
Abstract
Study Design
Retrospective Comparative Study, Level III.
Objective
In patients with scoliosis >90°, cranio-femoral traction (CFT) has been shown to obtain comparable curve correction with decreased operative time and blood loss. Routine intraoperative CFT use in the treatment of AIS <90° has not been established definitively. This study investigates the effectiveness of intraoperative CFT in the treatment of AIS between 50° and 90°, comparing the magnitude of curve correction, blood loss, operative time, and traction-related complications with and without CFT.
Methods
73 patients with curves less than 90° were identified, 36 without and 37 with cranio-femoral traction. Neuromuscular scoliosis and revision surgery were excluded. Age, preoperative Cobb angles, bending angles, and curve types were recorded. Surgical characteristics were analyzed including number of levels fused, estimated blood loss, operative time, major curve correction (%), and degree of postoperative kyphosis.
Results
Patients with traction had significantly higher preoperative major curves but no difference in age or flexibility. Lenke 1 curves had significantly shorter operative time and improvement in curve correction with traction. Among subjects with 5 to 8 levels fused, subjects with traction had significantly less EBL. Operative time was significantly shorter for subjects with 5-8 levels and 9-11 levels fused. Curves measuring 50°-75° showed improved correction with traction.
Conclusion
Intraoperative traction resulted in shorter intraoperative time and greater correction of major curves during surgical treatment of adolescent idiopathic scoliosis less than 90°. Strong considerations should be given to use of intraoperative CFT for moderate AIS.
Introduction
Adolescent idiopathic scoliosis (AIS) is defined as a coronal curvature of the spine greater than 10° and occurs in 1-3% of otherwise healthy adolescents. 1 Advances in techniques and instrumentation, from the Harrington rod to widespread use of thoracic pedicle screws, has allowed surgeons to achieve significant 3-dimensional correction of spinal alignment. However, the surgical correction of AIS is associated with longer operative times and greater blood loss than most other pediatric procedures. 2 Therefore, studying interventions that may reduce operative time and blood loss are critical.
There are few studies in the literature studying the routine use of intraoperative cranio-femoral traction (CFT) in the treatment of AIS curves measuring less than 90°. 8 As surgical treatment of AIS is typically recommended once curves exceed 50°, most scoliosis surgeons are quite familiar with reduction strategies employed when treating these patients. In patients with severe rigid scoliosis in whom curve sizes are greater than 90°, the use of halo-femoral traction both before and during an operation has been shown to vastly improve curve correction.3–5 Recent reports suggest that the use of CFT may supplant the need for anterior release and the associated morbidity of entering the thoracic cavity. 6 The aim of this study is to assess the potential risks and benefits of routine intraoperative CFT when surgically treating AIS with major curves ranging between 50° and 90°.
Materials and Methods
Institutional Review Board (IRB) approval, exempt of informed consent, was obtained prior to accessing patient medical records. A retrospective review of electronic medical records and the picture archiving and communication system (PACS) was performed for review of preoperative and initial standing postoperative patient radiographs prior to discharge. Inclusion criteria were age less than 18 years, diagnosis of AIS with curve 50° to 90°, and posterior only fixation with or without intraoperative CFT. Exclusion criteria consisted of neuromuscular scoliosis and revision surgery. All surgeries were performed at the same pediatric tertiary referral hospital between 2006 and 2017 by 3 fellowship trained surgeons. All surgeons, following an institutional protocol, used traction in the same manner: 50% body weight, with half of traction weight divided between the head and lower extremities. Variables analyzed included patient age at index operation, gender, preoperative major curve measurement, Cobb angle on bending radiographs, percentage correction, and curve type based on Lenke classification (Types 1-6).
Surgical characteristics and outcomes for the traction and no traction group were analyzed including number of levels fused, implant density, number of osteotomies, estimated blood loss (EBL), operative time, percent correction of major curve (%), and degree of postoperative kyphosis. Operative time was defined as time from incision to wound closure. Sub-analysis of the traction and no traction group was performed for each Lenke curve type; number of levels fused: five to eight (5-8), nine to eleven (9-11), twelve and above (>12); percent correction of curve, curve severity (<60°, 60-75°, 75-90°), and percent correction of each curve in subjects with multiple curves.
Continuous outcomes were compared between groups using two-sample t-tests. Categorical outcomes were compared between groups using the chi-square test. Analyses were conducted using R, version 3.5.0 (R Core Team, 2018).
Technique of Traction and Surgical Technique
After administration of anesthesia, traction is applied to the head using Gardner Wells tongs (Integra Life Sciences) and bilateral distal femora using smooth .062 Kirschner wires placed from medial to lateral approximately 2 cm proximal to the patella. Knee flexion is maintained during insertion to protect vascular structures. Traction bows are used in a standard fashion for skeletal traction and soft tissue padding is placed between the K-wires and bow medially and laterally to prevent soft tissue damage. In order to prevent pressure ulceration, the pre-tibial region is padded with foam and secured with Coban (3M). Once patients are placed in the prone position, the patient’s knees are flexed to ensure that there is no contact between the traction bow and the lower leg. Balanced in-line traction is applied to a standard amount of fifty percent of body weight divided between the head and lower extremities (Figure 1). Standard surgical technique included a posterior midline approach to the spine. In all cases, routine facetectomies were performed during exposure and screw placement; radical soft tissue and facet resection (Ponte osteotomies) were performed in cases demonstrating excessive stiffness despite all other adjunctive intraoperative measures. In nearly all cases, segmental pedicle screw fixation was applied for deformity correction. Routine motor and sensory neuromonitoring was used for all cases. Blood loss was estimated using cell-saver volumes, as well as surgical and anesthesia estimates. Intraoperative cranio-femoral traction set up for adolescent idiopathic scoliosis.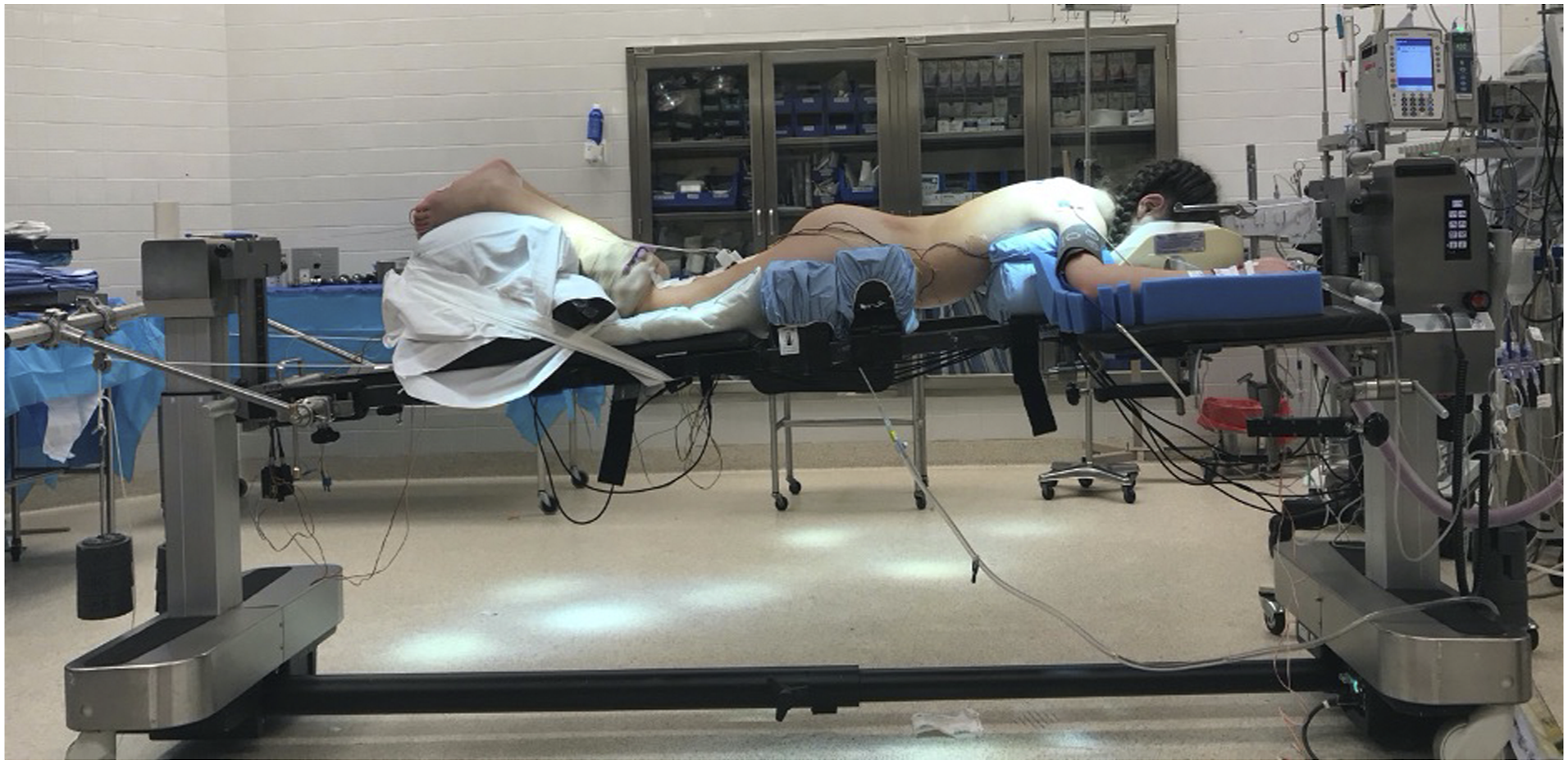
Results
Subject Baseline Characteristics.
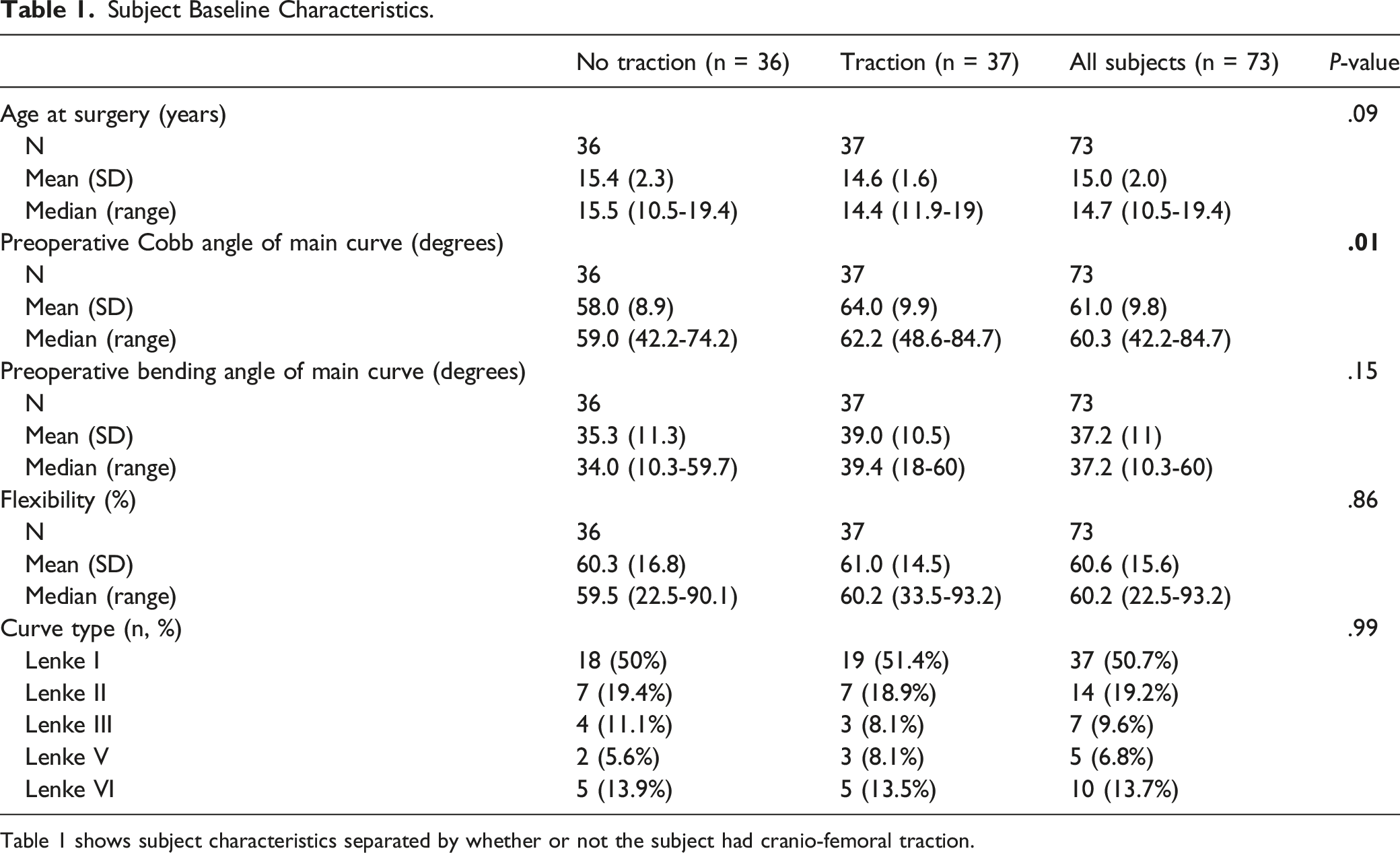
Table 1 shows subject characteristics separated by whether or not the subject had cranio-femoral traction.
Surgical Characteristics and Outcomes by Traction.
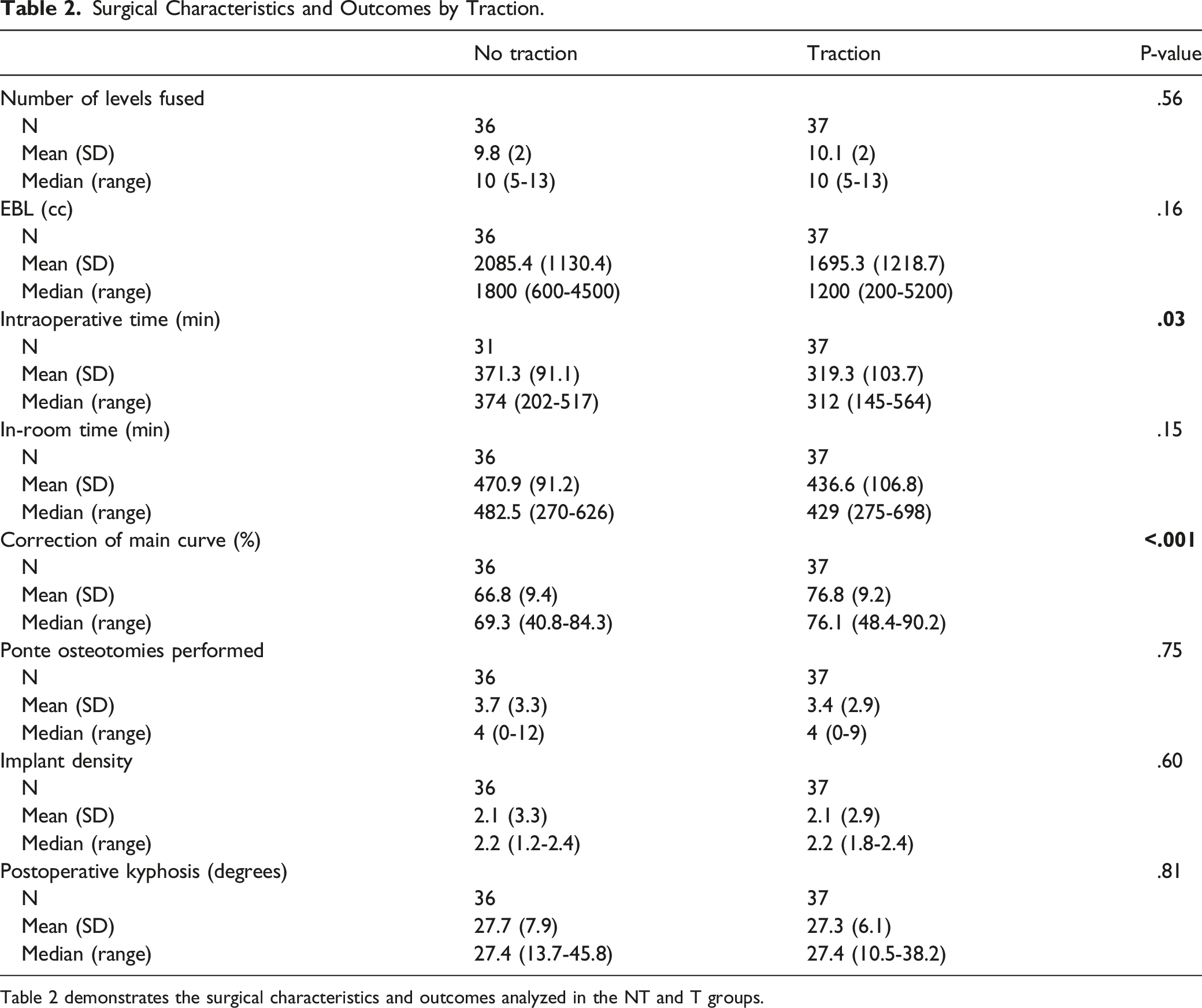
Table 2 demonstrates the surgical characteristics and outcomes analyzed in the NT and T groups.
Surgical Outcomes by Curve Type and Traction.
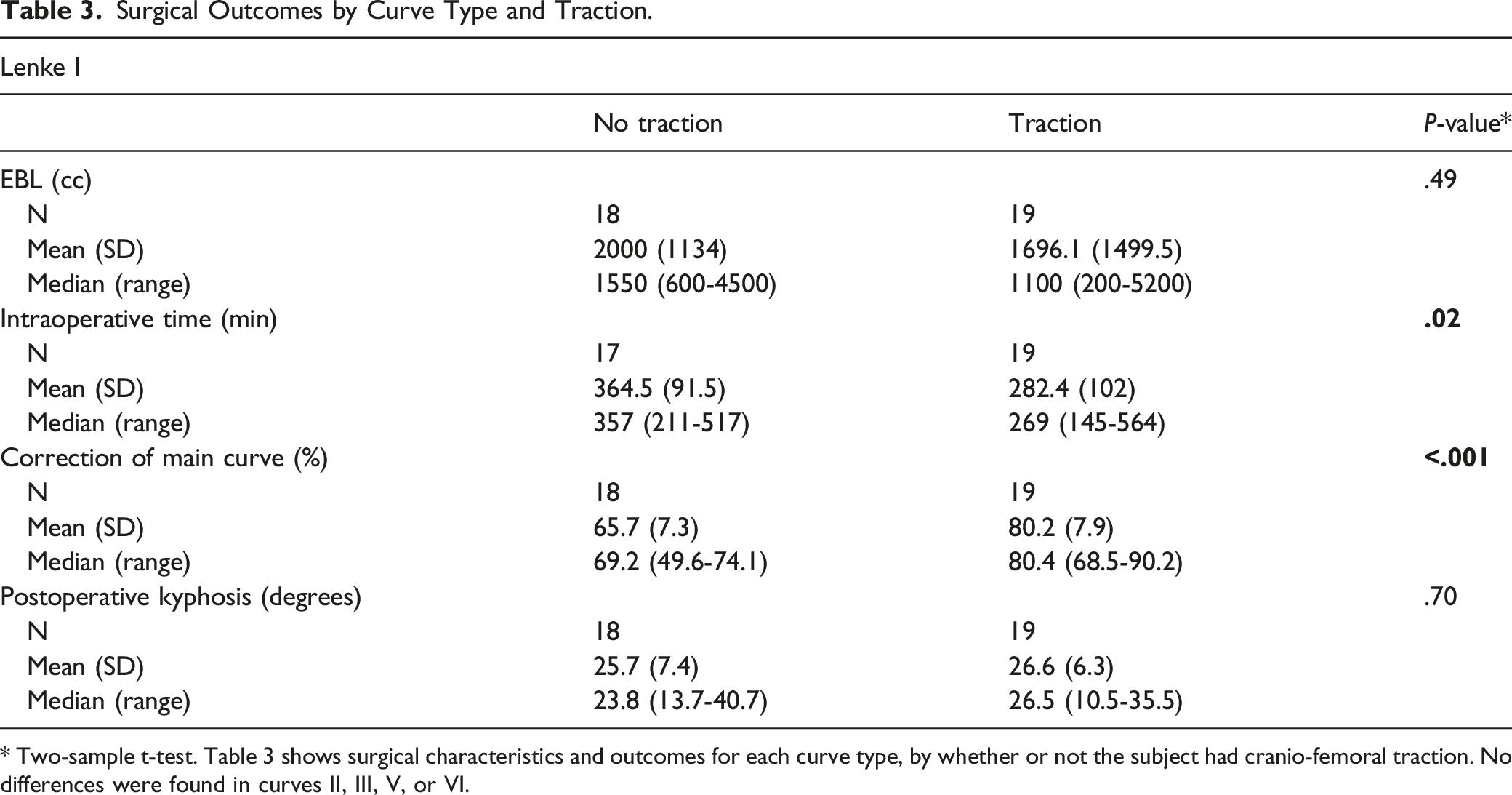
* Two-sample t-test. Table 3 shows surgical characteristics and outcomes for each curve type, by whether or not the subject had cranio-femoral traction. No differences were found in curves II, III, V, or VI.
Surgical Outcomes by Number of Levels Fused and Traction.
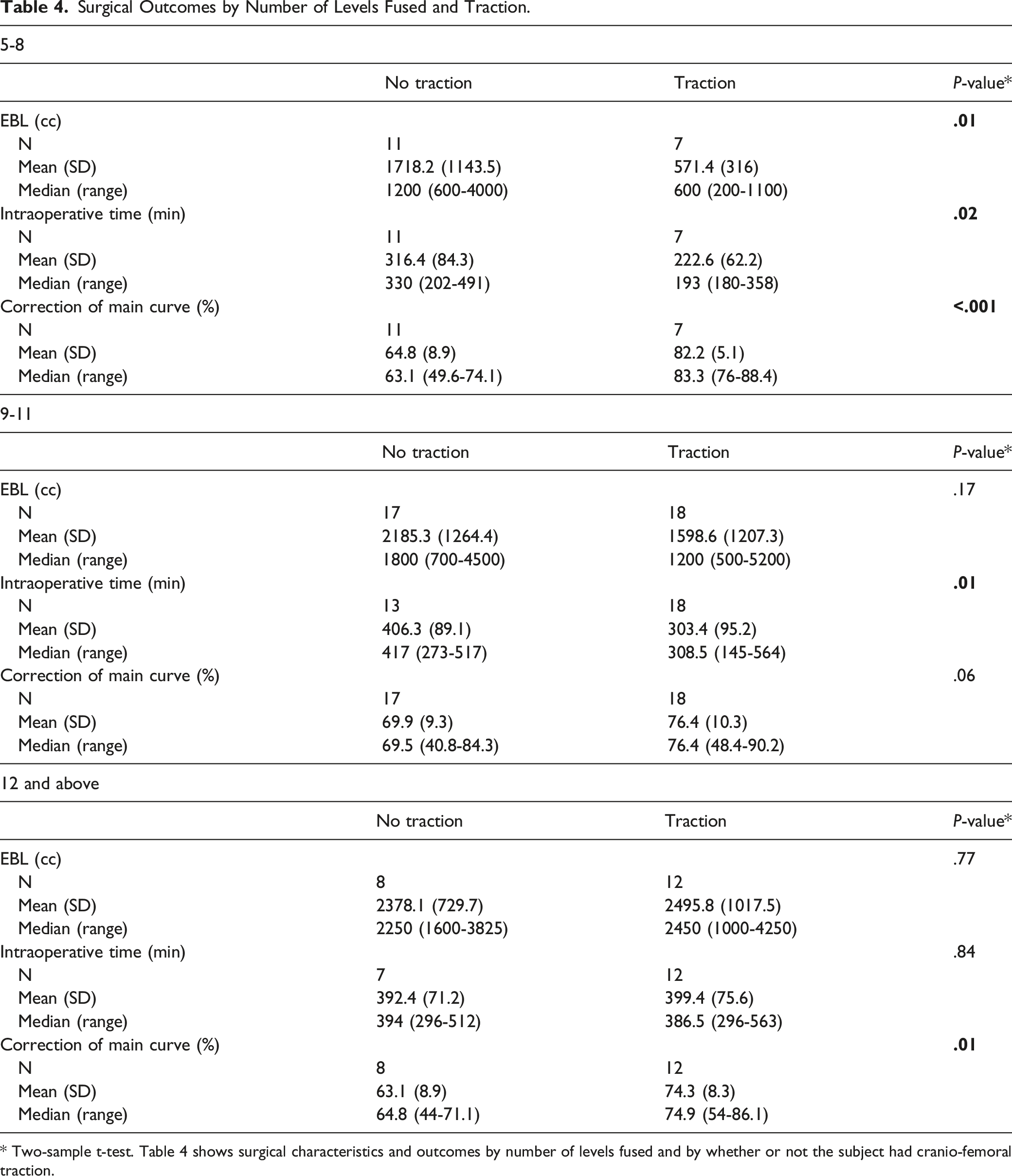
* Two-sample t-test. Table 4 shows surgical characteristics and outcomes by number of levels fused and by whether or not the subject had cranio-femoral traction.
Surgical Outcomes by Flexibility and Traction.
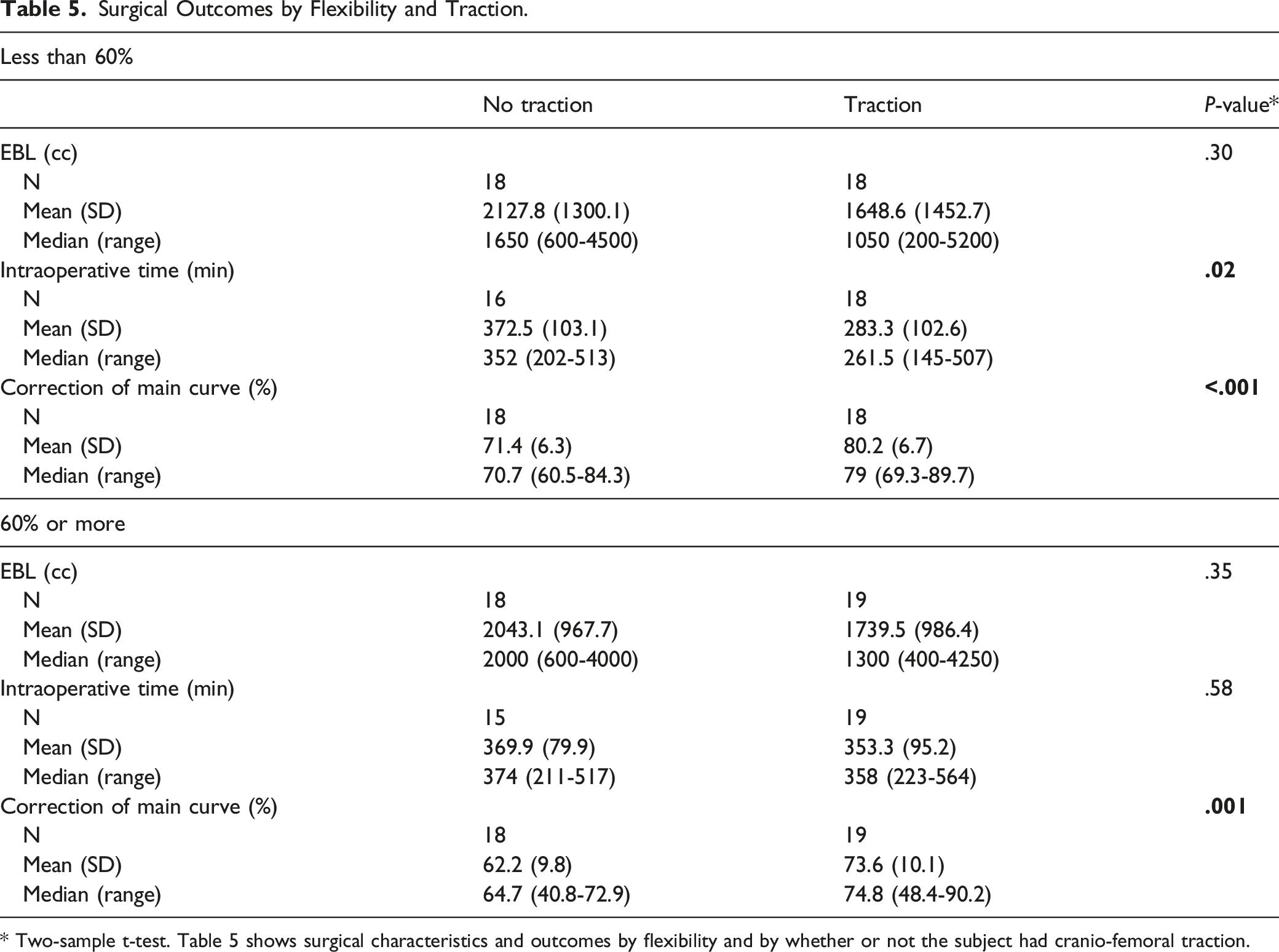
* Two-sample t-test. Table 5 shows surgical characteristics and outcomes by flexibility and by whether or not the subject had cranio-femoral traction.
Surgical Outcomes by Curve Severity and Traction.
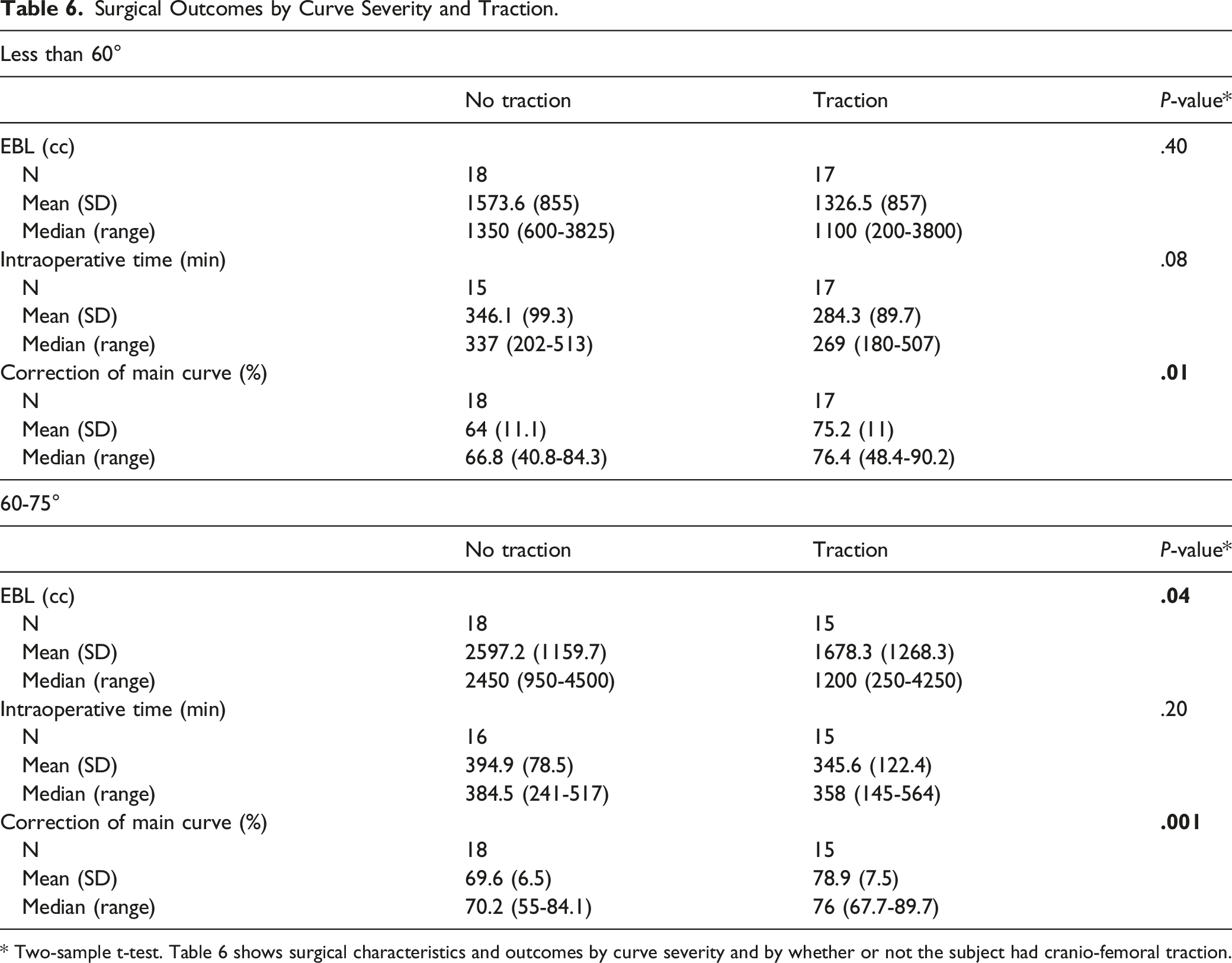
* Two-sample t-test. Table 6 shows surgical characteristics and outcomes by curve severity and by whether or not the subject had cranio-femoral traction.
Discussion
Surgical correction of AIS is associated with longer operative times and higher blood loss totals than many surgical procedures in the pediatric population. 7 The use of perioperative traction in the treatment of severe scoliosis has been well documented in the literature as an adjunct to surgical scoliosis correction.1,5,8–11 Preoperative halo-gravity traction (HGT) has demonstrated utility in improving curve correction and may decrease neurological risk when used in patients with Cobb angles exceeding 100°. 6 Furthermore, its use has been shown to result in lower operative blood loss.1,6,7 Iyer et al sought to examine the role of HGT in reducing preoperative surgical risk. They found that operative risk scores were decreased, curve magnitude improved, and rate of three-column osteotomies decreased from 91% to 38%. 8 The role of CFT in AIS curves less than 90° is less clear. In the present study, we analyzed AIS patients with curves less than 90° to identify whether CFT would affect magnitude of curve correction, EBL, and operative time.
In our cohort of AIS patients with major curves between 50° and 90°, the use of intraoperative CFT resulted in significantly greater curve correction than those without traction, as well as significantly lower operative times. Our results corroborate prior investigations which demonstrated that intraoperative CFT was an effective method for correction for curves between 70° and 90°, resulting in an overall curve correction rate of 85.7%. 5 A previous retrospective study of AIS patients did not demonstrate any significant difference between preoperative HGT and control groups in coronal or sagittal curve correction, EBL, operating time, or complications. However, this study was for curves averaging 93° to 105° and flexibility of only 20%. 9 Additionally, these groups received preoperative HGT compared to our intraoperative CFT group.
Despite having greater preoperative Cobb angles, patients with Lenke 1 curves in our study had significantly greater correction with CFT than without and were the only group to show a significant difference. Additionally, these patients had significantly shorter operative times despite having stiffer curves as represented by their larger preoperative bending angles. As this is the most common curve type in the AIS population, this demonstrates the potential applicability of this adjunct intervention in the surgical correction of AIS.
Previous authors studying traction methods have attempted to define rigid curves as those with Cobb angles >70° and those that cannot be reduced by >35% on bending radiographs. 10 Knowing that traction serves as an adjunctive measure to facilitate curve correction in severe scoliosis, we sought to find if there is a lower limit of curve size that one would consider not using traction. We believe this study answers this question as summarized in Table 6. We analyzed patients in whom curves were just above the 50° threshold for operative treatment (50°-60°) and those that were well above the minimal surgical threshold (60°-75°). In the patients whose curves ranged between 50° and 60°, better correction was achieved in the T group averaging 75% correction compared to the NT group averaging only 64% correction. For curves ranging between 60° and 75°, we also observed improved correction with the use of CFT. In the 17 patients in the traction group, the average curve correction was 79%. In the NT group, by contrast, the percentage correction of the main curve averaged 70%. While this result was statistically significant, it could be argued as to whether this was a clinically significant difference. As there is difficulty establishing a minimal clinically important difference using process measures for scoliosis correction, we may not be able to demonstrate the value of this increase in correction. Within the 60°-75° range, the NT was associated with a higher average blood loss of 2.6 L while the T group had an average blood loss of 1.7 L. Within the retrospective nature of the study, it is difficult to analyze all of the contributors to blood loss estimates; however, within our single hospital center anesthetic protocols, use of antifibrinolytics and other adjuvants was similar among the surgeons. Additionally, the number of Ponte osteotomies was similar between the traction and no traction groups. It is our interpretation, then, that CFT makes scoliosis correction faster with less blood loss, and therefore, we argue that the minimal clinical morbidity of traction placement is outweighed by the positive benefit.
Interestingly, patients with stiffer curves, less than 60% curve correction, showed significantly decreased operative times while those with more flexible curves did not reach significance. This suggests the greatest impact of CFT is seen in patients with stiffer curves; however, both groups showed significantly increased correction. When analyzing the levels fused, for those with 5 to 8 levels fused, patients with traction had significantly less blood loss, a significantly shorter operative times, and significantly greater correction of the main curve than those in the NT group. Among subjects with 9 to 11 levels fused, patients with traction had significantly shorter operative times with non-statistically significant effects on blood loss and percent correction. Other surgical factors such as Ponte osteotomies and implant density can influence the magnitude of curve correction.12,13 Between the NT and T groups, the number of osteotomies performed, and the implant density was similar suggesting that these factors did not contribute to the observed outcome. Our findings thus far are unique in published literature on the beneficial effects of intraoperative CFT regardless of the number of levels fused.
A theoretical risk of CFT during coronal plane correction is the potential for undesired alteration of normal physiological sagittal plane contours, for example, flattening of lumbar lordosis (flatback) or worsening thoracic hypokyphosis or lordosis. In our analysis, however, there was no significant difference in kyphosis between the T and NT groups. While we believe that attention to appropriate rod contour has been mostly responsible for obtaining normal sagittal plane alignment in the instrumented spine, there are nuances in positioning of the traction apparatus and table bolsters that may contribute to favorable outcomes.
The potential for serious neurological complication and soft tissue infection has been documented in previous studies of the long term use of halo-gravity traction in the preoperative setting.10,11,14–17 In our study, we did not observe any early or late complications documented among those undergoing intraoperative CFT with respect to placement of Gardner Wells tongs or Kirschner. As our cranial tongs and traction pins were placed in the operating room under sterile conditions and remained only for a short period of time, the potential for serious complications is mitigated. Additionally, we observed no documented neuromonitoring changes within this study population.
The limitations of the present study include a relatively small sample size, the retrospective nature of our analysis, and the increased surgeon experience over the study period. While there may have been subtle differences in the anesthetic methods utilized, during the period of study, tranexamic acid was used exclusively as the antifibrinolytic agent, typically in a high dosage regimen. As the study was performed at a smaller pediatric hospital with 4 or 5 consistent board-certified pediatric anesthesiologists, all sharing a common protocol, there was exacting consistency with regards to antifibrinolytic drug dosing and anesthetic technique. During the period of study, for instance, other modalities to reduce blood loss, such as advanced electrosurgical cautery systems (ie, Aquamantys-Medtronic) or an ultrasonic bone scalpel, were not utilized as they were not available at the hospital during the period of study. Finally, there is inherent variability in estimating blood loss, and given the retrospective nature of the study, there was no standardized method for recording blood loss during the time period.
Conclusion
The use of intraoperative cranio-femoral traction enhances scoliosis correction and may be associated with shorter operative times and blood loss during surgical treatment of AIS with major curves measuring between 50° and 90°. As the placement of femoral traction pins and cranial tongs falls easily within the skillset of most orthopaedic surgeons and can be performed without complication, it should be considered a routine adjunctive method to facilitate scoliosis correction.
Footnotes
Author Contributions
Jacob R. Carl MD: Interpretation of data, manuscript preparation, and final approval of manuscript; Gurpal Pannu MD: Conception and design, data acquisition and analysis, interpretation of data, manuscript preparation, and final approval of manuscript; Evan Cherng-Yeh Chua BS: data acquisition and analysis, interpretation of data, manuscript preparation, and final approval of manuscript; Adam Bacon BS: Interpretation of data, manuscript preparation, and final approval of manuscript; Blythe Durbin-Johnson PhD: Conception and design, analysis and interpretation of data, manuscript preparation, and final approval of manuscript; Yashar Javidan MD: Conception and design, manuscript preparation, and final approval of manuscript; Eric O. Klineberg MD: Conception and design, manuscript preparation, final approval of manuscript; and Rolando F. Roberto MD: Conception and design, analysis and interpretation of data, manuscript preparation, and final approval of manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One author declares personal fees from NuVasive, personal fees from Stryker, personal fees from Alphatec, and grants from AONA Spine outside of the submitted work. One author declares personal fees from Depuy Synthes, personal fees from Stryker, personal fees from Medicrea/Medtronic, and grants and personal fees from AO Spine outside of the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences, National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Informed Consent
Investigation performed at Shriners Hospitals for Children Northern California, Sacramento, CA. UNITED STATES. IRB Number NCA1801R. Exempt from informed consent.