
Abstract
Study Design
Prospective randomized controlled trial.
Objectives
No prospective studies have directly compared clinical and radiographic outcomes of unilateral vs bilateral instrumented lateral lumbar interbody fusion (LLIF) for lumbar degenerative disease (LDD). We compared the short-term radiographic, clinical outcomes, and some complications of the unilateral percutaneous pedicle screw (PPS) (UPS) vs bilateral PPS (BPS) fixation in short-level spinal fusion with LLIF for LDD.
Methods
This was a prospective randomized controlled study of 33 patients who underwent UPS or BPS fixation after LLIF for LDD; 18 patients were assigned to the UPS group and 15 patients to the BPS group. Clinical outcomes, complication rates, and fusion rates were assessed.
Results
The two groups were similar in age, sex, preoperative diagnosis, and level of surgery. Blood loss, length of hospital stay, and numeric rating scale score one year after surgery did not differ between groups. The operative time was longer in the BPS than UPS group (120.2 vs 88.8 min, respectively; P = .029). Both groups showed improvement in disc height and dural sac in the immediate postoperative computed tomography and magnetic resonance imaging, which did not differ significantly between groups. The subsidence grade and fusion rate did not differ, but cage subsidence was more severe in the UPS than BPS group.
Conclusion
Unilateral and bilateral PPS fixation after LLIF yielded similar short-term clinical and radiological outcomes. However, severe cage subsidence was more common in the UPS group, which suggests that BPS fixation after LLIF may be a better choice over the long term.
Keywords
Introduction
Lateral lumbar interbody fusion (LLIF) has become a popular procedure in spine surgery1-3 and is used to treat various spinal diseases such as lumbar spinal stenosis,4,5 and adult spinal deformities.6,7 Recent studies have reported using single-position surgery (SPS) using LLIF to reduce surgical invasiveness.8-12 A systematic review of SPS has suggested that, compared with dual position surgery with postural changes, SPS can reduce operative time without compromising alignment. 13 Compared with conventional posterior lumbar fusion, LLIF has some advantages, including the ability to perform a large discectomy, bilateral annular release, preservation of posterior bony structures, and insertion of large grafts. By contrast, given the graft size limitations, traditional posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF) has typically been performed using pedicle screws. 14 This has prompted discussion about the methods of posterior fixation associated with PLIF or TLIF.
Some studies have compared the efficacy of TLIF using unilateral or bilateral instrumentation.15-17 We should thoroughly discuss the need for this additional posterior instrument, including the rate of bone union and complications of the LLIF procedure. A previous study reported less cage subsidence and the need for reoperation after adding posterior instrumentation to LLIF compared to a stand-alone operation with or without posterior instrumentation. 18 Thus, we believe that many spine centers use posterior instrumentation during LLIF surgery.
A study that compared the clinical outcomes of LLIF surgery using unilateral or bilateral percutaneous pedicle screw (PPS) fixation found that LLIF with unilateral PPS had a shorter operative time and better clinical outcomes than LLIF with bilateral PPS fixation. 19 Du et al also reported that unilateral instrumentation following LLIF was associated with significant improvement in clinical outcomes and favorable radiographic outcomes. 20 If LLIF with unilateral instrumentation can produce results similar to bilateral instrumentation, the procedure could be much simpler and less invasive for the patient. To our knowledge, no prospective randomized controlled studies have directly compared clinical and radiographic outcomes of unilateral vs bilateral instrumentation with LLIF for patients with a lumbar degenerative disease (LDD). We have conducted the first randomized clinical trial of LLIF surgery with unilateral PPS (UPS) or bilateral PPS (BPS) fixation to explore the possibility of minimally invasive surgery. This study aimed to evaluate the short-term radiographic and clinical outcomes and some complications of UPS vs BPS fixation in short-level spinal fusion with LLIF for LDD patients.
Materials and Methods
IRB Statement
The authors’ affiliated institution IRB approved this research, and the study participants provided informed consent. We have received verbal and written consent to use their clinical and radiological data from all patients.
Study Design
This prospective randomized trial was approved by our institutional review board (19R-079) and was registered with the University Hospital Medical Information Network (UMIN) clinical trials registry (UMIN000037714). We have followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines. Enrollment was initiated on August 1, 2019 and closed on April 30, 2021. The final follow-up of the last patient was completed in April 2022.
Participants
All patients had experienced low back pain, severe radicular pain, or neurological symptoms. All patients underwent at least three months of conservative management before surgery with no response or inadequate response. We diagnosed all patients using plain radiographs, magnetic resonance imaging (MRI), and/or computed tomography (CT) scans. The operating spine surgeons recorded the location of the stenosis based on their evaluation of preoperative imaging studies.
All patients gave verbal and written consent to use their clinical and radiological data and consented not to be identifiable, as all data were fully anonymized. We prospectively included all patients with symptomatic lumbar degenerative disc disease, spondylolysis, or spondylolisthesis treated with LLIF (indirect decompression) in one institution. Bone mineral density (BMD) was analyzed using a dual x-ray absorptiometry (DEX) scan. We measured the BMD of the hip at the femoral neck and the lumbar spine over the L2–L4 region, expressed in g/cm2. In Japan, the diagnostic criteria for osteoporosis defined in 1996 were initially based on the percentage of the young adult mean (YAM) for the BMD of the lumbar spine or femoral neck, and osteoporosis is diagnosed as the presence of a fragility fracture at ≤70% of YAM.
Considering the sample size a priori using the G-Power Analysis software program (Heinrich Heine University, Dusseldorf, Germany), we estimated that a total of 52 included patients would be required with a 5% significance level and 80% power.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) age >50 years at the time of surgery, (2) LLIF surgery, (3) BMD of the lumbar spine and femoral neck >70% YAM, (4) history of anterior corrective fusion using multilevel LLIF under 3, (5) diagnosis of degenerative spinal disease based on physical and imaging findings, (6) receipt of a sufficient explanation about participation in this research and provision of written consent of the individual’s own free will, and (7) ≥1 year of follow-up. The exclusion criteria were a history of lumbar spine surgery, difficulty standing preoperatively because of severe neurological deficits, severe psychiatric illness, or being deemed unsuitable by the investigator or coinvestigator. We set the study termination criteria as follows. (1) there is a request to decline to participate in the study or withdraw consent. (2) there is a problem with the safety of the protocol treatment. (3) it is judged that the continuation of the study has become meaningless based on information other than this clinical study, such as papers and conference presentations. In addition, (4) it is difficult to complete the study, or the principal investigator judged it appropriate to discontinue the study for some other reason (Figure 1). Anteroposterior radiographs images of patients in each group. (A) Bilateral PPS fixation group. (B) Unilateral PPS fixation group. PPS, percutaneous pedicle screw.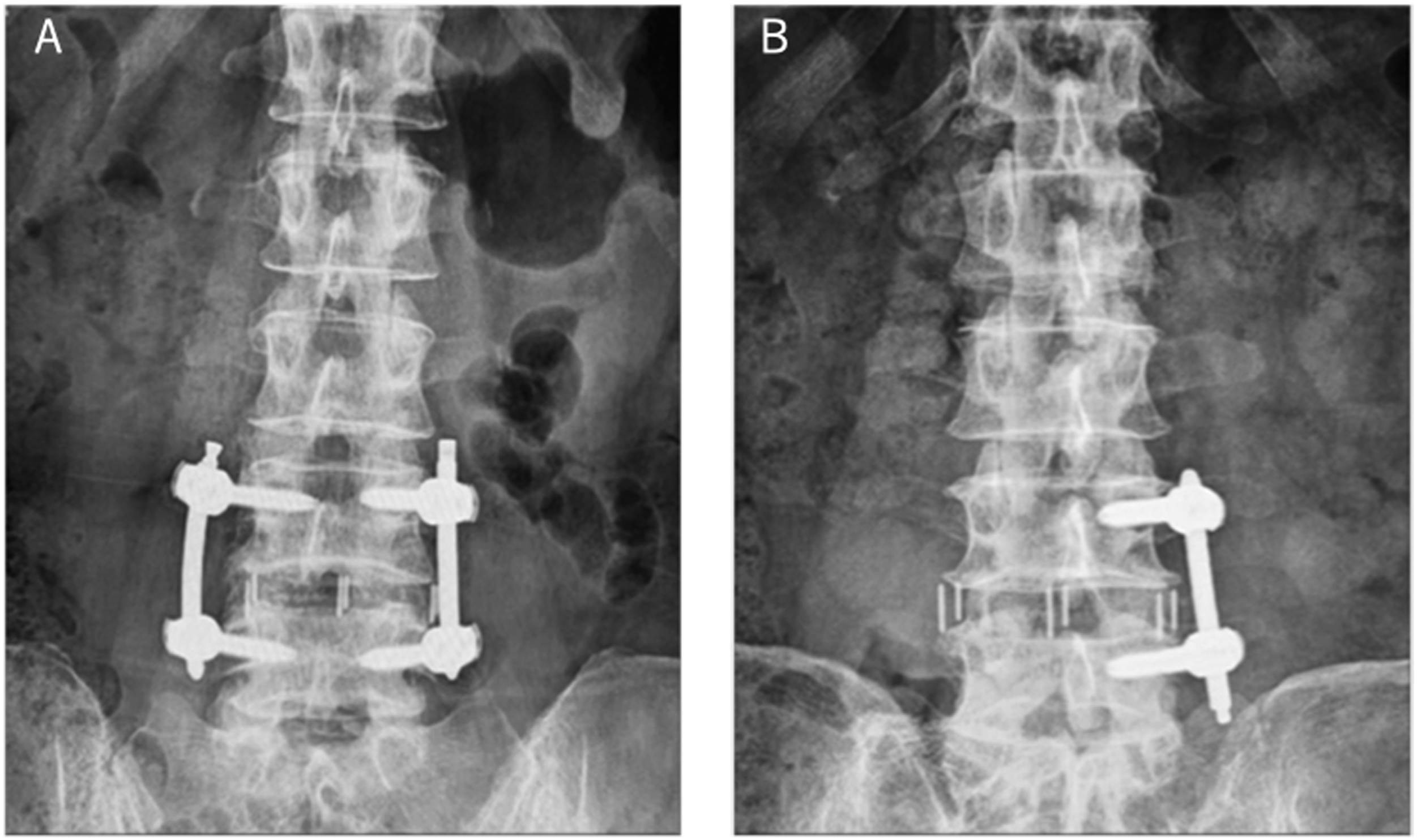
Randomization and Masking
The surgeon first explained the details of the study to patients scheduled to undergo indirect decompression with LLIF and asked if they consented to the study. We informed patients that they would be randomly assigned to unilateral or bilateral PPS fixation with LLIF and confirmed eligible to participate in the study. We also explained that for patients who did not participate in the study, conventional LLIF with bilateral PPS fixation would be performed. After receiving informed consent from eligible patients, baseline assessments, including YAM values, were performed to confirm participant eligibility. We then assigned the groups by a randomizer who was not involved in the study using Excel’s basic random number generator (randomization code), and the assignment of posterior fixation was then directed to the surgeon by the study site administrator immediately before surgery. We allocated the patients to either the UPS fixation group (UPS group) or the BPS fixation group (BPS group) (Figure 2). Patients were blinded to their assignment until after surgery. All surgical procedures were performed in accordance with ordinary LLIF procedures previously reported.10,11,21-24 Three spine surgeons primarily performed the surgery. Briefly, all patients were performed with a left-sided approach and underwent LLIF through a single incision, mini-open direct visualizing approach. We placed the patient in the lateral decubitus position, and an incision was made on the disc’s skin to be treated. After approaching the disc, we performed additional disc curettage and rasping of the endplates. The surgeon determined the appropriate cage size by combining preoperative images and intraoperative cage template findings and inserted the appropriate cage size. All cages were lordosis cages and were 18 mm wide. We have supplemented all LLIF segments with UPS or BPS fixation. At the surgeon’s discretion, PPS insertion was performed with the SPS technique in the lateral decubitus position or with the dual position (DPS) technique after repositioning in the prone position. Study design. Patients were randomized to the UPS or BPS group. UPS, unilateral PPS fixation; BPS, bilateral PPS fixation; IC, informed consent.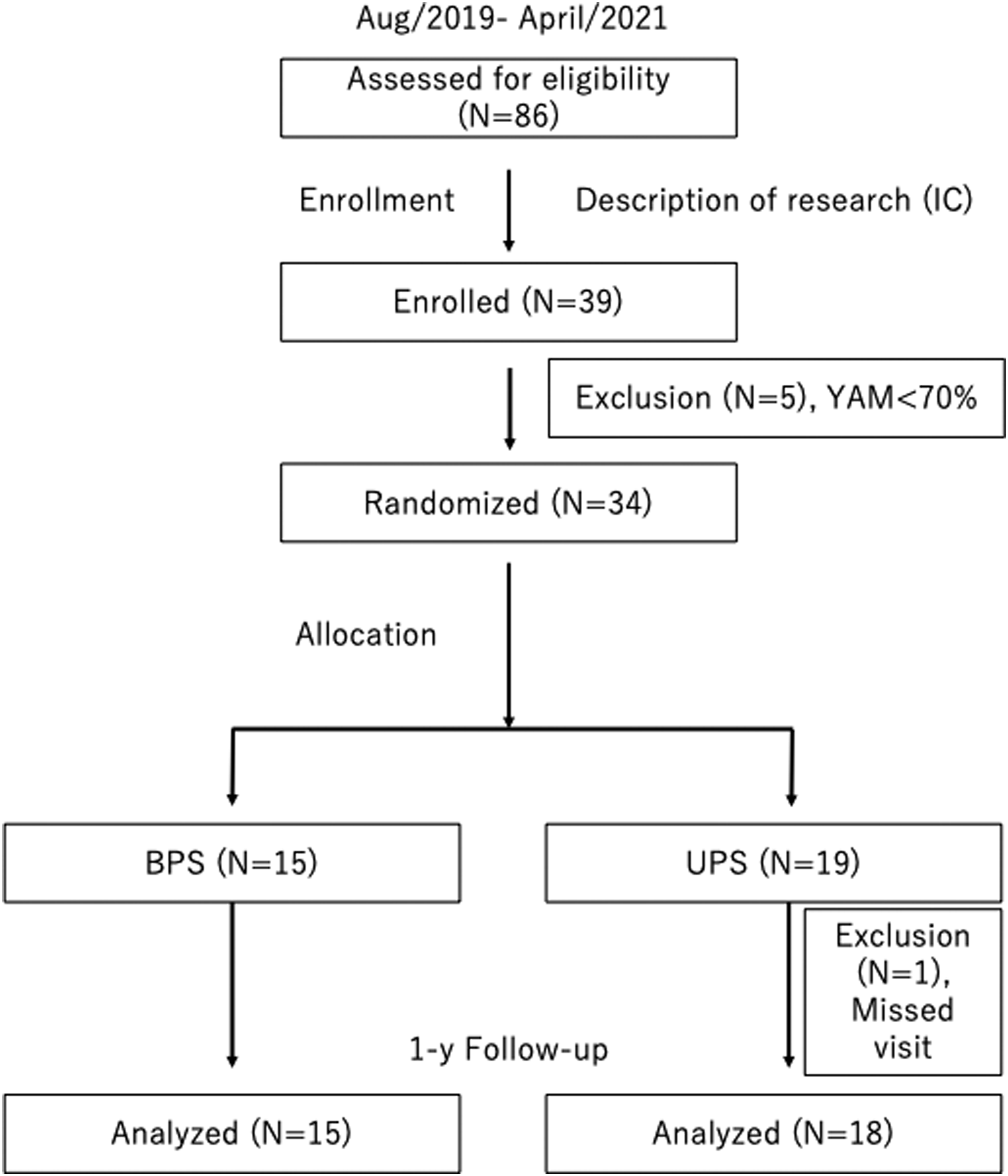
Outcomes
Our primary analysis, which was a per-protocol analysis, included patients who underwent the assigned surgery and completed the one -year follow-up. We used the change in the pain score from before to after the operation in the UPS and BPS groups as the study’s primary endpoint outcome. Secondary study measures included intraoperative outcomes, radiographic success, fusion rate, and complication profile.
Clinical Assessment
The data collected for analysis included demographics, fusion level, diagnosis, operative time, intraoperative blood loss, type of cage and PPS used, duration of hospital stay, and postoperative complications. All adverse and serious adverse events that occurred intraoperatively or during the follow-up were recorded by the investigators. We also evaluated patients who required additional surgery at one year after first surgery.
Clinical outcomes were assessed using a numeric rating scale (NRS) one year after the surgery. The 11-point numeric scale ranges from '0' representing one pain extreme (eg “no pain”) to '10' representing the other pain extreme (eg “pain as bad as you can imagine” or “worst pain imaginable”). The pain intensity before and after the operation was assessed using the NRS scores obtained for lower back pain (LBP; NRSLBP), leg pain (LP; NRSLP), and leg numbness (LN; NRSLN). Improvements in symptoms were evaluated by the change in NRS (ΔNRS), which was calculated as a one-year postoperative NRS score – preoperative NRS score). 25
Radiological Assessment
We assessed radiographic outcomes using standing radiographs before surgery and one year postoperatively. Sagittal parameters were defined as previously reported.26,27 We used standard measurements reported elsewhere to assess sagittal vertical axis (SVA), lumbar lordosis (LL; T12–S1), thoracic kyphosis (TK, T5-12), pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS).
About two weeks after the operation, we measured intervertebral disc height and segmental lordosis (SL) using CT scans. The intervertebral disc heights of anterior disc height (ADH) and posterior disc height (PDH) were evaluated, and average disc height [Av DH]) was defined as the average of the ADH and PDH. SL was determined according to the disc angle between lines perpendicular to the inferior end plate of the superior vertebra and the superior endplate of the inferior vertebra in each treated level. The symbol Δ indicates each change from before to after the operation.
We performed CT scans preoperatively and immediately postoperatively to assess cage position and to identify instrumentation failure and possible endplate injuries. The position of the interbody cage was assessed based on the locality of the midpoint of the cage relative to the inferior endplate length.
Intraoperative endplate injuries and cage subsidence were categorized as caudal (superior endplate) and/or cranial (inferior endplate) and classified using radiographs and CT scans according to the Marchi classification. 28 Briefly, Grade 0 is a loss of 0-24% of the postoperative DH, Grade 1 is 25-49%, Grade 2 is 50-74%, and Grade 3 is 75-100%. Cage subsidence was defined as early cage subsidence (ECS) if evidenced by radiographs and/or CT scans during hospitalization. On the other hand, if we did not find obvious evidence of endplate injury on radiographs and CT scans during hospitalization, subsidence detected on subsequent radiographs and/or CT scans was deemed delayed cage subsidence (DCS). 29 The criteria for determining bone fusion status from CT scans were the presence of a bony bridge in the sagittal and coronal reconstructed CT scans and its partial or complete connections to the lower and upper endplates, including around the cage. That is, our fusion criteria also included cases of partial fusion. If there was only partial fusion on the CT scan, additional radiographic confirmation of the presence of regional motion of <5° and intervertebral translation of <3 mm at 1 year after surgery was performed to assess bony union. 30
We performed MRI to determine the midsagittal canal diameter (CD) and axial central canal area (CCA) of the thecal sac before and within two weeks after surgery. 31 This study used a 1.5 or 3.0 T MRI system (Ingenia or Achieva; Philips Medical Systems, Best, the Netherlands). Two reviewers, who are also authors, determined the average image measurements used for the analyses.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics (version 23.0; IBM Corp, Armonk, NY, USA). All values are expressed as the mean (± standard deviation). The Shapiro–Wilk test was used to confirm the normality of the data distribution. For the primary analysis, we used Student’s t test or the Mann–Whitney U test to compare the two groups. Student’s t test was used to analyze normally distributed data, and the Mann–Whitney U test to analyze nonnormally distributed data. Comparisons of categorical variables between groups were assessed using Fisher’s chi-squared test. The significance of the obtained results was accepted at the 5% level.
Results
Characteristics of the Subjects in the Present Study.
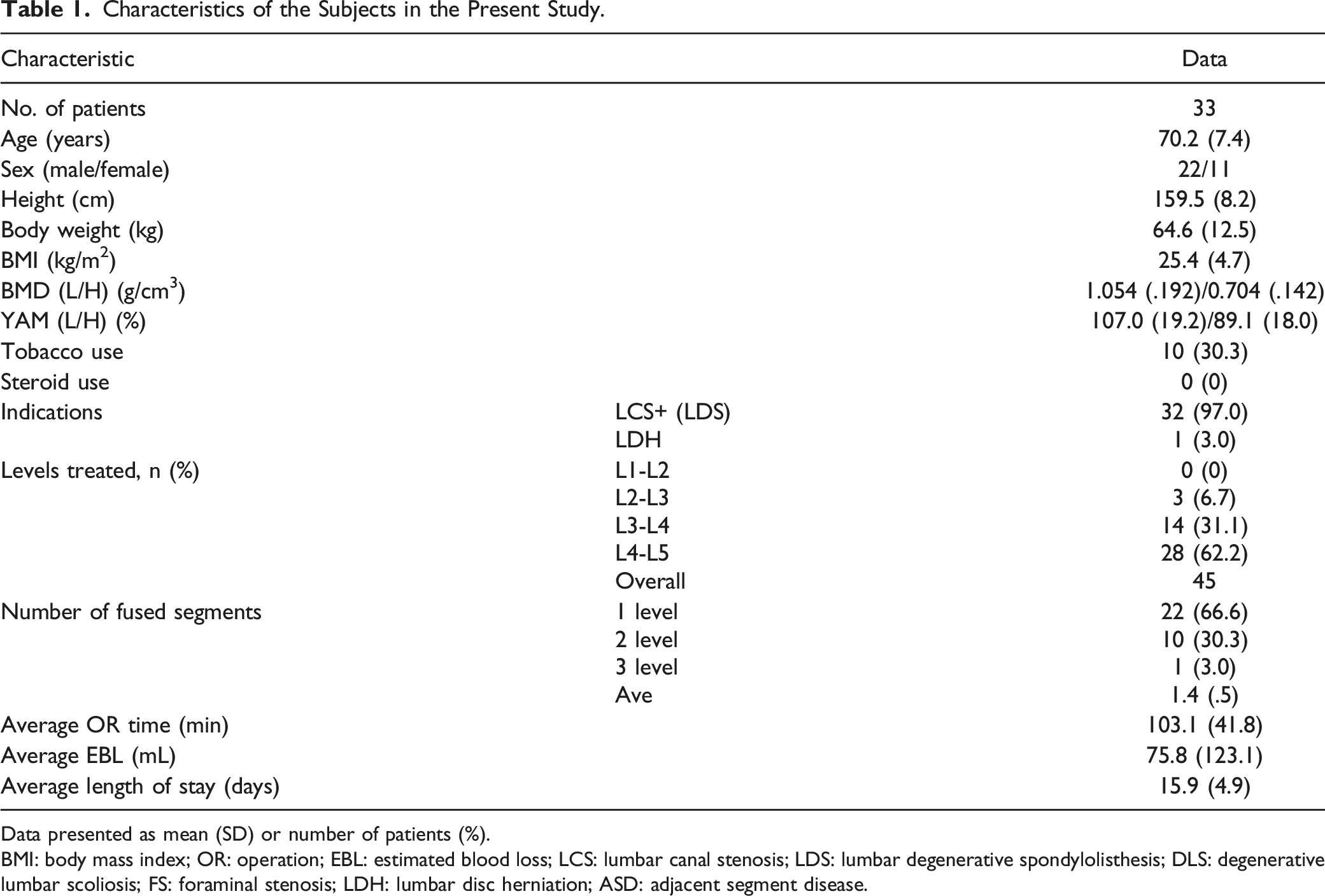
Data presented as mean (SD) or number of patients (%).
BMI: body mass index; OR: operation; EBL: estimated blood loss; LCS: lumbar canal stenosis; LDS: lumbar degenerative spondylolisthesis; DLS: degenerative lumbar scoliosis; FS: foraminal stenosis; LDH: lumbar disc herniation; ASD: adjacent segment disease.
Comparison of Two Groups.
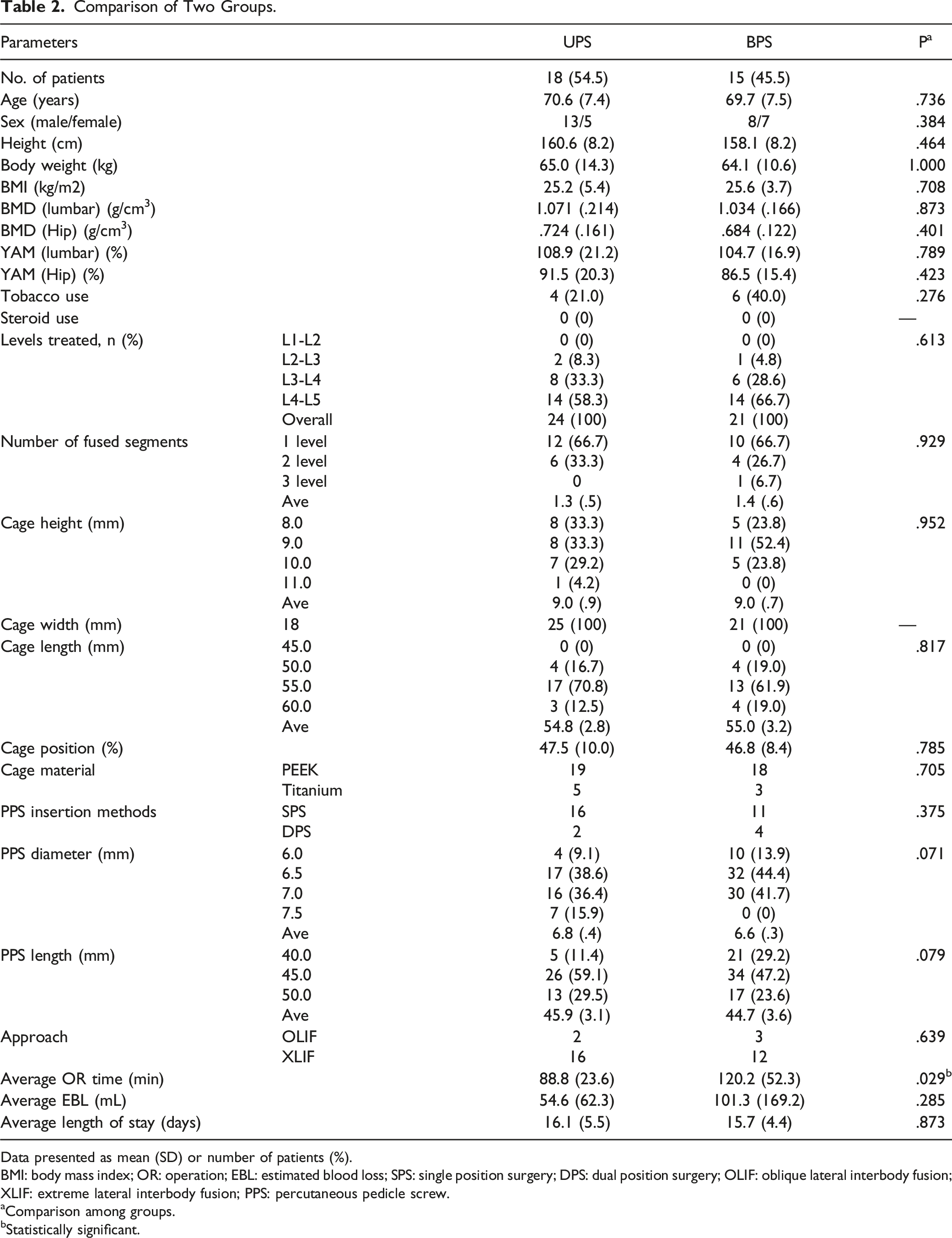
Data presented as mean (SD) or number of patients (%).
BMI: body mass index; OR: operation; EBL: estimated blood loss; SPS: single position surgery; DPS: dual position surgery; OLIF: oblique lateral interbody fusion; XLIF: extreme lateral interbody fusion; PPS: percutaneous pedicle screw.
aComparison among groups.
bStatistically significant.
Preoperative, Postoperative, and Change From Pre-to Postoperative Sagittal Measurements.
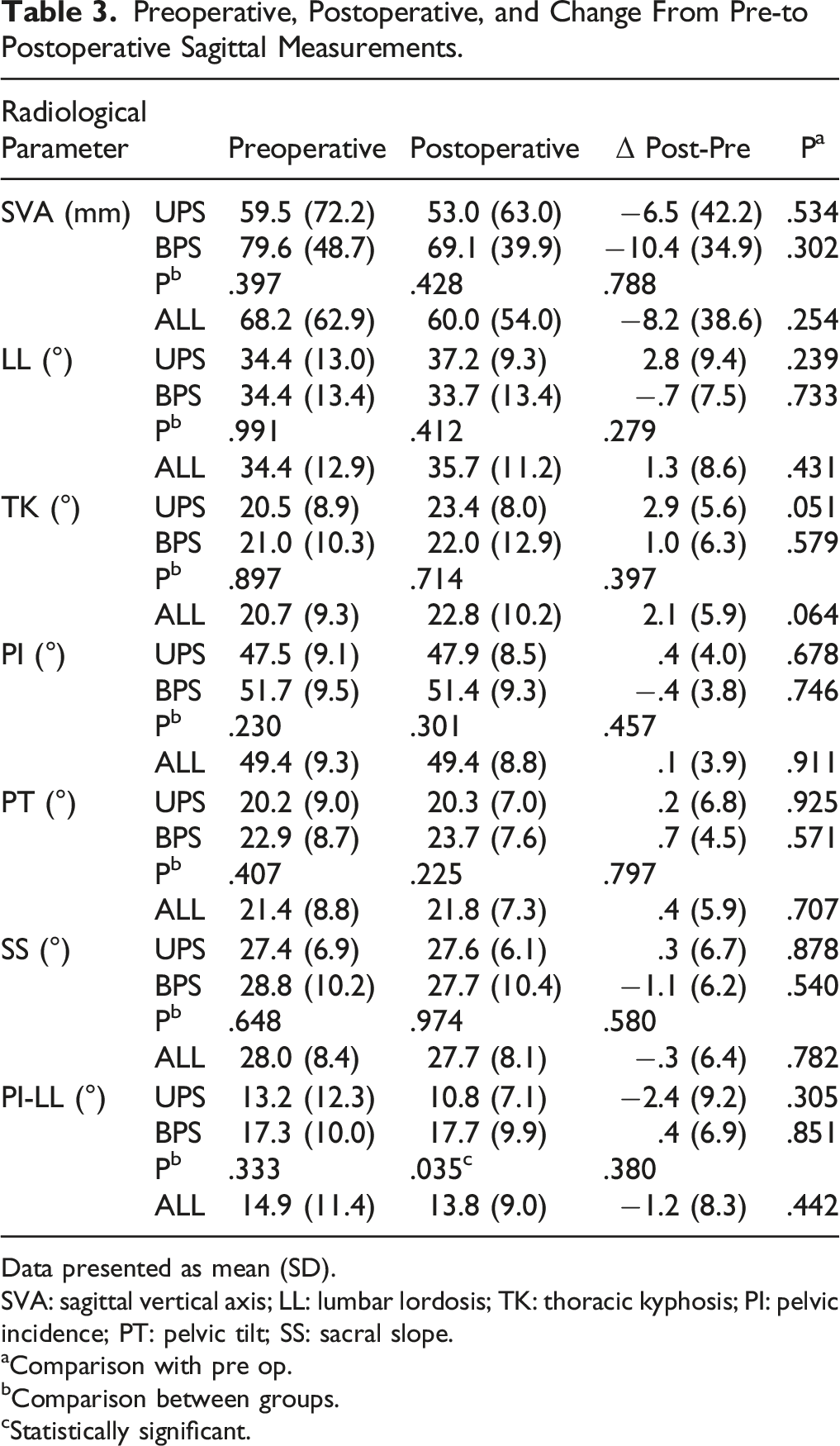
Data presented as mean (SD).
SVA: sagittal vertical axis; LL: lumbar lordosis; TK: thoracic kyphosis; PI: pelvic incidence; PT: pelvic tilt; SS: sacral slope.
aComparison with pre op.
bComparison between groups.
cStatistically significant.
Preoperative, Postoperative, and Change From Pre-to Postoperative Sagittal Measurements.
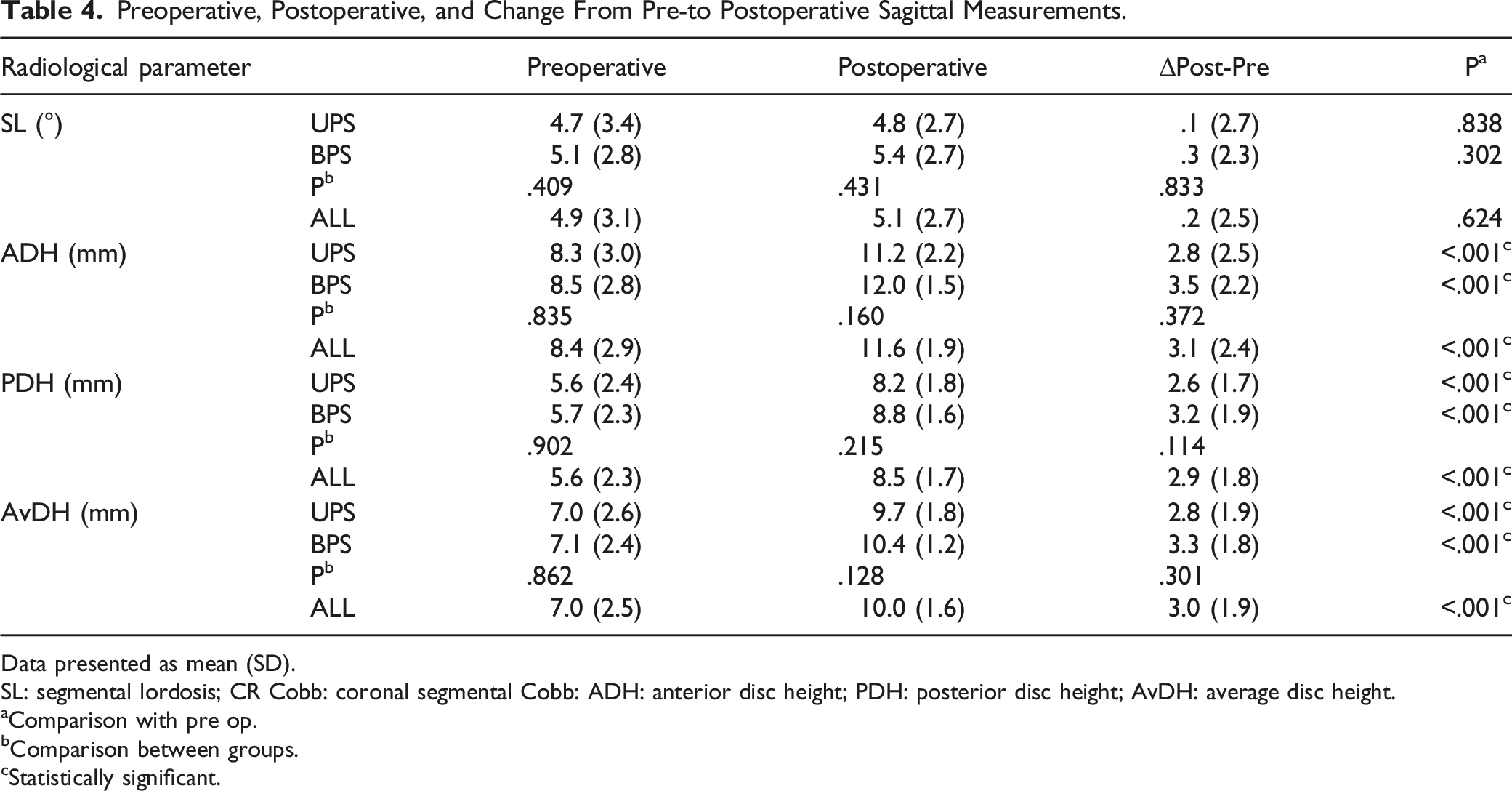
Data presented as mean (SD).
SL: segmental lordosis; CR Cobb: coronal segmental Cobb: ADH: anterior disc height; PDH: posterior disc height; AvDH: average disc height.
aComparison with pre op.
bComparison between groups.
cStatistically significant.
Radiographic Measures-Canal Dimension (Canal Diameter and Central Canal Area of Dural sac) Changes Evaluated on Pre-and Postoperative MRI.
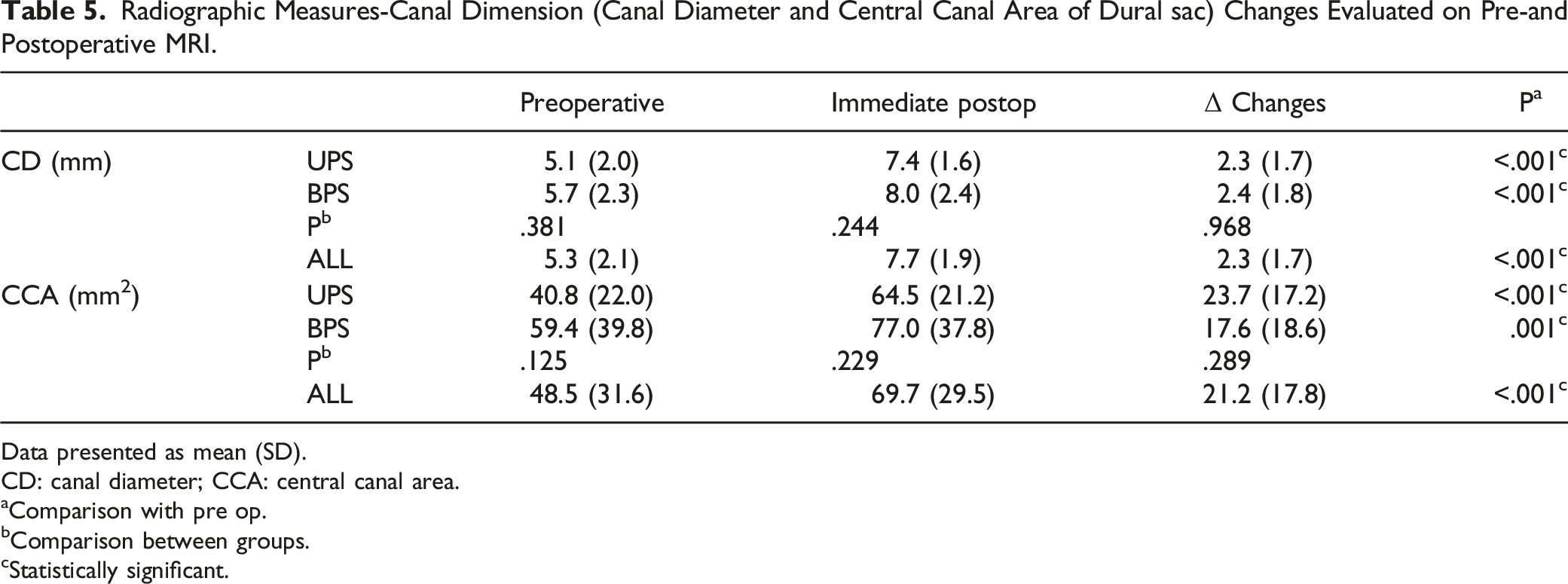
Data presented as mean (SD).
CD: canal diameter; CCA: central canal area.
aComparison with pre op.
bComparison between groups.
cStatistically significant.
Comparison of Complications Between the Two Groups.
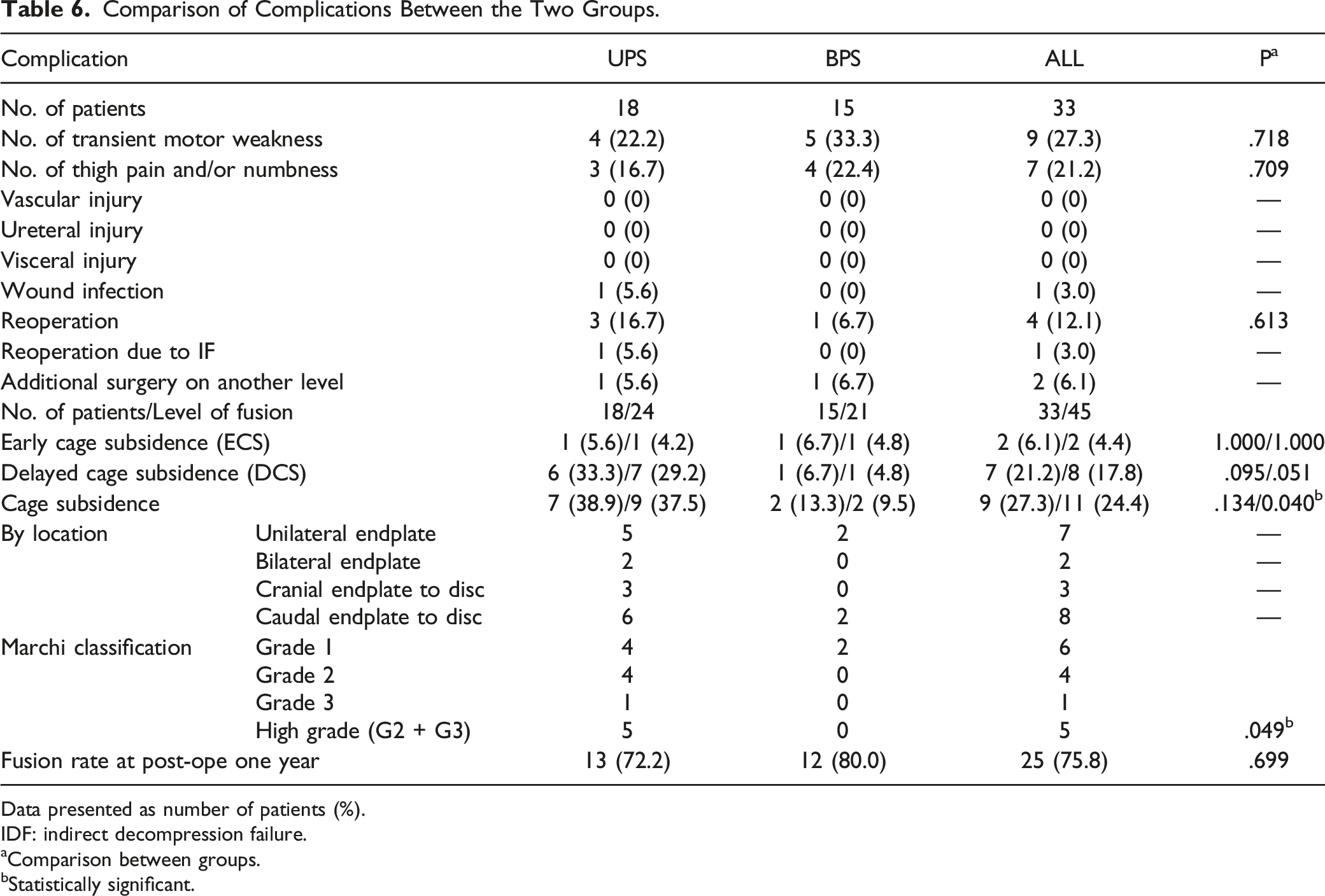
Data presented as number of patients (%).
IDF: indirect decompression failure.
aComparison between groups.
bStatistically significant.
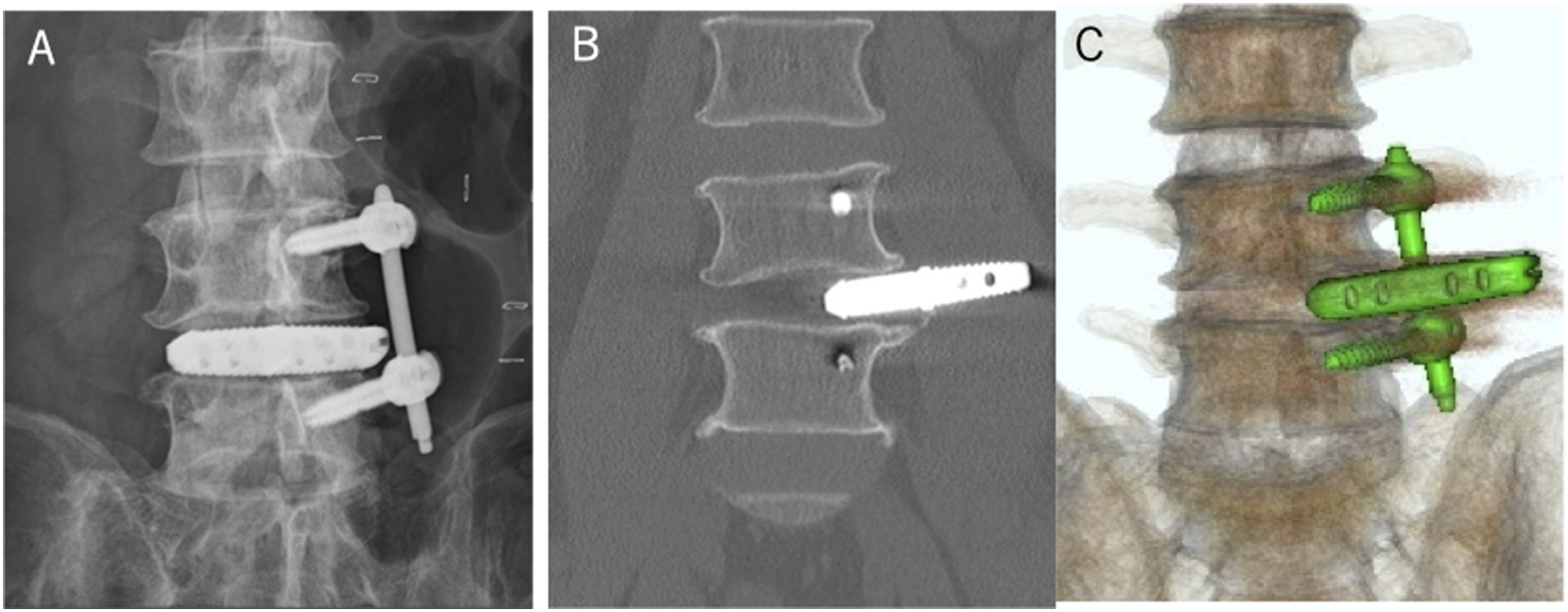
Cage prolapse after LLIF with unilateral PPS fixation at L4/5 segment in a 74-year-old man. (A) Anteroposterior radiographs images on the day after surgery. (B) Coronal CT image 1 week after surgery. (C) Coronal three-dimensional (3D) reconstruction CT image 1 week after surgery. LLIF, lateral lumbar interbody fusion.
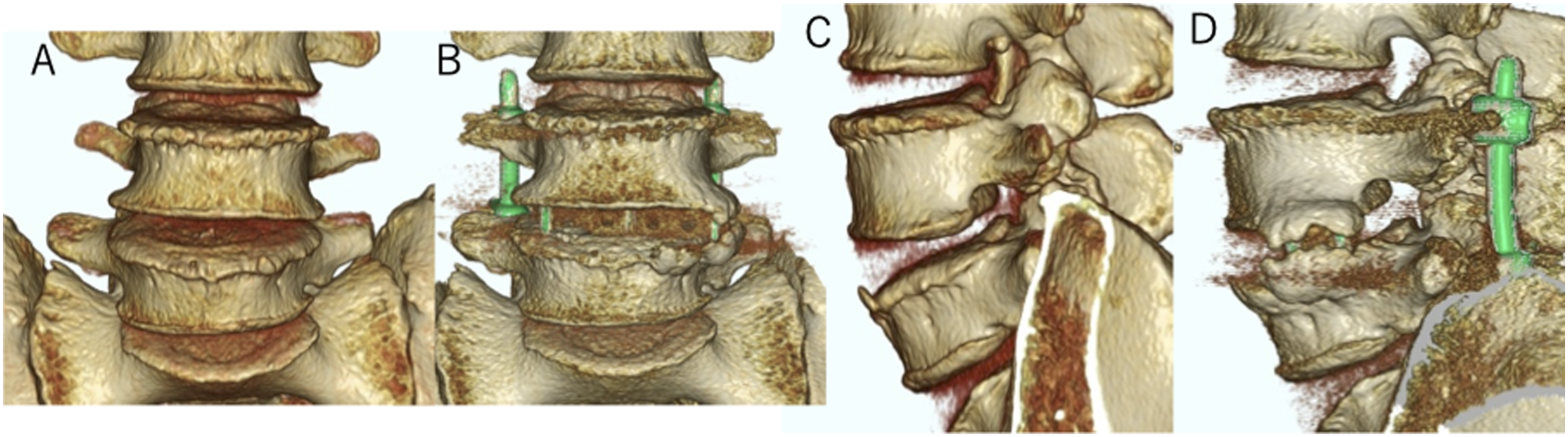
ECS was observed in two patients and two levels, and DCS was observed in seven patients and eight levels. Cage subsidence, including ECS and DCS, was found in eleven levels in nine patients, which differed significantly between the two groups at the intervertebral level (P = .040). High-grade cage subsidence (Marchi classification Grade 2 or 3) was observed in the UPS group (P = .049). A typical example of cage subsidence is shown in Figure 4. The fusion rate was judged from the CT scans (Figure 5) and radiographs one year postoperatively. Twelve patients in the BPS group and 13 in the UPS group achieved fusion one year after the operation. The fusion rate was 80% in the BPS group and 72% in the UPS group (P = .699). Comparison of preoperative (A and B), postoperative (C and D), and 1-year (E and F) anteroposterior and lateral views after lumbar interbody fusion at L3/4 segment in a 74-year-old woman with lumbar canal stenosis. Evaluation of bone fusion using 3D reconstruction CT image, showing bone bridging at L4/5 segment. (A) Preoperative coronal image. (B) Postoperative coronal image. (C) Preoperative sagittal image. (D) Postoperative sagittal image.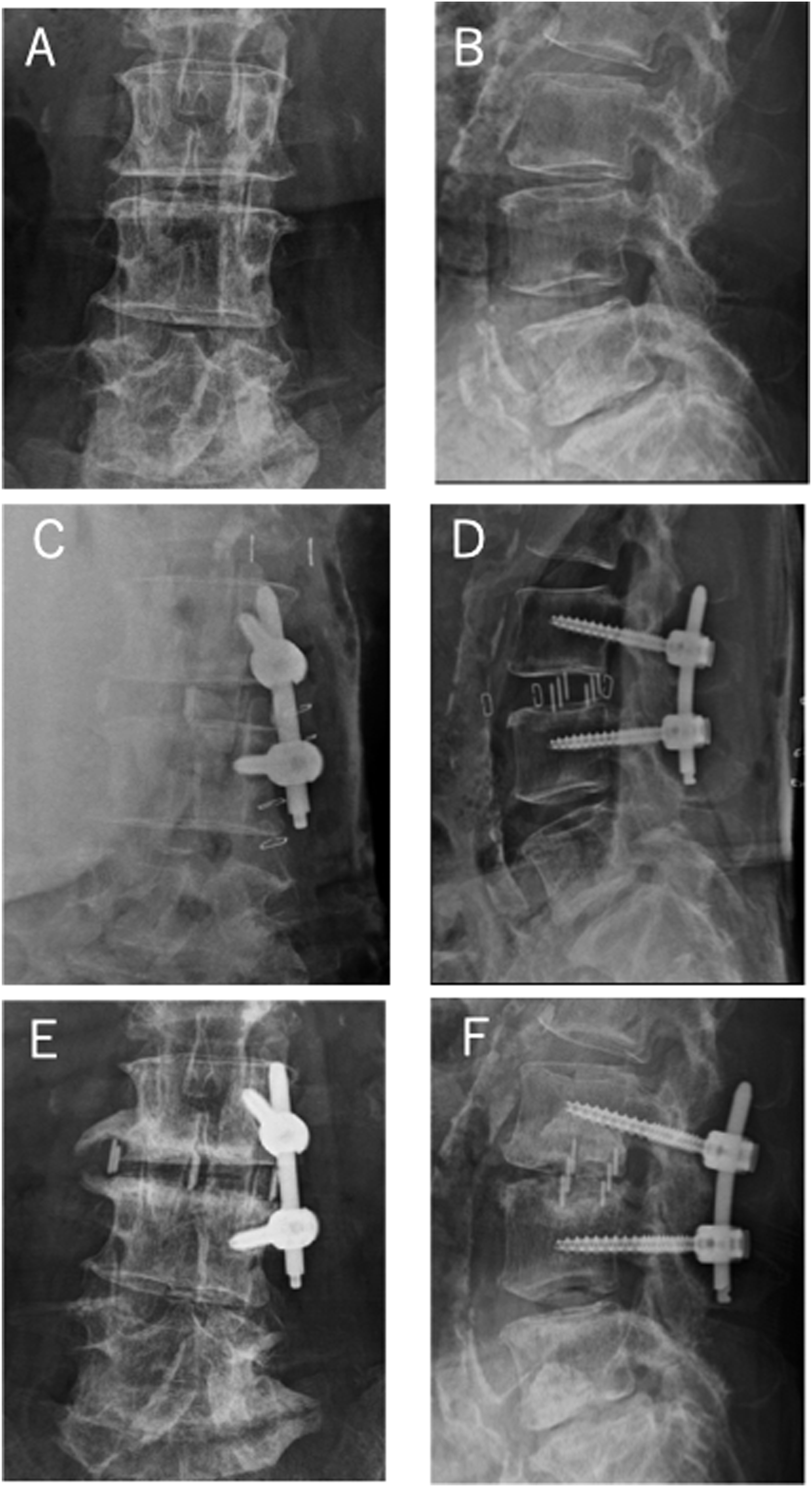
Pain Intensity for Each Group.
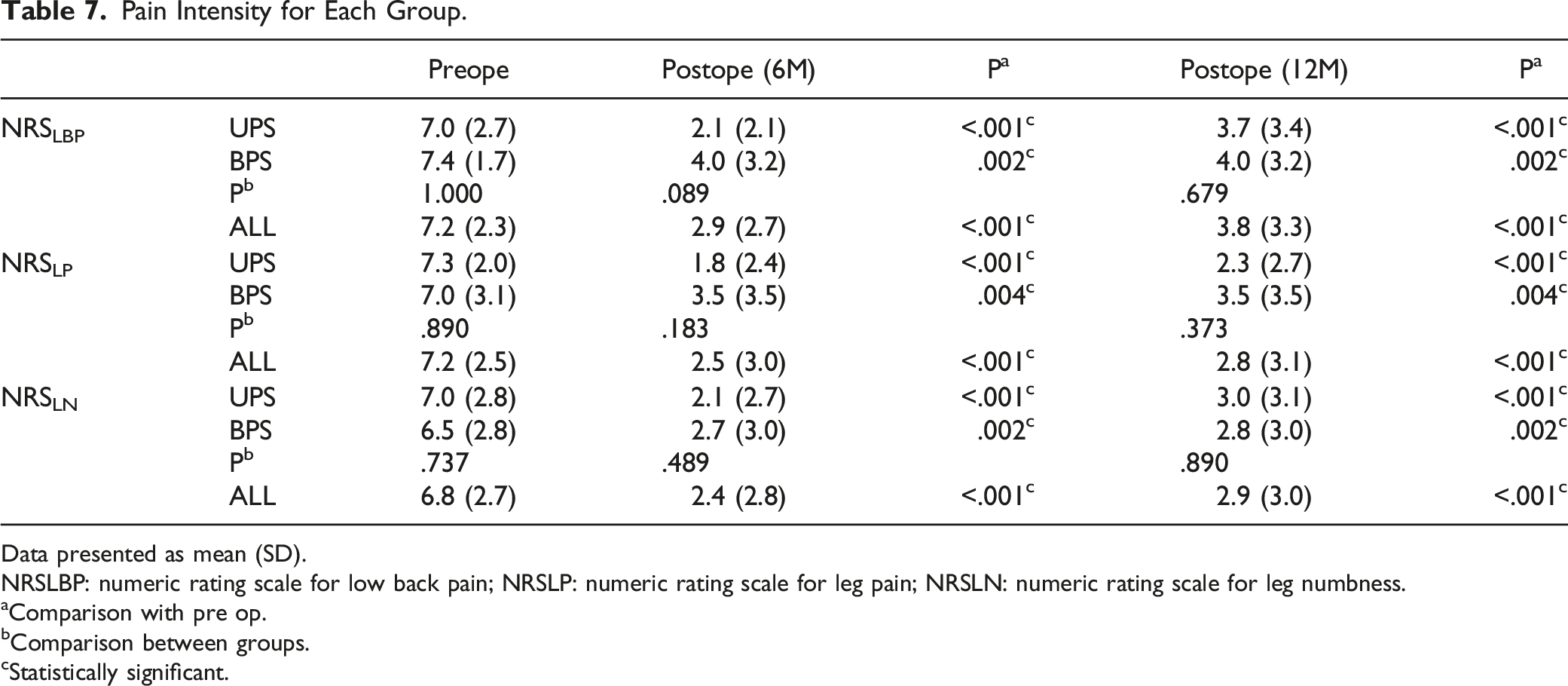
Data presented as mean (SD).
NRSLBP: numeric rating scale for low back pain; NRSLP: numeric rating scale for leg pain; NRSLN: numeric rating scale for leg numbness.
aComparison with pre op.
bComparison between groups.
cStatistically significant.
Discussion
We first investigated short-term radiography, clinical outcomes, and some complications of LLIF in short-term spinal fusion between UPS and BPS fixation in a prospective randomized clinical trial. LLIF with UPS fixation obtained similar alignment and indirect decompression in a shorter operation time than BPS fixation. Moreover, the pain one year after surgery for the study’s primary endpoint did not differ between patients treated with LLIF with UPS fixation and those treated with BPS fixation. However, severe cage subsidence was observed in the UPS group.
The need for unilateral or bilateral screw instrumentation for lumbar fusion is controversial. Earlier studies compared the need for either unilateral or bilateral PPS instruments for posterior fusion. This issue is also controversial for LLIF techniques, and comparisons with the stand-alone LLIF, which does not require posterior instrumentation, are needed. In LLIF, the addition of unilateral and bilateral PPS fixation significantly decreases the range of motion compared with stand-alone cages.33-35 Fukushima et al reported a shorter operative time for LLIF surgery with UPS fixation than this surgery with BPS fixation. 19 However, LLIF with UPS fixation might require additional surgery. Thus, they have reported that unilateral pedicle screw instrumentation should be confined to a single-level lumbar interbody fusion and should not be used for multi-level fusion because of inadequate fixation strength. This means that the surgeon must choose a fusion option for each patient according to these research results. However, it remains difficult for surgeons to determine the optimal fixation option because of varying ages and genders and the presence of osteoporosis. To resolve this issue, we compared the first radiographic and clinical outcomes of LLIF with UPS vs BPS fixation for LDD in this prospective randomized clinical trial. Our findings suggest no statistical difference in clinical, most radiographic, and canal dimension data. However, more occurs in cage subsidence of high-grade in UPS groups. Compared with BPS fixation, the LLIF with UPS fixation may not have been enough to stabilize the lumbar spine. Of the patients treated with LLIF with UPS fixation, only one had reoperation due to a loose cage. Thus, we cannot draw firm conclusions based on one patient with LLIF with UPS fixation results. Additionally, we have not performed any compression forces between the screws to achieve indirect decompression for all patients. Of course, we must consider the possibility of the cage becoming loose because of this technical problem.
A systematic review has suggested that the cage subsidence and graft failure rates after LLIF are inversely related to bone density. 36 Therefore, we evaluated the YAM values in patients and excluded those with osteoporosis from this prospective study. In a short-term study, improvements in LBP, LP, and LN were similar in patients who underwent LLIF with UPS fixation as in those treated with BPS fixation. These results suggest that, over the short term, LLIF with UPS fixation may reduce surgical invasiveness and avoid muscle damage, leading to similar clinical outcomes as BPS fixation. However, we have observed high-grade cage subsidence in the group treated with UPS fixation, which suggests that UPS fixation may not be sufficient. In the long-term, there are concerns about the possibilities of indirect decompression failure caused by cage subsidence and radiculopathy because of the progression of coronal and/or sagittal deformity. Therefore, it may be better in the long term to perform the LLIF procedure with BPS fixation in patients with or without osteoporosis. Against this background, we have decided to discontinue the study, as we fear that continuing the UPS procedure may be detrimental to patients who participate in the study in the future.
This study has some limitations. First, the number of cases in each group was small, and the follow-up period of one year was short. Future studies with a longer follow-up and larger study populations must identify the clinical and radiological signs of scoliotic changes after UPS fixation with LLIF. We found that severe cage subsidence occurred in the short term in the group treated within the UPS fixation and that this may have resulted from insufficient fixation. Therefore, we have decided to discontinue this prospective randomized study, given the concerns about possible long-term harm to patients. Second, although this was a prospective randomized trial, the study population was somewhat heterogeneous in terms of the diagnoses, age and sex distributions, and surgical segment. The heterogeneity of the study group may affect postoperative outcomes. However, the two groups did not differ significantly. We should target future research more precisely, although this may mean fewer patients. This is the limit of single-center research. Third, we performed per protocol analysis by excluding patients who deviated from the protocol. Therefore, the existence of attrition bias is suspected. The per-protocol analysis may exaggerate the effect of treatment compared to the intention to treat analysis. Fourth, there is the issue of medical insurance. The length of hospital stay in our patients is due to differences in medical insurance from country to country. Fifth, although there are various risk factors for cage subsidence, we did not perform multivariate analysis in this study. The reason is the not purpose of this study and/or the small number of patients. However, the UPS group had significantly more cage subsidence, although there was no statistically significant difference in BMD, YAM, and postoperative DH values between the two groups. Sixth, this study did not include third-party reviewers who did not participate in surgical treatment and performed separate radiological evaluations and statistical analyzes to reduce bias. Finally, differences in surgical technique in the LLIF procedure may have contributed to the results. However, the surgeon who performed the surgery has >10 years of experience in spine surgery and is an instructor about the spine. Despite these limitations, this prospective study provides valuable information about the presence or absence of clinical posterior fixation during LLIF.
Conclusions
LLIF with UPS fixation reduced the operative time compared with BPS fixation. Short-term postoperative pain scores and bone union rates did not differ significantly between the two groups, but LLIF with a UPS fixation had more severe cage subsidence. In the long-term, this may lead to the failure of indirect decompression by LLIF. Therefore, it may be necessary to carefully judge the selection of UPS fixation at the time of LLIF in short-level spinal fusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.