
Abstract
Study Design
Single-center retrospective study.
Objective
The objective of this study was to evaluate the association of psoas muscle mass defined sarcopenia with perioperative outcomes in geriatric patients undergoing elective spine surgery.
Methods
We included geriatric patients undergoing thoracolumbar spinal surgery. Total psoas surface area (TPA) was measured on preoperative axial computerized tomography or magnetic resonance imaging at the L3 vertebra and normalized to the L3 vertebral body area. Patients were divided into quartiles by normalized TPA, and the fourth quartile (Q4) was compared to quartiles 1–3 (Q1-3). Outcomes included perioperative transfusions, length of stay (LOS), delirium, pseudoarthrosis, readmission, discharge disposition, revision surgery, and mortality.
Results
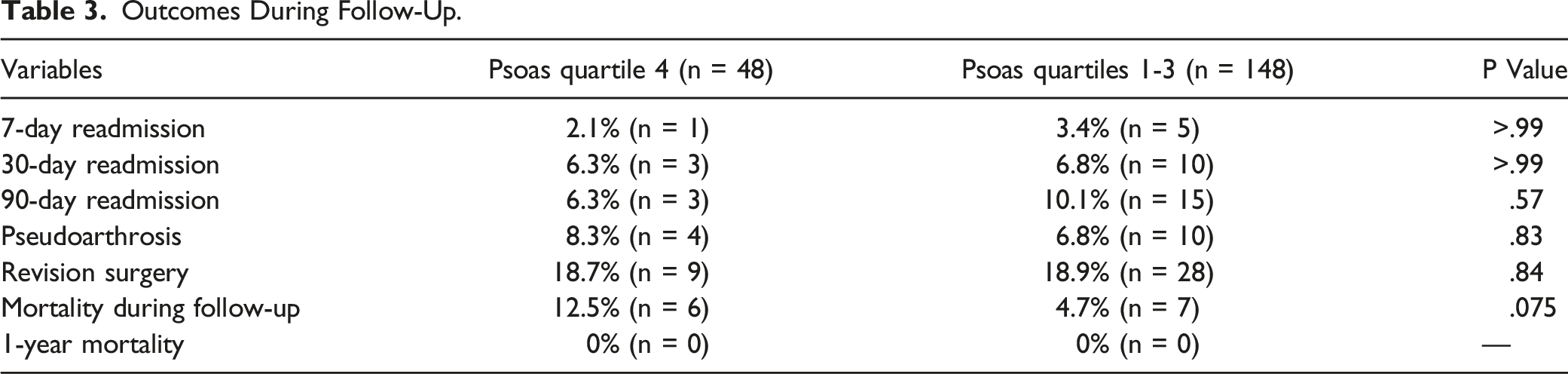
Of the patients who met inclusion criteria (n = 196), the average age was 73.4 y, with 48 patients in Q4 and 148 patients in Q1-3. Q4 normalized TPA cut-off was <1.05. Differences in Q4 preoperative characteristics included significantly lower body mass index, baseline creatinine, and a greater proportion of females (Table 1). Q4 patients received significantly more postoperative red blood cell and platelet transfusions and had longer ICU LOS (P < .05; Table 2). There was no difference in intraoperative transfusion volumes, delirium, initiation of walking, discharge disposition, readmission, pseudoarthrosis, or revision surgery (Tables 2 and 3). Mortality during follow-up was higher in Q4 but was not statistically significant (P = .075).
Conclusion
Preoperative TPA in geriatric patients undergoing elective spine surgery is associated with increased need for intensive care and postoperative blood transfusion. Preoperative normalized TPA is a convenient measurement and could be included in geriatric preoperative risk assessment algorithms.
Introduction
As the geriatric population continues to grow in the United States, so too will the number of patients undergoing elective spine surgery to correct age-related degenerative changes.1-3 The elevated risk of adverse postoperative outcomes in older individuals are well-documented and include increased hospital length of stay, higher mortality, and higher rate of complications.4-6 Aside from conventional operative risk factors such as smoking, heart and liver disease, and obesity, there are challenges to assessing individual patient risk, especially in geriatric patients who may have unique risk factors.7-11 Objective measures are needed for preoperative assessment of frailty and complication risk in geriatric patients undergoing spine surgery.
Frailty is an age-related state of physiological decline shown to correlate with poorer postoperative outcomes.5,12 Current frailty risk assessments include the Fried Frailty Index, Modified Frailty Index, and Canadian Study of Health and Aging Frailty Index/Clinical Frailty Score which assess physiological metrics of muscle strength, cardiopulmonary function, and preexisting comorbidities, among others.13-15 Sarcopenia, as defined by the European Working Group on Sarcopenia in Older Persons (EWGSOP), is an age-related decline in skeletal muscle mass, muscle strength, and muscle function. 16 Of note, there is considerable clinical overlap between sarcopenia and cancer cachexia, both observed more often in older patients but with a better understanding of the etiology and pathophysiology in the cachexia. 17 Patients with sarcopenia are known to have higher rates of mortality, rates of hospitalization, and risk of falls.16,18-21 Most risk assessments focus on frailty, a broader category which may encompass sarcopenia, but few have evaluated whether the pre-intervention muscle mass of patients is predictive of clinical outcomes.
Several efforts have been made to establish muscle mass measurements as reliable indicators of sarcopenia and predictors of surgical outcomes. Eguchi et al. 22 demonstrated that sarcopenic patients, as defined by total appendicular lean muscle mass on dual-energy x-ray absorptiometry (DEXA), correlated with poor alignment and increased pain after surgery for lumbar spinal stenosis. While whole body imaging studies such as DEXA offer the most reliable assessment of total body muscle mass, they are costly, time-consuming, and are not a routine component of preoperative planning for spine surgery.16,23 Recently, cross-sectional measurements of the psoas muscle have emerged as a quick and reliable correlate of lean body muscle mass.24-27 Decreased psoas muscle cross-sectional area was shown to be an independent predictor of mortality and complications in patients with liver cirrhosis and colorectal cancer, respectively.28-30 Further, Bourassa-Moreau et al. 24 demonstrated that decreased psoas cross-sectional area was associated with postoperative adverse events and an increased 3-month mortality following surgery for metastatic spine disease. Similarly, Gakhar et al. 31 showed that decreased psoas area was a predictor of 1-year mortality in surgical decompression of spinal metastases. With computerized tomography (CT) and magnetic resonance imaging (MRI) being standard preoperative imaging for thoracolumbar surgery, psoas muscle measurements are readily available, easy to assess, and may provide a convenient means of determining low muscle mass and predicting operative risk in elective spine surgery. The lack of established psoas muscle area cut-off values for defining sarcopenia by the EWGSOP highlights the importance of expanding data on this topic. 16
The current single-center retrospective study examined high-risk geriatric patients who underwent elective thoracolumbar spine surgeries. The objective of our study was to assess whether psoas cross-sectional area, a surrogate for sarcopenia, was associated with known baseline health characteristics and predictive of perioperative outcomes in these patients. Data from existing literature suggests that lower psoas muscle mass may be associated with patient frailty and sarcopenia. Establishment of reproducible psoas measurements and associated outcomes may allow spine surgeons to better risk-stratify patients.
Methods
Protocol
This was a retrospective, single-center study that included consecutively treated patients who underwent spine surgery between January 2014 and March 2019. Patient data was prospectively collected and retrospectively reviewed in the electronic medical records system. The study protocol was approved by our institutional review board and no informed consent was required (IRB#2019-0947).
Study Population
The study population included high-risk geriatric patients who underwent elective inpatient thoracolumbar spine surgery for degenerative processes or spinal deformity. High-risk geriatric patients were defined as those ≥65 y old with select comorbidities or risk factors as described previously by Pernik et al. 32 or any patients ≥85 y old. Patients were excluded if they did not meet age and risk criteria, underwent cervical spinal surgery, oncologic spine surgery, outpatient spine surgery, or had unavailable lumbar CT or MRI studies within 6 months prior to surgery.
Psoas Muscle Measurements
Measurements were made on axial CT or MRI images of the lumbar spine, abdomen, or pelvis up to 6 months preoperatively. If multiple imaging studies were available in this timeframe, the most recent imaging was used. The Picture Archive and Communication System (PACS) freehand tool was used to trace the circumference and measure the area (mm2) of the bilateral psoas muscles in the axial plane at the midpoint of the L3 vertebral body. In the same axial plane, the L3 vertebral body area (mm2) was also measured in the same fashion and used to normalize psoas muscle measurements to a ratio (TPA/L3-VBA), referred to as the psoas muscle index (PMI). Figure 1 illustrates the psoas measurement methodology. Psoas and vertebral body measurements were conducted by MNP and WHH after training by a fellowship-trained spine surgeon (SGA). Fifteen patient images (both CT and MRI) were selected at random for independent, measurement by a fellowship-trained spinal surgeon (SGA) to assess rater reliability. MNP, WHH, and SGA were blinded to outcomes during measurement. Representative illustration of cross-sectional psoas and L3 vertebral body area measurements at the midpoint of the L3 vertebral body using the Picture Archive and Communication System freehand tool on a preoperative magnetic resonance imaging. Psoas muscle index was calculated as right psoas area plus left psoas area divided by L3 vertebral body area.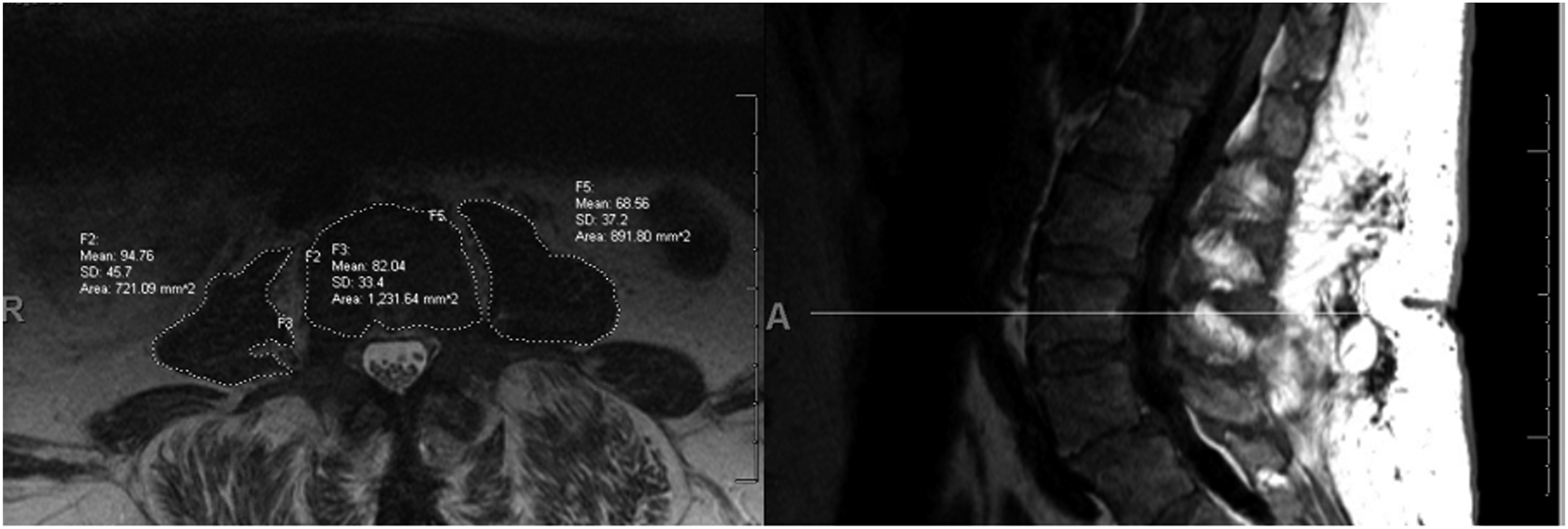
Baseline Characteristics
Demographic characteristics included body mass index (body mass index (BMI); kg/m2), age at the time of surgery, race, smoking status, and alcohol use history. Comorbidities were defined as the number of active chronic health conditions listed at the preoperative anesthesia assessment. American Society of Anesthesiology (ASA) score was also determined at this assessment. Baseline laboratory data included white blood cell count (WBC), Hemoglobin (Hb), blood urea nitrogen (BUN), and creatinine within 1 month of surgery. Polypharmacy was defined as use of >5 systemic prescription medications at the time of surgery.
Perioperative Outcomes
Surgical characteristics included levels of vertebral fusion, receipt of pelvic fixation, duration of anesthesia (min), estimated blood loss (EBL), percent Hb drop, intraoperative blood product transfusions (mL), and intraoperative albumin (mL). Percent Hb drop was calculated as preoperative Hb minus postoperative Hb within 24 h of surgery divided by preoperative Hb. Intraoperative transfusions of red blood cells (RBC), platelets, and fresh frozen plasma (FFP) were those that occurred between incision and closure and were summed to calculate total intraoperative transfusion volume. RBC transfusion thresholds were standardized at our institution to a threshold of 9 g/dL intraoperatively and 8 g/dL postoperatively regardless of patient age.
In-hospital outcomes were hospital and ICU length of stay (LOS), postoperative delirium, postoperative blood product transfusions (mL), postoperative Hb within 24 h of surgery, postoperative day of ambulation, and discharge to a skilled nursing facility (SNF). Postoperative delirium was determined by a validated chart review method.32,33 Postoperative transfusions of RBC, platelets, and FFP were those that occurred between operative closure and hospital discharge and were summed to calculate total postoperative transfusion volume. To account for variance in length of stay, RBC transfusion was normalized to hospital length of stay (mL/day). Postoperative day of ambulation was determined based on documentation in nursing, physical therapy, and occupational therapy notes. Outcomes during follow-up included all-cause 7-, 30-, and 90-day readmission, all-cause mortality during follow-up, pseudoarthrosis, and receipt of revision surgery. Mortality was determined using the Ancestry® death registry (Ancestry.com LLC, Lehi, Utah).
Statistical Analysis
Patients were divided into quartiles based on normalized psoas area measurements. Patients in the fourth quartile (Q4) were compared to patients in quartiles 1 through 3 (Q1-3). Descriptive statistics were calculated as means with standard deviations or rates. Interrater reliability of psoas measurements was analyzed with a two-way mixed intraclass correlation model and reported as Cronbach’s Alpha. Continuous variables were assessed for parametricity using Levene’s Test for Equality of Variances. Continuous variables were compared with a two-sided independent samples t-test if parametric, and a Welch’s t-test for non-parametric data. Rates were compared using χ2, or a Fischer’s Exact test when n < 5 for a single observation. Mortality, pseudoarthrosis, and revision surgery during follow-up were analyzed with Kaplan–Meier survival Log-Rank (Mantel-Cox) test. Data analysis was performed using the Statistical Package for the Social Sciences (v24; IBM Corporation, Armonk, NY).
Results
Study Population
Our database contained 324 patients, and after exclusion criteria were applied, 196 patients were eligible for study enrollment. The mean age was 73.4 years (SD = 5.10) and 46.4% (n = 91) were male. The mean normalized psoas area was 1.30 (Range: .60–2.25). PMI intraclass correlation was high (Cronbach’s Alpha = .96; P < .001) indicating excellent interrater reliability. The normalized psoas area cut-off for Q4 was < 1.05. Q4 included 48 patients with a mean PMI of .90 (SD = .11) and Q1-3 included 148 patients with a mean PMI of 1.44 (SD = .29; P < .001). The availability of CT vs MRI used to measure preoperative PMI did not differ significantly between groups.
Demographic and Clinical Characteristics
Preoperative Demographic and Clinical Characteristics.
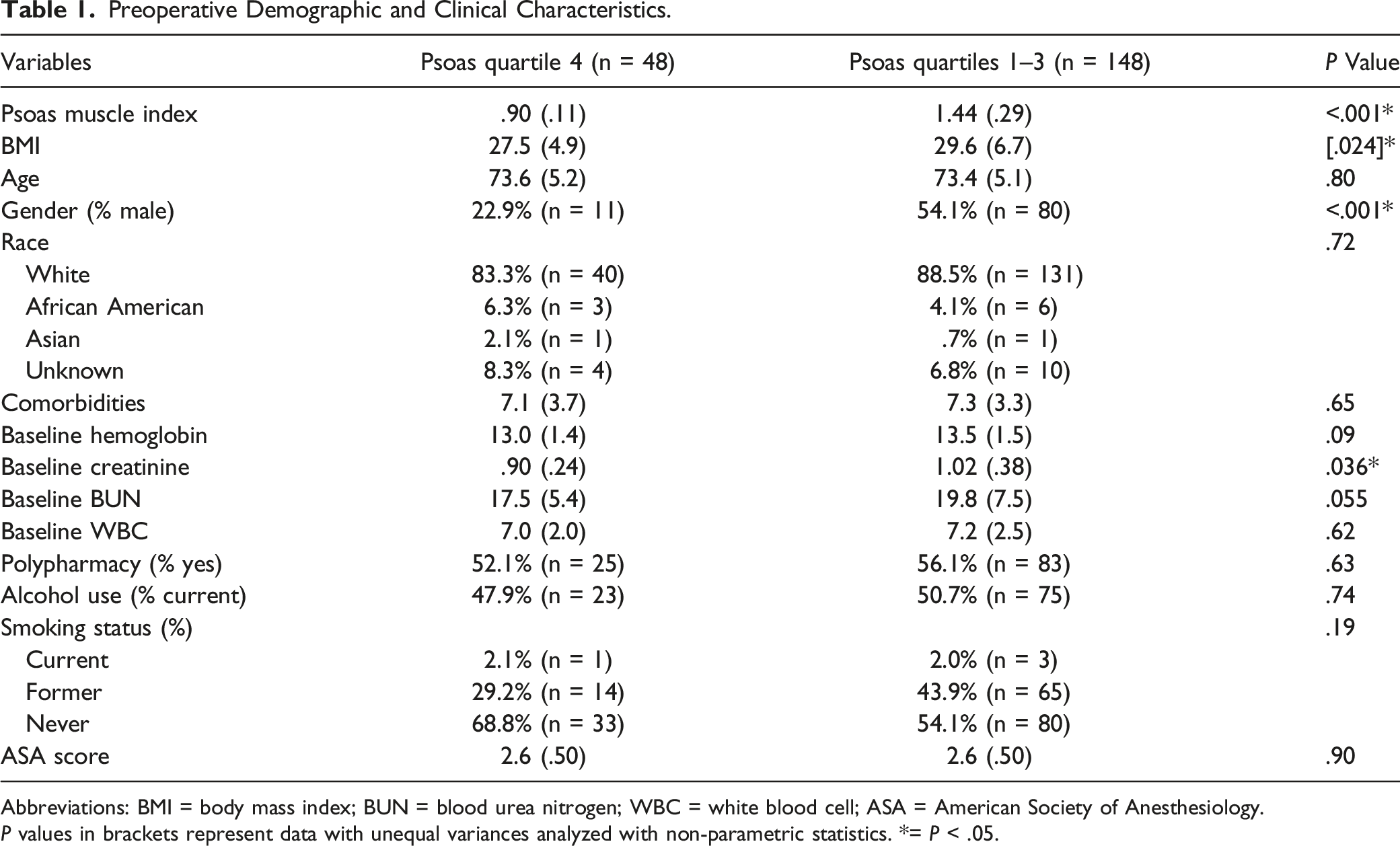
Abbreviations: BMI = body mass index; BUN = blood urea nitrogen; WBC = white blood cell; ASA = American Society of Anesthesiology.
P values in brackets represent data with unequal variances analyzed with non-parametric statistics. *= P < .05.
Perioperative Outcomes
In-Hospital Outcomes.
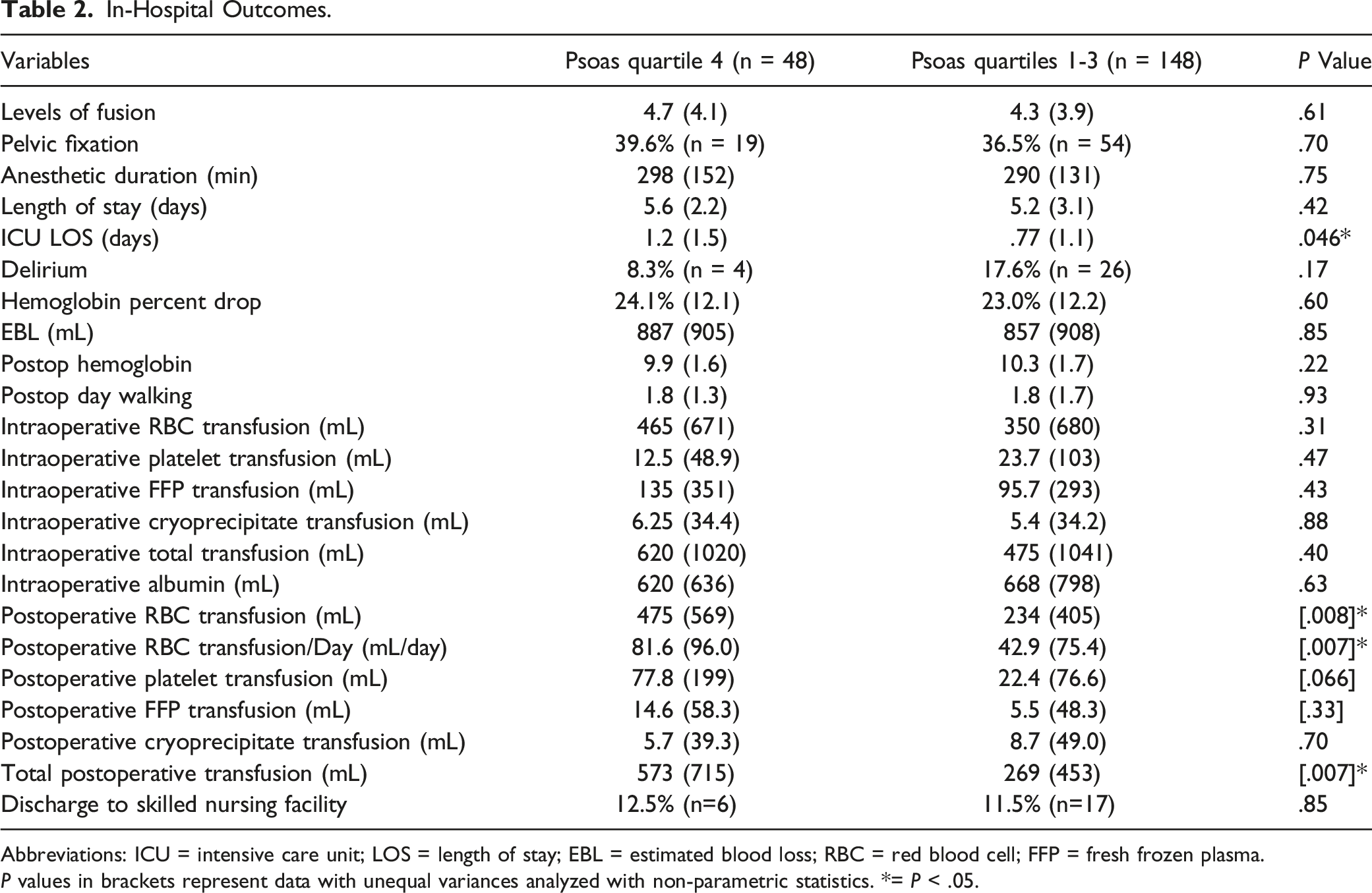
Abbreviations: ICU = intensive care unit; LOS = length of stay; EBL = estimated blood loss; RBC = red blood cell; FFP = fresh frozen plasma.
P values in brackets represent data with unequal variances analyzed with non-parametric statistics. *= P < .05.
Outcomes During Follow-Up.
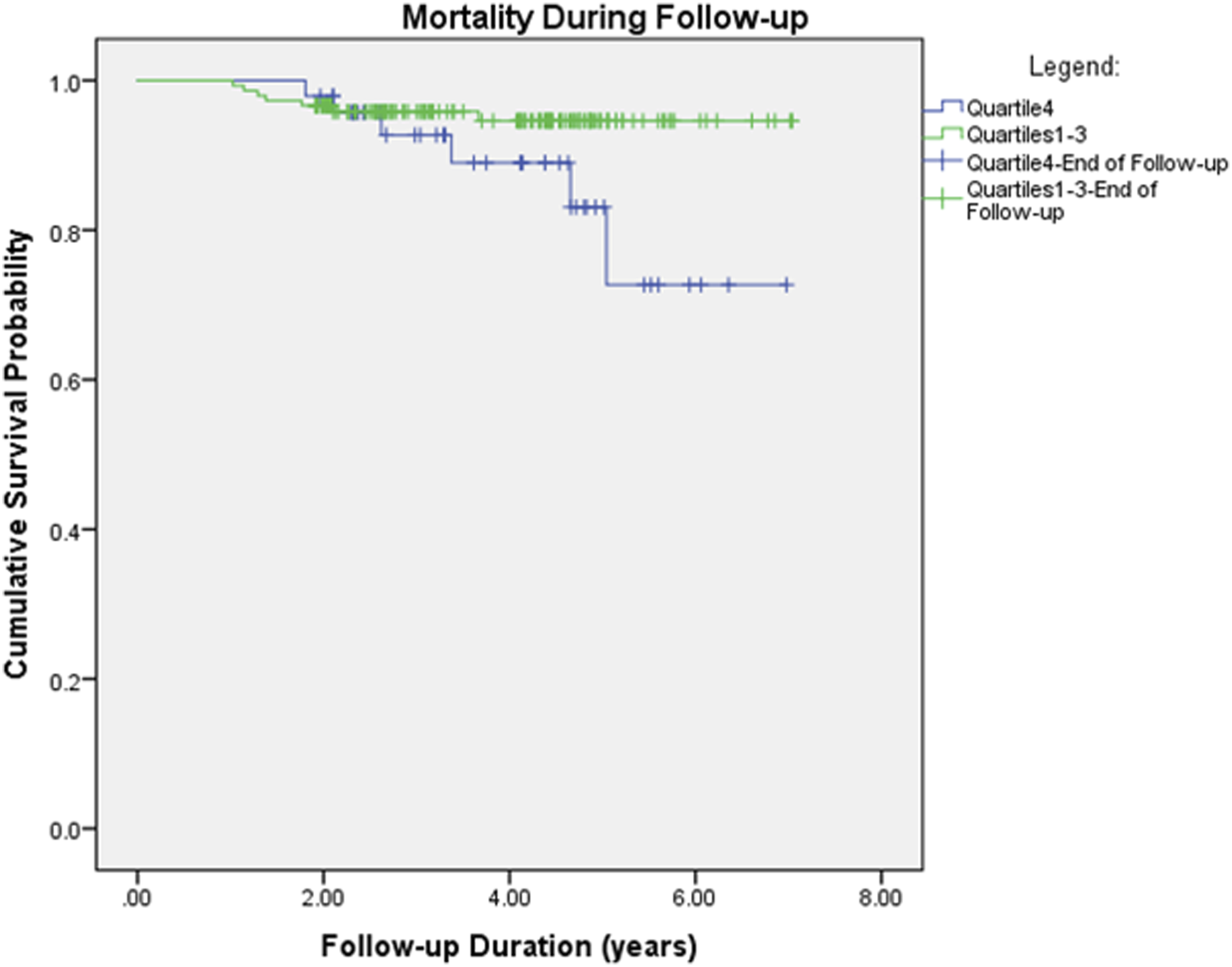
Kaplan–Meier survival curve of mortality during the follow-up period (P = .075).
Discussion
Sarcopenia is a well-established underlying health condition in the geriatric population and is known to present additional risks in the surgical management of patients. 34 Sarcopenia has been associated with increased perioperative mortality, hospital LOS, reoperation rates, readmission rates, and adverse events in studies using conventional means and psoas muscle measurements to define muscle mass.24,35-42 Advanced perioperative geriatric care programs like the Perioperative Optimization of Senior Health (POSH) Program and Hospital Elder Life Program (HELP) have improved elective surgical outcomes in high-risk geriatric populations; however, enrollment in these programs is often resource intense.32,43-45 This points to the need for efficient and cost-effective improvements in preoperative risk assessments. The present study reveals an association between lower preoperative PMI, a proposed correlate of sarcopenia, and perioperative outcomes in high-risk geriatric population undergoing elective thoracolumbar spine surgery. Our findings support the relevance of psoas muscle measurements in preoperative planning for spine surgery in geriatric patients.
While the gold standard of diagnosis of muscle mass is with DEXA, several studies have used psoas muscle measurements on other imaging modalities to assess patient muscle mass.23-25 Preoperative evaluation of sarcopenia via PMI—the total psoas area normalized to the L3 vertebral body area—has been shown to correlate with surgical outcomes as prior noted, indicating its potential prognostic capability.31,46 PMI may be a better predictor of surgical outcomes compared to other methodologies like cross-sectional area of paraspinal muscles which was not associated with outcomes following single-level lumbar fusion. 47 A significant limitation of assessing sarcopenia via PMI is the lack of defined cut-off values for classifying patients as sarcopenic vs non-sarcopenic. 16 Stratifying patient PMI by quartile resulted in a potential PMI cut-off of 1.05, however, additional research is necessary to evaluate whether this is a relevant cut-off in other patient populations.
Preoperatively, patients in Q4 PMI were similar in age and race pointing to the absence of major demographic influences. However, a greater proportion of patients in Q4 PMI were female (% male, 22.9% Q4 vs 54.1% Q1-3; P = <.001). While some studies find that sarcopenia is more prevalent in women, other studies find no difference.48-50 The similarity in baseline laboratory values, comorbidities, and smoking status indicates homogeneity of baseline health status in our patient population. While Q4 had a significantly lower BMI compared to Q1-3, this may be expected given these patients may have been more frail. Q4 patients were also found to have a lower serum creatinine, but the observed values are roughly equivocal from a clinical standpoint and the significance is undetermined.
We find the lower quartile of PMI was associated with increased ICU LOS. This indicates that patients with lower PMI may be more likely to require prolonged intensive care in the immediate postoperative period. Similarly, Toptas et al. 51 , find that in a series of hospitalized ICU patients, sarcopenic patients had longer ICU LOS and higher mortality. Nonetheless, further investigation is needed to establish the reason for increased ICU LOS in postoperative patients with PMI defined sarcopenia as our data does not address this question and the modest effect size seen in our data may not be clinically significant. While we did not find a difference in total hospital LOS, several studies report associations between decreased psoas mass and increased hospital LOS.39,40,52 In a study on patients undergoing complex thoracolumbar revision surgery, Hirase et al. 40 found an increase in hospital LOS in addition to 30-day readmission and reoperation rates in patients with lower psoas mass. However, our study included all elective inpatient spine surgery in which patients undergoing smaller non-deformity and non-fusion were likely to have robust postoperative recoveries. Consistent with our findings, Charest-Morin et al. 53 revealed total psoas area defined sarcopenia was not predictive of hospital LOS in elective thoracolumbar spine surgery. Thus, PMI may be a reliable predictor of postoperative ICU LOS, but may only predict total hospital LOS in patients undergoing complex surgery.
The lowest PMI quartile was also associated with increased postoperative blood transfusion requirements. Patients in the Q4 PMI received over twice the RBC and total transfusion volume compared to patients in the lower quartiles despite having nondifferent preoperative Hb, Hb percent drop, and EBL. While there was no significant association with transfusion of platelets, cryoprecipitate, or FFP, this may have been due to the infrequent use of these products in our cohort. Our results are consistent with findings from Hirase et al. 40 and Bokshan et al. 39 which showed approximate 4-fold and 2-fold higher likelihood of postoperative blood transfusion in patients with lower psoas mass following thoracolumbar spine surgery, respectively.40,54 Similarly, sarcopenic patients undergoing reconstructive head and neck surgery were found to have increased rates of blood transfusion.55,56 Interestingly, we found no association between PMI and intraoperative blood transfusion requirements, pointing to challenges in postoperative recovery in sarcopenic patients as opposed to the intraoperative period. Together, the increased ICU LOS and likelihood of postoperative transfusions are important considerations in the preoperative planning and perioperative management of spine surgery patients.
Although there was a large relative increase in the mortality in Q4 patients (12.5 vs 4.7%), the difference in mortality during follow-up was not statistically significant (P = .075) However, the relative difference in these values, the lack of power in our current study, and mortality differences reported in existing literature points to a clinically important difference. Several existing studies find a significant association between sarcopenia and mortality following spine surgery and abdominal surgery.24,31,38,39,57-59 The lack of statistical significance in our study may have stemmed from a lack of power. With limited availability of established cut-off values for assessing sarcopenia via psoas muscle measurements and mortality, a power analysis to inform study enrollment was not possible. Post hoc power analysis indicated of the current enrollment revealed a power of 7.7% to detect a difference. An enrollment of 416 patients would have increased our power to 80%, provided mortality rates and distribution between PMI in Q4 and Q1-3 remained constant.
The present study had several limitations. First, our retrospective design may have introduced confounding factors that were not measured. Next, the patient population included high-risk geriatric patients, thus, our results may not represent the broader population of patients undergoing spine surgery. Additional work is needed to investigate PMI cut-offs and outcomes in a broader spine surgery population. The lack of established sarcopenia psoas muscle area cut-off values by the EWGSOP limited the comparison between sarcopenic and non-sarcopenic groups. 16 Cut-off values for sarcopenia using psoas measurements have been established in select populations, but it is unclear if this is consistent with DEXA-based diagnosis in our patient population. Further, the lack of information regarding muscle strength and function limits our delineation of sarcopenic patients based solely on muscle mass. While Q4 psoas measurements served as a stand-in for a sarcopenic cut-off, there may have been overlap in true clinical sarcopenia between the groups. However, a secondary aim of this paper was to contribute to the data supporting psoas muscle measurements as an indicator of sarcopenia. Our study also included multiple surgeons, which may have influenced results due to individual provider treatment decisions, perioperative management, and/or surgical technique. Lastly, the retrospective nature of the psoas muscle measurements may have introduced observer bias. In an effort to minimize this bias, outcomes were blinded during measurements and we assessed interobserver reliability via comparison of measurements collected between observers and with that of an independent blinded observer.
Conclusion
Our study finds that lower PMI, a correlate of sarcopenia, was associated with an increased ICU LOS and a higher incidence of postoperative blood transfusion in high-risk geriatric patients undergoing elective inpatient thoracolumbar spine surgery. Further research is required to validate our proposed psoas muscle measurement cut-off value to ensure it reliably indicates true sarcopenia and has predictive value for perioperative outcomes in broader spine surgery populations. With additional research, preoperative psoas muscle measurements would provide a convenient marker in the preoperative surgical risk assessment algorithms for geriatric patients undergoing spinal surgery. Once validated, psoas muscle mass could be considered in concert with other known perioperative risk factors to produce risk-prediction models.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Bagley receives royalties from K2M/Stryker. The remaining authors have no conflicts of interest to report.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the UT Southwestern Department of Neurological Surgery
IRB statement
This study was written in compliance with our institutional ethical review board (IRB#2019-0947)