
Abstract
Study Design
Systematic Review and Meta-analysis
Objectives
Raised patient BMI is recognised as a relative contraindication to posterior lumbar interbody fusion (PLIF) due to the anaesthetic challenges, difficult positioning and increased intraoperative and postoperative complications, with the relative risk rising in patients with a BMI >25 kg/m2. The impact of obesity defined as a BMI > 30 kg/m2 on Anterior Lumbar Interbody Fusion (ALIF) outcomes is not yet established. The aim of this review was to evaluate if the presence of a raised BMI in patients undergoing ALIF procedures was an independent risk factor for intra- and postoperative complications.
Methods
A systematic review of search databases PubMed; Google Scholar and OVID Medline was made to identify studies related to complications in patients with increased body mass index during anterior lumbar interbody fusion. PRISMA guidelines were utilised for this review. Complication rates in raised BMI patient cohort was compared to normal BMI complication rates with meta-analysis where available.
Results
315 articles returned with search criteria applied. Six articles were included for review, with 2190 patients included for analysis. Vascular complications in obese vs. non-obese patients undergoing the anterior approach demonstrate no significant difference in complication rates (P = .62; CI = −.03–.02). Obesity is found to result in an increased rate of overall complications (P = .002; CI = .04–.16).
Conclusions
Obesity was demonstrated to have an impact on overall complication rates in Anterior Lumbar Interbody Fusion procedures, with postoperative complications including wound infections and lower fusion rates more common in patients in increased BMIs. Increased focus on patient positioning and reporting of outcomes in this patient cohort is warranted to further evaluate perioperative complications.
Introduction
Obesity, defined as a body mass index (BMI) of ≥30 kg/m2, is regarded among the most renowned risk factors for attributable mortality. 1 An increasing global incidence is of concern for practicing surgeons, as obesity can precipitate various perioperative complications such as an prolonged operative time and increased blood loss.2,3 Regarding spine surgery in particular, lumbar fusion is one of the most commonly performed procedures, and is employed to treat various spinal pathologies, including degenerative disc disease, 1 spondylolisthesis, 2 and discogenic back pain. 3 Subsequent to the widespread innovation witnessed in the field of spine surgery, multiple modern approaches to the lumbar spine were developed; posterior, transforaminal, 4 oblique 5 and anterior approaches. 6 Fusion in the lumbar spine can be achieved through the implementation of screw-rod constructs and/or the use of interbody cages. Interbody cages are an efficacious form of instrumentation that serve to improve the stability, balance and function of the treated lumbar segment. At present, the posterior fixation approach remains the preferred method. 7 However, De la Garza Ramos et al. 8 report increased BMI as a relative contraindication to posterior lumbar interbody fusion (PLIF) due to certain anaesthetic challenges, difficult positioning and increased complication rates. It is noted that the relative risk of complications rises in patients with a BMI >25 kg/m2, and the greatest rate of complications is evident in those with a BMI >30 kg/m2.
Alternatively, anterior lumbar interbody fusion (ALIF) is an approach growing in popularity secondary to advances in technology and instrumentation that have facilitated improvement of the surgical approach. 9 Reports convey that the rates of ALIF procedures performed from 2007 to 2014 in the USA have more than doubled 10 ; often for revision surgery due to failed posterior or transforaminal lumbar interbody fusion. 11 Although the relative risk of complications in overweight and obese patients has been highlighted in studies evaluating combined ALIF and artificial disc replacement (ADR) procedures,12-14 the impact of obesity on ALIF outcomes are not well established in the current literature. 15 Given the variability in reporting of intraoperative and postoperative outcomes in patients with raised BMIs, this review aims to collectively evaluate the impact of obesity on perioperative and postoperative outcomes following ALIF.
Methods
Search Strategy
A comprehensive search strategy was performed of electronic databases including PubMed, Ovid Medline, Google Scholar, EMBASE and Cochrane databases with study selection identification from September 2020 to November 2021. The aim was to identify studies in the English language that contained a combination of search terms consisting of: {“Anterior Lumbar Interbody Fusion” AND “obesity”}, {“ALIF” AND “Obesity”}, {“ Anterior Lumbar Interbody Fusion” AND “BMI”}, {“ ALIF” AND “BMI”}, {“ Anterior Lumbar Interbody Fusion” AND “weight”}, and {“ALIF” AND “weight”} {“ Anterior Lumbar Interbody Fusion” AND “BMI” AND “complications”}, {“ Anterior Lumbar Interbody Fusion” AND “BMI” AND “outcomes”}, {“ Anterior Lumbar Interbody Fusion” AND “obesity” AND “outcomes”}, {“ Anterior Lumbar Interbody Fusion” AND “obesity” AND “complications”}, {“ ALIF” AND “BMI” AND “outcomes”}, {“ ALIF” AND “BMI” AND “complications”}, {“ ALIF” AND “obesity” AND outcomes”}, {“ALIF” AND “obesity” AND “complications”}, placed in “all fields” of the papers retrieved.
The search was carried out in accordance with PRISMA guidelines. Two independent reviewers (A.F and J.M.M) performed a literature search per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and reviewed the search results using the Boolean strings agreed upon by author consensus, to identify articles through title and abstract screening from which full-length texts were selected for further review, with a senior author (I.F) arbitrating in the event of a disagreement. Full texts were then evaluated using eligibility criteria, with agreement from all authors required for inclusion. Reference lists of selected full-length texts were also reviewed for articles eligible for inclusion. Selected articles were imported to Endnote (Microsoft Office 365), where duplicates were removed prior to organisation and analysis.
Eligibility Criteria
The inclusion criteria consisted of (i) in-vivo studies (ii) reported complication rates for obese cohorts comparative to control (iii) were in English or had full translation freely available. The exclusion criteria included (i) case reports, (ii) case series, (iii) did not report complication rates for obese cohorts and (iv) studies that pertained to artificial disc replacements performed in conjunction with ALIF.
Outcomes Analysed and Statistical Analysis
Data extraction tables were designed to summarise data from the included studies. Authors extracted data agreed upon by consensus including country of origin, sample size, methodology, technical approach applied by authors, and use of access surgeons. Studies outcomes were extracted from each study as applicable and analysed including: operative metrics, perioperative complications, postoperative complications and fusion rates. If complication rates provided for patients with normal and raised BMIs were reported in three or more studies, meta-analysis was carried out on the complication in question. Statistical analysis was carried out using RevMan 5.4. A difference in complication rates with a P value of <.05 was taken as significant. Heterogeneity was reported using the I2 statistic. Risk of bias was assessed using the ROBINS-I tool, a risk of bias assessment tool for non-randomised studies.
Objectives and Aims
The objective is to review and collectively compare complication rates for obese cohorts to non-obese patients that underwent ALIF. The aim is to understand if an increased BMI is a risk factor for complications in ALIF.
Results
Search Criteria
The search strategy yielded 435 articles. After removal of duplicates, application of inclusion/exclusion criteria and full-text review, 6 of these were included for review with flowchart demonstrated. (Figure 1). PRISMA flowchart.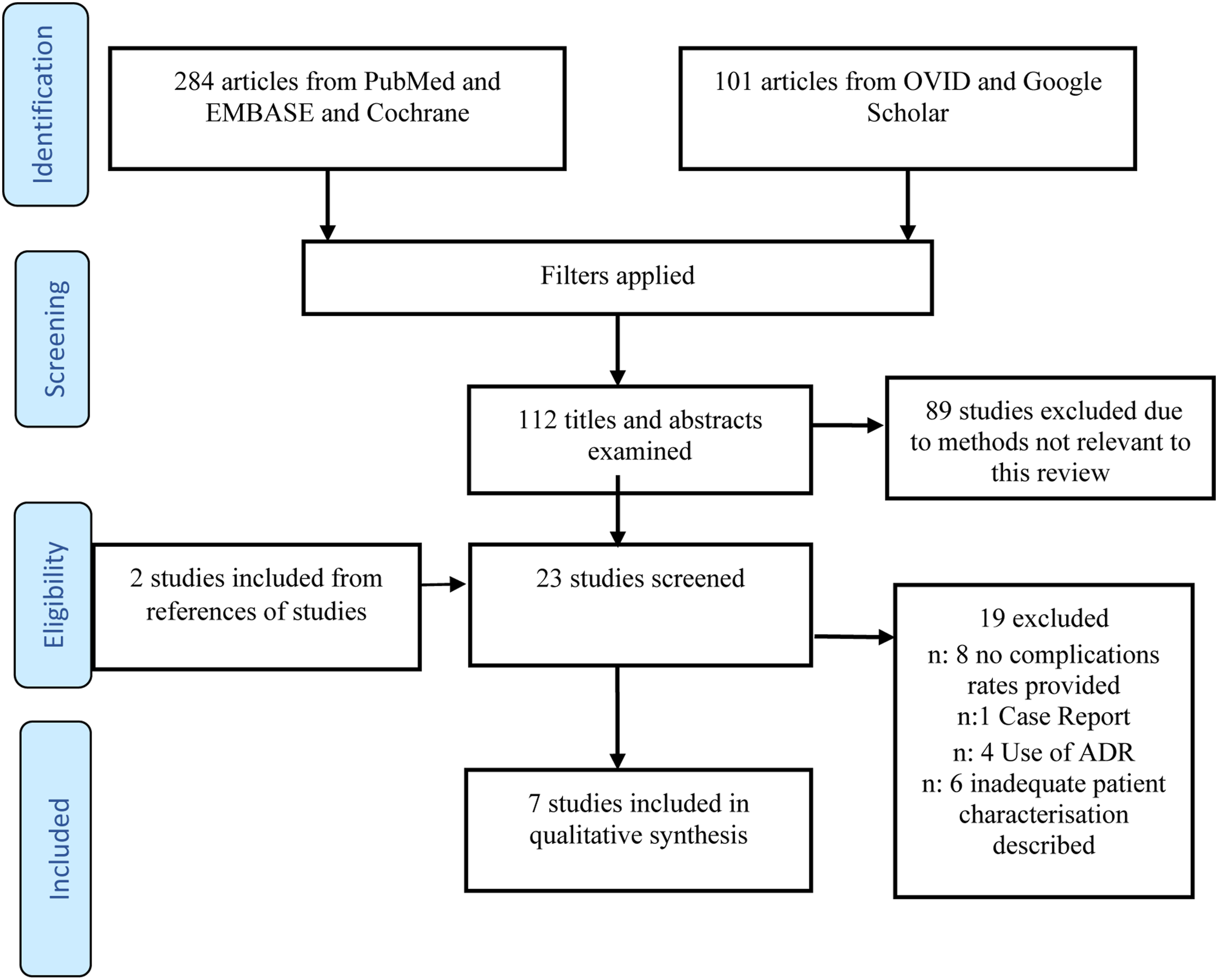
Studies included for Review.
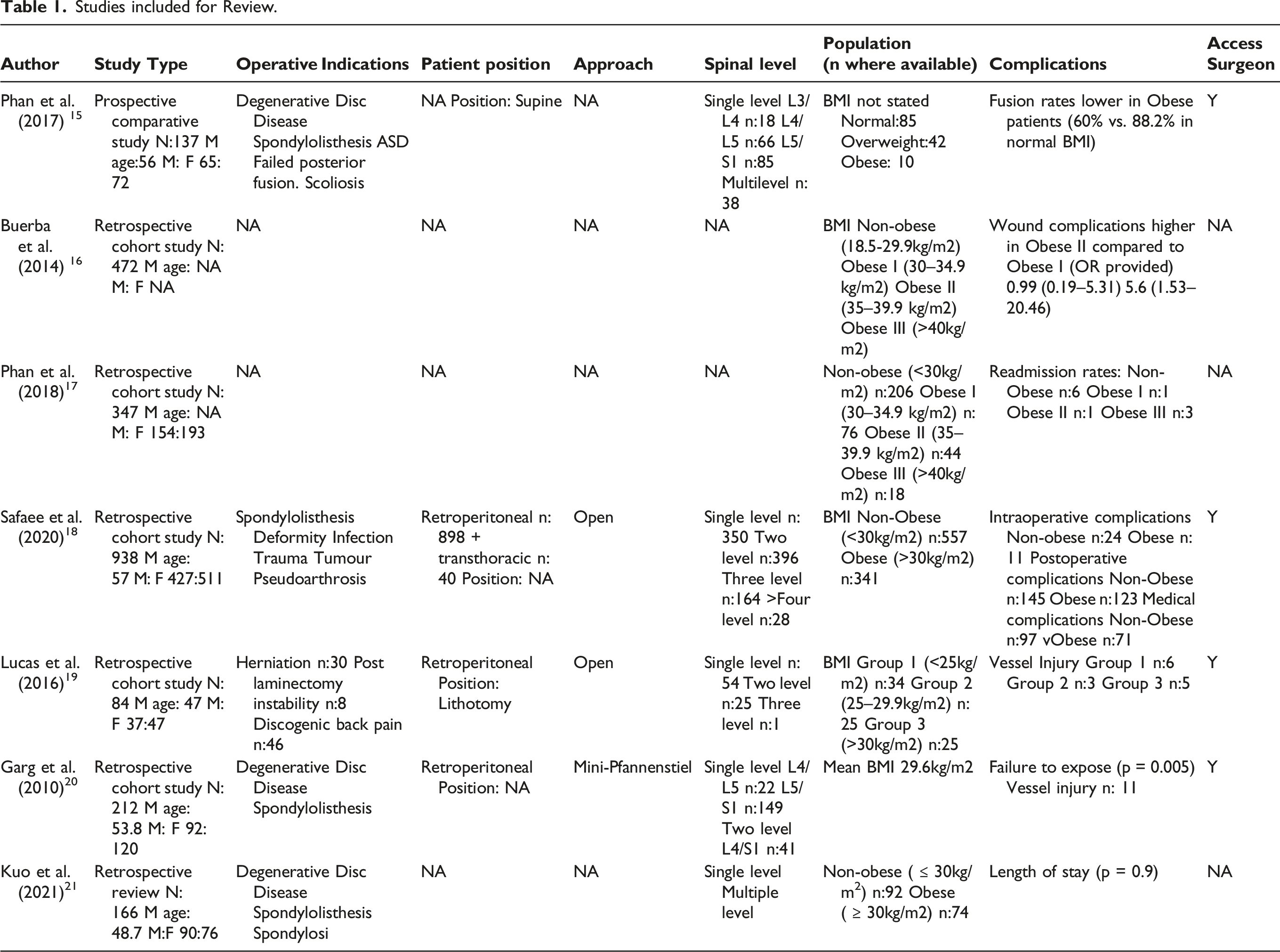
Patient populations were included with BMIs clearly defined in five studies. Two studies grouped patients into obese and non-obese cohorts. Two studies categorised patients into a non-obese category and stratified categories of obesity (BMI 30–35 kg/m2, 35–40 kg/m2, >40 kg/m2). One study classed patients into normal weight, overweight (BMI 25–30 kg/m2), obese (BMI >30 kg/m2). Two studies further subdivided patients with a BMI >30 kg/m2 into obese I (30–34.9 kg/m2), obese II (35–39.9 kg/m2) and obese III (>40 kg/m2). Two studies did not clearly define BMI categories for cohorts. Non-obese participants were more commonly included into studies, with 588 participants defined as obese (>30 kg/m2), 119 recruited with a normal BMI, and 1555 participants having a BMI of <30 kg/m2. Priori analysis was not carried out in any study included in this review, with six studies either demonstrating equity across groups, or indicating sufficient powering was achieved to detect clinically significant differences. The characteristics of each respective study are outlined in Table 1.
Quality of Studies and Risk of Bias
A risk of bias assessment, was carried out using the Cochrane ROBINS-I tool, with all studies included for analysis fulfilling the criteria. Four of seven studies included for analysis demonstrated bias in confounding factors due to the inclusion of patients with multiple risk factors for complications not adequately accounted for in the methodology and subsequent analysis (Figure 2). The remaining three studies demonstrated sufficient delineation of risk factors to demonstrate a clear analyses on the effect of patient BMI and outcomes post-ALIF. ROBINS-I risk of Bias Tool.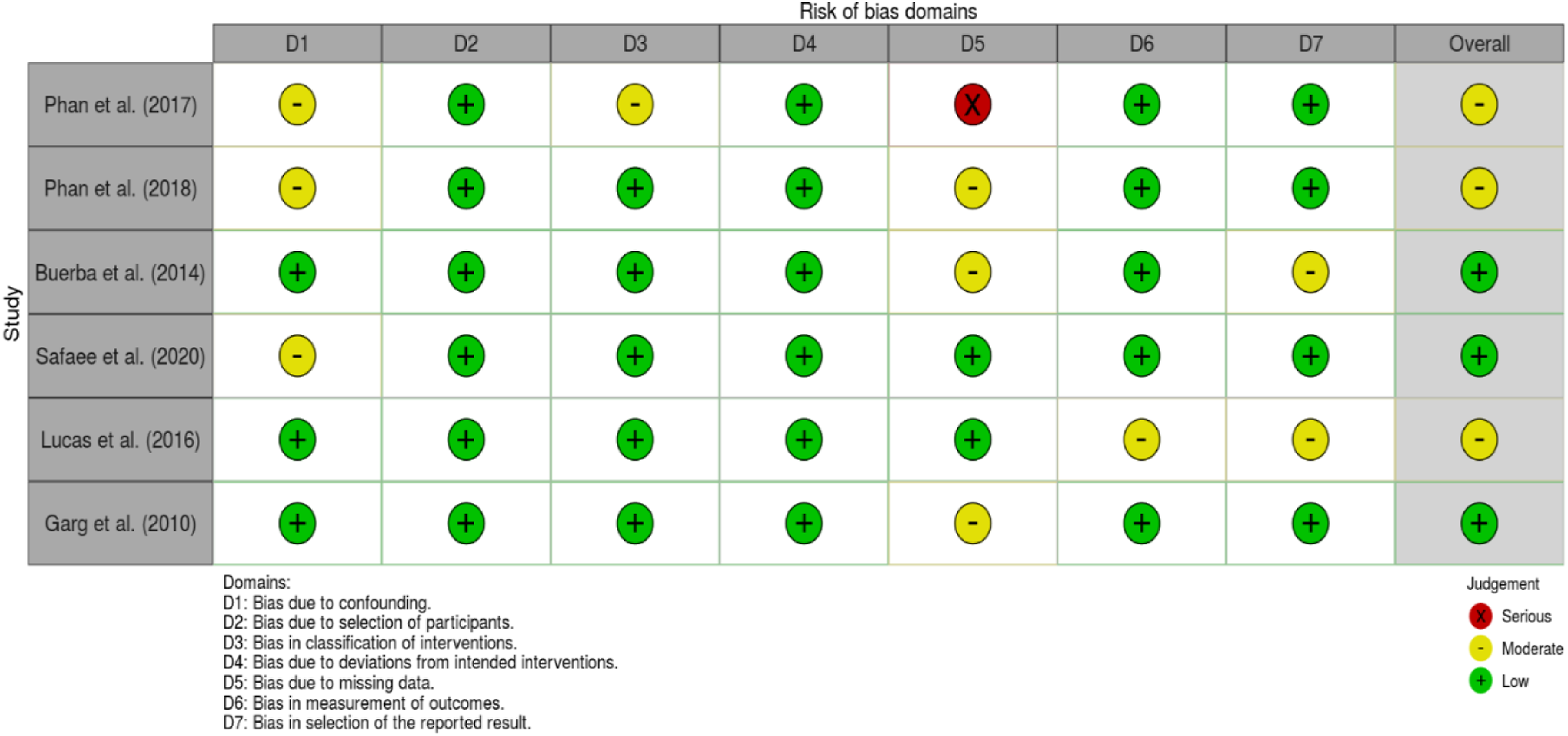
GRADE of Evidence.
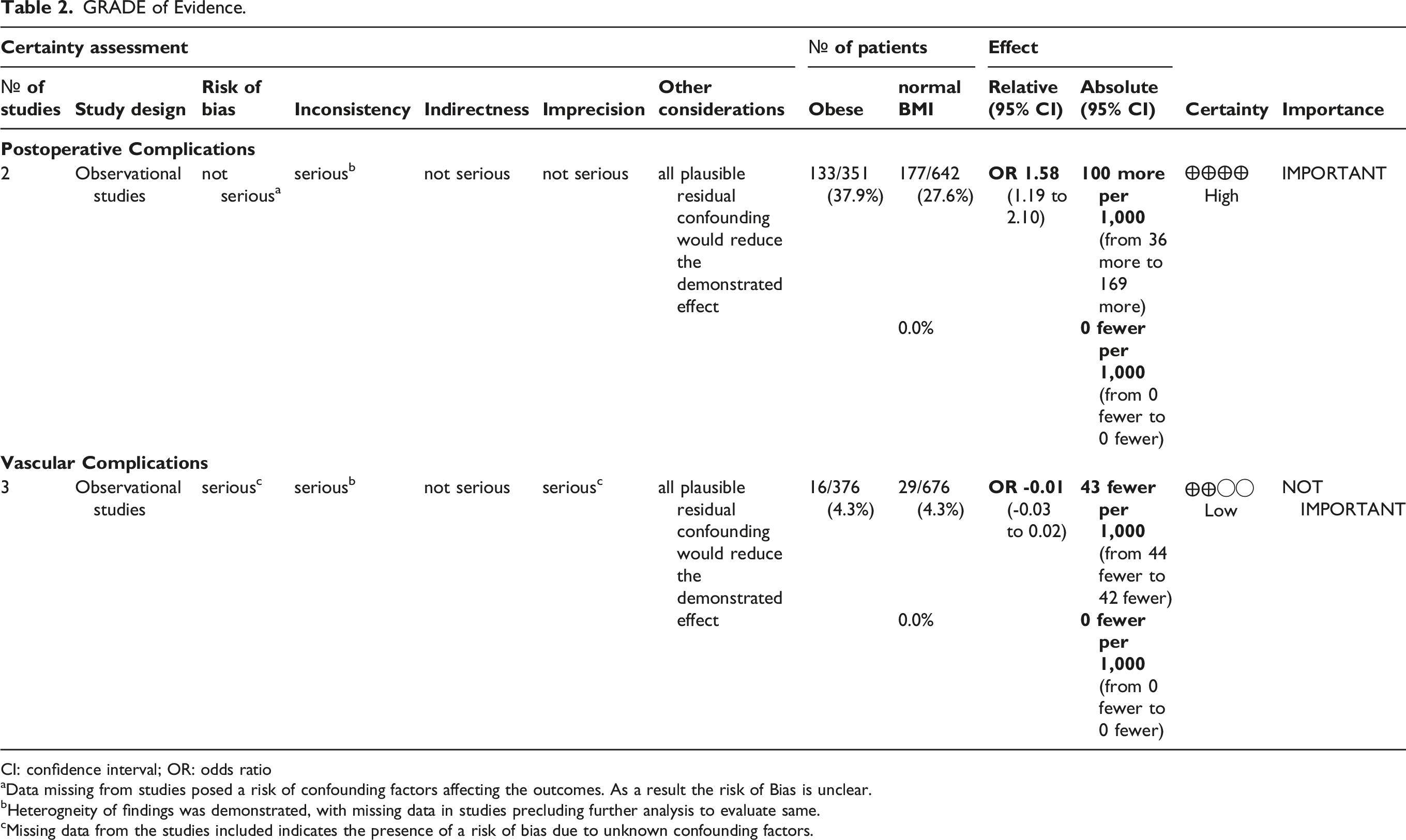
CI: confidence interval; OR: odds ratio
aData missing from studies posed a risk of confounding factors affecting the outcomes. As a result the risk of Bias is unclear.
bHeterogneity of findings was demonstrated, with missing data in studies precluding further analysis to evaluate same.
cMissing data from the studies included indicates the presence of a risk of bias due to unknown confounding factors.
Operative Metrics
Four studies reported the comparative degree of blood loss between cohorts. Three studies found noted no significant difference between groups in terms of blood loss. Lucas et al. reported equivalent losses for normal weight, overweight and obese patients (P = .13). Phan et al. 15 found no significant difference between groups for recorded blood loss (P = .26). Similarly, Safaee et al. noted no difference in blood loss between non-obese and obese patients (P = .6). In contrast, Garg et al. 20 noted a significant correlation between increasing BMI and estimated blood loss (P = .021).
Three studies reported the comparative operative time between cohorts. Operative time was found by Lucas et al. 19 to be significantly longer in patients with BMI >30 kg/m2 (P = .01), with no difference noted between patients with normal BMIs and overweight patients. In contrast, two studies noted no difference in operative time between BMI groups. Phan et al. 15 reported no significant difference between the respective groups of BMI classification (P = .6). Once again, Safaee et al. 18 similarly reported no difference in operative time regardless of BMI (P = .2).
Two studies reported the comparative length of stay in relation to increased BMI. Length of stay was not found to be related to BMI (P = .08) by Phan et al., 15 or Safaee et al 18 (P = .4).
Overall Complications
Comparative rates of overall comparations in obese and non-obese groups were reported in two studies. As indicated in the forest plot in Figure 3, obese patients experienced a significantly increased rate of overall complications compared to non-obese patients (P = .002; 95% CI: .04.0.16; I2 = 86%). Diversity of study methodologies included in this review precluded a thorough sub-analysis of each complication reported within each group defined by outlined BMIs. Risk of total complications across comparative study in obese and normal BMI patients.
Vascular Complications
Vascular complications in obese and non-obese patients undergoing ALIF were reported in three studies. Comparative analysis demonstrated no significant difference in complication rates (P = .62; 95% CI-.03.0.02; I2 = 0%), outlined in Figure 4. An access surgeon was employed in all three studies. An open retroperitoneal approach was utilised in two studies, while Phan et al.
15
did not specify the approach method. Risk of vascular complications arising from each study group.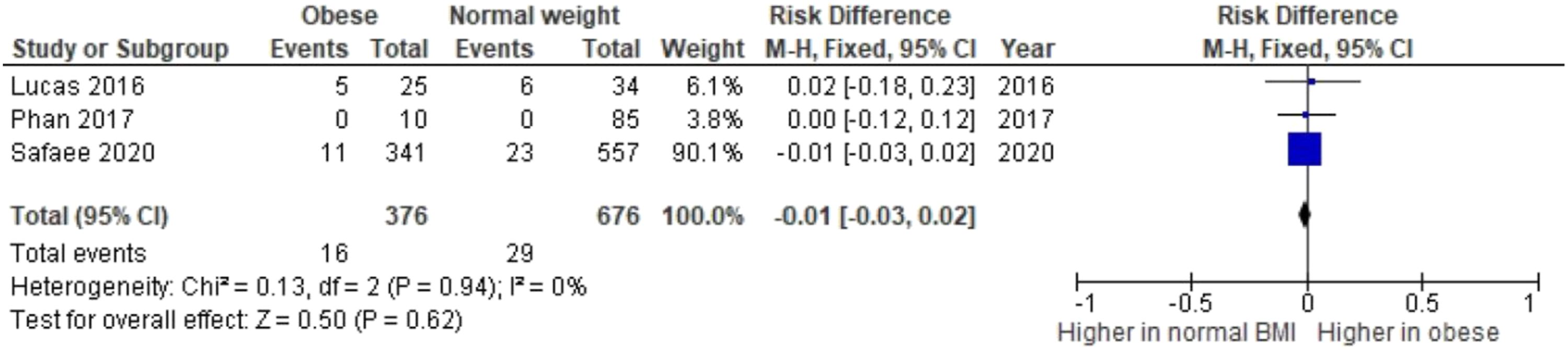
Wound Complications
Two studies reported on wound complications. Safaee et al. 18 reported a significant increase in wound complications in obese compared to non-obese (11.4% vs 3.4%, P < .001).However, Phan et al. 15 found no significant increase in wound complications in patients with BMI >25 (2.4% vs. 10%, P = .19).
Postoperative Ileus
Postoperative Ileus in overweight and obese patients was reported in two studies. Safaee et al. 18 reported a significant association (11.7% vs 7.2%, P = .02), while Phan et al. 15 noted no increased risk (2.4% vs. 0%, P = .537). Risk of hernia in patients with raised BMI was found to be significant (5.3% vs 2.0%, P = .007) by Safaee et al. 18
Fusion Rates
Fusion rates were reported in only one study in this review. Phan et al. (2017) 15 found patients with BMI >30 kg/m2 had a fusion rate of 60% compared to 76% and 88% fusion in patients with a BMI 25–30 kg/m2 and BMI <25 kg/m2 at 12 months.
Discussion
The obesity paradox is a controversial theory that patients with an increased BMI have significantly lower rates of mortality when compared to those with normal BMI. 23 This phenomenon has been depicted in several recent meta-analyses. Niedziela et al. 24 reported that overweight (RR: .7; 95% CI: .64.0.76), obese (RR: .6; 95% CI: .53.0.68) and severely obese patients (RR: .7; 95% CI: .58.0.86) had lower mortality compared to those with normal BMI (RR: .7, 95% CI: .64.0.76) when concerned with acute coronary syndrome cohorts. Comparatively, although Zhi et al. 25 noted obesity as a risk factor for developing acute respiratory distress syndrome (ARDS) or acute lung injury (ALI), obesity was inversely associated with 60-day (OR: .84; 95% CI: .75.0.94) and 90-day mortality (OR: .38; 95% CI: .22.0.66). This paradox is not without its challenges, with several sceptics referring to inherent collider stratification bias and illness-associated weight loss bias. 23 Collider stratification bias relates to the comparison of obese and non-obese cohorts for particular pathologies, and is well described by Banack et al. 23 It is summarised in that a larger proportion of the non-obese cohorts have more influential risk factors for mortality. Illness-associated weight loss bias refers to scenarios in which more advanced disease would be associated with a greater degree of weight loss. Morality analyses may highlight obesity as a protective factor with regards to mortality rates, ignoring the stage of the disease as a confounder. Nevertheless, while several hypotheses exist, there remains a lack of consensus regarding the aetiology of the paradox to date2326. However, one might assume that morbidity and mortality are not mutually exclusive, and this has been depicted in several studies.26-28
In our study, there was a greater overall complication rate (P = .002) evident when obese cohorts were compared to non-obese patients, with moderate Risk of Bias highlights and a high certainty of evidence demonstatrated using the GRADE tool. However, analyses of specific complications proved conflicting. One study reported a significantly larger degree of perioperative blood loss for an obese cohort. 20 Comparatively, while another study reported increased rates for vascular complications in the obese cohort, 24 this did not reach statistical significance on collective meta-analysis (P = .62). This is an important parameter, as vascular injury, increased blood loss, and a need for transfusion have been shown to significantly influence 30-day morbidity and mortality.29,30 Also required for consideration is the dearth of information on potential confounding factors across studies including approach level, method of approach, and the use of an access surgeon. These highlight the need for further high-quality studies with adequate analysis to account for confounding factors and other sources of bias which arise in clinical studies.
Equally important in spine surgery is the degree of fusion, as poor fusion can precipitate poor patient reported outcome measures and influence readmission and revision rates. Fusion rates in the anterior approach have been evaluated extensively, with fusion rates as high as 98% 31 for combined approaches reported in the literature, and between 57.5% and 99% in stand-alone procedures. 32 Obesity has been reported to impact subsidence and fusion rates following spinal lumbar fusion, with variability evident in studies. 8 In this review, one study noted a lower disc height in obese patients at follow-up, with lower fusion rates achieved at 12 months compared to patients with a normal and overweight BMI. 15 However, studies in the literature often show conflicting results regarding obesity and overall fusion rates.33,34 Regardless, the need for readmission and revision is of concern. In a large study of approximately 223 000 patients by Ma et al., 35 the incidence of procedure-related complications was 16.02% among revision thoracic or lumbar spinal fusion, compared with 13.44% in primary thoracic or lumbar spinal fusion patients (P < .0001). Although this study does not pertain to ALIF patients specifically, it raises an interesting query regarding the clinical relevance of reported complications in obese ALIF patients. Undoubtedly, increased rates of complications, readmissions and revision surgeries all incorporate the utilisation of resources at an increased cost, in addition to the increased risk of hospital acquired infections associated with a prolonged length of stay. However, the extent of reporting in the studies included in this review serves a limitation. It is not feasible to assess if complication rates reflect mortality rates for obese patients undergoing ALIF. Another limitation to included studies is the lack of obesity stratification for further analyses. In a study of 24 196 patients, Marquez-Lara et al. 36 highlight the importance of obesity stratification. Cohorts were categorised into those with a normal BMI (18.5–24.99 kg/m2), overweight (25.0–29.99 kg/m2), class 1 obese (30.0–34.99 kg/m2), class 2 obese (35.0–39.99) and class 3 obese (≥40 kg/m2). Relative risk showed a linear increase across categories for superficial wound infection (range 1.3–3.8), urinary tract infection (range .9–1.7), acute renal failure (range 1.2–15.3) and sepsis (range 7.9–17.5). Pulmonary embolism and deep venous thrombosis portrayed similar findings. 36 However, a decrease in relative risk was witnessed between class 1 and class 2 obesity, respectively. Interestingly, a decrease in mortality was seen among increasing classes of obesity (Relative risk: 2.5 vs 1.1 vs 1.2).36
Such reports highlight the need to categorise and stratify the degree of obesity. This would provide a greater understanding of complications associated with levels of obesity. It is of great importance for risk stratification and is pertinent to spine surgery given the nature of the procedures. Additionally, it allows for improved pre-operative planning with novel approaches, such as minimally invasive surgery (MIS) and awake spinal fusion. 37 Future prospective studies should aim to delineate if patients with a certain BMI are suitable for MIS or awake spinal fusion. MIS is attractive as an option for particular patient cohorts. However, notable adipose tissue may make an MIS approach difficult, and ultimately require conversion to a traditional open approach. Such was noted by Brau et al. 38 who described the mini-open approach for ALIF, recommending the L2–L3 level be avoided in higher BMIs due to the significant increase in technical difficulty on the approach. Furthermore, further investigation is needed for novel techniques to spinal fusion, such as awake spinal fusion. Awake spinal fusion is proclaimed to be the next inevitable widespread adoption in spine surgery, with proclamations of a potential reduction in complications and improvement in patient reported outcome measures. 37 However, awake spinal fusion has particular considerations with regards to anaesthesia. 37 Thus, whether obese patients are generally suitable for awake spinal fusion remains to be validated, as they can represent an anaesthetic challenge. Lack of patient-reported outcomes measures in included studies provides another limitation to deciphering the clinical relevance of increased complication rates associated with obese ALIF patients. In addition, incomplete procedural details outlined in studies in this review preclude thorough evaluation of certain approaches and patient positioning on outcomes in obese patients. Similarly, short follow-up and a paucity of data on fusion rates in patient cohorts was noted. Therefore, the current literature does not allow for meaningful analyses on the impact of obesity in ALIF patients. Future studies should focus on stratifying obesity, and the relation of morbidity to patient reported outcome measures and mortality. By doing so, practicing spine surgeons will be able to optimise treatment strategies for obese patients requiring ALIF.
In this review, obesity was associated with significantly higher overall complication rates in patients undergoing ALIF. However, the current available literature does not allow for meaningful analyses. More robust studies that assess how the degree of obesity can affect complication rates and postoperative morbidity, mortality and patient-reported outcome measures are needed in order for practicing spine surgeons to optimise treatment strategies for this particular cohort.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.