The results were summarized in Table 3. From the statistical analysis (as stated in methodology), Risser grade, preoperative CA and final follow-up lumbar Cobb angle were found to be the significant predictive factors for distal adding-on phenomenon. For every 1° increase in final follow-up lumbar Cobb angle, patients had only 0.9 times the odds of developing distal adding-on (OR 0.9, 95% CI 0.8-1.0, P = 0.004). Furthermore, our study concluded that the lower the Risser grade, the higher the OR of getting distal adding-on, as listed in Table 3. There were 45.1 times the odds of having distal adding-on if a patient had Risser 0 (OR 45.1, 95% CI 2.9-697.2, P = 0.006). Risser 1 had an odds ratio of 0 because we had only 1 patient in that group.
Logistic Regression for Predicted Factors of Distal Adding-On (n = 100).
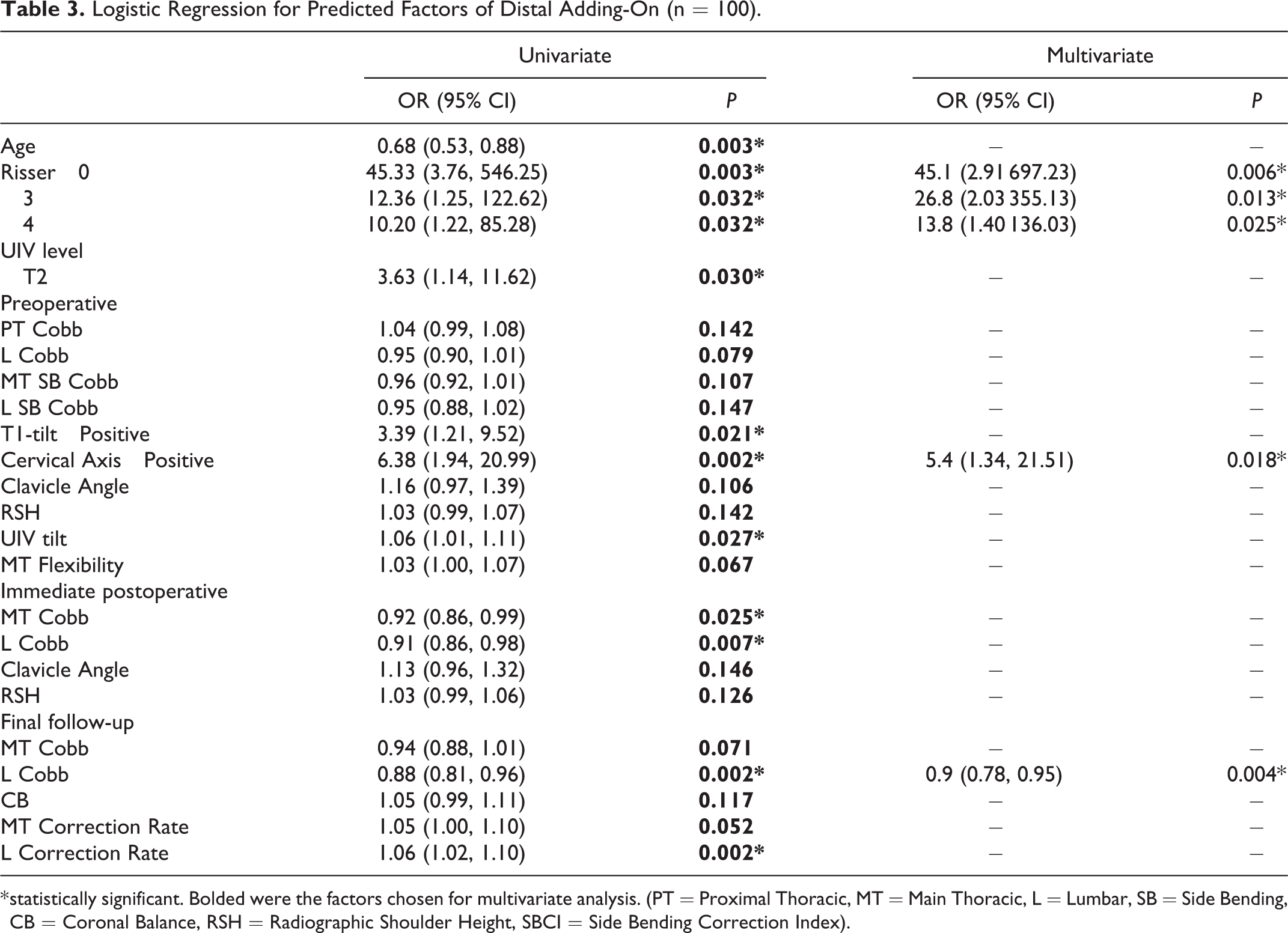
* statistically significant. Bolded were the factors chosen for multivariate analysis. (PT = Proximal Thoracic, MT = Main Thoracic, L = Lumbar, SB = Side Bending, CB = Coronal Balance, RSH = Radiographic Shoulder Height, SBCI = Side Bending Correction Index).
Distal Adding-on Phenomenon and Neck (CA), Medial Shoulder (T1-tilt) and Lateral Shoulder (RSH, Cla-A)
Preoperative parameters
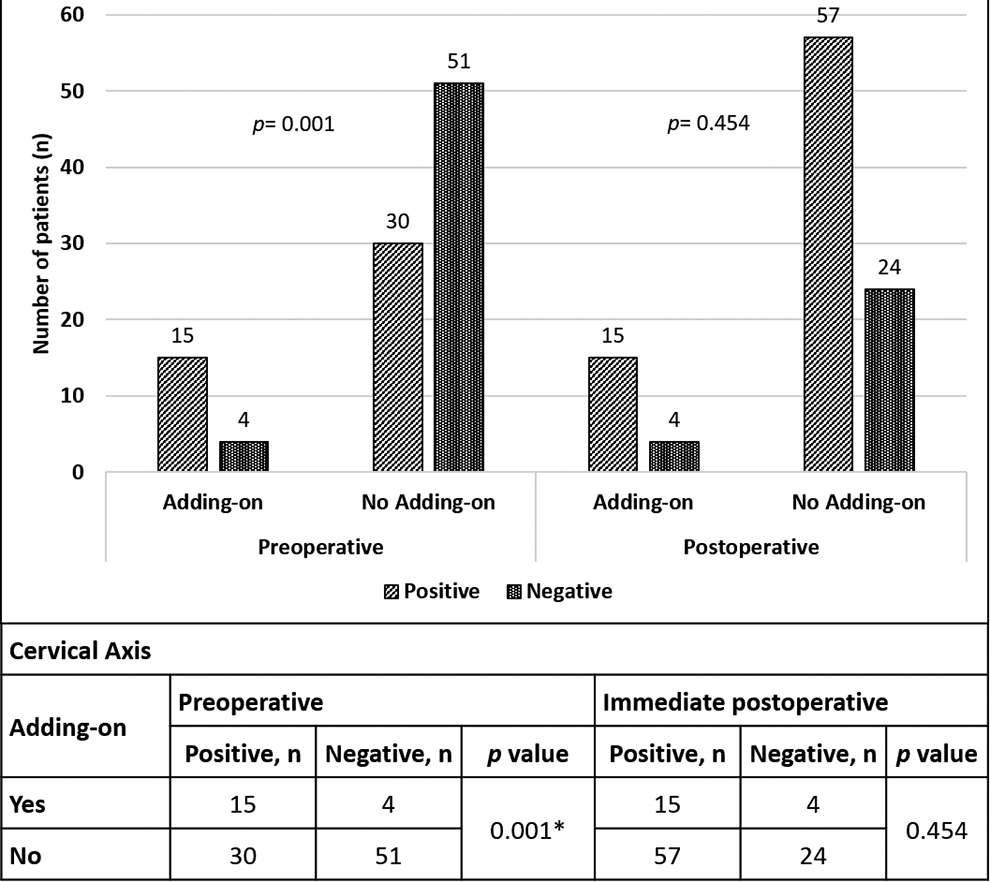
From the univariate and multivariate logistic regression analysis, preoperative CA was an independent factor that increased the risk of distal adding-on phenomenon. T1-tilt was found to be a significant factor only in univariate analysis. Cla-A and RSH were not significant factors. We noted that for every 1° increase in preoperative CA, the odds of getting distal adding-on increased by a factor of 5.4 if a patient had a positive value with reference to negative value (OR 5.4, 95% CI 1.3-21.5, P = 0.018). Two patients with CA deviation who developed adding-on phenomenon during follow-up is shown in Figure 1. Chi-squared analysis of preoperative CA further confirmed the association with distal adding-on phenomenon (Figure 2).
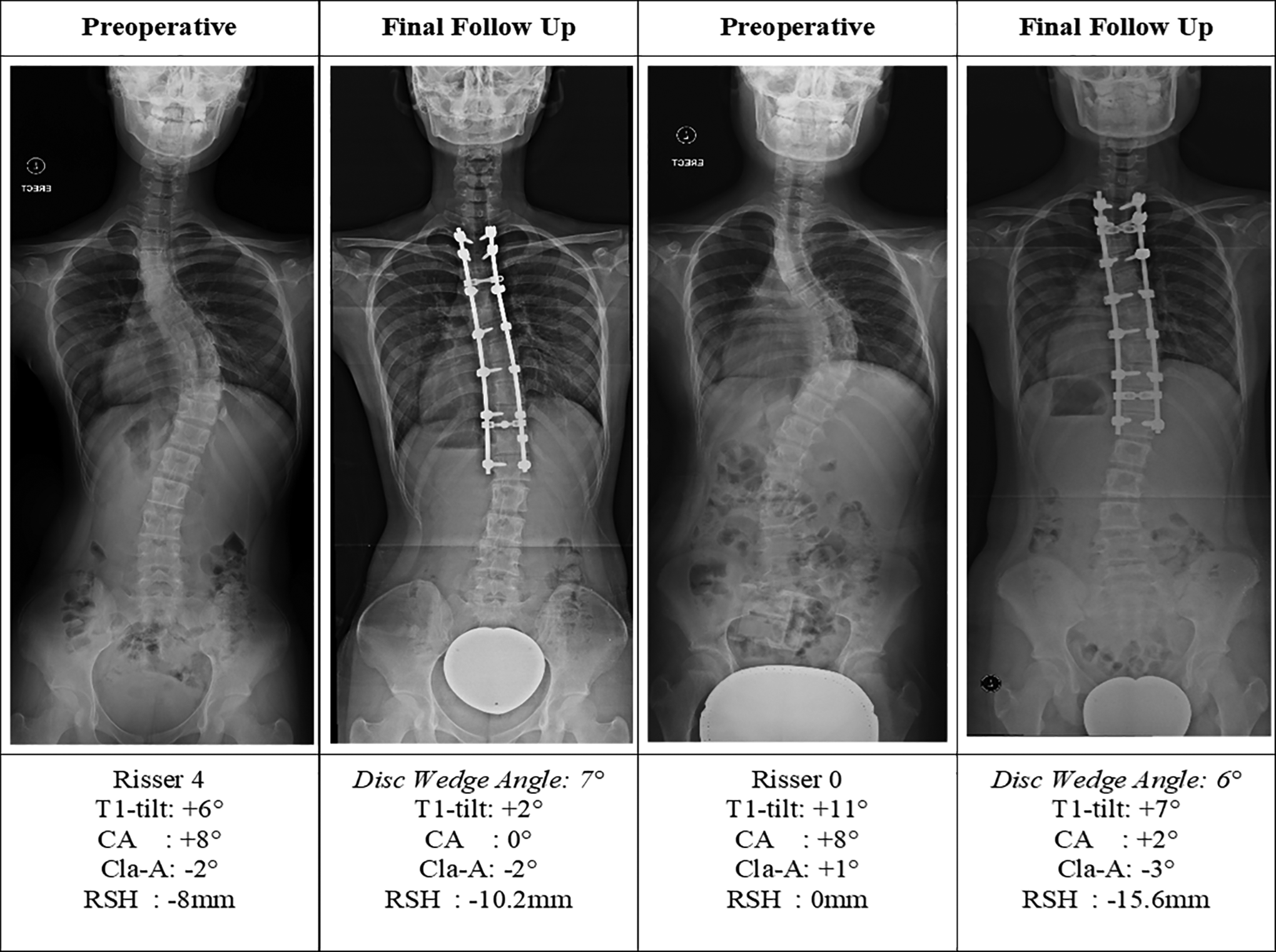
Case examples of 2 patients who had distal adding-on.
Schematic diagram on the postulation of how preoperative cervical axis deviation is associated with distal adding-on phenomenon.
Radiological shoulder parameters comparing patients with/without adding-on phenomenon
Preoperative T1-tilt and CA showed significant differences when comparing the 2 groups. The mean preoperative T1-tilt was 1.4 ± 6.7o and −2.6 ± 5.8 o for those with adding-on and those without (P = 0.010). The mean preoperative CA was 3.0 ± 3.0o and −0.1 ± 3.3o for both groups (P < 0.001). Radiological shoulder parameters measured in the immediate postoperative period and at final follow-up were comparable between both groups (Table 4).
Radiological Neck and Shoulder Parameters With and Without Distal Adding-On (n = 100).
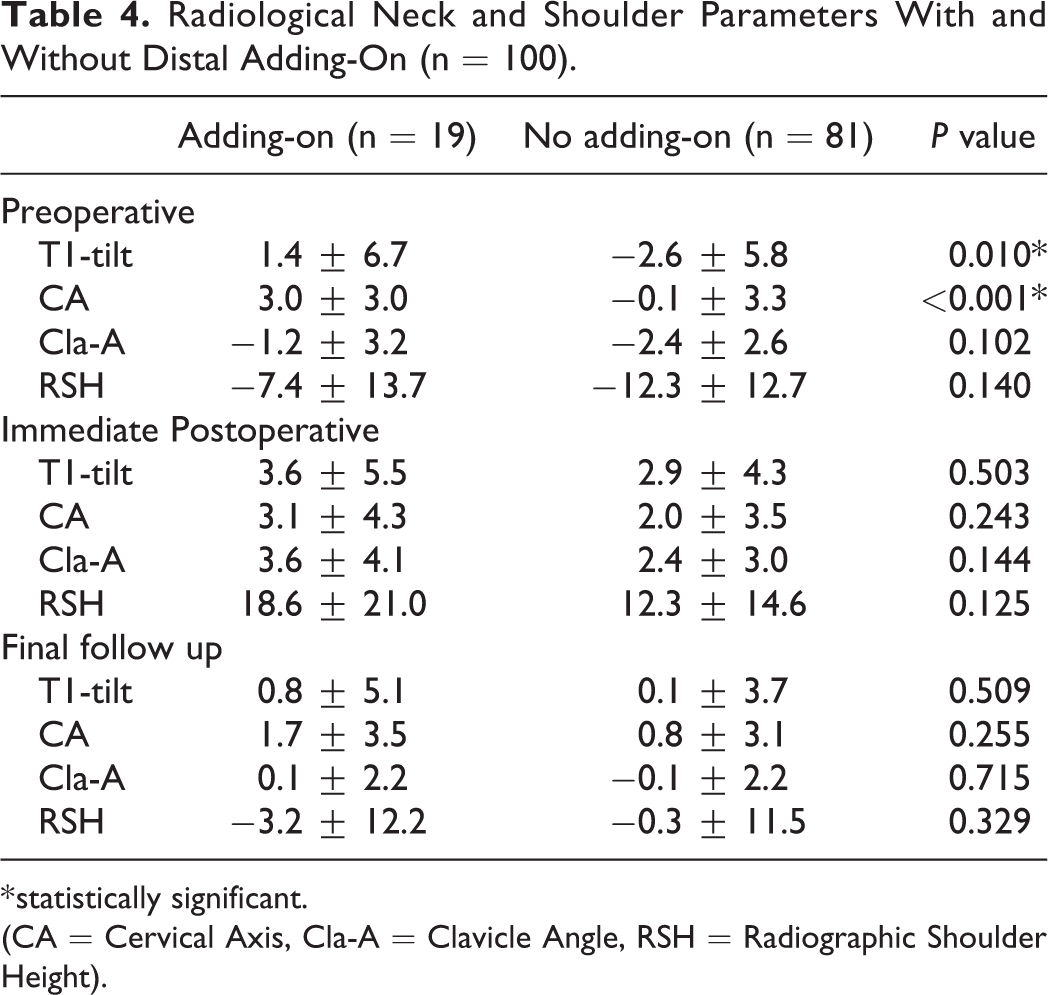
* statistically significant.
(CA = Cervical Axis, Cla-A = Clavicle Angle, RSH = Radiographic Shoulder Height).
Discussion
Distal adding-on phenomenon was postulated to have an association with PSI in many previous studies. Some authors postulated that adding-on phenomenon may compensate PSI as reported initially by Matsumoto et al. 27 Cao et al supported this proposed compensatory mechanism and revealed a weak association between adding-on and PSI. 18 Lee et al. found that distal adding-on could be related to PSI, but this association did not reach statistical significance. 19 Zhang et al noticed that distal adding-on had high occurrence among patients with PSI (OR 8.5, 95% CI 1.6-46.1). 28 Yang et al. also noted less shoulder imbalance in patients with adding-on. 1 Qin et al. reported that higher postoperative left shoulders increased the risk of adding-on progression. 29 Our study concluded that there was no significant association and differences between PSI and distal adding-on phenomenon (P > 0.05).
In this cohort, we had 19.0% patients (majority Lenke 1, non-AR) with distal adding-on. A few factors were known to increase the risk of distal adding-on phenomenon. First was AR curves. Cho et al. proved that by having an AR curve compared to AL curve had 2.2 times more risk of adding-on. 7 Another established factor was the selection of LIV. Distal fusion level proximal to the STV was proven to be one of the predictors of adding-on. In patients with fusion shorter than the last STV, the odds of distal adding-on increased by 3.6 (P = 0.01) as concluded by Murphy and colleagues. 3 Zang et al. also reported that LIV selection proximal to the last touched vertebra had higher incidence of distal adding-on. 30 Xu et al. classified the positional relationship between LIV and CSVL (Touch classification), which was categorized into A, the CSVL was located lateral to LIV pedicle; B, the CSVL touched the LIV pedicle; and C, the CSVL was located between both LIV pedicles. 31 The authors found that 58% of patients with Touch type A and 12% type B had adding-on phenomenon, while no adding-on was found in type C patients. As these factors were well proven, this study was designed specifically to analyze the predictive factors for distal adding-on in non-AR curve patients with selected LIV at the STV and located at L1 or more proximal.
After excluding the above factors, we found that the predictive factors of adding-on were skeletal maturity, preoperative CA and final follow-up lumbar Cobb angle. Skeletal maturity i.e. Risser grade was the established factor related to distal adding-on. It had been reported previously in literature.1-3,5-8 Our study echoed similar findings of which, lower Risser grade had higher OR of developing distal adding-on phenomenon. The association between lower Risser grade and adding-on phenomenon had been extensively reported as cited in our manuscript. The mechanism for this association had not been reported. Wang et al recommended that posterior spinal fusion is delayed in patients who were skeletally immature (Risser grade 3 or less) and these patients should undergo growing rod surgery while waiting for them to mature. 6 No mechanism on the association between skeletal immaturity/ younger age with adding-on phenomenon was proposed. Murphy et al also reported Risser 0 as a risk factor. Additional factors that were predictive of adding-on mechanism in their cohort was fusing short of LSTV and patients who were preoperatively balance in the coronal plane. The authors proposed under-correction of the main thoracic curves when the patients were skeletally immature. 3 Yang et al suggested that one of the reasons for younger patients to develop adding-on phenomenon was that surgeons had the tendency to opt for a shorter fusion to preserve motion. 1 However, in our cohort, younger age and lower Risser grade was still a significant independent factor despite all patients having their LIV at/more distal to LSTV.
Currently, no literature analyzed the association between neck balance with distal adding-on phenomenon. Interestingly, we found that patients with positive preoperative CA deviation was more likely to experience distal adding-on phenomenon. We postulated that CA deviation could lead to abnormal perception of horizontality in AIS patients. After surgery, we hypothesize that distal adding-on phenomenon could be a compensatory mechanism to restore perception of horizontality (Figure 3). Perception of horizontality could be related to either the patients’ vision or their vestibular system. Numerous studies discovered the association between the etiology of scoliosis and vestibular tone imbalance.32–34 Rousie et al reported that out of 445 patients with vestibular symptoms, 95 of whom had scoliosis. They also reported an abnormal direct connection between the posterior and lateral vestibular canal in 55% and 15% of patients with and without scoliosis, respectively. 34 Polak et al studied 23 boys and 48 girls with AIS and concluded that 60.0% of AIS patients had asymmetric skull positioning due to persistent muscle contracture. An asymmetric skull position combined with asymmetric neck muscle tone caused spinal compensation (scoliotic curve) to restore the natural horizontality of ears and labyrinths. This was because the horizontality of ears is essential for reflex equilibration. 33
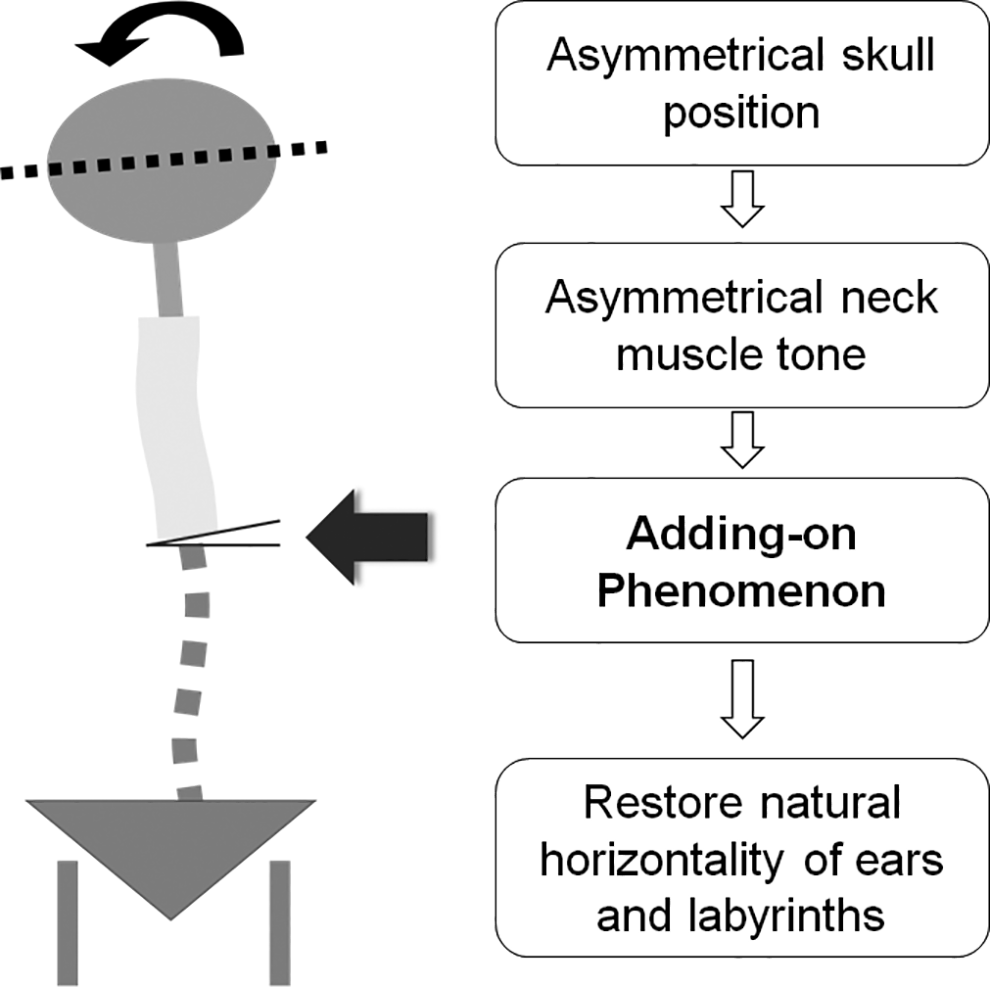
Association between cervical axis and distal adding-on.
Final follow-up lumbar Cobb angle was also found to be one of the significant predictive factors in our study. Our analysis showed that a lower lumbar Cobb angle during final follow-up increased the risk of getting distal adding-on. Over correction of the MT curve should therefore be avoided as this would lead to reciprocal correction of the lumbar curve. This was consistent with the findings reported in a study carried out by Qiu et al where they predicted that a more flexible lumbar hemicurve increased the risk of developing distal adding-on. 10 Yang et al further verified it because they discovered postoperative lumbar Cobb angle as a significant predictor for distal adding-on (OR 0.7, 95% CI 0.6-1.0, P = 0.020). 15
There were several limitations in our study. This was a retrospective study although the data used for analysis was collected prospectively. We analyzed radiographic parameters and not clinical parameters that reflected shoulder and neck balance. Distal adding-on phenomenon was a complication noted on postoperative radiographs. None of the patients with distal adding-on developed any clinical signs and symptoms. Therefore, none of the patients required any revision surgery. However, the long-term outcome of this phenomenon had not been established and is a subject for future study. The duration of follow-up might influence the occurrence of postoperative distal adding-on. A longer follow-up study may yield more patients with distal adding-on. Plain radiographs that were analyzed were taken at a single time point and may not reflect the patient’s actual or natural position throughout the day. All radiological parameters were measured by a single surgeon in which, measurement bias may be present. It would be more ideal if there were more raters to minimize measurement bias.
Conclusions
Distal adding-on phenomenon occurred in 19.0% of patients. Preoperative “Cervical Axis” deviation was an important factor and increased the risk of distal adding-on by 5.4 times. Other significant predictive factors were Risser grade and lumbar Cobb angle at final follow-up. Immediate postoperative shoulder or neck imbalance was not a significant factor for postoperative distal adding-on phenomenon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.