
Abstract
Study Design
Retrospective comparative study.
Objective
To compare patient-reported physical activity between anterior thoracic vertebral body tethering and posterior lumbar spine tethering (ATVBT/PLST) and posterior spinal instrumentation and fusion (PSIF) with minimum 2 year follow-up.
Methods
Consecutive skeletally immature patients with idiopathic scoliosis and a thoracic and lumbar curve magnitude ≥40° who underwent either ATVBT/PLST or PSIF from 2015-2019 were included. The primary outcome was rate of returning to sport. Secondary outcomes included ability to bend and satisfaction with sport performance as well as weeks until return to sport, school, physical education (PE) classes, and running.
Results
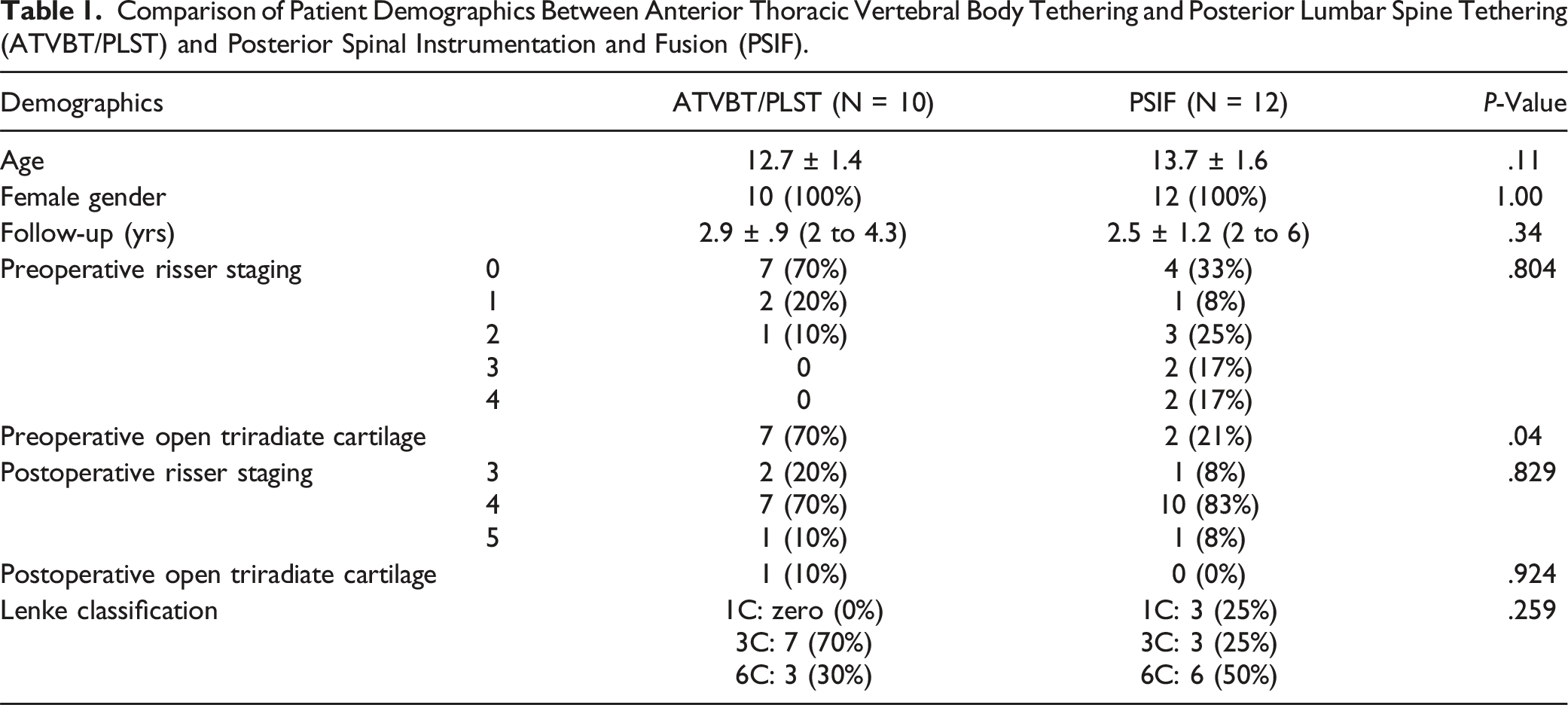
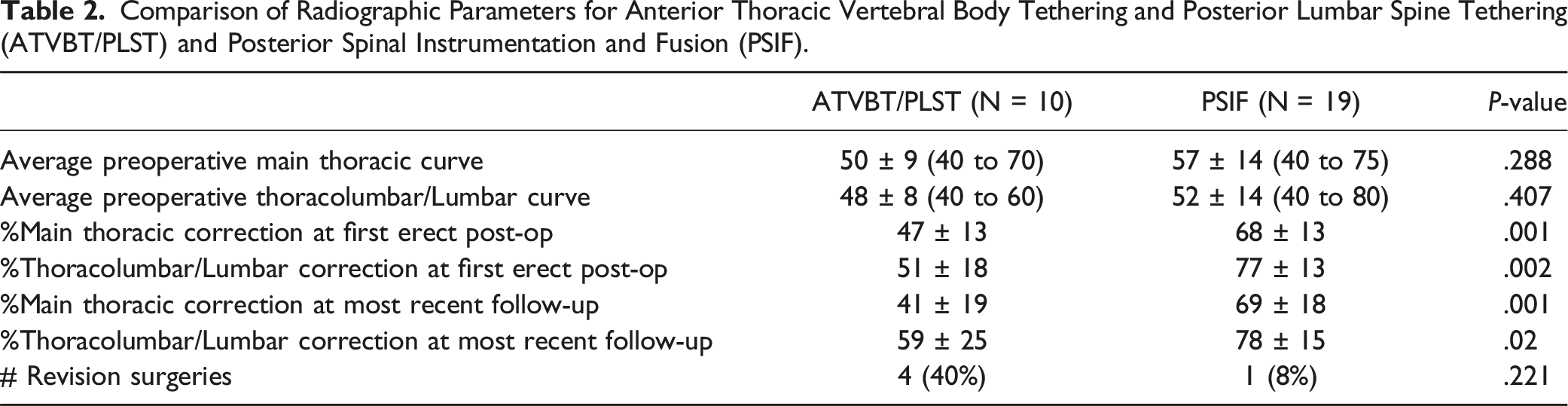
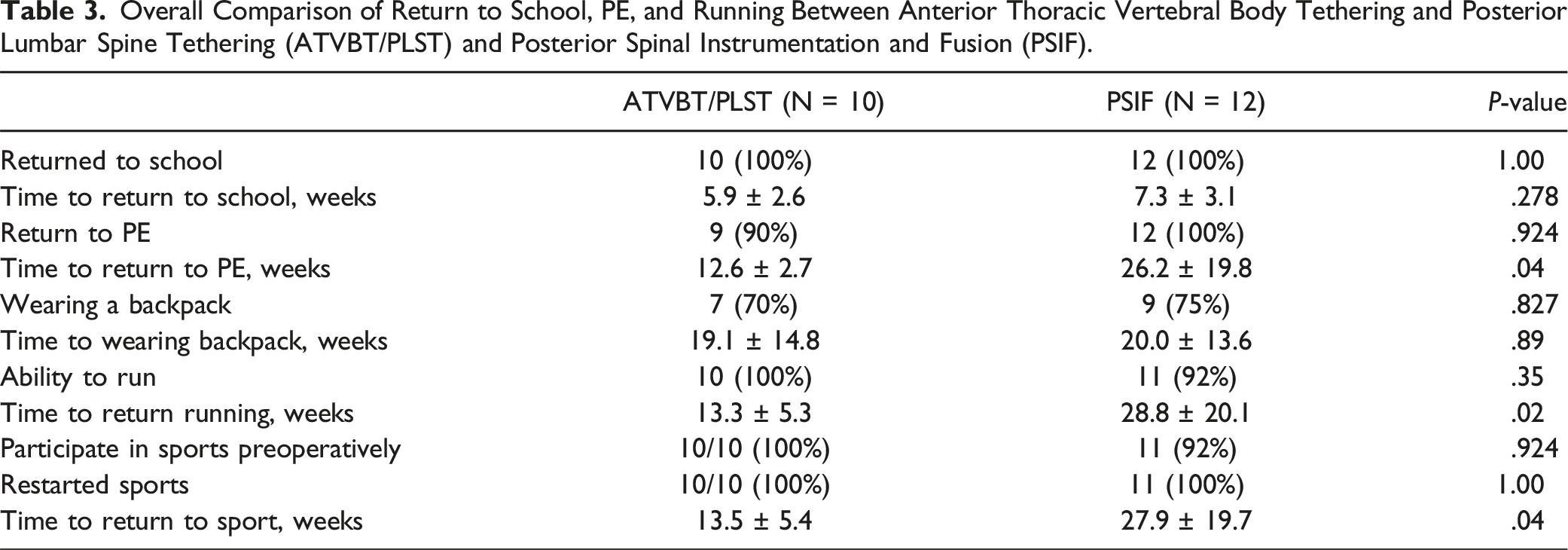
Ten patients underwent ATVBT/PLST and 12 underwent PSIF. ATVBT/PLST patients reported significantly faster return to sport (13.5 weeks vs 27.9 weeks, P = .04), running (13.3 weeks vs 28.8 weeks, P = .02), and PE class (12.6 weeks vs 26.2 weeks, P = .04) compared to PSIF patients. ATVBT/PLST patients reported that they had to give up activities due to their ability to bend at lower rates than PSIF patients while reporting “no changes” in their ability to bend after surgery at higher rates than PSIF patients (0% vs 4% giving up activities and 70% vs 0% reporting no changes in bending ability for ATVBT/PLST and PSIF, respectively, P = .01). Compared to PSIF patients, ATVBT/PLST patients experienced less main thoracic and thoracolumbar/lumbar curve correction at most recent follow-up (thoracic: 41 ± 19% vs 69 ± 18%, P = .001; thoracolumbar/lumbar: 59 ± 25% vs 78 ± 15%, P = .02). No significant differences in the number of revision surgeries were observed between ATVBT/PLST and PSIF patients (4 (40%) and 1 (8%) for ATVBT/PLST and PSIF, respectively, P = .221).
Conclusions
ATVBT/PLST patients reported significantly faster rates of returning to sport, running, and PE. In addition, ATVBT/PLST patients were less likely to have to give up activities due to bending ability after surgery and reported no changes in their ability to bend after surgery more frequently than PSIF patients. However, the overall rate of return to the same or higher level of sport participation was high amongst both groups, with no significant difference observed between ATVBT/PLST and PSIF patients.
Keywords
Introduction
Posterior spinal instrumentation and fusion (PSIF) has been the historic standard of care for the surgical treatment for pediatric patients with adolescent idiopathic scoliosis (AIS). Recently, however, vertebral body tethering (VBT) has emerged as an alternative strategy for the treatment of AIS that overcomes some of the long-term limitations of PSIF, which include loss of spinal mobility as well as restricted growth at the fused spinal levels.1-6 Prior reports documenting VBT as a non-fusion approach to AIS have focused primarily on patients with an isolated main thoracic curve.1,6-10 However, given their skeletal immaturity and growth potential remaining, VBT candidates are at risk for developing an additional thoracolumbar/lumbar curve11-15 or lumbar decompensation16,17 that may require further instrumentation in the lumbar spine. In these skeletally immature patients who are at risk for adding-on phenomenon or those already with additional thoracolumbar/lumbar structural curves, fusion of the lumbar spine has been the standard-of-care. Recently, anterior thoracic vertebral body tethering and posterior lumbar spine tethering (ATVBT/PLST) has been proposed as a novel treatment strategy for skeletally immature patients with both thoracic and lumbar scoliosis as well as skeletally immature patients at risk for adding-on phenomenon. 18 By preserving lordosis and flexibility of the lumbar spine, posterior lumbar tethering allows for growth modulation and spinal mobility that is constrained during fusion.1-5,8 In a single case series of 14 patients treated with ATVBT/PLST with minimum 2 year follow-up, ATVBT/PLST was associated with a high rate of clinical success (defined as ≤ 35-degree correction of both main thoracic and lumbar curves without requiring PSIF) in patients who reached skeletal maturity at most-recent follow-up. 18
A critical concern of adolescents and parents of adolescents undergoing spine surgery surrounds the child’s ability to return to sport and activity following the procedure. Given the increasing prevalence of childhood obesity worldwide and the well-documented deleterious effects of an increased body mass index (BMI) on outcomes after surgical correction of AIS,19-22 return to sport and activity following treatment options for AIS are important outcome metrics to consider when conducting a shared decision-making discussion with patients and their families. It is thought that modifications to a growing patient’s flexibility and range of motion may affect their ability to return to activity and sport. While several studies have reported return to sport rates after PSIF,23-26 only 1 study has evaluated return to sport after VBT, 27 and no studies have analyzed return to sport after combined TAPLT. Although the 1 analysis of return to sport after VBT looked at outcomes after anterior vertebral body tethering only and lacked a fusion group for comparison, the authors reported that the majority of patients returned to their preoperative activities and sports within 3 months of surgery. 27
The purpose of this study is to compare the rate and timing of return to sport and activity in patients undergoing ATVBT/PLST vs PSIF in children with AIS.
Materials and Methods
This retrospective cohort study was conducted at a single academic tertiary medical center which included consecutive cases from a single surgeon. All skeletally immature patients between the ages of 10 and 15 years with AIS who underwent either ATVBT/PLST or PSIF between the years 2015 and 2019 were included. Additional inclusion criteria were main thoracic curve and lumbar curve ≥40°, combined VBT and LPT, and a minimum of 2-year’ follow-up. Patients with Lenke 1C lumbar curves ≥40° standing but ≤25° bending were instrumented if there was concern for distal adding on phenomenon. Patients with prior spinal surgery, neuromuscular or syndromic scoliosis, or a history of infection, tumor, or trauma were excluded. Our Institutional Review Board (University of California, San Francisco Human Research Protection Program Institutional Review Board, #21-35847) approved the study, and informed consent was obtained from all patients and their parents if under the age of 18.
Patient demographics included age at the index operation, sex, height, weight, body-mass index (BMI), curve magnitudes, Risser grade, triradiate cartilage status, and Lenke classification. Radiographic data were evaluated preoperatively, as well as at the first, second year and most recent postoperative visits. We measured curve magnitude according to Cobb. 28
A questionnaire was designed to assess physical activity after surgery, including return to school, physical education, and sports. Return to sport, in particular, was chosen as a primary outcome due to the high importance of athletics in the lives of many middle and high school-aged patients. In addition, returning to sport is often an important concern for patients’ families, with over half of all children aged 6 to 17 reported to participate in organized sports. 29 Patients were enrolled by telephone and/or email; consent was provided by parent or guardian. Patients were contacted at minimum 2 years postoperatively. The questionnaire included questions on preoperative sports participation, return to sports, PE classes, running, and wearing a backpack, as well as satisfaction with sports performance, bending maneuvers, appearance, and surgical experience. Sports were classified as according to the American Academy of Pediatrics (AAP). Sport activities were classified as defined by the American Academy of Pediatrics (AAP). 30 Limited contact and noncontact sports were grouped together.
Statistical analyses were performed using R software (The R Foundation v4.0.2 and RStudio v.1.3.1093; Vienna, Austria). The threshold of statistical significance was set at α = .05. For continuous variables, Welch’st test was used, and for categorical variables, Pearson’s chi square test or Fisher’s exact test was used. Comparisons of quantitative continuous variables were performed using dependent t-tests. Kaplan-Meier curves were constructed where applicable.
Surgical Technique
All ATVBT/PLST and PSIF procedures were completed by the senior author (M.D.) at a single academic institution. PSIF was performed with pedicle screw anchors (Stryker). ATVBT/PLST was performed as described in a previous study. 18 Postoperatively, all patients were initially advised to limit activities and sport, and these limitations were liberalized as per the senior author’s standard of care. ATVBT/PLST patients had no restrictions beginning at 3 months postoperatively, and PSIF patients had no restrictions at 6 months.
Results
Patient Demographics
Comparison of Patient Demographics Between Anterior Thoracic Vertebral Body Tethering and Posterior Lumbar Spine Tethering (ATVBT/PLST) and Posterior Spinal Instrumentation and Fusion (PSIF).
Radiographic Data
Comparison of Radiographic Parameters for Anterior Thoracic Vertebral Body Tethering and Posterior Lumbar Spine Tethering (ATVBT/PLST) and Posterior Spinal Instrumentation and Fusion (PSIF).
Complications
Four (40%) ATVBT/PLST patients required revision surgery. Two patients underwent revision surgery for lumbar overcorrection. A third patient underwent revision surgery for an unstable L4 set screw. Finally, a fourth patient underwent cable replacement due to cable breakage.
Among PSIF patients, 1 patient (8%) required revision surgery for anterior spinal fusion. However, the difference in the number of revision surgeries between groups did not reach statistical significance (P = .221).
Return to School and Activities
Overall Comparison of Return to School, PE, and Running Between Anterior Thoracic Vertebral Body Tethering and Posterior Lumbar Spine Tethering (ATVBT/PLST) and Posterior Spinal Instrumentation and Fusion (PSIF).
Return to Sport
Preoperative sport participation was high in both groups, with no significant differences (100% ATVBT/PLST vs 92% PSIF, P = .924).
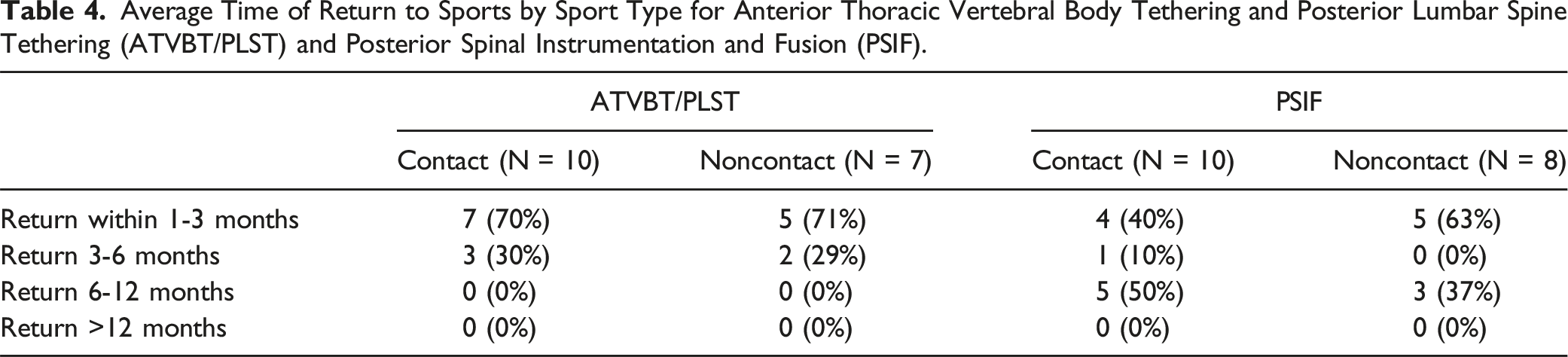
Average Time of Return to Sports by Sport Type for Anterior Thoracic Vertebral Body Tethering and Posterior Lumbar Spine Tethering (ATVBT/PLST) and Posterior Spinal Instrumentation and Fusion (PSIF).
Sport Level, Performance, and Satisfaction
Level, Performance, and Satisfaction in Sport following Surgery Between Anterior Thoracic Vertebral Body Tethering and Posterior Lumbar Spine Tethering (ATVBT/PLST) and Posterior Spinal Instrumentation and Fusion (PSIF).
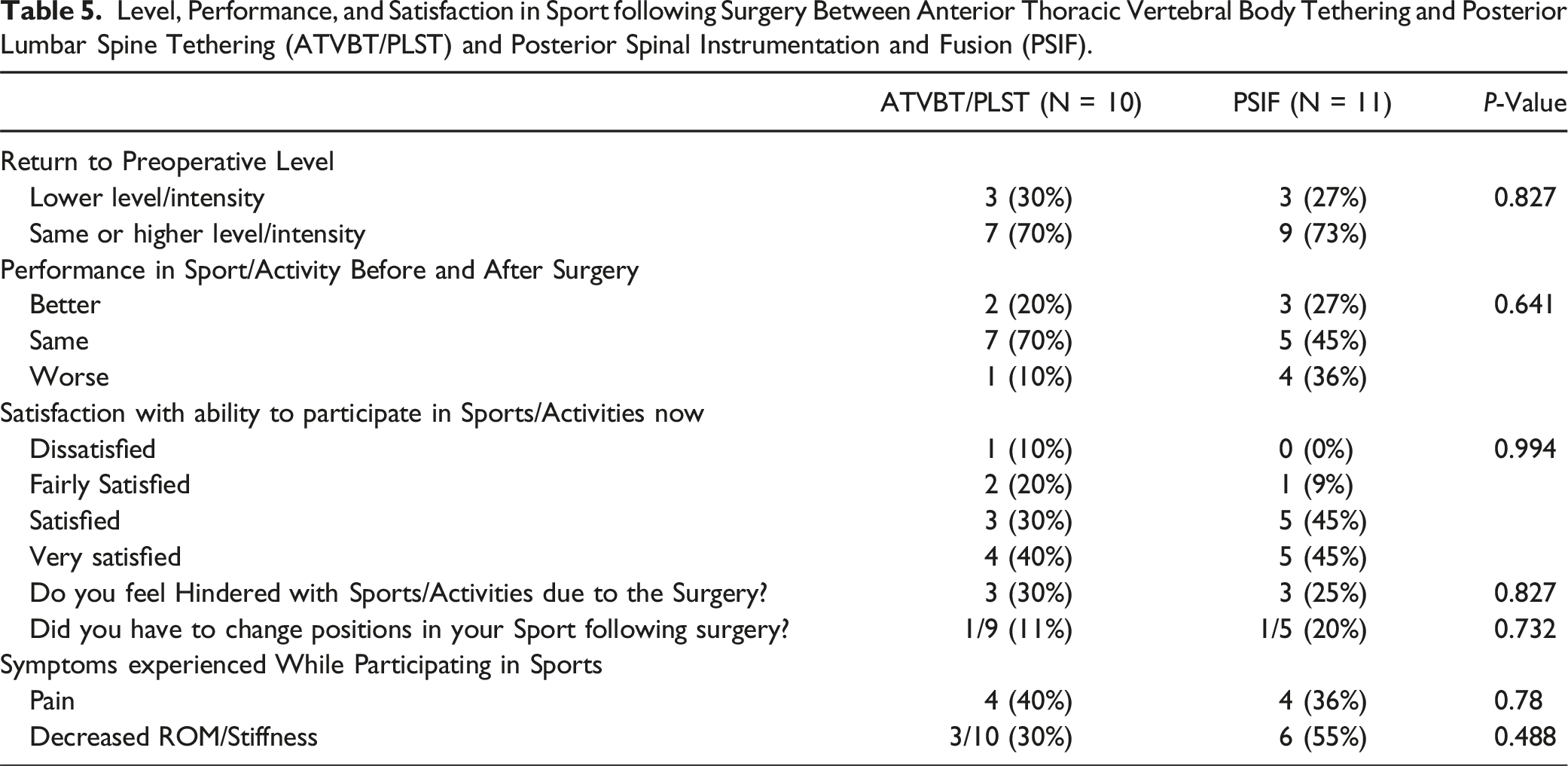
Patients who underwent ATVBT/PLST and PSIF felt hindered due to the surgery at similar rates (30% vs 25%, P = .827). Among symptoms experienced while playing sports, 40% in the ATVBT/PLST group reported pain compared to 36% in the PSIF group (P = .78). Patients who underwent ATVBT/PLST reported decreased ROM or stiffness while participating in sports at a rate of 30%, while those who underwent PSIF reported decreased ROM or stiffness during sports at a rate of 55% (P = .488).
Subjective Experiences following Surgery
Subjective Experience following Surgery for Anterior Thoracic Vertebral Body Tethering and Posterior Lumbar Spine Tethering (ATVBT/PLST) and Posterior Spinal Instrumentation and Fusion (PSIF).
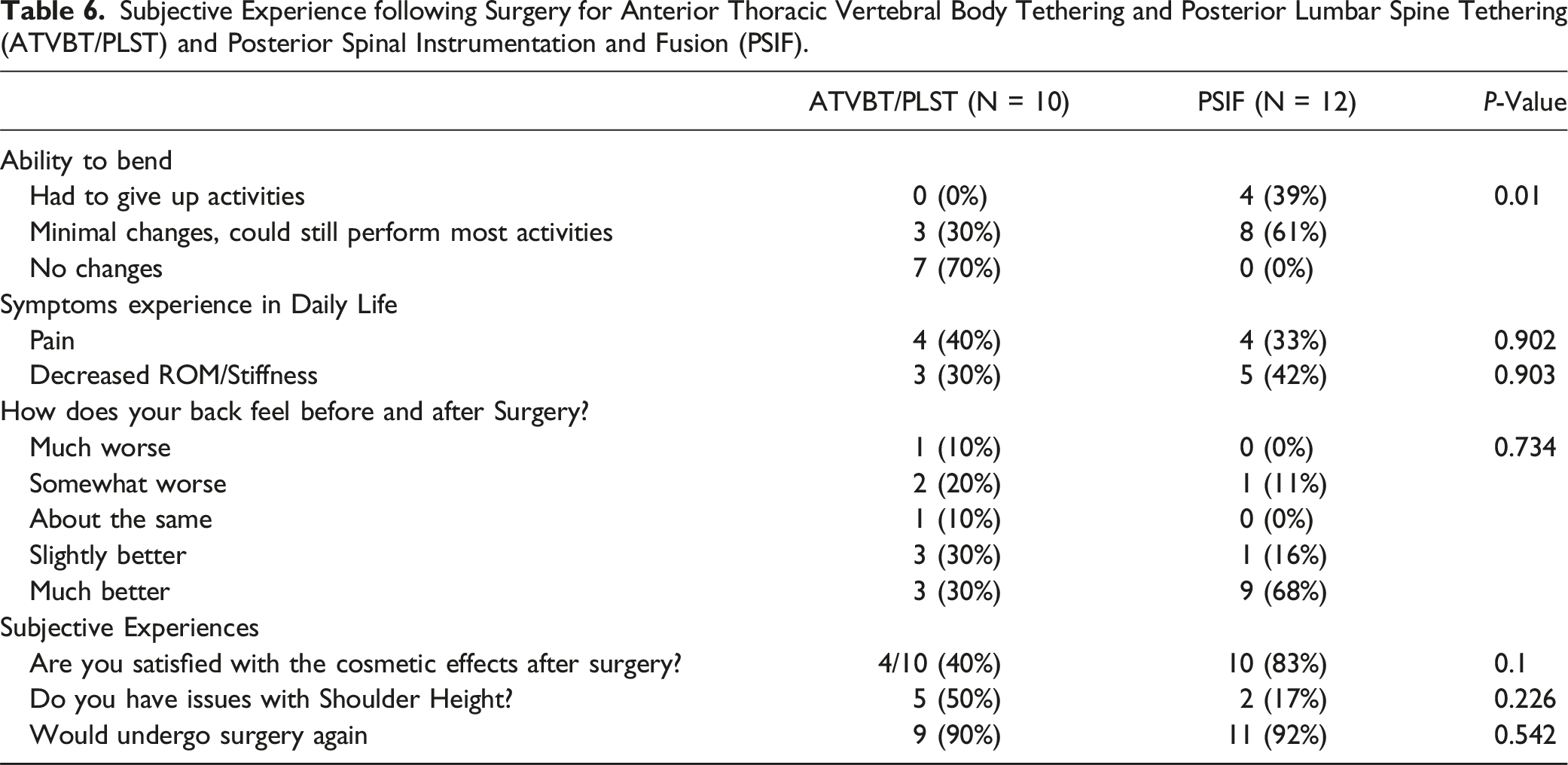
There were lower rates of cosmetic satisfaction among the ATVBT/PLST cohort than the PSIF cohort, although this difference did not reach statistical significance (40% vs 84%, P = .1). Issues with shoulder height were more common in the ATVBT/PLST group than in the PSIF group, although again, this difference did not reach statistical significance (50% ATVBT/PLST vs 17% PSIF, P = .226). Lastly, patients in the ATVBT/PLST group and PSIF group reported that they would undergo the surgery again at similar rates (90% ATVBT/PLST vs 92% PSIF, P = .542).
Body Mass Index (BMI)
Mean preoperative BMIs for ATVBT/PLST and PSIF patients were 18.7 ± 1.6 and 20.9 ± 4.8, respectively, while mean postoperative BMIs for ATVBT/PLST and PSIF patients were 21.0 ± 1.7 and 23.0 ± 5.3, respectively.
Discussion
The primary finding of this study was that skeletally immature patients undergoing ATVBT/PLST returned to sport and activity at significantly faster rates and were more flexible compared to PSIF patients. In contrast to patients undergoing PSIF who took approximately 8 months to return to sport, patients undergoing ATVBT/PLST returned to sport in approximately 3 months. Both groups ultimately reported high rates of returning to the same or higher level or intensity of sport participation when compared to their preoperative levels.
Among surgical options for AIS, those that utilize VBT are unique in that they do not disrupt the 3 spine columns of Denis 31 ’s three-column spine concept for spinal stability. In other words, while spine fusion requires implants or the formation of new bony structures to maintain spinal stability following surgery, tethering options do not. Thus, anatomical or biomechanical concerns after ATVBT/PLST are, in theory, substantially less than those after PSIF. Because PSIF does cause disruption to the spinal columns and stability, more precaution and time to return to sport and activity is warranted. This concept was previously proposed by Baroncini et al 27 in their report of return to sport after VBT in a case-series of 31 patients. The hypothesis was supported by a lack of any observed cases of screw loosening or other adverse events at the bone-implant interface such as vertebral fracture. Importantly, however, 1 ATVBT/PLST patient in our study required revision for an unstable L4 set screw, suggesting that further research involving the relationship between early return to sport and complications at the bone-implant interface is needed.
Of the 10 patients who underwent ATVBT/PLST, 1 patient required revision surgery due to cable breakage. Given the relative infancy of VPT for AIS, the relationship between an early return to sport and cable breakage remains unclear. The single prior study that analyzed return to sport after VBT found that 14 of 31 patients experienced cable breakage. 27 However, none of these patients required revision surgery for loss of correction and no ruptures were observed at the 3-month follow-up, the time by which most patients had resumed their sport. Additionally, no association was found between cable breakage and any of the items of their questionnaire, which the authors argued supports the hypothesis that an early return to sport does not affect risk for cable breakage. 27 Nevertheless, given the small sample size sizes of both studies, further research is needed to investigate the relationship between early return to sport and risk for cable breakage.
Given the increasing prevalence of childhood obesity worldwide and the well-documented deleterious effects of an increased BMI on outcomes after surgical correction of AIS,19-22 return to sport and activity following treatment options for AIS are important outcome metrics to consider when conducting a shared decision-making discussion with patients and their families. While, on average, patients in our study had BMIs within the healthy range, an increase in BMI was observed for both cohorts, pre to postoperatively. In addition, PSIF patients had postoperative BMIs that were on the high end of the normal range, indicating that they could be at risk for obesity if postoperative weight gain continues. Our results suggest that patients undergoing ATVBT/PLST are able to return to sport and activity at significantly faster timeframes than patients undergoing PSIF. Furthermore, ATVBT/PLST patients reported having to give up prior activities due to their ability to bend at a significantly lower rate than did PSIF patients. While an analysis of the effect of an earlier return to sport and activity on BMI was not performed in the present study, it is possible that patients able to return to sport faster than patients with longer return to sport timelines are at decreased risk of weight and adipose tissue accumulation due to the period of inactivity. When considering the negative effects of obesity on outcomes after surgery for AIS,19,20 it is important to note that the faster return to sport allotted by ATVBT/PLST may have implications for complications and outcomes in AIS patients by allowing exercise and physical activity earlier than after PSIF. In addition, by retaining their ability to bend, ATVBT/PLST patients did not have to give up activities they were used to performing, which may also have an impact on postoperative weight gain, as patients may be more likely to exercise if able to perform activities they previously enjoyed and in which they had more experience. However, more data with longer-term follow-up is needed to evaluate this hypothesis.
The effect of lumbar spine instrumentation on return to sport rates remains somewhat controversial.23,25,26,30 Multiple prior studies have suggested detrimental effects of lumbar instrumentation on outcomes regarding sport participation after surgery for AIS, including delays in return to sport and limitations in athletic performance after fusion.23,30 On the other hand, reports have also documented a lack of association between instrumentation of the lumbar spine and return to sport outcomes.25,26 Our study found that 100% of patients in both ATVBT/PLST and PSIF groups, which both consisted entirely of patients with both main thoracic and thoracolumbar/lumbar corrections performed, were able to return to sport. Furthermore, 70% or greater of each cohort reported returning to the same or higher level/intensity of sport when compared to their preoperative level/intensity. As a result, our study adds to the body of evidence that suggests that correction of thoracolumbar/lumbar curves does not hinder return to sport or sport performance upon return.
Limitations
This study has limitations. Most importantly, this study was conducted retrospectively and included a relatively small number of patients, which was necessary given the novelty of the ATVBT/PLST procedure. Second, while cultural and psychosocial factors undoubtedly played a role in return to sport rates between the groups, the effect of these variables was not studied. Finally, while the mean follow-up times for ATVBT/PLST and PSIF patients were 2.9 and 2.5 years, respectively, with all patients having a minimum 2 year follow-up, medium- and long-term studies are required to fully understand a condition and procedure. These studies should utilize maturity to define timeframes, which may be defined by Risser stage 5, status of distal physes of the ulna and radius, or other radiographic methods such as that of Sanders. This is because growth can deform the spine and challenge any system that would resist such deformation. Unanticipated consequences (such as the health of squeezed and partially immobilized intervertebral discs) may potentially be exposed with long-term follow-up. Long-term follow-up may also help identify technical issues such as cable fracture and determine whether the intervention is temporary during growth. If so, and the device acts like a brace in this way, cable breakage may have no negative effects and may even be an advantage. Otherwise, cables should be made to be durable as long as possible.
Conclusion
ATVBT/PLST patients reported significantly faster rates of returning to sport, running, and PE. In addition, ATVBT/PLST patients were less likely to have to give up activities due to bending ability after surgery and reported no changes in their ability to bend after surgery more frequently than PSIF patients. However, the overall rate of return to the same or higher level of sport participation was high amongst both groups, with no significant difference observed between ATVBT/PLST and PSIF patients. Long-term studies are needed to further delineate relationships between an earlier return to sport and complications after ATVBT/PLST, as it is unclear whether the benefits of an earlier return to activity and an improved ability to bend justify the reduced curve correction and potential trend toward increased risk for revision surgery after ATVBT/PLST vs PSIF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.D. serves as an advisor at Auctus, a startup developing a magnetically controlled tethering system. The remaining authors declare no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.