
Abstract
Study Design:
Retrospective cohort study.
Background:
Percutaneous pedicle screws (PPS) have the advantage of being able to better preserve the paraspinal muscles when compared with a traditional open approach. However, the nature of changes in postoperative paraspinal muscle after damage by lumbar fusion surgery has remained largely unknown. It is clinically important to clarify and compare changes in paraspinal muscles after the various surgeries.
Objective:
(1) To determine postoperative changes of muscle density and cross-sectional area using computed tomography (CT), and (2) to compare paraspinal muscle changes after posterior lumbar interbody fusion (PLIF) with traditional open approaches and minimally invasive lateral lumbar interbody fusions (LLIF) with PPS.
Methods:
We included data from 39 consecutive female patients who underwent open PLIF and 23 consecutive patients who underwent single-staged treatment with LLIF followed by posterior PPS fixation at a single level (L4-5). All patients underwent preoperative, 6 months postoperative, and 1-year postoperative CT imaging. Measurements of the cross-sectional area (CSA) and muscle densities of paraspinal muscles were obtained using regions of interest defined by manual tracing.
Results:
We did not find any decrease of CSA in any paraspinal muscles. We did find a decrease of muscle density in the multifidus at 1 year after surgery in patients in the PILF group, but not in those in LLIF/PPS group.
Conclusions:
One year after surgery, a significant postoperative decrease of muscle density of the multifidi was observed only in patients who underwent open PLIF, but not in those who underwent LLIF/PPS.
Keywords
Introduction
Spinal interbody fusion has been used widely as a surgical procedure to fuse 2 or more vertebrae and to stabilize spinal segments. Traditional open posterior approaches for fusion and supplemental internal fixation require large skin incisions and extensive dissection of the paraspinal musculature. Therefore, open lumbar spine surgeries have been more often associated with stubborn surgical site pain than minimally invasive techniques. 1 Recently, the usefulness and validity of minimally invasive lumbar interbody fusions with percutaneous pedicle screws (PPS) for spondylodiscitis have been described.2,3 The advantages of these minimally invasive techniques over open techniques include reduction of blood loss, less surgical site pain, quicker recovery, and reduction of postoperative wound infections.4-6 Moreover, one of the most important benefits may be reduced invasion of paraspinal muscles. Compared with traditional open approaches, an advantage of PPS is the relative preservation of the posterior components of the lumbar spine.7-9 However, the extent of postoperative paraspinal muscle change after damage by lumbar fusion surgery has remained largely unknown.
The importance of paraspinal muscles in the pathophysiology of spinal disorders has attracted increasing attention. 10 Numerous studies have indicated paraspinal muscles play a potential role in spinal disorders, successful bone union in patients with osteoporosis, maintenance of spinopelvic alignment, and low back pain.11-13 Therefore, it is clinically important to clarify changes in paraspinal muscles after surgery. The purpose of the present study was (1) to determine postoperative changes of muscle density and cross-sectional area (CSA) using CT, and (2) to compare paraspinal muscle changes after posterior lumbar interbody fusion (PLIF) with traditional open approaches and minimally invasive lateral lumbar interbody fusions (LLIF) with PPS.
Materials and Methods
The present study was approved by the Institutional review board of the authors’ affiliated institution. Informed consent was obtained and documented from all patients using a signed consent form.
Patient Group and Surgical Techniques
Patients were candidates for surgery if fusion was indicated because of degenerative lumbar spondylolisthesis and if an adequate conservative treatment, such as drug, exercise and brace treatments, had been exhausted. The following criteria were applied: (1) no history of previous lumbar surgery, (2) female sex, (3) one fusion length at the L4-5 level (4) severe low back and leg pain, and no improvement with conservative therapy for at least 3 months. Patients with spondylolytic spondylolisthesis or spinal deformities, or both, were excluded.
We included data from 62 consecutive patients with degenerative spondylolisthesis grade I or II treated at a single institution by 2 board certified spinal surgeons who had gained expertise in the LLIF procedure before the beginning of the study. From April 2012 to March 2013, 39 consecutive patients underwent open PLIF, and from April 2013 to March 2015, 23 consecutive patients underwent single-staged treatment with LLIF, followed by posterior PPS fixation using intraoperative CT (O-arm) image-guidance navigation as previously described 7 but without posterior decompression. All patients were followed up for a minimum of 1 year in our outpatient clinic. Patient data including age, body mass index (BMI), bone mineral density (BMD), surgical time, and intraoperative blood loss was obtained from medical records (Table 1).
Demographics of Patients Undergoing Open PILF or XLIF With PPS.
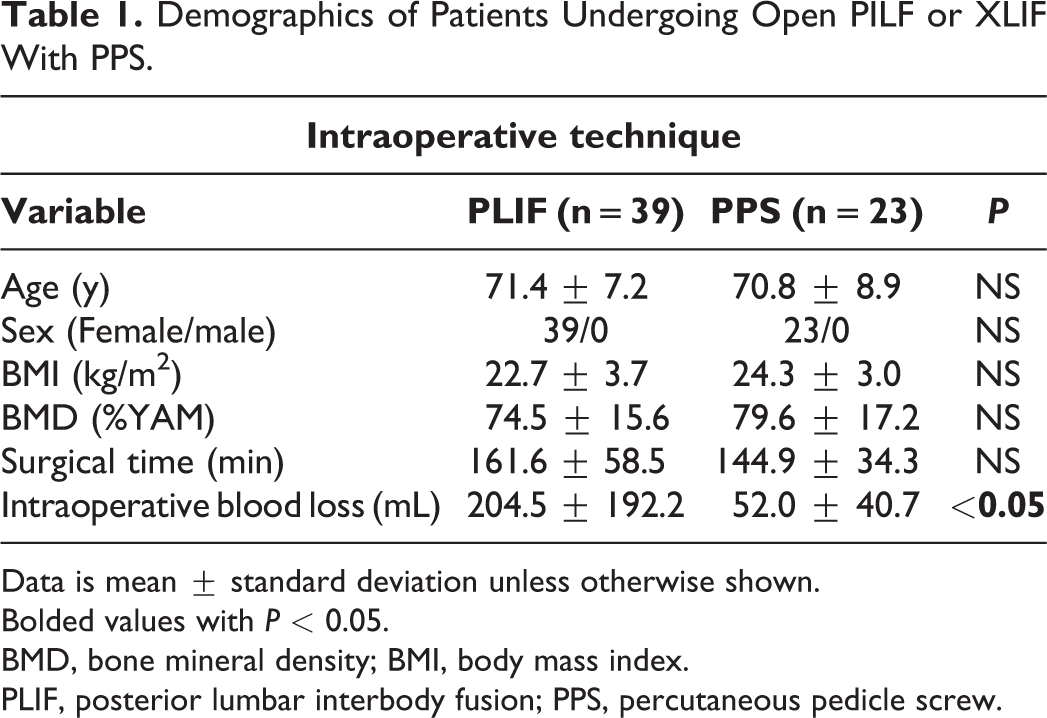
Data is mean ± standard deviation unless otherwise shown.
Bolded values with P < 0.05.
BMD, bone mineral density; BMI, body mass index.
PLIF, posterior lumbar interbody fusion; PPS, percutaneous pedicle screw.
Computed Tomography
All patients underwent preoperative, 6 months postoperative, and 1 year postoperative imaging using an 8 slice multidetector CT system with a 0.83 mm section thickness (Lightspeed Ultra; GE Healthcare, Milwaukee, WI, USA).
Measurement of the rCSA and Muscle Density of Paraspinal Muscles With CT
To determine interobserver error, all CT measurements were acquired by 2 experienced orthopedic surgeons (KK; author 1 and TE; author 3) blinded to the clinical information and study hypothesis. We applied the mean values of these measurements to the following analysis. The intraclass coefficient of multifidi CT density (Hu) was 0.9578, indicating that the inter-rater reliability was almost ideal (Figure 1A). Following the previously described methodology, 14 regions of interest (ROI) were defined by manual tracing of the fascial boundary of the following muscles on both sides of the spinal column to the superior endplate of L3 vertebral body to exclude instrumentation that appeared on CT images: psoas major, multifidus, and erector spinae (encompassing both the longissimus and iliocostalis muscles), and the quadratus lumborum muscles (Figure 1B). Relative CSA (rCSA) was defined as the CSA of each of the muscles divided by the CSA of the spinal column to the superior endplate of the fixed upper end vertebral body.15-17 Measurements of the muscle densities (by CT) of the average of the left and right paraspinal muscles were obtained using the same ROI as for CSA. Change of CT density (▵CT density) was calculated as 1 year postoperative values – preoperative values.
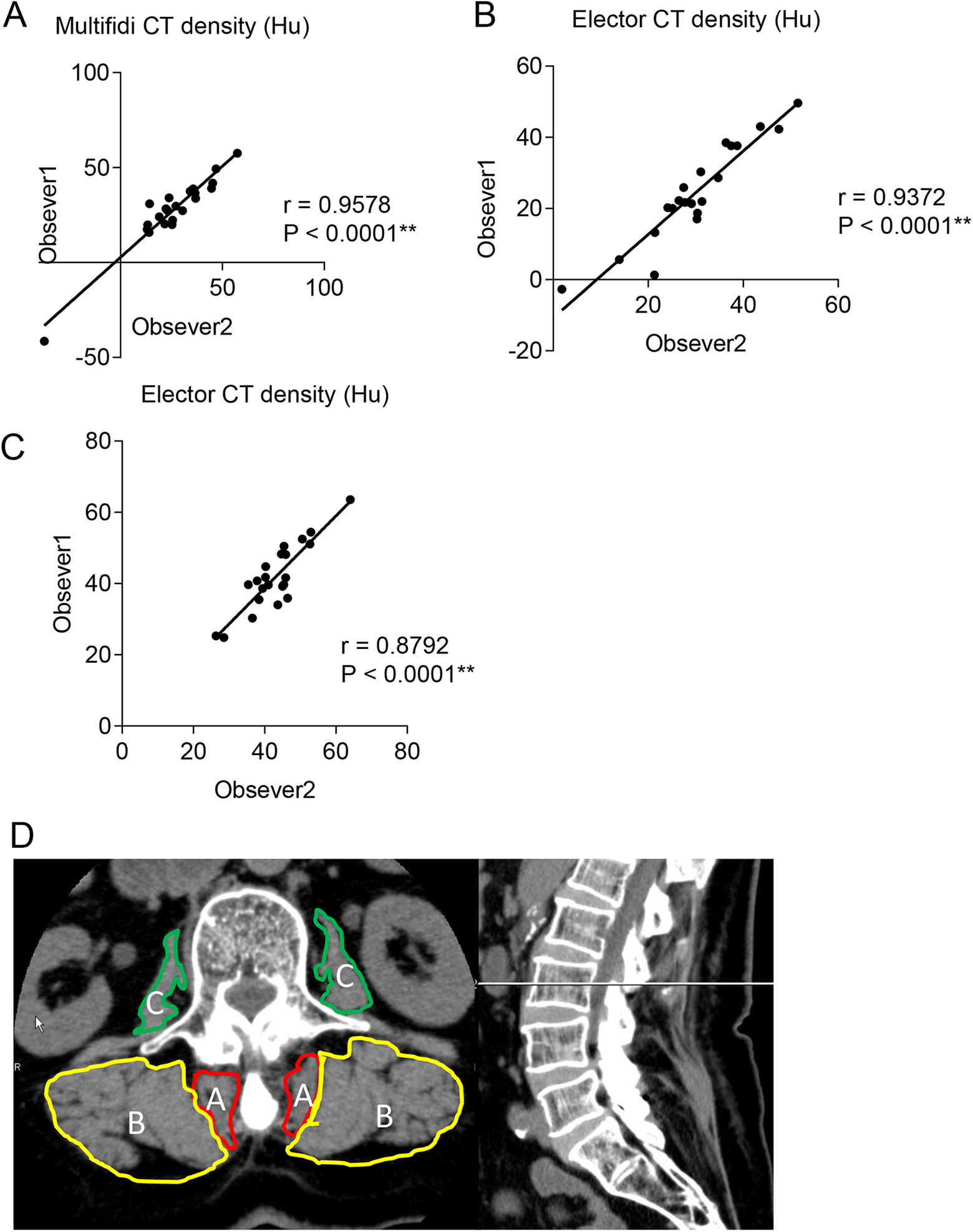
A. Interobserver errors in CT values of paraspinal muscles by 2 readers. B. Measurement of the cross-sectional area and muscle density on CT axial images of paraspinal muscles using Synapse. A = multifidi; B = erector spinae; C = psoas.
MRI Protocol
Patients were supine while maintaining a neutral spine position with a pillow placed under their knees during imaging. The MRI was performed using a 3.0 T dual gradient superconducting MRI system (Discovery 750; GE Medical Systems, Milwaukee, WI) with an 8-channel NeuroVascular-full neck coil, at a gradient strength of 40 mT/m, and a slew rate of 150 mT/m/ms. Sagittal and axial T1-weighted and T2-weighted images were acquired routinely.
Measurement of the rmCSA of Paraspinal Muscles as Visualized by MRI
Following previously described methodology,11 regions of interest (ROI) were defined by manual tracing of the fascial boundary of the multifidus muscles on both sides of the spinal column to the superior endplate of the L3 vertebral body on T1 axial images. The ROIs were analyzed and histograms showing the signal intensity were generated using digital image processing software (Image J, National Institutes of Health, Bethesda, MD). FI (%) within the total CSA of muscles on both sides was evaluated using a threshold technique. Briefly, the number of pixels representing intramuscular fatty tissue were distinguished using a threshold grayscale value of 120. Relative CSA (rCSA) was defined as the CSA of each of the muscles divided by the CSA of the L3 vertebral body.15-17 T1-weighted fat signal was removed from the rCSA to determine rmCSA using the following equation: rmCSA (100%–FI%)*rCSA.
Statistical Analysis
All data is reported as means ± standard deviation. Data was analyzed using a 2-sided Student t test, a Kruskal–Wallis test, or Fisher exact test to determine any differences. rCSA and CT-density of paraspinal muscles were compared between preoperatively, and 6 months after surgery, and 1 year after surgery using a 2-sided Student t test. Correlations between FI (%) measured with MRI, and muscle density measured with CT, rCSA measured with MRI and CT, and muscle density measured by 2 observers were correlated using Pearson coefficients. All statistical calculations were performed using Prism (version 8.0; GraphPad Software, La Jolla, CA). P < 0.05 was considered significant.
Results
Comparison of Patient Demographics
Table 1 summarizes the demographics of the patients who underwent spinal interbody fusion with open PLIF or LLIF/PPS. There was no significant difference in the mean age, the average body mass index (BMI), bone mineral density (BMD), or number of fused levels per patients between the groups. Surgical time was not significantly different between the groups. Intraoperative blood loss in patients in the LLIF/PPS group was significantly lower than in those in the PLIF group (Table 1).
Postoperative Changes of rCSA and Muscle Density of the Multifidi
There was no significant difference in rCSA of the multifidi between preoperatively, and 6 months after surgery or 1 year after surgery in either group (Figure 2A, B). Muscle density of the multifidus was not significantly different 6 months after surgery, but decreased significantly 1 year after surgery in patients in the open PLIF group (Figure 2C). By contrast, muscle density of the multifidus in patients in the LLIF/PPS group was not changed significantly. The multifidus of a patient representative of the PLIF group preoperatively and 1 year after surgery are shown in Figure 2E.
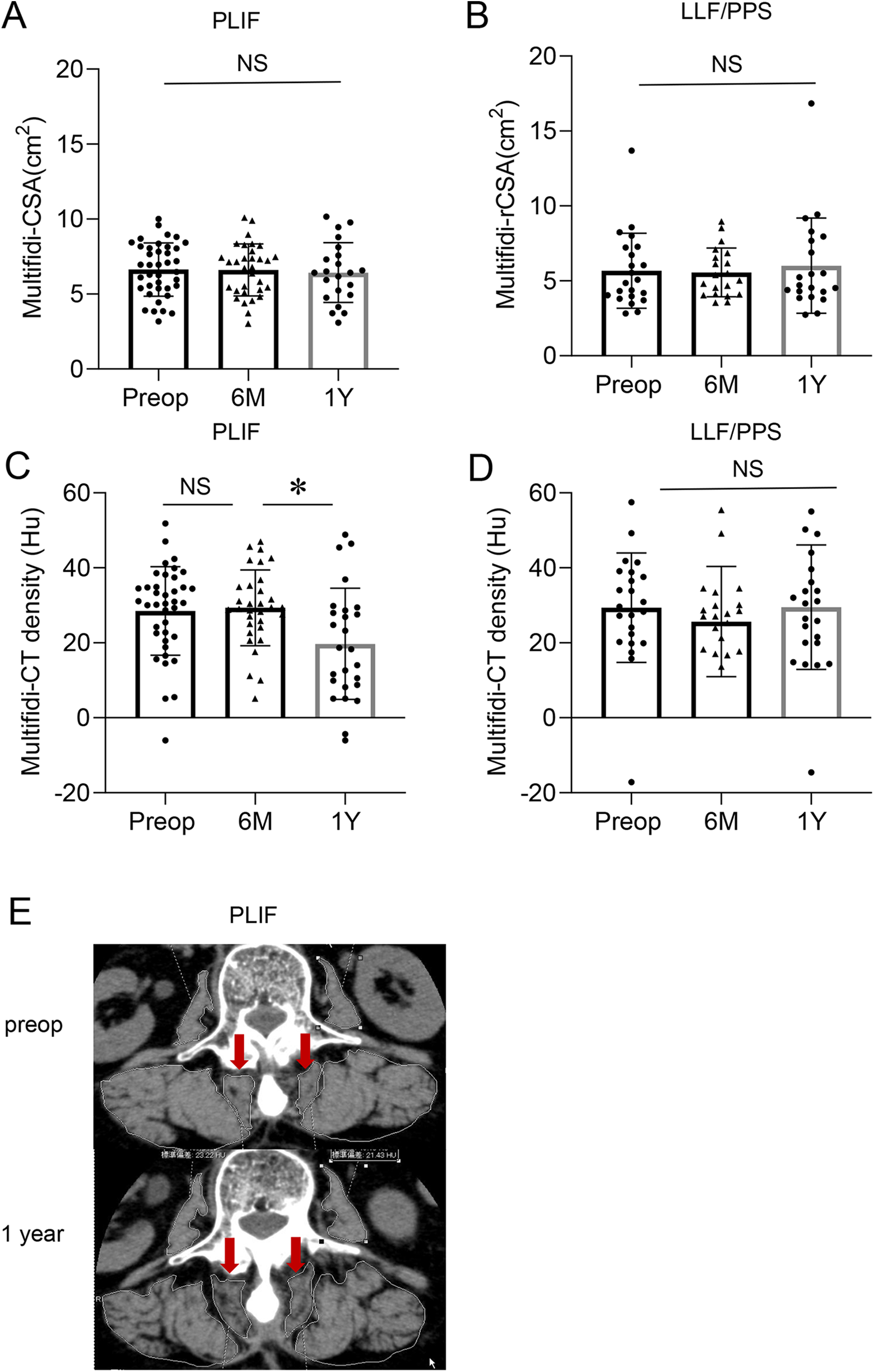
Comparison of the total relative muscle cross-sectional area (rCSA) of the multifidi preoperatively, and 6 months after surgery, and 1 year after surgery in patients in the PLIF group (A) and in those in the LLF/PPS group (B). Comparison of the muscle density of the multifidi preoperatively, and 6 months after surgery, and 1 year after surgery in patients in the PLIF group (C) and in those in the LLF/PPS group (D). Representative CT axial imaging of postoperative decrease of muscle density in the multifidi of a patient in the PLIF group 1 year after surgery (E). LLIF; lateral lumbar interbody fusions. PPS; percutaneous pedicle screws. NS; not significant. P < 0.05.
Correlation Between Evaluations of Paraspinal Muscle by CT and MRI
To verify the validity of evaluating paraspinal muscles by CT, we analyzed the correlation with the MRI data, which is a conventional criterion standard method to evaluate the size and especially the quality of the muscles of preoperative multifidi in both groups. There was a significantly high correlation of preoperative multifidi between rCSA measured by CT and MRI (Supplemental Figure). Additionally, a significantly negative correlation between FI (%) of preoperative multifidi measured with MRI and muscle density measured with CT is shown in the Supplemental Figure.
Postoperative Changes of rCSA and Muscle Density of the Psoas
There was no significant difference in rCSA of the psoas between preoperatively, and 6 months after surgery or 1 year after surgery in either group (Figure 3A, B). By contrast, the muscle density of the psoas was increased significantly 1 year after surgery in both groups (Figure 3C, D).
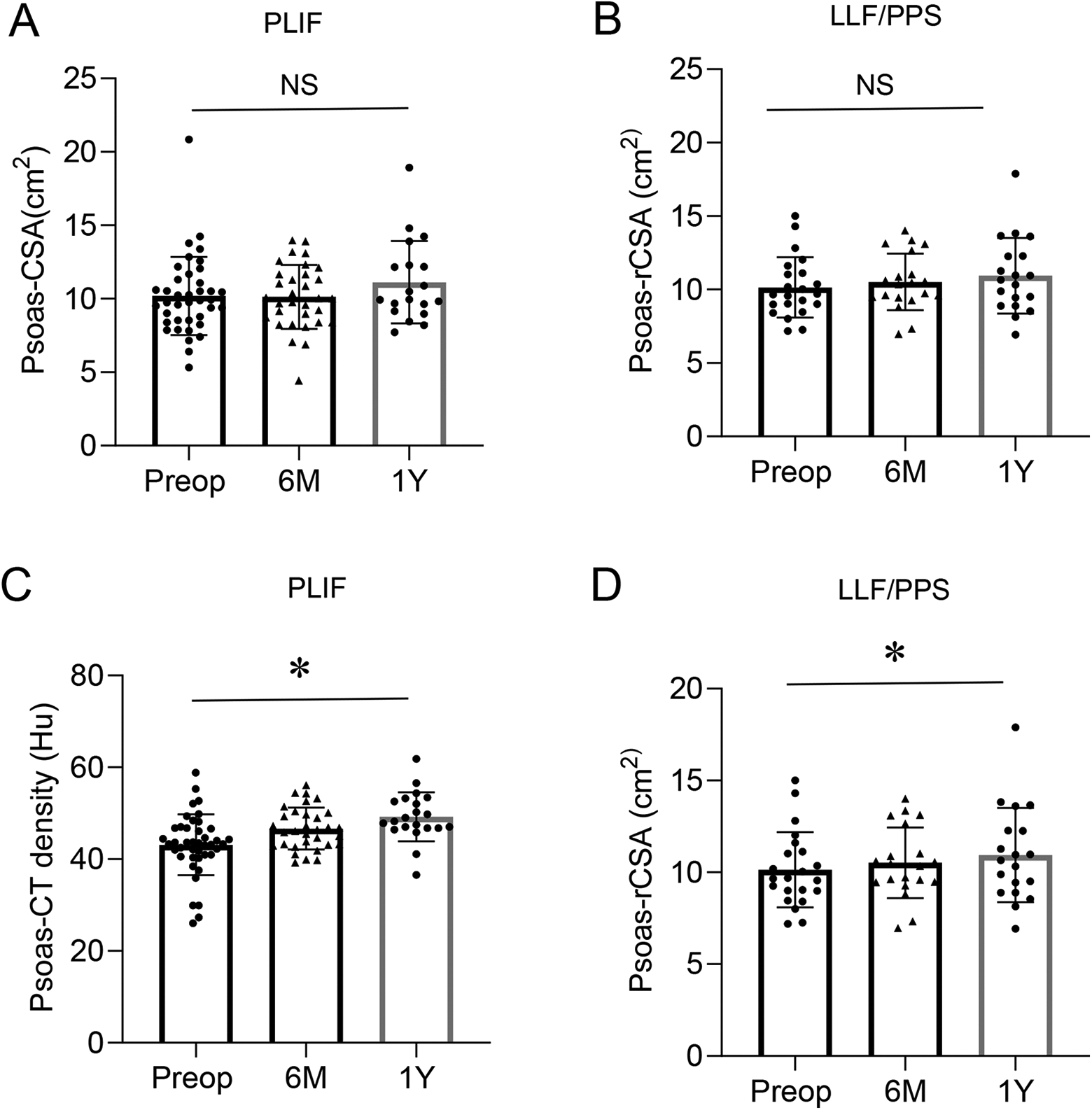
Comparison of the total relative muscle cross-sectional area (rCSA) of the psoas preoperatively, and 6 months after surgery, and 1 year after surgery in patients in the PLIF group (A) and in those in the LLF/PPS group (B). Comparison of the muscle density of the psoas preoperatively, and 6 months after surgery, and 1 year after surgery in patients in the PLIF group (C) and in those in the LLF/PPS group (D). LLIF; lateral lumbar interbody fusions. PPS; percutaneous pedicle screws. NS; not significant. *P < 0.05.
Postoperative Changes of rCSA and Muscle Density of Erector Spinae
There was no significant difference in rCSA or muscle density of erector spinae between preoperatively, and 6 months after surgery or 1 year after surgery in either group (Figure 4A-D).
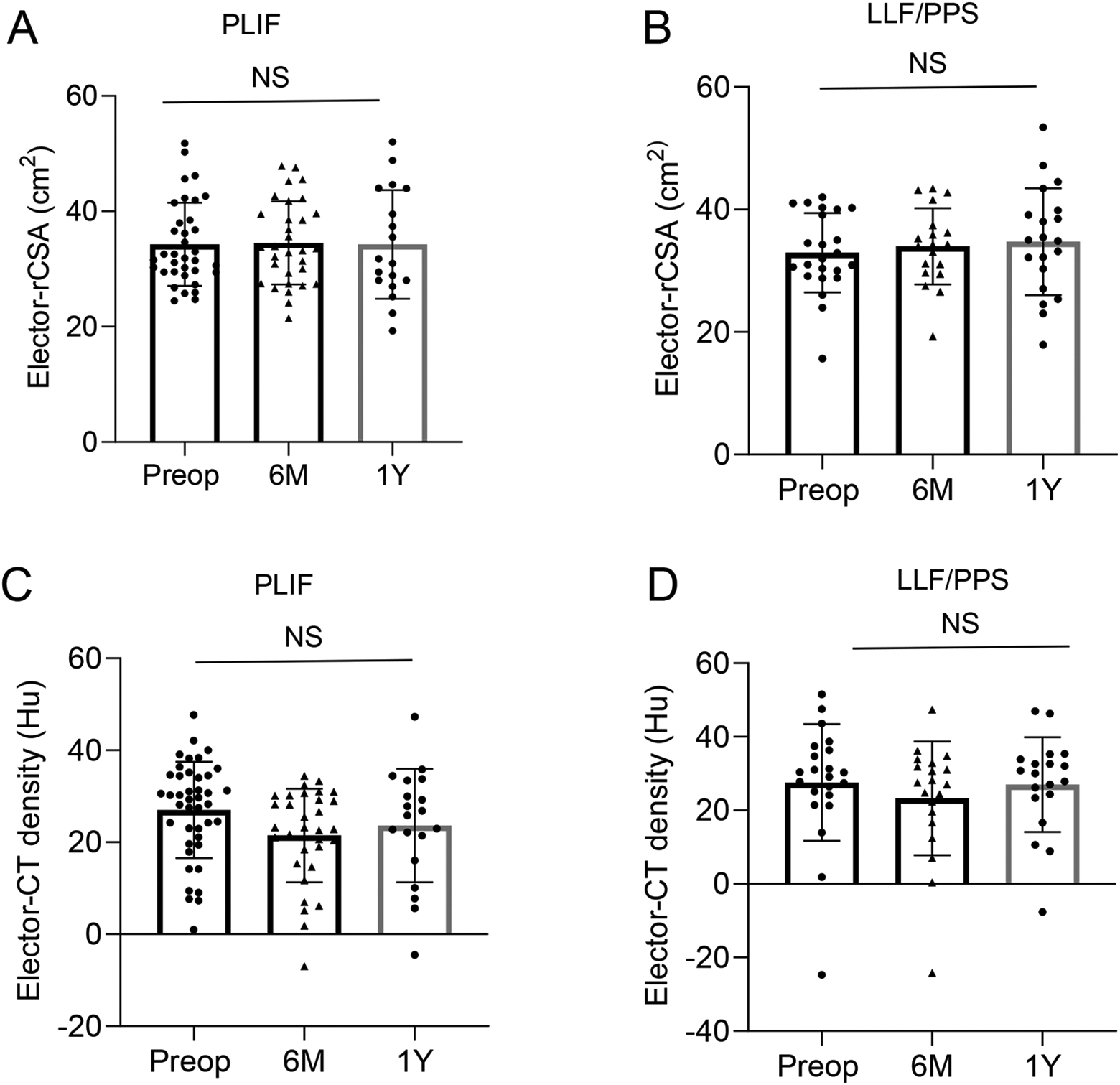
Comparison of the total relative muscle cross-sectional area (rCSA) of erector spinae preoperatively, and 6 months after surgery, and 1 year after surgery in patients in the PLIF group (A) and in those in the LLF/PPS group (B). Comparison of the muscle density of elector spinae preoperatively, and 6 months after surgery, and 1 year after surgery in patients in the PLIF group (C) and in those in the LLF/PPS group (D). LLIF; lateral lumbar interbody fusions. PPS; percutaneous pedicle screws. NS; not significant.
Comparison of Postoperative Muscle Density Changes of Paraspinal Muscles Between PLIF vs LLIF/PPS Group
The muscle density of the multifidus in patients in the PLIF group was decreased significantly 1 year after surgery. By contrast, muscle density of the multifidus in patients in the LLIF/PPS group was not changed significantly (Figure 5A). By contrast, muscle density of the psoas was increased significantly in both groups, but there was no significant difference between patients in the open PLIF or LLIF/PPS groups (Figure 5B).
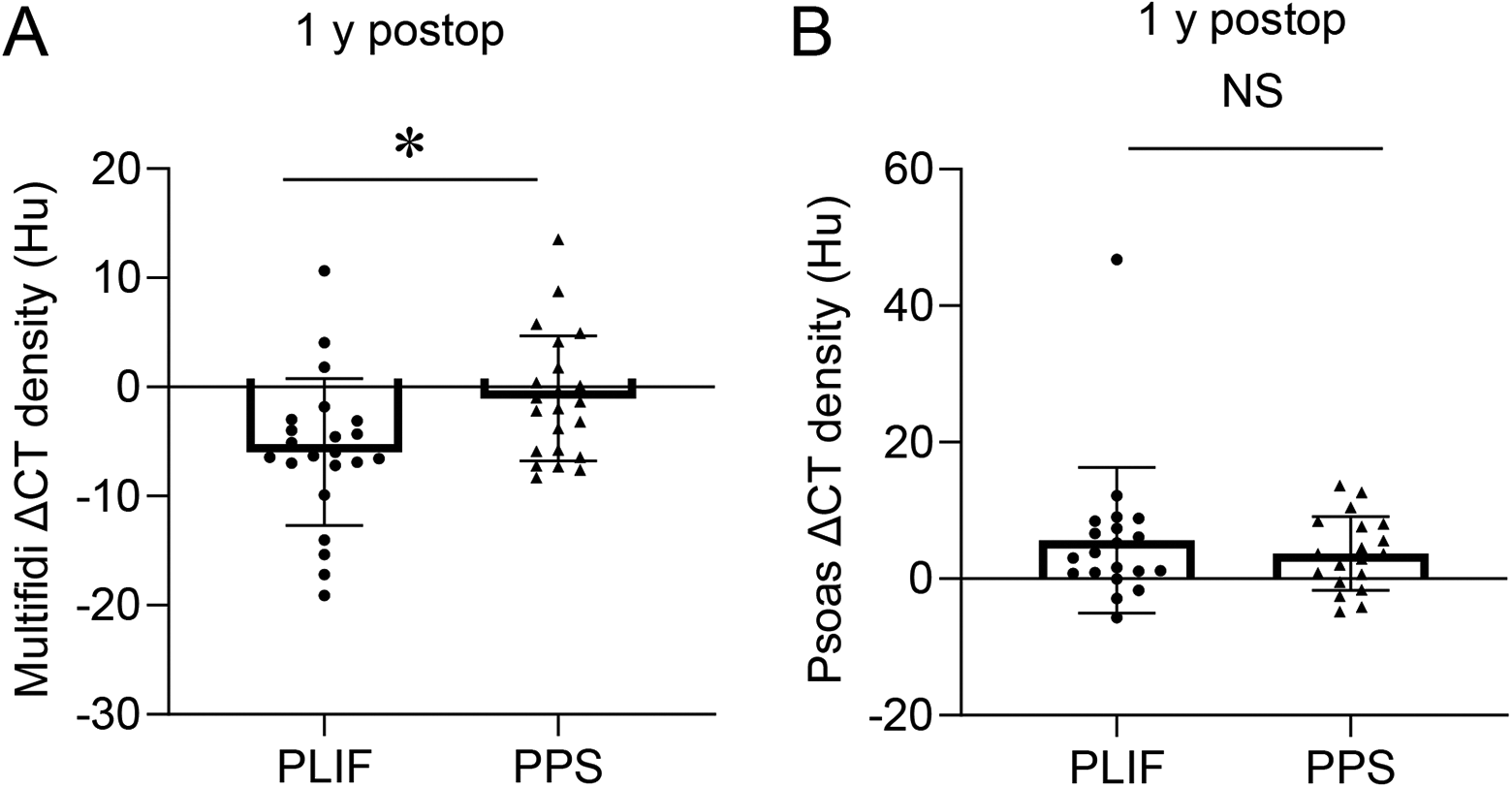
Comparison of changes of muscle density of the multifidi in patients 1 year after surgery between those in the (A) PLIF group and (B) those in the LLIF/PPS group. ▵, preoperative values – postoperative values.
Discussion
CT and MRI are useful techniques for quantifying the CSA and fat infiltration of paraspinal muscles.11,12 However, specific postoperative changes associated with posterior surgical intervention of paraspinal muscles have remained largely unknown. Posterior surgical postoperative atrophy of paraspinal muscles quantified using CSA has been correlated with operation time.18,19 Interestingly, the present study did not show a decrease of CSA in paraspinal muscles, but found a decrease of muscle density in the multifidus as measured by CT. Reduction in paraspinal muscle density is known to be associated with degenerative disc and facet joint disease, which might result in exacerbation of either postoperative low back pain, adjacent segment disease, progressive deformity, 2 of these, or all 3 conditions.20-22 The present study made 4 important clinical observations. First, it clarified that postoperative changes of the multifidi did not occur within 6 months of surgery, but changes appeared by 1 year after surgery. Second, the postoperative atrophy of the multifidi did not change rCSA, but a difference in muscle density was found. Third, postoperative changes in paraspinal muscles could be observed using a relatively simple CT method, but not by MRI. Fourth, we found LLIF/PPS is less invasive to the multifidi than traditional open PLIF.
Numerous studies have compared muscle damage in open versus PPS insertion procedures using serum markers such as creatinine kinase.8,23,7 However, changes in muscle volume and quality that may occur postsurgically cannot be determined using serum markers. Traditional posterior open lumbar fusion surgery is associated with significant damage to paraspinal muscles as a result of long incisions and extensive retraction resulting in denervation of the paraspinal musculature.24,25 During the surgical procedure retractors cause a significant increase in the intramuscular pressure of the paraspinal muscles and this pressure causes a reduction in capillary perfusion, resulting in ischemic changes within the muscle.26,27 Postoperative trunk muscle performance is dependent on the time for which muscles are retracted. 28 The present study found that radiological changes in the multifidi musculature associated with this damage did not appear within 6 months after surgery, but had appeared within a 1 year after the surgery in patients in the open PLIF group, but not in those in the LLIF/PPS group,where retractors were not used for posterior surgery. We presume 2 potential physiological reasons why it took 1 year for this decrease in muscle density. First, the main pathogenesis of decreased postoperative trunk muscle density is thought to be fatty infiltration into postoperative muscles. 29 It is still unclear how long it takes for fat infiltration to progress from muscle damage, and further research is needed to clarify the period. However, our past report about vertebral fractures showed that until about 1 year after the injury, the longer the elapsed time after the injury, the more the fatty infiltration of the trunk muscle progresses. 11 Second, past reports demonstrated that follow-up imaging at approximately 1 year after surgery is preferable for evaluating fatty infiltration into postoperative muscles because postoperative muscle edema and swelling can be present for up to 6 months after surgery.29-30
Despite that MRI has been well recognized as the criterion standard to identify the size and especially the quality of the muscles, a problem with using it in clinical practice is that it takes more time and effort to evaluate muscle quality such as fatty infiltration. Recent reports showed CT density is useful and valid for evaluating muscle volume and fatty infiltration.21,22 We confirmed a significantly high correlation between %FI evaluated with MRI and muscle density evaluated with CT, and a significantly high correlation of CSA evaluated with MRI and CT (Supplemental Figure). These results indicate CT can be used instead of MRI to evaluate rCSA and density of paraspinal muscles. Because CT is a relatively simple method and highly reproducible, it can be more easily adapted for use in the clinic.
Limitations of the present study are that assessments were only made radiologically, and we did not conduct physical examinations or make electrophysiological assessments.
Conclusion
One year after surgery, a significant postoperative decrease of muscle density of the multifidi was observed with CT only in patients who underwent open PLIF, but not in those who underwent LLIF/PPS.
Supplemental Material
Supplemental Material, sj-jpg-1-gsj-10.1177_2192568221994794 - Radiological Assessment of Postoperative Paraspinal Muscle Changes After Lumbar Interbody Fusion With or Without Minimally Invasive Techniques
Supplemental Material, sj-jpg-1-gsj-10.1177_2192568221994794 for Radiological Assessment of Postoperative Paraspinal Muscle Changes After Lumbar Interbody Fusion With or Without Minimally Invasive Techniques by Keigo Kameyama, Tetsuro Ohba, Tomoka Endo, Marina Katsu, Fujita Koji, Koyama Kensuke, Kotaro Oda, Nobuki Tanaka and Hirotaka Haro in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB
The study was approved by University of Yamanashi institutional review board (application No. 1632).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.