
Abstract
Study Design:
Retrospective database study.
Objectives:
To compare the accuracy and safety of 2 types of a computer-assisted navigation system for percutaneous pedicle screw placement during endoscopic lumbar interbody fusion.
Methods:
From May 2019 to January 2020, data of 56 patients who underwent Endo-LIF with a robot-assisted system and with an electromagnetic navigation system were compared. The pedicles in all patients were subjected to postoperative CT scan to assess screw correction by measuring the perpendicular distance between the pedicle cortical wall and the screw surface. The registration and matching time, guide-wire insertion time, the entire surgery time, and X-ray exposure time were recorded.
Results:
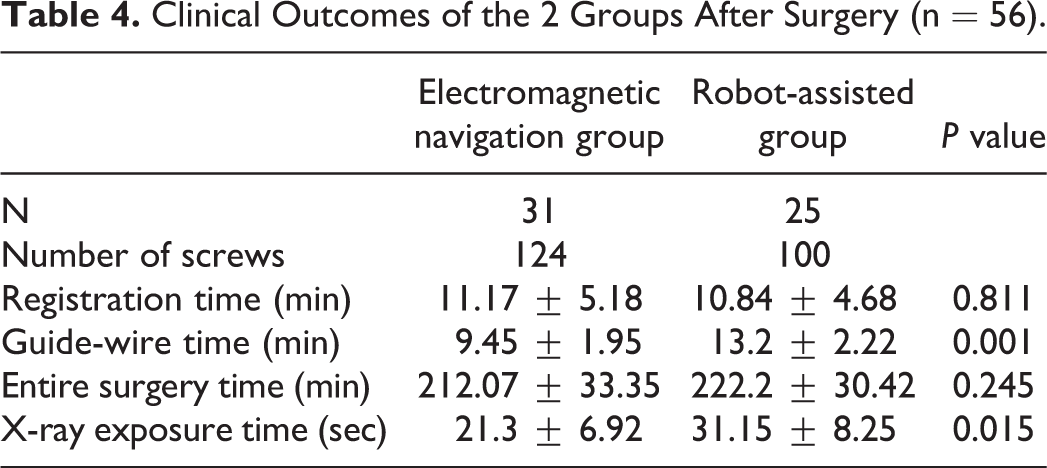
In the robot-assisted group, 25 cases with 100 percutaneous pedicle screws were included, and the excellent and good rate was 95%. In the electromagnetic navigation group, 31 cases with 124 screws were included, and the excellent rate was 97.6%. There was no statistical difference between the two groups (P > 0.05). The registration time and the total time for the surgery also showed no statistical differences (P > 0.05). The main difference between the two groups was the guide-wire insertion time and the X-ray exposure time (P < 0.05).
Conclusions:
Both electromagnetic navigation and robot-assisted are safe and efficient for percutaneous pedicle screw placement. Electromagnetic navigation system has obvious advantages over robot-assisted in terms of faster guide-wire placement and less X-ray exposure. Robot-assisted for percutaneous pedicle screw placement offers a preoperative planning system and a stable registration system, with obvious drawbacks of a strict training curve.
Introduction
Endoscopic lumbar interbody fusion (Endo-LIF), such as minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) for the treatment of lumbar spondylolisthesis, has been widely used over the past 2 years, with obvious advantages of lower soft tissue damage, lower blood loss, lower complication rate, faster recovery speed, and shorter hospital stay. 1 However, several factors, such as low efficiency, long learning curve, difficult pedicle screw insertion, and high X-ray exposure, hinder its development. Percutaneous pedicle screw placement is one of the key factors in Endo-LIF that should be performed precisely and efficiently.
As is well known, the optical navigation method, a representative of the computer-assisted navigation system, has been widely used to assist in the insertion of normal pedicle screws in an open surgery and of percutaneous pedicle screws in a minimally invasive spine surgery (MISS), with obvious advantages when compared with the free hand technique.2,3 To improve the accuracy and avoid hinderance in optical navigation, other stable navigation systems have been developed; electromagnetic navigation system and robot-assisted system are typical examples.
In the past year, we attempted one type of novel electromagnetic navigation to improve the efficiency of percutaneous pedicle screw placement and Endo-LIF. We herein conducted a retrospective study to compare electromagnetic navigation with robot-assisted to help spine surgeons become familiar with the differences between each of the systems used in MISS.
Materials and Methods
Patients
From May 2019 to January 2020, 56 patients were selected based on the inclusion and exclusion criteria, and they received Endo-LIF from a spine surgeon with one fellow doctor. For the first 25 cases, a robot-assisted, known as the renaissance robot, from Israel was used to help with percutaneous pedicle screw placement; and for the next 31 cases, a novel electromagnetic navigation (Fiagon GmbH, Hennigsdorf, Germany) based on electromagnetic field (EMF) was used. Basic information, including age, gender, duty level, and spondylolisthesis classification, is presented in Table 1. Intraoperative real-time anteroposterior and lateral (AP & Lat) X-ray fluoroscopy was used for system registration and screw position confirmation. The pedicles in all patients were subjected to postoperative 3-dimensional (3D) reconstructed computed tomography (CT) to assess screw correction by measuring the perpendicular distance between the pedicle cortical wall and the screw surface. This retrospective study was approved by the Affiliated Hospital of Qingdao University, and informed consent was obtained from all the participants.
Basic Information About the Patients (n = 56).
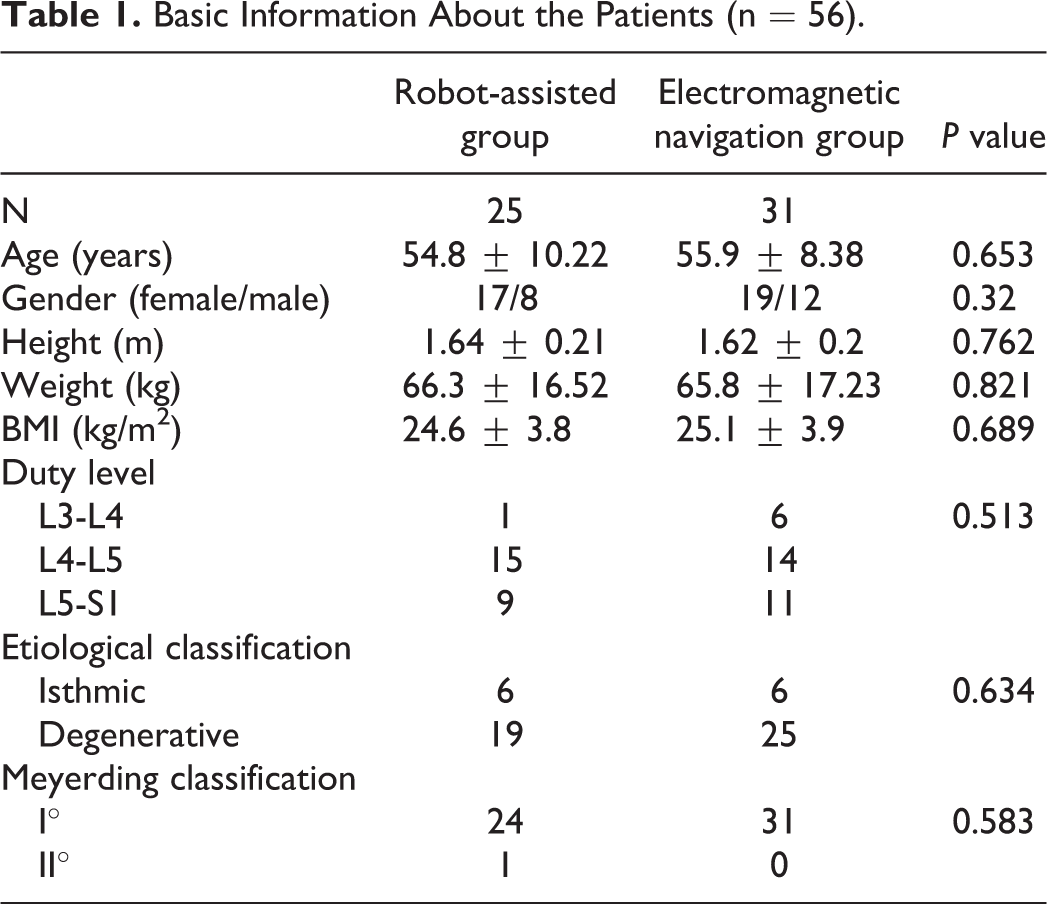
The inclusion criteria were as follows: (1) single-segment lumbar spondylolisthesis with Meyerding stage I or II; (2) persistent, severe low back pain and sciatica or neurogenic intermittent claudication, along with no response to standardized conservative treatment and severely affected daily life and work; (3) preoperative flexion-extension radiographs, CT, and magnetic resonance imaging (MRI) showing isthmic or degenerative spondylolisthesis with instability, lateral recess, and foraminal stenosis; and (4) no obvious decline in muscle strength and cauda equina syndrome. The exclusion criteria were as follows: (1) revision history in the duty level; (2) spondylolisthesis combined with infection, trauma, scoliosis, osteoporosis, kyphosis, and tumors; (3) severe central canal stenosis or bilateral recess stenosis; and (4) cerebrovascular and cardiovascular diseases that make the patient intolerant to operation.
Surgical procedure
Before the surgery, 3D reconstructed CT scans with a slice thickness of less than 1 mm were performed for the 2 groups; the scan reports were used to match with the intraoperative X-ray fluoroscopy. The robot-assisted needed anteroposterior and 60° oblique X-ray films for registration, and a surgical planning system was used to determine the entry point, diameter, and direction of the trajectory. Electromagnetic navigation, however, only needed intraoperative AP and Lat X-ray films for image matching. The CT dataset was stored in DICOM format and copied onto a workstation for further processing. Surgery was performed in the operating room with a strictly sterile environment. Patients were kept in the prone position with the abdomen unsupported. General anesthesia was achieved in all the cases, except for one in the electromagnetic navigation group for which local anesthesia was achieved using a mixed solution of 20 ml of 2% lidocaine, 10 ml of 1% ripovacaine, and 30 ml of normal saline, owing to the contraindications to intravenous anesthesia. Intraoperative spinal monitoring was also necessary to avoid nerve root injury in the early stage. Before Endo-LIF, the guide-wire of the percutaneous pedicle screw was inserted first with the help of electromagnetic navigation or robot-assisted via a Jamshidi needle. The guide-wire location was verified by X-ray fluoroscopy confirmation to improve the one-time success rate of pedicle screw insertion. Then, canal decompression, discectomy, reduction, and interbody fusion under full-endoscopy were performed in sequence, following which percutaneous pedicle screws were inserted along the guide-wire to pull the dislocation again and to fix the duty level. In most cases, no drainage tube was necessary, and only 2 or 4 small incisions were left. Antibiotics were used no more than 24 h. On day 2 postsurgery, all patients could get out of bed with the help of a thoracolumbar brace. To eliminate bias, the team, the operating room and bed, and the type of minimally invasive percutaneous pedicle screw system (China) used were the same for all groups.
Procedure of Percutaneous Pedicle Screw Placement in the Robot-Assisted Group
Before the operation, the surgical plan, including the trajectory of the screw, the distance from the entry point to the middle line, and the pedicle shape, were verified at the workstation based on preoperative 3D CT (Figure 1). For the percutaneous procedure, a specialized working platform, known as hover-T, and the corresponding accessories were selected (Figure 2). Anteroposterior and 60° oblique high quality X-ray images were obtained and transferred to a workstation (Figure 3). The robot system calculated and verified the preoperative CT data. Minor adjustment or re-registration of the trajectory was required, at times. The robot was aseptically packed and fixed on the platform and could automatically adjust according to the surgical plan (Figure 4). An incision was made mechanically, and a depth-limited electric drill was used to tap in the pedicle guided by the robot arm. The guide-wires were inserted, followed by endoscopic decompression, discectomy, and interbody fusion. Percutaneous pedicle screw placement was the final step and checked again by X-ray fluoroscopy (Figure 5).
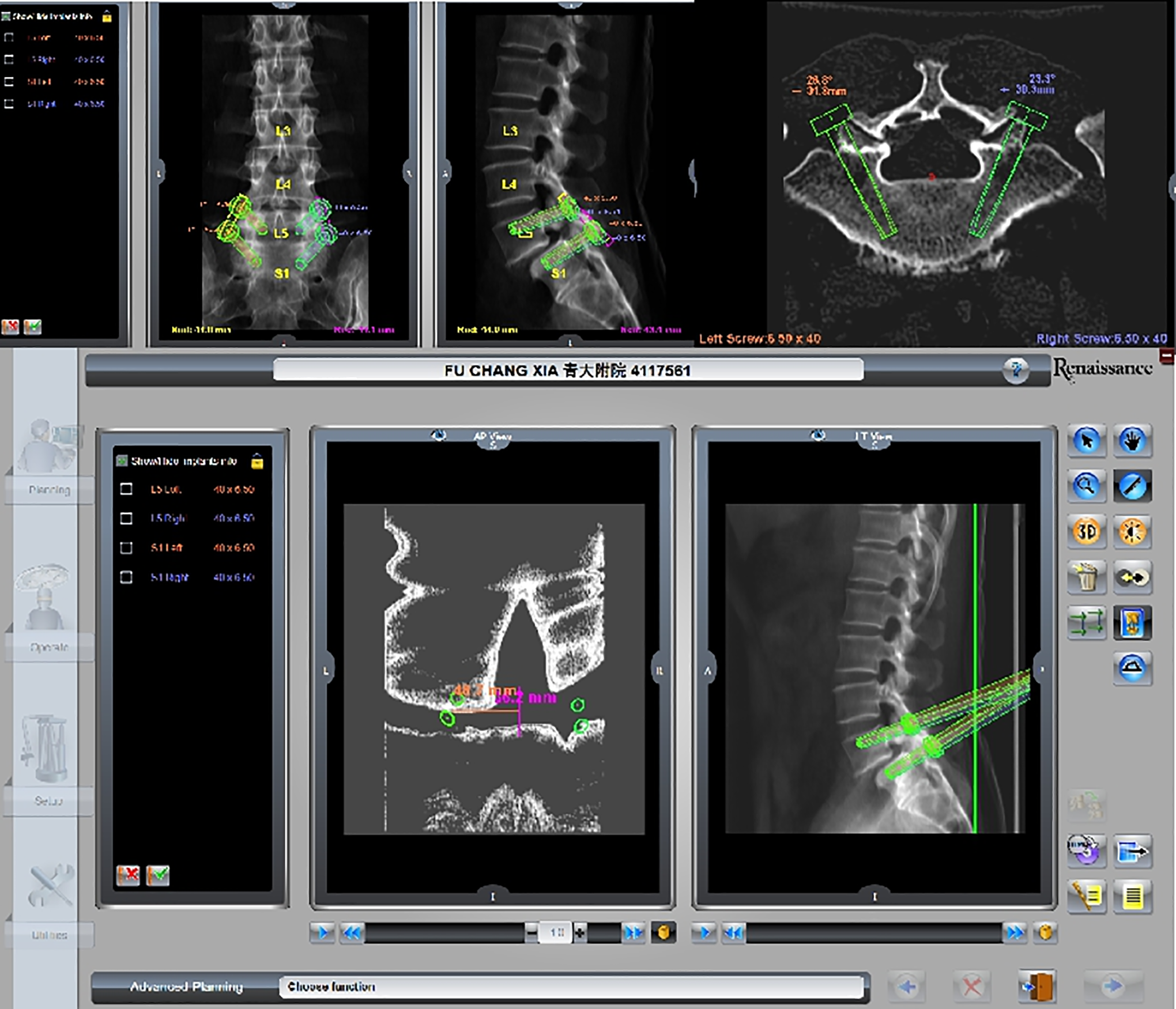
Surgical plan was prepared according to preoperative 3D CT. The reasonable angle of left S1 pedicle screw was 26.8°, appropriate length was 40 mm, diameter was 6.50 mm, and the distance from the entry point to the middle line was about 48.7 mm.
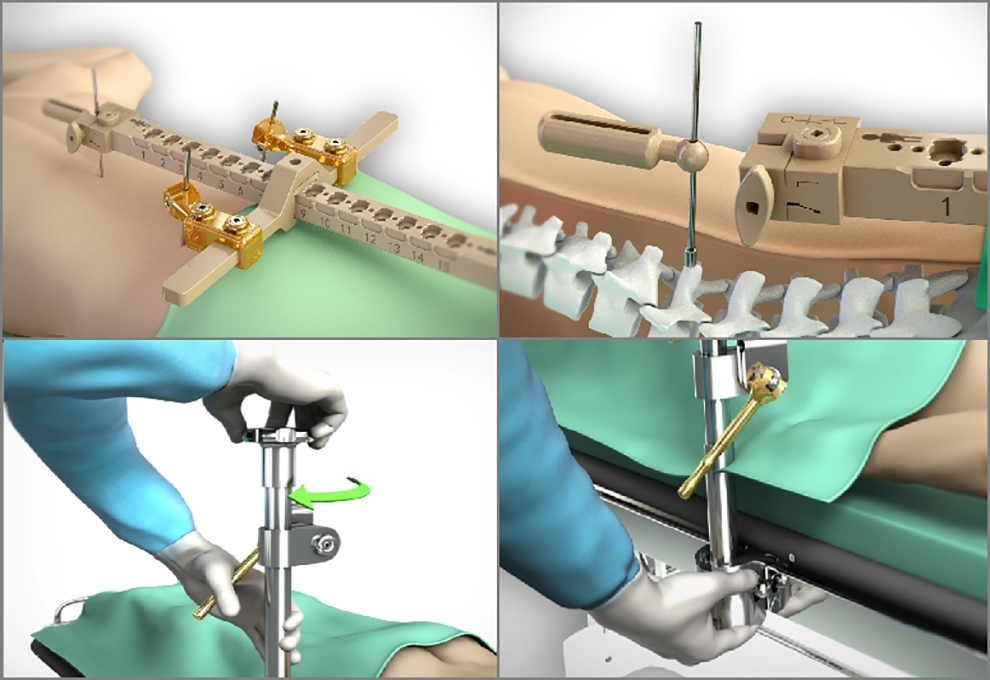
Hover-T and other parts were selected and installed.
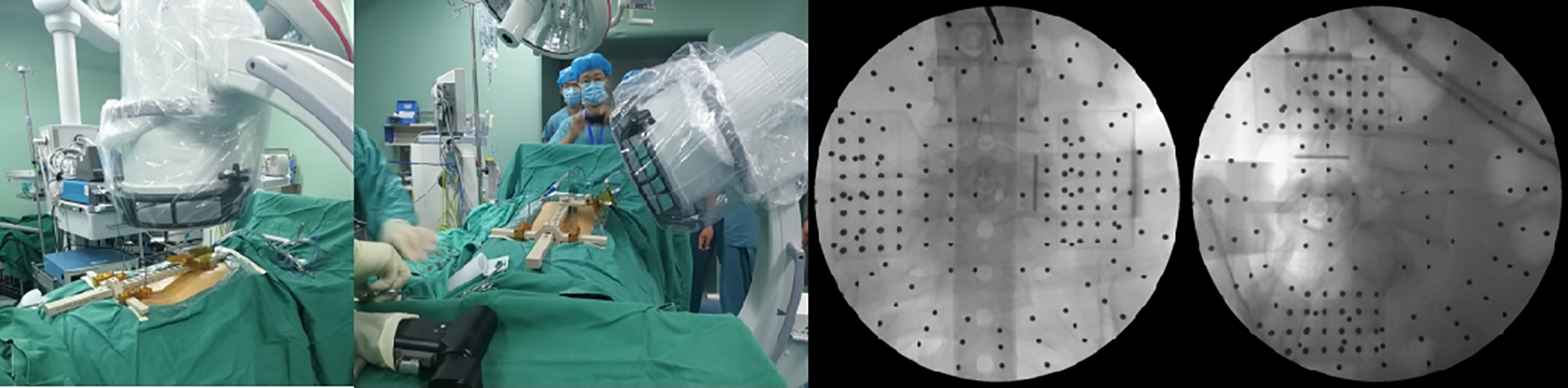
Anteroposterior and 60° oblique X-ray images were obtained and transferred to a workstation.

Robot was aseptically packed and fixed on the platform to automatically move. The incision was made and the depth-limited electric drill was used to tap into the pedicle guided by the robot arm.
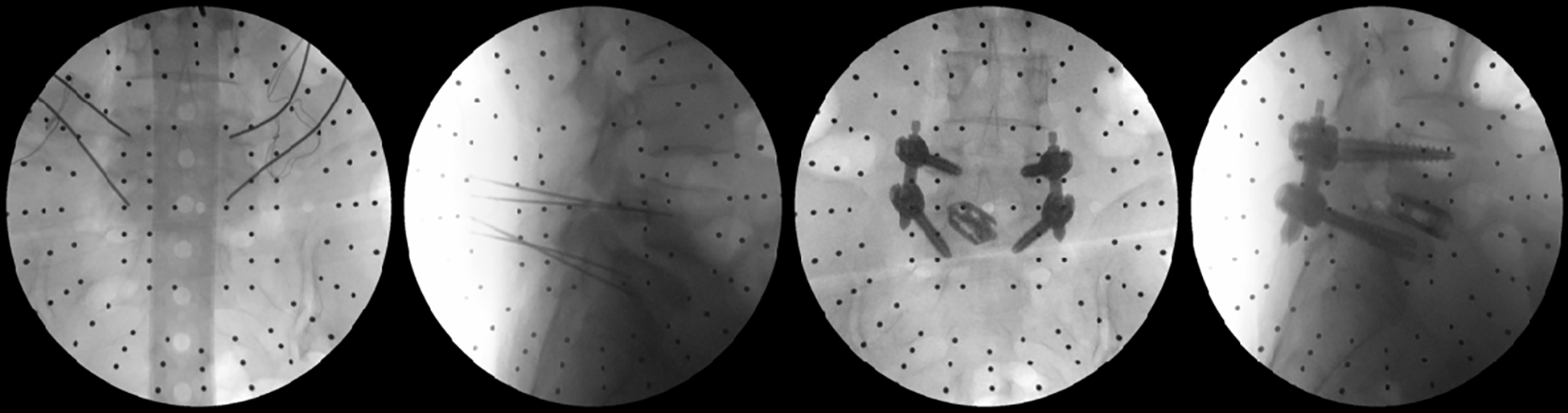
The guide-wires were always inserted, followed by decompression, discectomy, interbody fusion, and the last step would be percutaneous pedicle screw placement, which should be verified by anteroposterior and lateral X-ray fluoroscopy.
Procedure of Percutaneous Pedicle Screw Placement in the Electromagnetic Navigation Group
A new electromagnetic navigation system (Fiagon GmbH) based on EMF and adapted for spine surgery was tested. A special field generator was used to generate the EMF. All required and specially developed instruments were free from ferromagnetic substances to prevent measurement and instrument errors; thus, navigable screwdrivers were developed with titanium-alloy.
The field generator was placed close to the button (non-sterile area) so that the frame encompassed the entire surgical field (Figure 6). The EMF had a spherical size of 500 mm, which facilitated the generation of EMF that could be detected by the instruments fitted with signal coils. To match the generated EMF with the image dataset and the spine of the cadaver, a reference coil, called the patient tracker, was inserted firmly into the spinous process by a short, thin K-wire similar to the bone pin (Figure 7). A Mapper bridge with 17 mapping points was placed on the lower back and standard anteroposterior, and lateral X-ray films were performed to match the preoperative 3D CT scans (Figure 8). A MultiPad was placed close to the patient tracker, and all navigable instruments were identified and registered (Figure 9). A specialized pedicle opener and a bone awl were percutaneously placed at the entry point, and they were inserted into the soft tissues to touch the anatomical landmark following the route designed by the navigation (Figure 10). Four percutaneous pedicle screws were placed accurately and safely under navigated guidance. The depth of the screw entry was also monitored by the navigation system. The incision was independently designed according to the pedicles and decompression procedure, which could be shorter and better aesthetically (Figure 11). AP and Lat radiographs were validated to ensure that the position was reasonable.
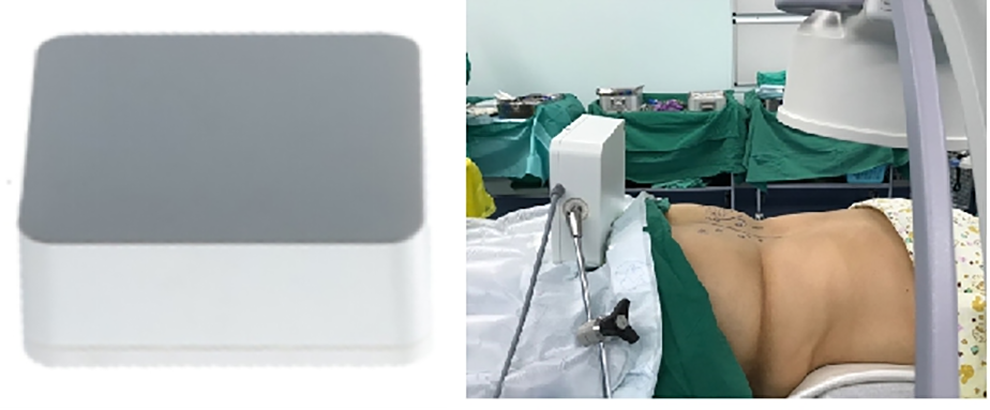
EM field generator and its position close to the button.

The reference coil, called the patient tracker, was attached to the spinous process. In order to avoid rotation, the second generation with 2 holes at the center was developed.
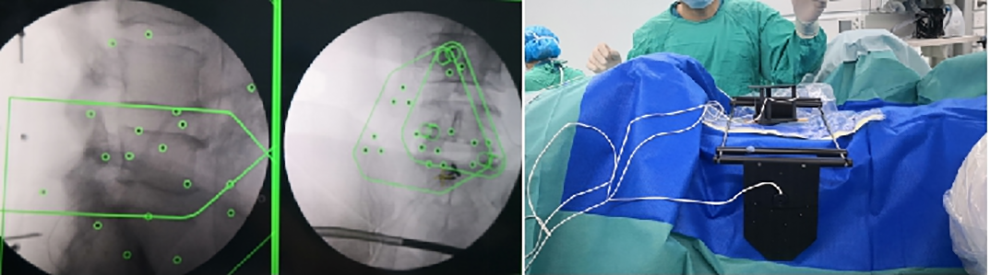
Mapper bridge was placed on the lower back, and standard anteroposterior and lateral X-ray films were done to match with the preoperative 3D CT scans.

MultiPad should be placed close to the patient tracker, and all the navigable instruments should be registered.
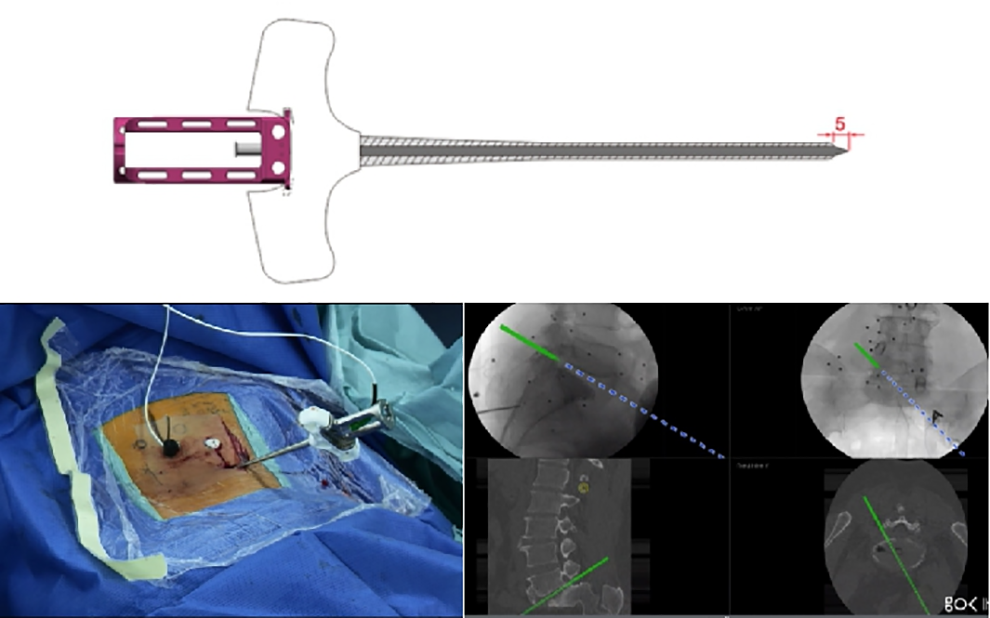
Specialized pedicle opener and bone awl were percutaneously placed at the entry point and inserted into the soft tissues to touch the anatomical landmark following the route designed by the navigation.
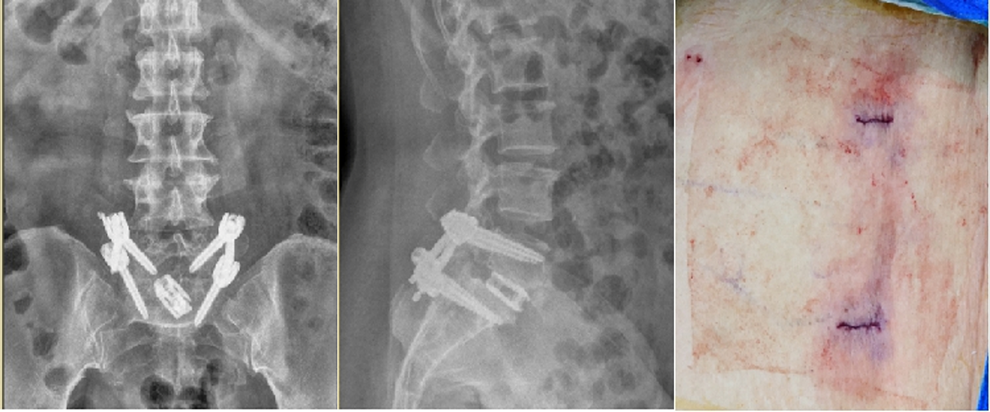
Four percutaneous pedicle screws were placed accurately and safely under navigated guidance, and the incision was always much shorter.
Evaluation Standard for the Accuracy
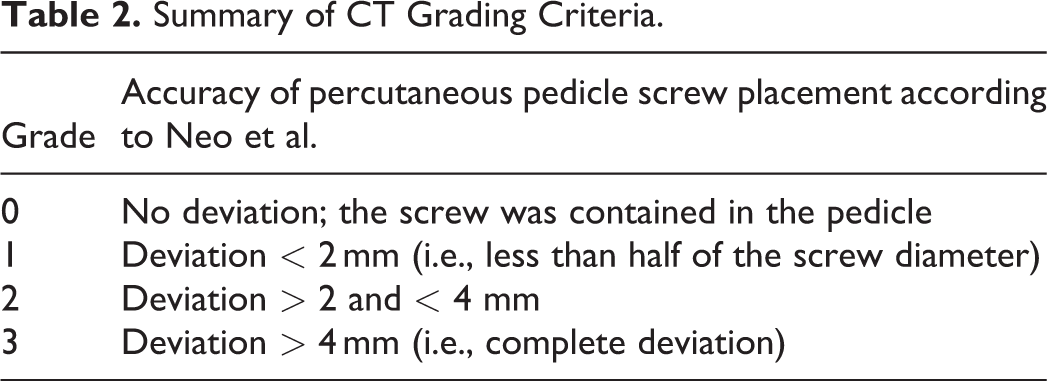
All patients were subjected to postoperative 3D CT scans to assess screw orientation by measuring the perpendicular distance between the pedicle cortical wall and the screw surface. Radiographic analysis was conducted by an independent, blinded radiologist. Pedicle screw placement was classified as grades 0, 1, 2, and 3, according to the position of pedicle screws, as described by Neo et al. 4 (Table 2). Grades 0 and 1 were considered as excellent and good rates.
Summary of CT Grading Criteria.
Statistical Analysis
Statistical analysis was performed using SPSS 19.0 software. Measurement data were expressed as mean ± SD. Comparison between 2 groups was performed by the independent sample t-test and correlation analysis. Statistical significance was defined as P-values < 0.05.
Results
All percutaneous pedicle screws used had a diameter ranging from 6.0 to 6.5 mm. In the robot-assisted group, the diameter was selected according to the preoperative plan, while in the electromagnetic navigation group, it was selected based on clinical experience.
In the robot-assisted group, 25 cases with 100 percutaneous pedicle screws were included, of which 90 pedicle screws were rated as Grade 0, 5 as Grade 1, 2 as Grade 2, and 3 as Grade 3. Three pedicle screws inserted by the fellow surgeon showed penetration of the pedicle wall on an intraoperative X-ray fluoroscopy, and they were adjusted immediately; these screws belonged to Grade 3. The excellent and good rate was 95%. In the electromagnetic navigation group, 31 cases with 124 screws were included, of which 114 pedicle screws were rated as Grade 0, 7 as Grade 1, 3 as Grade 2, and none were Grade 3. The excellent and good rate was 97.6%, and there was no statistical difference between the two groups (P > 0.05) (Table 3) (Figure 12). With respect to the registration time and the total time for the surgery, there were no statistical differences between the two groups (P >0.05). The main differences between the two groups were the guide-wire insertion time and the X-ray exposure time (P < 0.05) (Table 4). Due to the ease of operation of electromagnetic navigation, local anesthesia was first successfully applied during Endo-TLIF. There was one case of rod dislocation in the robot-assisted group, but there were no cases of dural tear, nerve root injury, postoperative hematoma, postoperative infection, or other kinds of complications in this research.
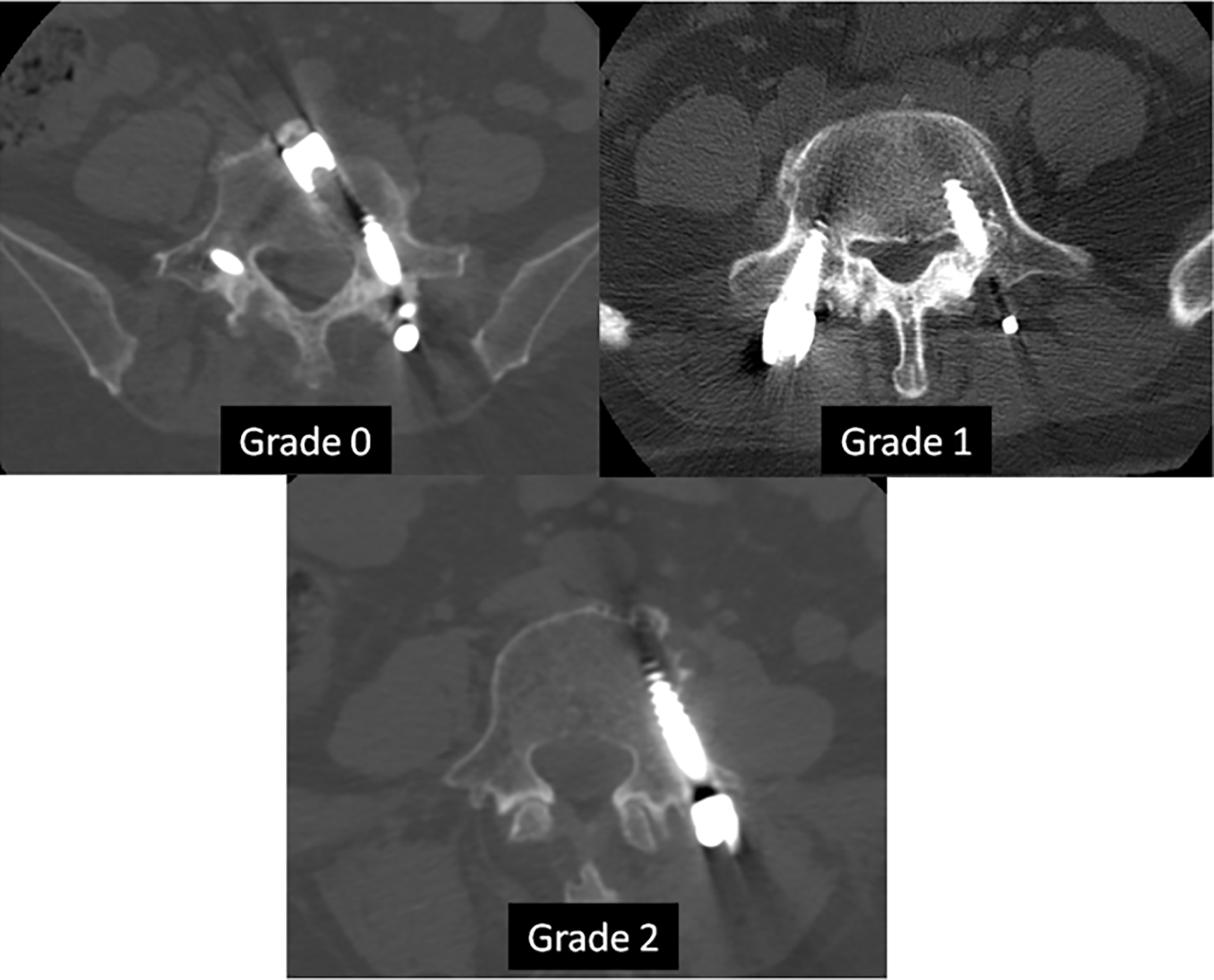
Grades 0, 1, and 2 of the two groups, and no Grade 3 according to the postoperative CT scans.
Pedicle Grading of the Two Groups After Surgery (n = 56).a
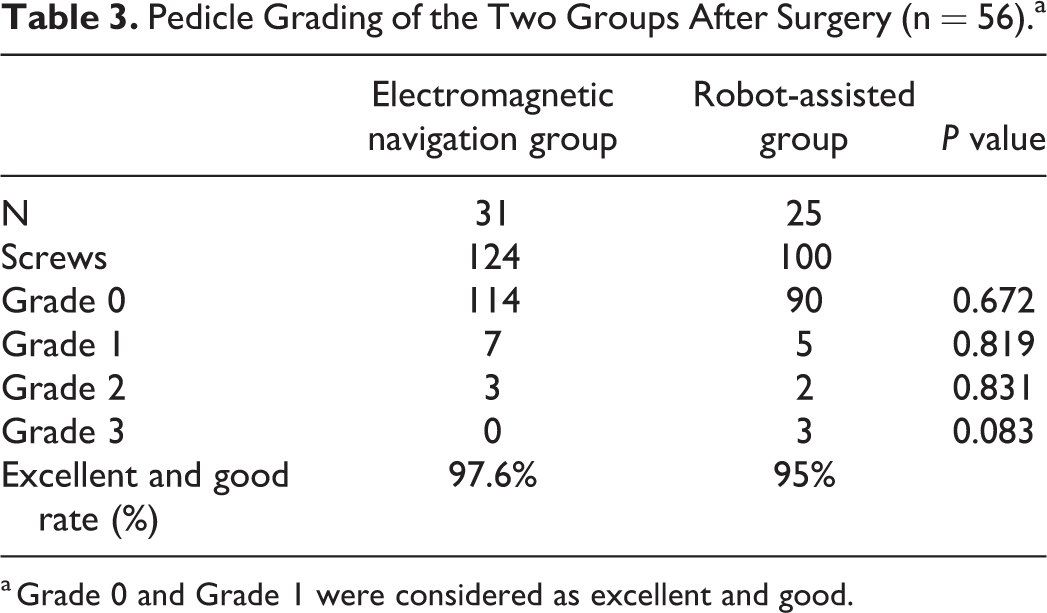
a Grade 0 and Grade 1 were considered as excellent and good.
Clinical Outcomes of the 2 Groups After Surgery (n = 56).
Discussion
Clinically available navigation systems can be classified into optoelectronic navigation, robot-assisted surgery, and magnetic navigation systems.5,6 Navigation systems based on optical sensors have been widely used over the past several years, particularly in pedicle screw placement. However, the disadvantage is that the line of sight can never be interrupted, which limits the operator’s degree of freedom during the procedure, thus also limiting the intuitive use of surgical instruments. In addition, the trackers must be designed so that they extend beyond the operation site to be detected by the navigation camera. Even very small changes in position due to accidental contact with the reference base can lead to faulty positioning and subsequent complications. The complications related to pedicle screw misplacement, such as postoperative neuralgia, decline in muscle strength, iatrogenic infection, revision surgery, instability and corresponding back pain, prolonged hospital stay, and added health care costs, pose a challenge for spine surgeons. 7
MISS, with the advantage of minimal tissue damage, is a promising alternative but at the cost of losing direct visualization of anatomic landmarks, which would result in a high incidence rate of percutaneous pedicle screw placement malposition. Innocenzi et al. published a series comparing 4 groups of pedicle screw placement, which included navigated MIS and navigated open screw placement, and they showed a higher screw malposition rate in the MIS group (13.9% vs. 7.3%) (P = 0.0263). 8 However, in our study, because both robot-assisted system and electromagnetic navigation system are precise surgical techniques that are far superior to the other navigation systems, the excellent and good rate was 95%-97.6%, and there were no statistical differences between the two.
It has been shown that medial pedicle perforation of more than 4 mm may endanger the neural elements, causing neurological deficits. Although there is no strong evidence in the literature suggesting that pedicle violation less than 2 mm is safe, most surgeons consider it as a safe zone for pedicle perforation. 9 Therefore, accuracy is important in screw placement, that is, the screw must fully be included in the pedicle, and there must be no cortex violation in the early stage. Thus, with this theory as the standard, we evaluated the excellent and good rates in our study. Three pedicle screws in the robot-assisted group had to be adjusted with the help of intraoperative real-time X-ray fluoroscopy confirmation as the assistant surgeon was not well-trained on the robot technique, which resulted in the high-speed electric drill slipping out of the entry point and causing an error. Here, we consider those 3 pedicle screws as Grade 3 in order to emphasize the importance of training on using the robot technique. Besides, only one patient received local anesthesia in our study. For the 55 cases with general anesthesia, intraoperative neurophysiological monitoring was necessary in order to reduce the risk of nerve root injury during pedicle screw insertion and cage implantation, especially for a beginner using the computer-assisted navigation system. The preparation for neurophysiological monitoring required about 10 min, which was usually completed during the anesthesia induction and intubation of trachea, prior to the operation.
In contrast to the other relatively mature navigation, robotics is a relatively new and developing technology in spinal surgery. As is well known, DaVinci, as a robot-assisted system, is a proven technology in laparoscopic surgery. Lippross et al. successfully employed DaVinci as an access tool to assist in corpectomy and cage implantation to treat an L3 fracture. 10 The first-ever spine robot, the SpineAssist (Mazor Robotics Ltd., Caesarea, Israel), obtained FDA approval in 2004. With its ability to provide real-time intraoperative navigation and rigid stereotaxy, robotic-assisted surgery has the potential to increase in accuracy while decreasing radiation exposure, complication rates, operative time, and recovery time. 11 The initial focus of spinal robotics has been on accurate pedicle screw placement, and early studies have shown it to be successful. 12 Our spine department was the third one to have Mazor robotics in China in 2016, and all our spine surgeons received strict training on its use. Based on the success of open surgeries and MIS-TLIF conducted in the past, the accuracy in pedicle screw placement was approved; therefore, robot-assisted was selected as the control group. From the clinical applications, we found that the software of the robot system was stable and helpful for replanning and registration, but strict training was necessary. Also, after inserting the guide-wire, other procedures, like decompression and depth measurement of pedicle entry, were not useful, which increased the X-ray exposure compared to electromagnetic navigation (31.15 ± 8.25 s vs. 21.3 ± 6.92 s, P < 0.05).
The principle of the new navigation system based on electromagnetic navigation is the continuous tracking of the instruments and the patient’s anatomical structures during the surgical procedure. The navigation system thus supports the operative procedure by providing additional information without changing or hindering the operator’s general process. Another advantage of EMF navigation in comparison with optical methods is the position of the reference coil on the instruments. It is placed near the tip of the instrument, which can result in lower torsion errors. Patrick had also used the same electromagnetic navigation system to test its accuracy, and it was placed in 24 pedicles of 2 human lumbar spine specimens obtained during postmortem. By evaluating the position of the screws in the direction of the trajectory and any injury to the surrounding cortical bone, he concluded that EMF navigation offered a high accuracy in pedicle screw placement, short set-up time and easy handling, absence of intraoperative radiation exposure, and free mobility without interfering with navigation. 13 Fraser utilized 2-dimensional EM navigation in a cadaveric study to evaluate percutaneous pedicle screw insertion. Five cadaveric specimens underwent bilateral screw placement from L1 to S1, using conventional fluoroscopy (CF) on one side and EM guidance (EM) on the matching contralateral side. The study provided a modality for lumbosacral percutaneous pedicle screw fixation, which was more efficient and safer than CF. 14 Similar results have been reported in another study. 15
Electromagnetic system, as an alternative to the robot-assisted system, significantly reduced the guide-wire insertion time (9.45 min vs. 13.2 min, P = 0.001). In summary, the results indicate that the new EMF navigation system is a good placement technique for pedicle screw placement for lumbar spondylolisthesis. It should be emphasized that the system is easy to handle and does not limit the operator’s workflow or use of standardized instruments.
Conclusions
In our study, we compared the accuracy and safety of electromagnetic navigation with robot-assisted system during Endo-LIF. Both of them are safe and efficient for percutaneous pedicle screw placement and have high accuracy, which could promote the popularization of Endo-LIF. Electromagnetic navigation had obvious advantages over robot-assisted in terms of faster guide-wire placement and less X-ray exposure. Robot-assisted for percutaneous pedicle screw placement offers a preoperative planning system and a stable registration system, with obvious drawbacks of a strict training curve. The limitation of this study is that we could not determine whether or not the degree of screw invasion into the intervertebral joints is associated with increased stress on the facet joints and increased pressure on the adjacent discs, which should be evaluated in further studies. Furthermore, technical issues, such as differences in surgeons’ skills and varying complexity of surgery and screw/pedicle dimensions, could be further evaluated.
Footnotes
Authors’ Note
Derong Xu and Xuexiao Ma are co-first authors. This study was approved by the Affiliated Hospital of Qingdao University and informed consent was signed by all patients. This is a retrospective study and the IRB approval is not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received support from National Natural Science Foundation of China (81 871 804).