
Abstract
Study Design
Retrospective comparative study.
Objective
To compare the accuracy of intra-operative navigation-assisted percutaneous pedicle screw insertion between bone fixed and skin fixed dynamic reference frame (DRF) in Minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF).
Methods
Between October 2018 and September 2022, patients who underwent MIS-TLIF were included in this study with DRF fixed either on bone (group B) or skin (group S). Pedicle screws were inserted under the guidance of intra-operative Cone bean Computed tomography (cbCT) based navigation. Accuracy of pedicle screw placement was immediately checked by a final intra-operative cbCT Spin.
Results
Among 170 patients, group B included 91 patients and group S included 79 patients. Out of total 680 screws, 364 screws (group B) and 316 screws (group S) were placed. Patient’s demographic data and distribution of screws showed no statistically significant difference. The accuracy showed no significant difference between both the groups (94.5% in group B and 94.3% in group S).
Conclusion
Skin fixed DRF can serve as an alternate way for placement and avoids extra incision with similar accuracy in pedicle screw insertions with bone fixed DRF using intra-operative CT guided navigation in MIS TLIF.
Keywords
Introduction
The prevalence of Minimally-invasive transforaminal interbody fusion (MIS-TLIF) in treatment of diversified lumbar degenerative disorder has increased in last 2 decades due to low invasiveness of this procedure, thus reducing surrounding tissue damage, post operative pain, hospital stay and complication rates compared to open transforaminal interbody fusion.1,2
Indirect visualization of anatomic landmarks in fluoroscopy for pedicle screw placement increases the risk of malposition or perforation of the pedicle screw instrumentation. 3 Evolution in advanced intra-operative imaging and incorporation of mobile intra-operative cone beam computed tomography (cbCT) has increasingly improved the accuracy of pedicle screw insertion to 92-99%.4,5
The Dynamic Reference Frame (DRF) is a key component that maintains the synchronization between the virtual data acquired by intraoperative 3D Computed Tomography (CT) scan and the actual anatomical position for maintaining accuracy of navigation system. A stable reference frame fixation is therefore a critical step in navigated spine surgery. 6 Traditionally bone anchored DRF on spinous process and posterior superior iliac spine (PSIS) are robustly fixed to increase accuracy of navigation, but requires a separate incision. 7
Skin fixed DRF as a reliable method for navigation in cervical and minimally invasive lumbar surgery has been described in literature.8-10 However, the literature regarding skin fixed DRF in minimally invasive spine surgery is encouraging, but is still in nascent stages.
To best of our knowledge, there is paucity of literature on comparison of accuracy of pedicle screw placement in MIS TLIF with bone vs skin fixed DRF. The purpose of this study is to compare accuracy of pedicle screw placement in MIS TLIF with bone vs skin fixed DRF.
Material and Methods
Indication, Inclusion, and Exclusion Criteria
This study was a retrospective comparative analysis of accuracy of percutaneous pedicle screw placement under intraoperative cbCT guided navigation in MIS TLIF with bone vs Skin fixed DRF. This study was approved by institutional ethical committee of Stavya Spine hospital and research institute and registered in Clinical Trial registry India (CTRI) (Registration no: CTRI/2023/01/048766) and was conducted according to the principles of the Declaration of Helsinki. The informed consent was exempted from institutional review board as per retrospective nature of this study. The inclusion criteria were (1) single level fusion between L3 and S1 (2) Symptomatic lumbar disc herniation combined with segmental instability, degenerative spondylolisthesis or lumbar stenosis requiring facetectomy and fusion (3) Failure of at least 6 weeks of conservative therapy. The exclusion criteria were (1) Previous spinal surgery at index level or active infection (2) spinal deformity requiring multiple level fusion surgery (3) Grade III, IV spondylolisthesis requiring open surgeries (4) severe internal medical/autoimmune disease.
In accordance with above inclusion criteria, patients who underwent MIS TLIF with intra-operative cbCT machine (O arm, Medtronic, Minneapolis MN) and navigation system (Stealth S8 navigation system, Medtronic sofamor danek, Memphis, USA) from October 2018 to September 2022 were included in this study after institutional review board approval. The DRF during MIS TLIF was fixed on skin or spinous process (bony) as per surgeon’s preference. Three surgeons (BRD, SM, RR) preferred bony fixation of DRF and 2 surgeons preferred (AK, DD) preferred fixation of DRF on skin.
Surgical Technique
The patients were positioned prone on the standard radiolucent operative table with chest roll under general anaesthesia. Patient was strapped to the operating table with the use of fast adhesive tapes. MIS-TLIF was performed on more symptomatic sides. A paramedian longitudinal skin incision (25-30 mm) is made 3.5 cm-4.5 cm off the midline after confirmation of the level to be operated. A tubular retractor system (Mast quadrant, Medtronic Sofamor Danek, Memphis, TN, USA) of diameter 22 mm was docked at facet complex after serial dilatation of increasing diameter and secured to the operative table under 2 dimensional fluroscopic guidance using a image intensification machine. All the surgeries were performed using loupe magnification. The inferior facet and the underlying ligamentum flavum were removed to expose the traversing nerve roots and the lateral edge of the dura. The posterolateral annulotomy and complete discectomy was performed using pituitary forceps, curette and serial dilators. The anterior portion of the prepared disc space was adequately filled with autologous bone fragments obtained during the decompression process. After confirming the disc size, titanium cage filled with autologous bone graft was inserted obliquely into the disc space, confirmed under imaging for proper placement.
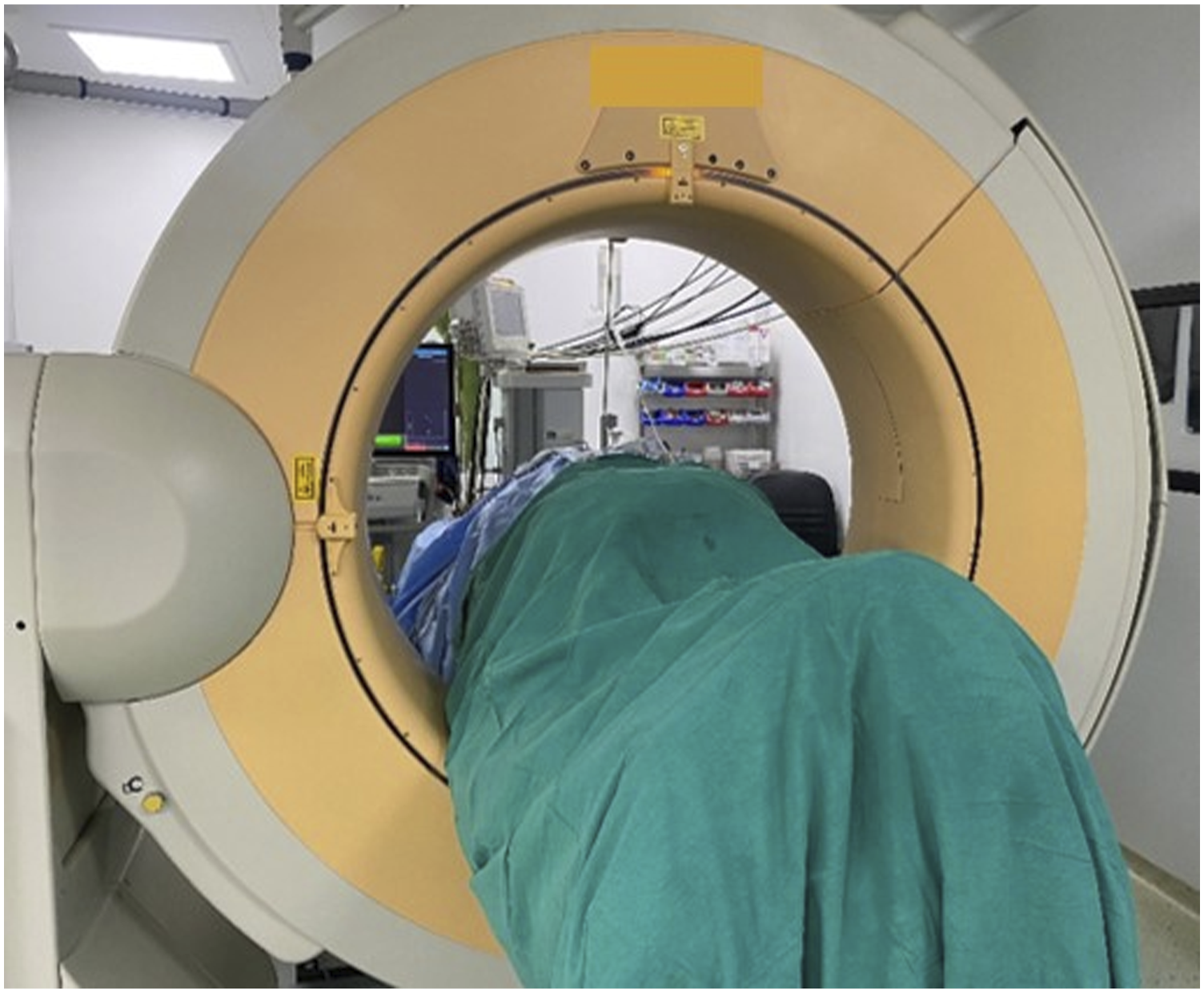
The DRF (Stealth system, Medtronic sofamor Danek, Memphis, TN, USA) in bone fixed group (group B) was fixed to spinous process using a separate skin incision at 2 level above the index level on an aluminum stand (Figure 1). The DRF in skin fixed group (group S) was fixed on skin 2 spinous process level above the index level with non-absorbable mono filament suture and sterile adhesive tape (Figure 2). The patient was subsequently covered temporarily with a large sterile reusable drape which works as barrier to sterile surgical field during acquisition of images (Figure 3). Fixation of DRF with aluminum stand on spinous process 2 level above the fusion level. Fixation of DRF on skin with adhesive tapes and nylon suture 2 level above the fusion level. Intra-operative image acquisition with 3DCT machine with patient covered with large sterile reusable drape to maintain sterility.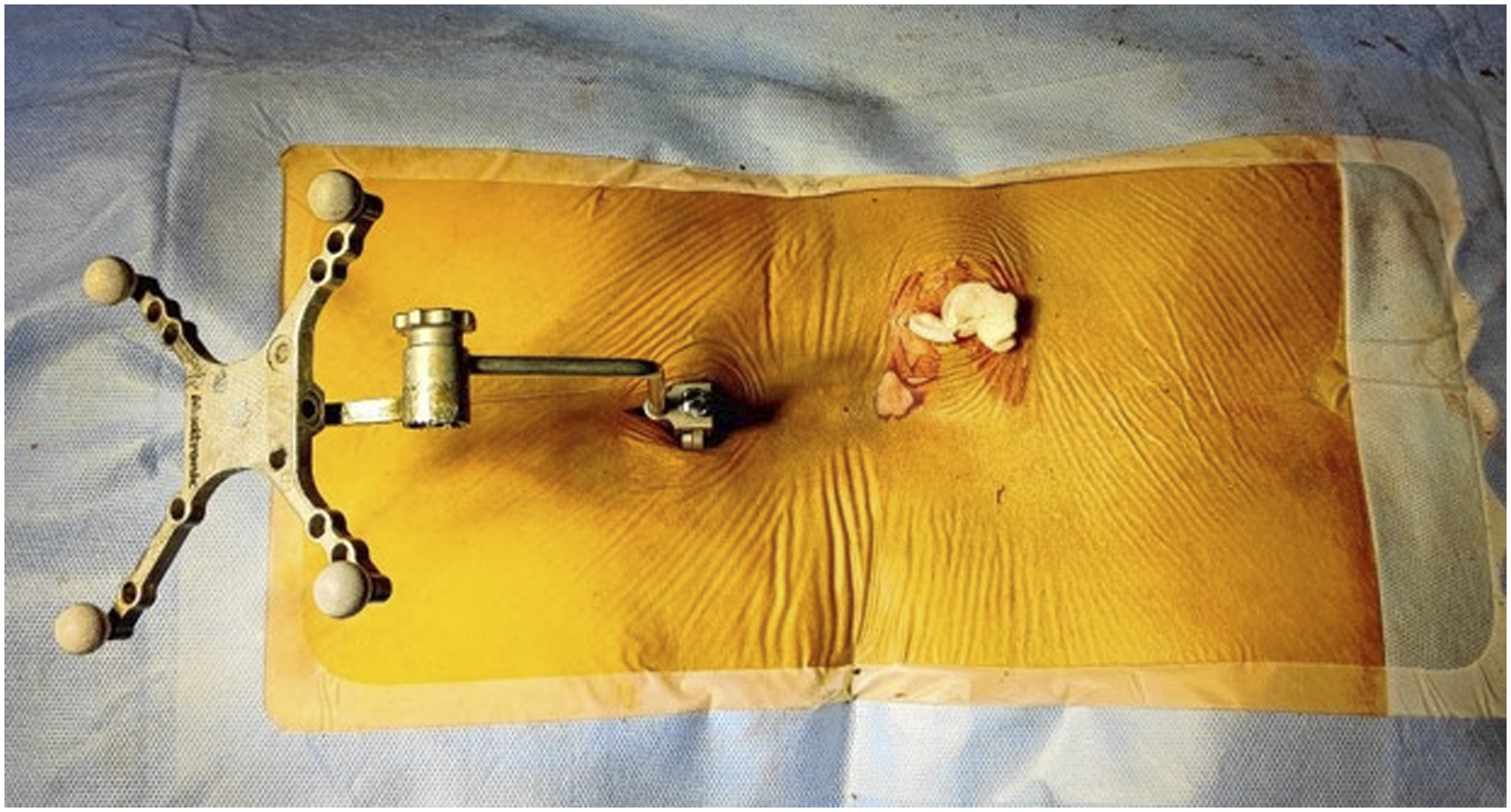

A CT scan was performed by intra-operative cbCT machine to acquire 3D images which are automatically transferred to the navigation system. All the steps of pedicle screw insertion were done under navigation guidance. Ideal pedicle entry points were sought and pilot hole was made with a passive array Pedicle access needle (PAK needle) (Medtronic, USA) using gentle tapping. The direction of the pilot pedicle hole was continuously monitored under navigation and guide wires were inserted in pilot holes. Tapping with 5.5-mm cannulated tap was done to a measured depth on navigation. The ipsilateral pedicle screw fixation was performed through the decompression incision and to prevent injury to neural tissue by the navigated PAK needle, a saline soaked radiopaque gauze piece is inserted in tubular track for decompression. Pedicle screw fixation on the contralateral side was done using similar technique percutaneously. After all the screws have been inserted, a second CT scan was performed to verify their actual positions. A contoured rod was then passed underneath the fascia and the intervertebral space was moderately compressed and final tightening of set screws was done. The surgical wound is washed and closed in layers.
Accuracy of Navigation
Pedicle screw accuracy and degree of cortical breaches were assessed and confirmed on intra-operative second CT scan. The accuracy of the navigation was assessed on axial and sagittal planes using the classification of 2-mm increment from Gertzbein and Robbins, et al: 11 grade 0- no pedicle breach; grade I- only the threads were outside the pedicle (less than 2 mm); grade II- the core screw diameter was outside the pedicle (2-4 mm); and grade III- the screw was entirely outside the pedicle. The assessment of the images and measurements of the pedicle perforations were performed by a surgeon who was independent of the study using a computerized DICOM viewer (Medsyanptic system, India).
Statistical Analyses
Patients age, body mass index (BMI) was analysed with independent sample t test. The peri-operative accuracy of pedicle screw insertions was analysed using paired t test. Statistical significance was set at P < .05. All statistical analyses were performed using SPSS version 25.0 (IBM, Chicago, IL, USA).
Results
Patient’s Demographics and Distribution of Screws.
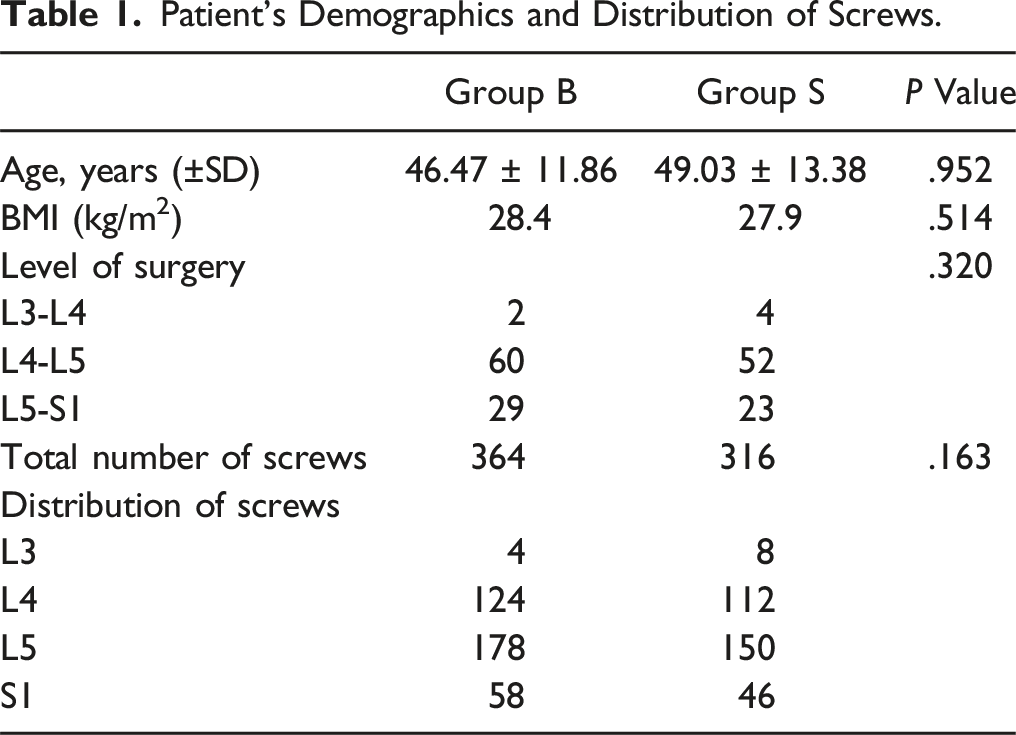
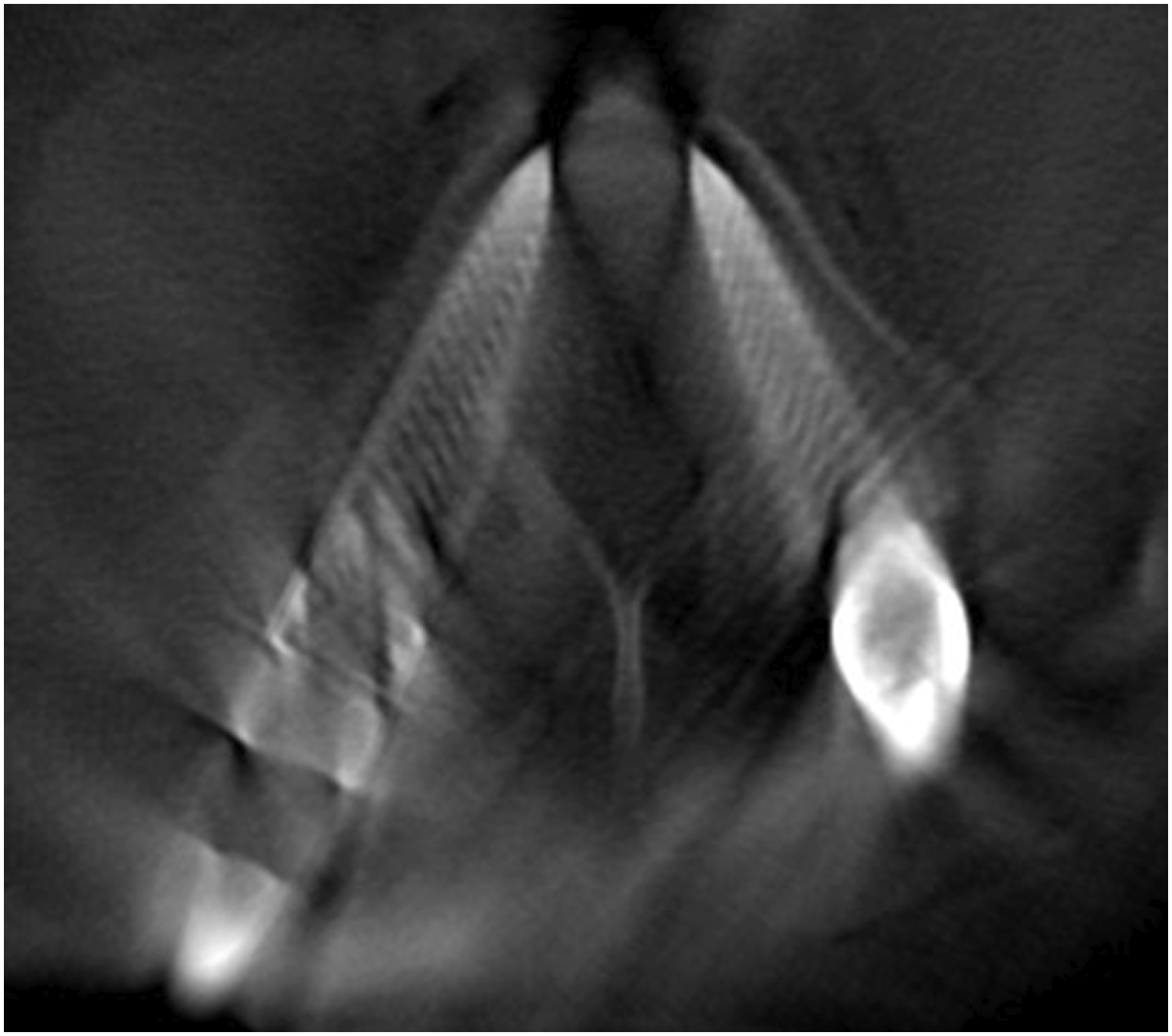
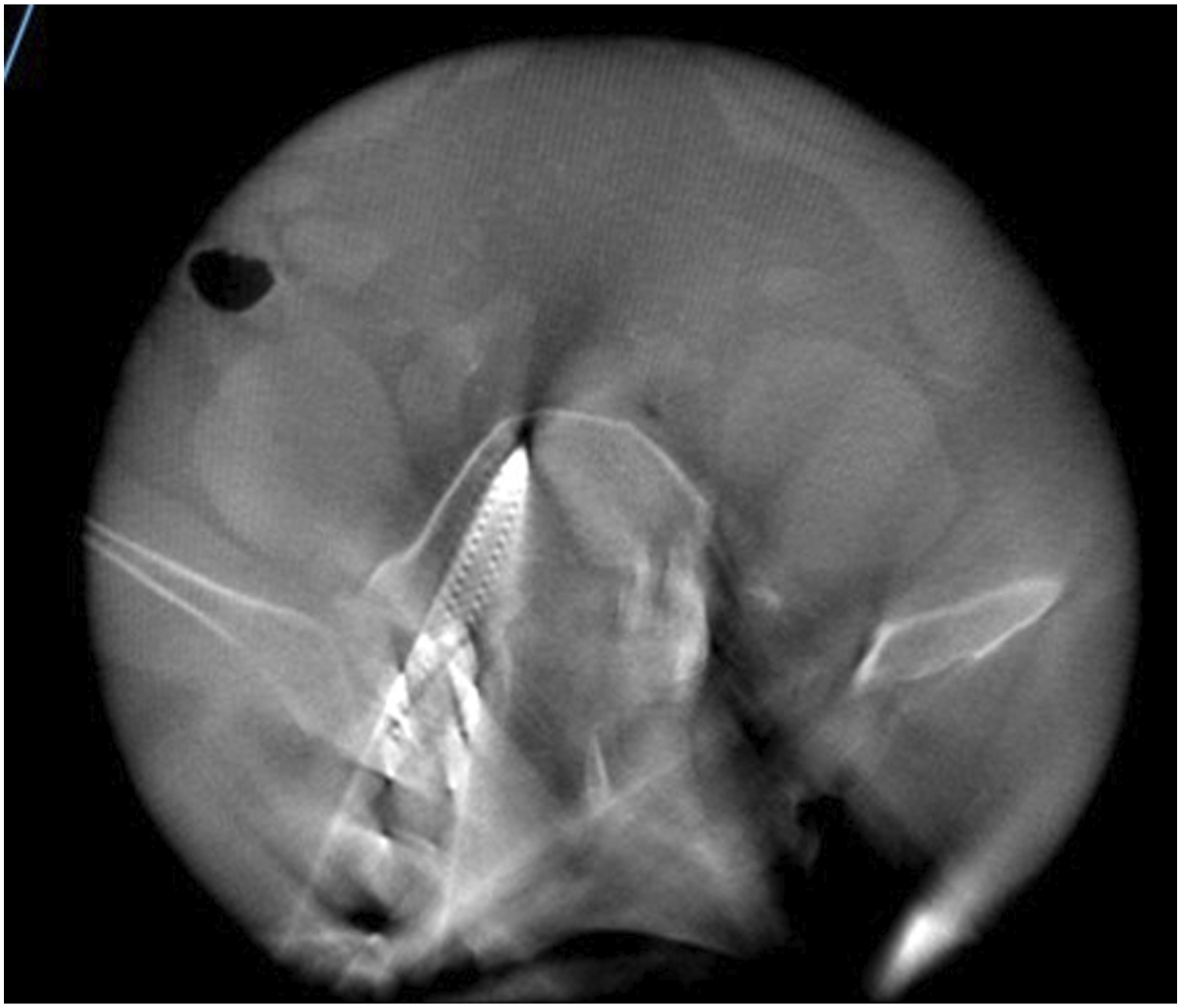
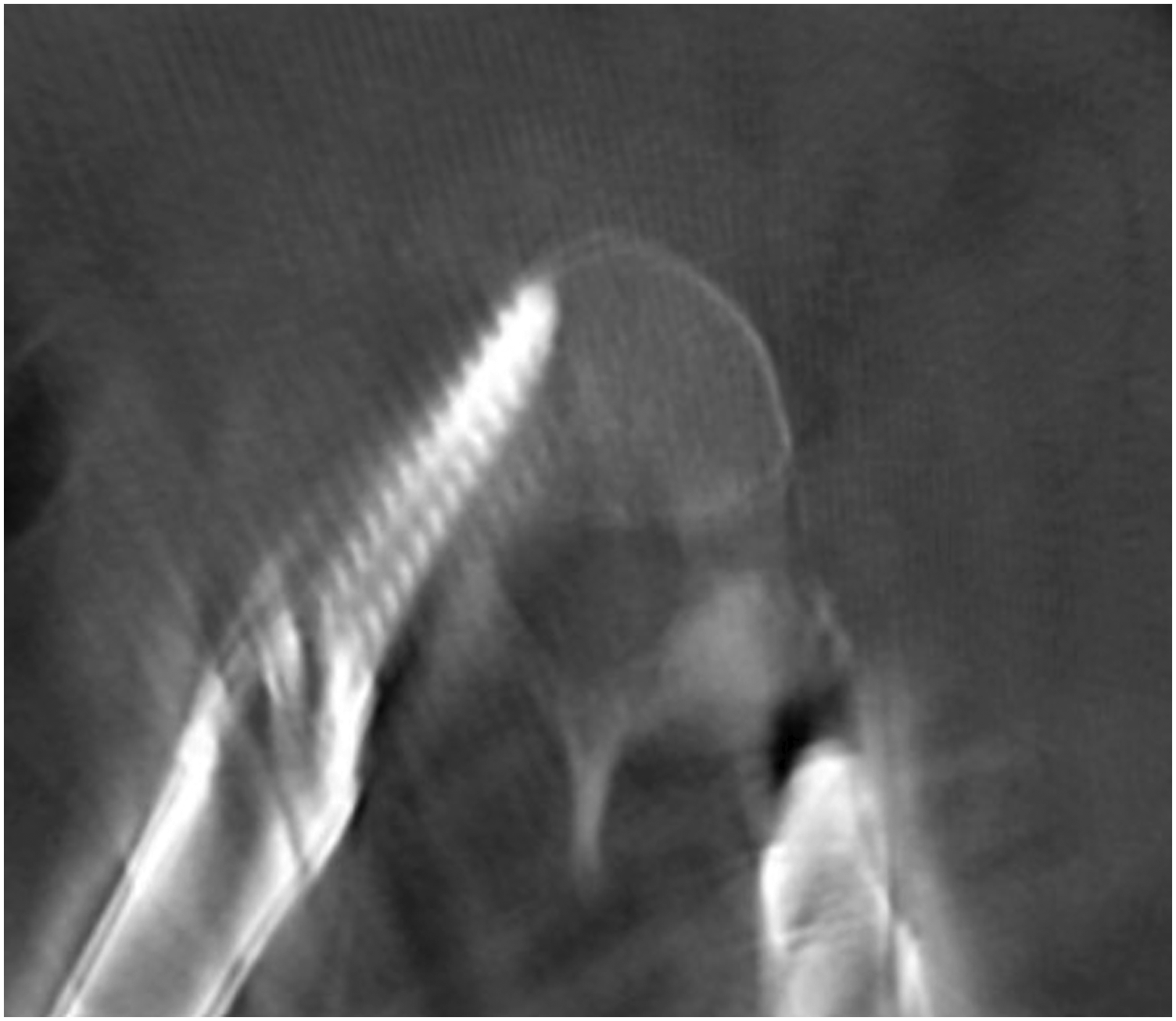
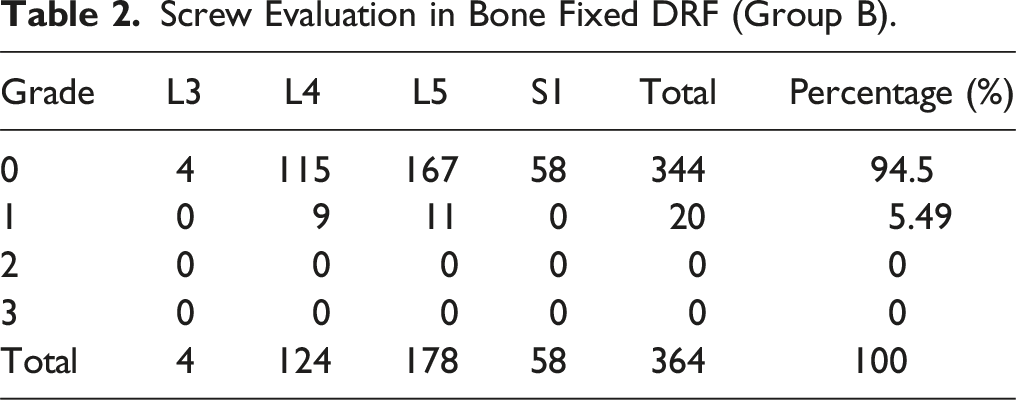
In total 680 pedicle screws were inserted. 364 screws inserted in group B and 316 were inserted in group S. 642 screws had no violation or breach of cortex, 36 screws had a grade I violation (Figures 4 and 5) and 2 screws had grade II violation (Figures 6 and 7). No screw had grade III violation as observed in this study. The accuracy of screw in group B and screws in group S was 94.50% and 94.30% respectively. (Tables 2 and 3) All screws with grade I violation were acceptable (Lateral and medial) while screws with grade 2 violation were changed intra-operatively with the third additional scan. Accuracy of screw placement showed no statistically significant difference between both the groups (Table 4). Instrumentation related complications, such as nerve root injury, cerebrospinal fluid leakage were not observed in the patients population. No patients had any complaint postoperatively and revision surgery was not needed. L4 screw left grade 1 medial breach. L5 screw right grade 1 medial breach. L4 screw right grade 2 medial breach. L5 screw right grade 2 lateral breach. Screw Evaluation in Bone Fixed DRF (Group B). Screw Evaluation in Skin Fixed DRF (Group S). Screw Accuracies in Both Groups.


Discussion
The evolution of Minimally invasive spine surgery (MISS) required the reliance on fluoroscopy image-based cannulation of pedicle for pedicle screw insertion rather than visible landmark in open surgeries. Presence of dural sac, exiting nerve root in the vicinity of pedicle are at risk of injury in screw trajectory misplacement that can sometimes lead to serious complication. 3
Screw breach or misplacement by free hand pedicle screw technique, assessed by postoperative CT is reported to be ranging from 7-40% in literature.12,13 With the aid of intra-operative 2D fluoroscopy, pedicle screw accuracy improved ranging from 72-90% as described in literature.3,14,15 Biplanar imaging, no axial reconstructed view, increased risk of radiation exposure, overcrowding of surgical field were inherent disadvantage of C arm based 2D fluoroscopy imaging. 16 Development of computer assisted navigation and 3D imaging has improved in accuracy of placement of pedicle screw.2,17 The median accuracy of pedicle screw placement improved to 95.1% from 90.3% with and without the assistance of navigation respectively as shown in a systemic review. 18
Preoperative CT image-based navigation was developed to circumvent the disadvantages related to fluoroscopic guided screw placement. The requirement of multi point paired registration intra-operatively with a preoperative acquired CT scan has a surgeon dependent inherent error. The position variation (preoperative CT in supine and intra-operative prone position) may change the intersegmental relationships between the adjacent vertebral levels, resulting in potential navigational inaccuracy. 19 Advancement in intra-operative 3D CT-based imaging technologies and navigation provide a real time coronal, axial and sagittal images which are of utmost importance specially in cases with variable pedicle morphometry, trefoil spinal canal and deformity 20 and negate the need on intra-operative fluoroscopy during pedicle screw insertion thus reducing the radiation exposure and requirement of heavy lead apron. Automatic registration of vertebral levels for spinal image guidance in intra-operative 3D CT with navigation is less cumbersome compared with previous techniques of paired point matching with preoperative CT scan. 21 The accuracy of the navigation system highly depends on the stability of DRF which maintains the synchronization between the virtual acquired navigated position and the actual anatomical positions, thus stable and sturdy fixation of the reference frame is a critical step in navigation-based surgery. 22 Unstable or flimsy fixation of DRF will result in desynchronization of the navigation tracking system leading to inaccuracy in pedicle screw placement. 16
Traditional placement of DRF on bony landmark on either adjacent spinous process or posterior superior iliac spine (PSIS) for stable fixation has been described in literature with accuracy ranging from 93-99%.6,16,23 Placement of the DRF on an adjacent spinous process requires a separate incision. The snag with bone-anchored DRF in lumbar spine surgery described in literature were (1) Streak artefact from the tracker in acquired virtual image, affecting image quality (2) Hindrance of instrument trajectory in deformity cases and S1 screw (3) Separate incision (4) DRF movement while using the mallet with the pedicle awl and pedicle probe (5) Hold of toothed DRF on spinous process is flimsy in elderly population due to osteoporosis. 10 Use of PSIS for anchoring DRF as described by Best et al 6 is still a source of streak artefact’s, especially for L5-S1 level surgery and close proximity of DRF can hinder with instrument/surgeon’s motion or can get dislodged when may require all together a new acquisition of intra-operative CT scan.
Placement of the DRF away from the surgical field has been reviewed in literature for cervico-occipital surgeries with accurate screw placement.6,21 Use of adhesive cutaneous non-invasive tracker (Spine mask, Stryker navigation, USA) eliminate the need of bony anchorage of DRF, thus reducing morbidity. In a prospective study by Malham et al, on use of spine mask as reference frame showed 93% accuracy in placement of pedicle screw. The cutaneous adhesive tracker is susceptible to any skin distortion which can affect the accuracy of navigation. Retraction within surgical field in spine mask, larger subcutaneous tissue mobility in obese patient and on-table patient movement are the factor affecting accuracy. 10 Cost and non-reusability also affect important limiting factor to use of adhesive cutaneous non-invasive tracker.
In our study, we mounted the DRF on the skin about 2-3 levels above the fusion level DRF is fixed with non-absorbable suture and sterile adhesive tapes, away from the surgical field without the use of any special device, and non-invasively eliminating the need for an additional skin incision. Placing the DRF away from the surgical site, avoided the streak artefact of tracker in intra-operative acquired images. We had an advantage of non-prominent DRF that had no interference with instrument movement throughout the surgical procedure especially at L5-S1 level without compromising the accuracy. The screw accuracy in our study in skin fixed group was demonstrated to be 94.3%. This was consistent with other recent publications reporting accuracies of 93-95.6% using skin fixed DRF.24,25
Mitigation by completion of decompression, placement of cage and removal of tubular retractor before application DRF over skin and intra-operative CT imaging are followed as a protocol in both the groups that helped us to achieve better accuracy. Avoiding contact by surgeon and assistant to table and patient after acquiring intra-operative CT scan to prevent inadvertent jolt, gentle tapping by cannulated tap over guide wire are crucial steps to be followed to avoid any excessive motion of table/patient, thus maintaining accuracy of navigation. Placement of guide wire through 2.3 mm navigation guided PAK needle and reconfirmation of transpedicular insertion on 2D fluoroscopy before screw placement adds to additional confirmation to avoid major pedicle screw malposition especially for the beginners.
Limitations of the Study
We acknowledge that the retrospective nature of our study, single observer participation in the study are the limitation of this study. Surgeon’s preference to use either skin fixed or bone fixed DRF was a confounding factor in selection of cohort. Another limitation was although number of cases are moderate for comparison which are homogenous for age/sex and BMI. But, disease and morphometry of the pathology has not been compared like listhesis, disc prolapse. It is important to note that although the present study suggests that skin fixed DRF provides similar accuracy in pedicle screw insertions with bone fixed DRF using intra-operative 3D image guided navigation, A prospective randomized controlled trial to eliminate potential biases that may have affected our conclusion.
Conclusion
The study re-confirms the accuracy of intra-operative CT guided navigation in pedicle screw insertion for MIS TLIF as described in literature. We observed the accuracy of navigation for pedicle screw insertion with Skin fixed DRF is similar as with spinous process fixed DRF. Skin fixed DRF circumvents the need of additional incision for fixation of reference frame. Skin fixed DRF can serve as an alternative placement point for the DRF in navigated screw placement without compromising the accuracy of navigation.
Footnotes
Acknowledgments
The author thanks to Stavya research team for assistance with manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Stavya spine hospital’s ethics Committee and the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Institutional review board of Stavya spine hospital and research institute approved this single centre, retrospective comparative Cross-sectional study and was registered in Clinical Trial registry India (Registration no: CTRI/2023/01/048766).