
Abstract
Study Design
Literature Review (Narrative)
Objective
To introduce the number one research priority for Degenerative Cervical Myelopathy (DCM): Raising Awareness.
Methods
Raising awareness has been recognized by AO Spine RECODE-DCM as the number one research priority. This article reviews the evidence that awareness is low, the potential drivers, and why this must be addressed. Case studies of success from other diseases are also reviewed, drawing potential parallels and opportunities for DCM.
Results
DCM may affect as many as 1 in 50 adults, yet few will receive a diagnosis and those that do will wait many years for it. This leads to poorer outcomes from surgery and greater disability. DCM is rarely featured in healthcare professional training programs and has received relatively little research funding (<2% of Amyotrophic Lateral Sclerosis or Multiple Sclerosis over the last 25 years). The transformation of stroke and acute coronary syndrome services, from a position of best supportive care with occasional surgery over 50 years ago, to avoidable disability today, represents transferable examples of success and potential opportunities for DCM. Central to this is raising awareness.
Conclusion
Despite the devastating burden on the patient, recognition across research, clinical practice, and healthcare policy are limited. DCM represents a significant unmet need that must become an international public health priority.
Keywords
Introduction
Degenerative Cervical Myelopathy (DCM) is an all-encompassing term for neural dysfunction secondary to cervical cord dysfunction caused by processes of a degenerative, arthritic, and/or congenital nature.1-3 It is estimated to affect up to 2% of adults 4 and is often associated with significant disability. 5 DCM can cause a wide range of symptoms, including pain, imbalance and difficulty walking, loss of dexterity, sensory loss, bowel or bladder dysfunction, and in extreme circumstances total paralysis. 2
Early diagnosis and surgical treatment can be beneficial. 6 However, many people with DCM are unfortunately not diagnosed in a timely manner, and despite appropriate yet delayed treatment at the time of their diagnosis, these individuals may have substantial residual neurological dysfunction. 7
The persistent neurologic dysfunction has life-long implications, with dependency, unemployment, and mental health difficulties prevalent.7,8 A comparison of SF-36 scores of people with chronic disease found that individuals with DCM have amongst the lowest quality of life scores. 8 Therefore, efforts to address and improve DCM patients’ quality of life should be a critical priority.
AO Spine RECODE-DCM (aospine.org/recode) REsearch objectives and COmmon Data Elements for DCM is an international consensus project which aims to accelerate knowledge discovery that can improve outcomes, by developing a set of research tools. 9 These include a James Lind Alliance research priority setting partnership, which brought together both individuals living and working with DCM, to establish the most important unanswered questions. Research prioritization aims to catalyze progress by consolidating resources on key knowledge gaps. The Number one priority identified was raising awareness amongst the public, health professionals, and funding agencies.
This article aims to contextualize the significance of this question, to illustrate the evidence that awareness is low, the potential drivers, and why this must be addressed. Finally, we will consider case studies of success from other diseases, drawing potential parallels and opportunities for DCM, some of which are already being considered.
What is the Evidence that Awareness of DCM is Low?
The lack of awareness for DCM can be demonstrated through the misconceptions that challenge diagnostic and treatment practice, but also perhaps the makeup and focus of DCM research, and relative lack of investment. It is strongly suspected that DCM is significantly under-diagnosed. 2 In one series of patients presenting with a neck of femur fracture (N = 159), 18% were identified to have undiagnosed DCM. 10 In another series of patients presenting to a neurology clinic with spastic tetraparesis (N = 585), DCM was 2.5 times more common than Multiple Sclerosis. 11 Moreover, a recent meta-analysis of MRI imaging of healthy volunteers (N = 3786, Mean Age of studies 40–66 years, with one additional study of teenagers) demonstrated that 24.2% of individuals had visualized spinal cord compression, and some series included current clinical assessment (N = 1202), providing a pooled-estimate of DCM of 2.3%. 4 This estimate of DCM in the general population is further supported by longitudinal studies of asymptomatic radiographic spinal cord compression, which noted that approximately 10% of these asymptomatic spinal cord compression patients progress to develop a clinical myelopathy overtime (range 2–12) years.12-14
The symptoms of DCM often mimic other pathological conditions, such as Carpal Tunnel Syndrome, which frequently leads to delays and misdiagnosis15,16: A survey of the Myelopathy.org community identified on average persons with cervical myelopathy wait 2–3 years, with over a third longer than 5 years, from onset of symptoms to diagnosis. 7
Research activity is also a potential surrogate of disease awareness. Dimensions Plus (Dimensions.ai, London, UK) is a proprietary bibliometric platform, indexing both published literature and research funding.
17
A comparative search of DCM, multiple sclerosis, amyotrophic lateral sclerosis, and spinal cord injury demonstrates that since 2011, DCM has received <2% of grant funding awarded compared to these other diseases (Figure 1). Whilst there are limitations to this comparison, which should not be used to suggest these other diseases are less deserving, it illustrates a significant awareness gap across the broader research environment. Certainly, given the importance of DCM to public health, a strong argument exists for funding initiatives to address this important health issue. Global Grant Funding for Research into Multiple Sclerosis, Amyotrophic Lateral Sclerosis (ALS), Traumatic Spinal Cord Injury, and Degenerative Cervical Myelopathy DCM 2011–2020. Data is extracted from Dimensions Plus (Dimensions.ai, United Kingdom), using search terms “Multiple Sclerosis,” “Amyotrophic Lateral Sclerosis,” “Spinal Cord Injury,” and “Degenerative Cervical Myelopathy” or “Cervical Spondylotic Myelopathy,” searched February 10th 2020.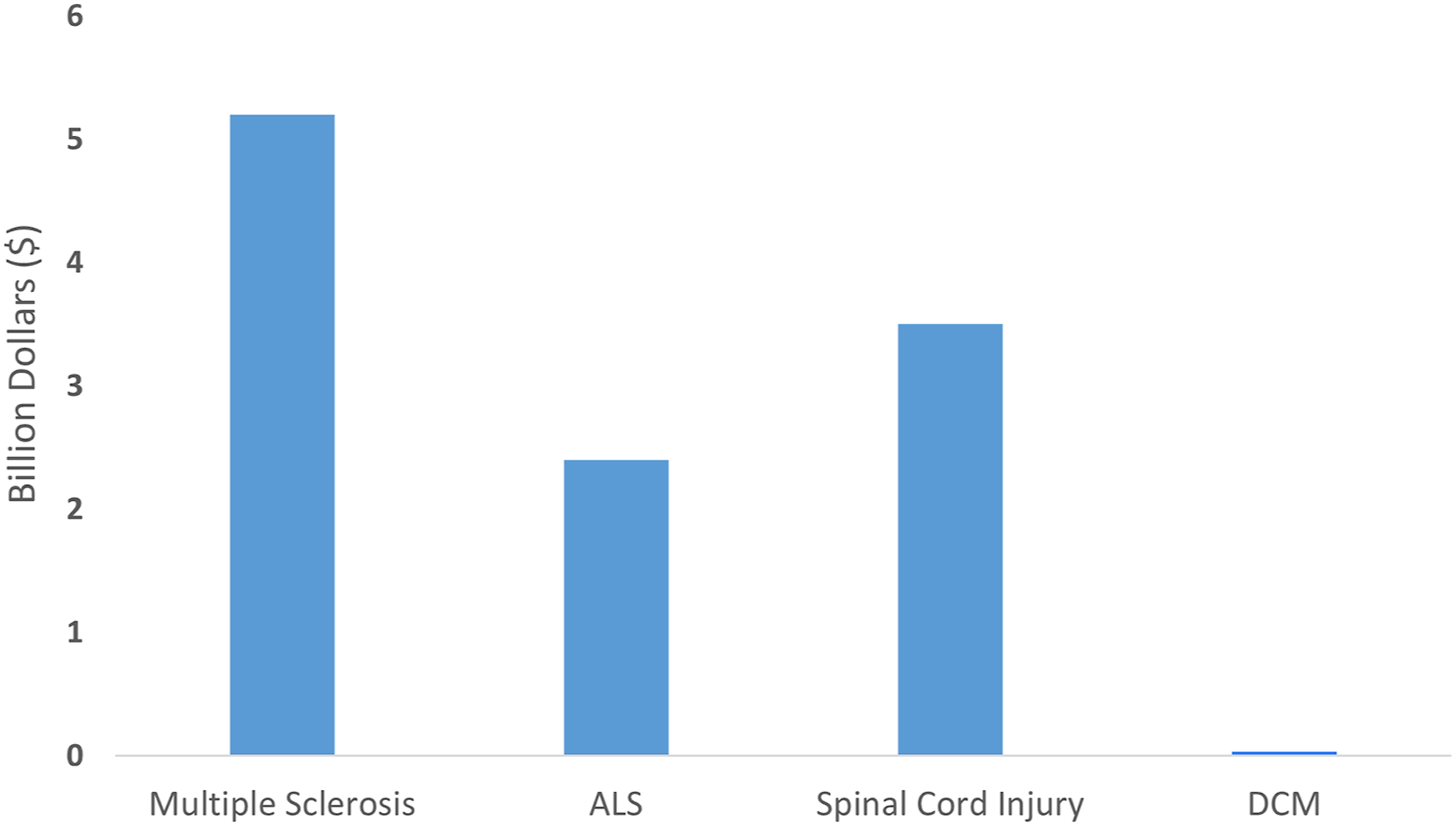
The care pathway for DCM often involves numerous specialties. 16 This is a testament to the challenges for diagnosis but also signifies the diverse and life-long disabilities that can result, even after surgical treatment. To date, these perspectives have not been well represented in DCM research, 18 with the field predominantly led by spinal surgeons. 19 In fact between 1995 and 2015, 79% of primary clinical studies, exclusively evaluating DCM in humans, evaluated cohorts undergoing surgical treatment and 55.7% specifically evaluated a surgical technique or approach. 19 Whilst this correlates with advances in the evidence guiding surgical treatment,20,21 it underrepresents the diverse issues which also exist before and after surgery, identified as priorities in this multi-stakeholder process.9,22
There are often challenges for research advances to successfully enter clinical practice. 23 Over the last decade, research has noted that DCM features captured using conventional MRI, such as the degree of compression and spinal cord signal changes, are only weakly correlated with disease severity.4,24-26 Instead, management of DCM is guided by clinical assessment of functional impairment using tools such as the modified Japanese Orthopedic association score (mJOA). 20 The 2017 International Consensus guidelines recommend surgical intervention in those patients with moderate to severe impairment, or those with mild disease in the presence of cord compression and symptomatic radiculopathy, with observation and non-operative measures considered for patients with mild disease. However, despite the publication of these guidelines, a significant heterogeneity exists in the management of DCM patients. A regional audit in the UK demonstrated that cervical MRI features of spinal cord compression was the predominant determinant of surgical vs non-operative management rather than the level of functional impairment. 27 This exemplifies the fact that even spine specialists may not be employing the most up-to-date evidence-based practice.
Why is Awareness Low?
A fundamental problem is that there is a perception that prevalence of DCM is rare.28,29 This may have arisen from early difficulties in diagnosing spinal cord compression, without advanced imaging such as MRI. However, this legacy remains, and whilst epidemiological studies in DCM still quote pooled prevalence estimates of 4-6/100,000, this data is a recognized under-estimate, relying on operative incidence, and unable to account for under diagnosis.30-32 The aforementioned 2.3% for the entire population, albeit indirect, is a more likely the most realistic estimate.2,4
Characterizing the epidemiology of DCM is also hampered by imprecise coding. DCM is referred to by numerous terms: 14 different terms were identified in our recent search of EMBASE, MEDLINE, and Clinicaltrials.gov. This inconsistency is also reflected within literature indexing and WHO ICD (International Classification of Disease) Coding, a fundamental component of epidemiology study. 32 For example, a recent review of spinal surgery for degenerative cervical spine disease in Finland used a combination of 18 different ICD codes to identify cases of DCM, with acknowledged specificity issues. 33 Efforts to raise awareness of a condition can only be diluted if multiple terms are being used.
Regardless of the terminology, DCM features poorly in medical student and general professional education programs. An evaluation of curricula and training resources for UK Medical Schools and Primary Care Training Pathways identified that DCM was rarely, if ever, specified.
34
In contrast, cauda equina syndrome, a much rarer disorder than DCM but well-publicized condition (likely owing to its medicolegal ramifications) featured more often. Despite the low representation in training, clinical knowledge as evaluated using multiple choice questions in an electronic question bank, was good (Figure 2).
34
Specifically, DCM questions were completed 127,457 times, by medical students or doctors preparing at 3 different stages: Entry into UK clinical practice (defined as medical school exit exams or the PLAB, a UK specific assessment of competency for professionals trained overseas), entry into primary care training or exit from primary care training. At each stage, users were more likely to answer DCM questions correctly, than the database average as a whole or for other neurological diseases.
34
Knowledge of DCM, compared to Multiple Sclerosis, General Neurology, Cauda Equina Syndrome, and Diabetes Mellitus amongst UK medical professions revising for entry into UK clinical practice (medical school exit exams or PLAB Professional And Linguistic Assessment Board—a UK specific assessment of competency for professionals trained overseas), entry into primary care training (SRA—Speciality Recruitment Assessment), or exit from primary care training (MRCGP—Membership Royal College of General Practitioners) (Reproduced from Ref. 34). Performance is expressed as relative to overall question bank mean. * denotes no questions included in question bank at this training stage.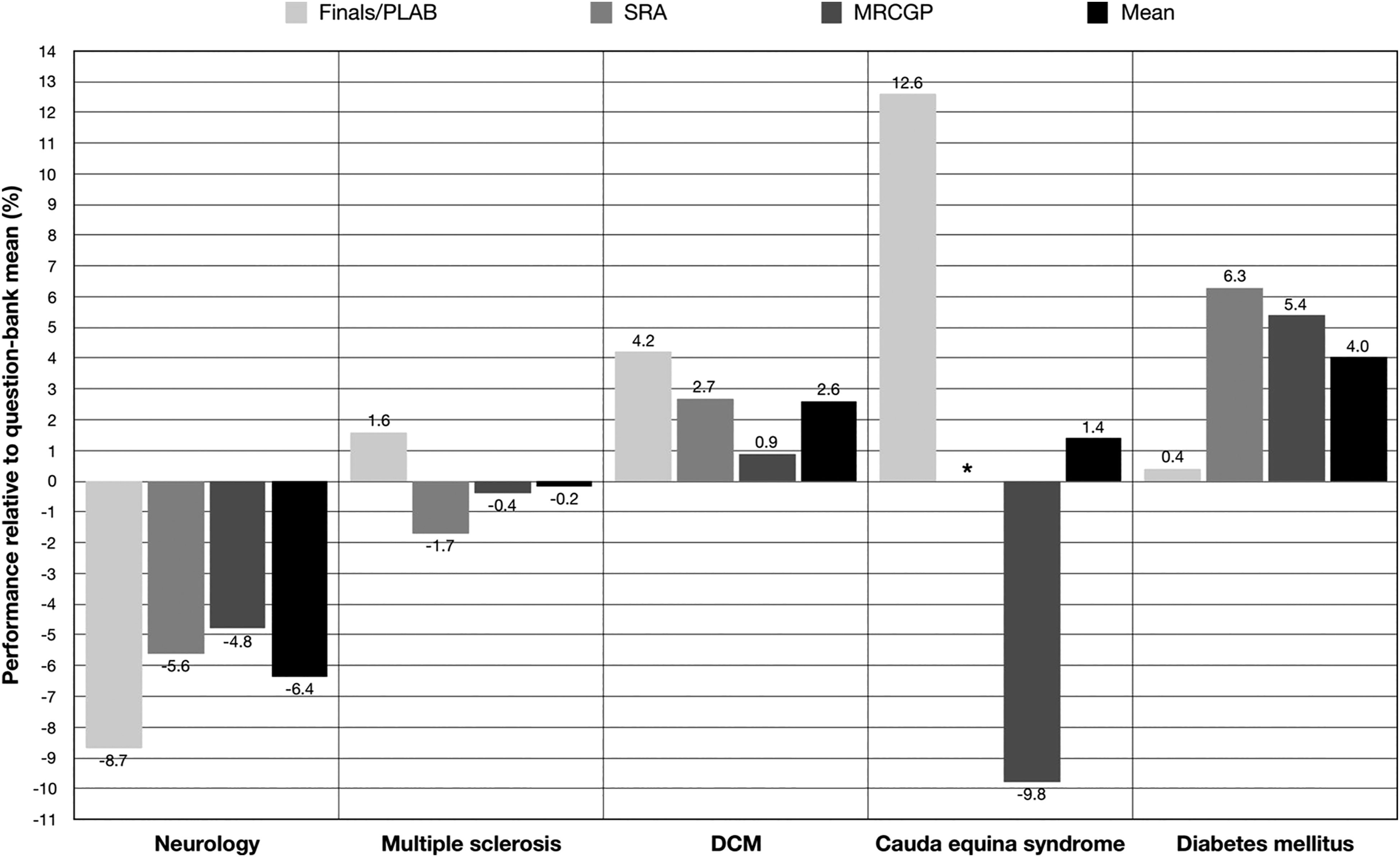
Whilst multiple-choice examination is not the same as clinical practice, associations between performance have been linked to in-practice indicators, such as clinical performance35,36 or medical board disciplinary actions. 37 The aforementioned findings therefore raise 2 additional questions. Firstly, is clinical education and current knowledge providing the right information for early detection of DCM and secondly, whilst professionals may recognize key neurological concerns on paper, do they raise the index of suspicion from clinical histories or examinations.
The presenting symptoms and duration of symptoms of DCM are often highly variable between individuals. The early features of DCM are poorly characterized, with most descriptions informed by advanced disease. 29 The recent imaging series by Martin et al 38 (2018) suggests that spinal cord damage, as identified using quantitative MRI techniques occurs prior to symptom onset or detection on conventional examination findings. Conventional diagnostic teaching has focused on neuromuscular features of the upper and lower limb29,39 but many other symptoms have also been associated with DCM, including headaches, hypertension, and respiratory dysfunction. 40 Their significance for diagnosis and early detection are unclear but unconventional symptoms such as chest pain have been shown to be potentially predictive of a distinguishing DCM from other related pathology in one study. 41 Taken together, this suggests a more complete assessment of the disability in DCM, may be important to help distinguish DCM from common differentials 29 ; for example, neck pain is reported by people with DCM, but has a population prevalence of ∼15%. 28
Physical examination is a key part of a neurological assessment of DCM. However, it has been recognized that in general, medical professionals are insecure about dealing with neurological disease. 42 This aversion was coined “Neurophobia” by Dr Ralph Jozefowicz, 43 who hypothesized that the perceived complexity of neurological disease, led to disengagement in learning and training and less proficiency as professionals. A number of professional surveys have since demonstrated this sentiment,44-46 with many professionals preferring to refer on to a “specialist”. This will inevitably add further delay in the diagnostic pathway, increasing time between presentation, diagnosis, and treatment. The neurological examination can be challenging, even in experienced hands, with signs often in fact incidental.47,48 Specialists often tailor their assessment to the specific neurological differential, without consensus on a minimum and standard assessment. 42 In a retrospective study of patients presenting with DCM to a single center, Hilton et al (2018) demonstrated the assessment was different between primary care, secondary care, and spinal surgery 49 ; in particular primary care focusing on peripheral limb strength, whereas secondary care and spinal surgery long-tract signs.
A solution to circumvent this would be a defined screening algorithm (46). Cauda Equina Syndrome (CES) has a well-defined list of “red flags” in order to prompt urgent MRI imaging. Whilst individually, or even in combination, these symptoms have a low predictive value for CES,50,51 they are better known across all healthcare professionals and used to triage immediate imaging. 34
Beyond symptoms and examination findings, MRI remains an important component of diagnosis. Unfortunately, access to MRI is challenging in many healthcare settings (49). In the UK, most primary care physicians are unable to access MRI directly, and instead patients must pass to a secondary care provider first, often waiting months for this study. 16 However access to MRI alone is not a panacea as MRI findings are not specific for DCM: visualized compression on MRI is a diagnostic hallmark, but more commonly incidental and in the setting of no symptoms; therefore diagnosis requires a combination of correlating symptoms, examination findings, and imaging features. However most non-specialists rely on qualitative reports of MRI, and the subjective language including “touching” or “indenting” the spinal cord can be falsely reassuring. 52 Improved access to MRI will therefore need to be complimented by education or a standardized reporting style (52).
Why Must Awareness Improve?
Optimizing the timing of surgical treatment is fundamental to maximizing its benefits. Surgery to remove spinal cord compression is the mainstay of present treatment. While typically patients sustain some improvement, the recovery, however, is rarely complete as the spinal cord has a limited intrinsic capacity for recovery and residual disability is considered to reflect irreversible damage. 1 Secondary analysis of trial data evaluating surgical intervention for DCM has demonstrated that time to treatment, specifically within 4–6 months of symptom onset, is an important positive predictor for greater recovery. 6 However, this starkly contrasts the frequent delays experienced in practice and highlights the significance of achieving early diagnosis.7,16
To complicate matters further the natural history of DCM is poorly understood, with a large proportion of spinal cord compression initially asymptomatic or minimally symptomatic. 53 Identifying which individuals are at high risk for the development of DCM or progression would allow a personalized medicine approach to early diagnosis and intervention allowing for safer application of surgery with improved outcomes.
This critical concept of optimizing the timing of surgical treatment is reflected throughout the top 10 research priorities identified during the AO Spine RECODE-DCM priority setting process; raising awareness to expedite diagnosis (Number 1), developing sensitive assessment tools to identify progression (Number 2), understand the natural history (Number 3), and individualizing surgical care (Number 10). These knowledge gaps illustrate that in order to improve outcomes, awareness must improve not just to increase early diagnosis, but more broadly: It is clear that a multi-disciplinary approach to managing DCM represents an optimal approach, 54 and this extends throughout the lifetime of someone with DCM. Awareness therefore needs to permeate DCM care specialties, but also more broadly, to entice both research funding and clinical researchers into this field.
Raising awareness can be considered fundamental to improving outcomes in DCM.
What Could Success Look Like? Perspectives From Other Diseases’
The management and outcomes of acute myocardial Infarction (MI) and cerebrovascular accident (CVA) have dramatically changed over the last 50 years.55-57 In the 1950s, care was supportive, often simply managed at home, whereas today many individuals will be left without disability or recurrent episodes. 58
Success has resulted from a comprehensive and multi-faceted approach, advancing both understanding but also awareness. Key milestones for care include the concentration of care into specialist units (e.g., Coronary Care or Stroke Units), 59 development of clear referral pathways, including triage or screening tools (e.g., FAST—Facial Droop, Arm Weakness, Speech Difficulty, Time to call an ambulance—for CVA),60,61 advances in and access to diagnostic tools (e.g., CT Head 62 or Cardiac Enzymes 63 ), significant professional but also general public awareness campaigns,61,64-66 and of course significant advances in treatment options beyond open heart surgery (e.g., Anti-Platelet medication and Interventional Radiology), including preventive medicine67,68 and symptomatic treatments.
Whilst these diseases may seem unrelated, particularly given their comparative acuity and risk of mortality, they hold major parallels with DCM: these are diseases of adulthood, where time to treatment is a determinant of outcome. Treatment is delivered by tertiary services, relying on non-specialists to suspect, diagnose, and initially manage patients. The implications for sub-optimal management are significant and life-altering, with all patients having some degree of life-long treatment and care requirements, and potentially recurrent disease. Furthermore, the current standards of DCM care; a common and disabling condition, treated in some cases with surgery and mostly managed by non-specialists, reflects the historical standards of care for MI and CVA.
One of the particularly interesting aspects of both MI and CVA care today, is the recognition that these conditions are syndromes, with a requirement for care to be tailored based on a range of demographic and diagnostic data. For example, for CVA, in simplistic terms, care has evolved from supportive only, to timely/reactive (e.g.,, Anti-Platelet/Interventional Radiology), to also pre-emptive detection (e.g.,, Transient Ischemic Attack emergency clinics 69 ) and preventative treatments (e.g.,, Carotid Endarterectomy and/or Anticoagulation).56,57,70 Within these treatment arms, there is a stratification of disease, to ensure that care is optimized for that individual scenario. One can foresee a similar future for DCM, although substantial evidence gaps need to be overcome.53,71
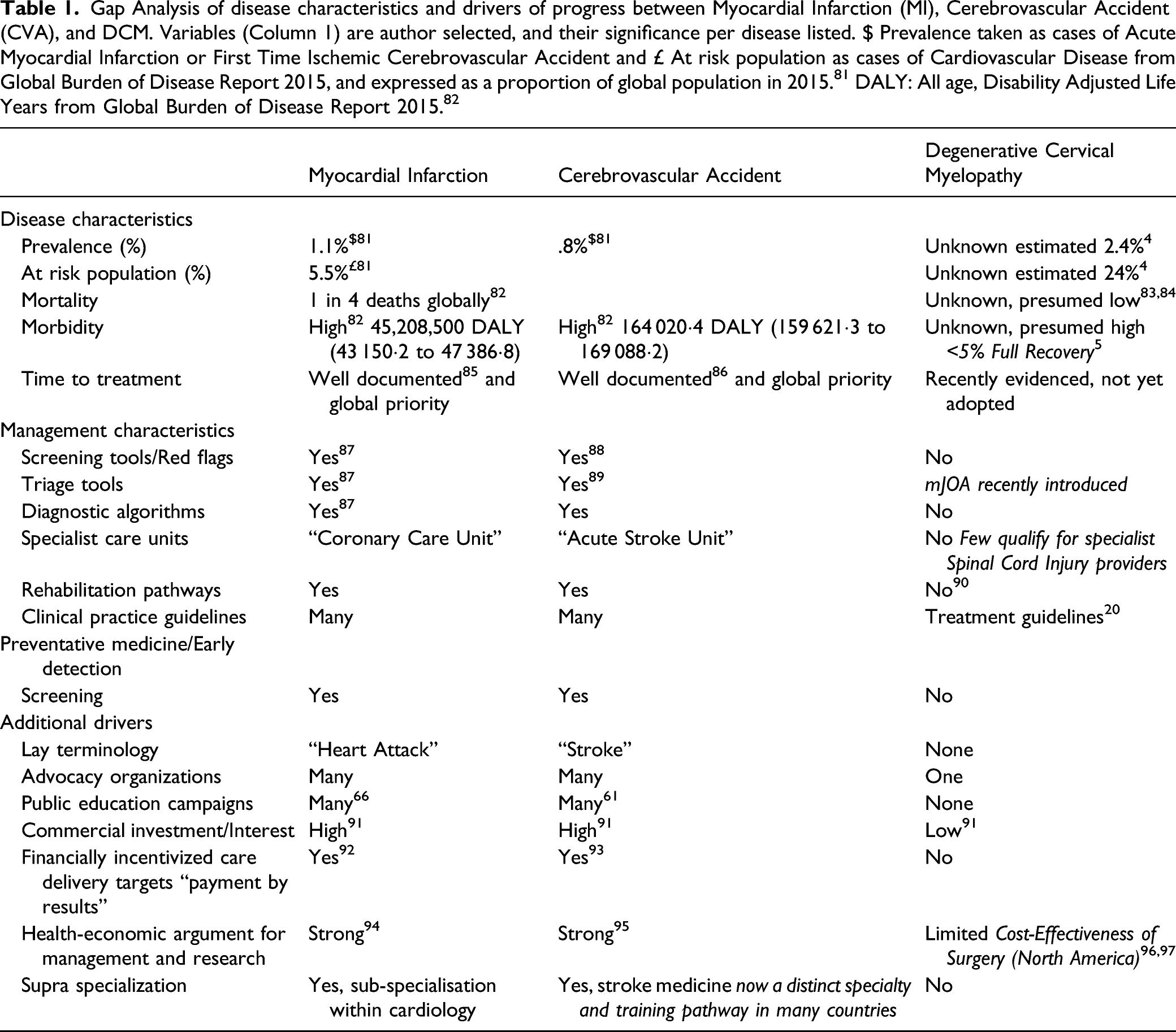
Gap Analysis of disease characteristics and drivers of progress between Myocardial Infarction (MI), Cerebrovascular Accident (CVA), and DCM. Variables (Column 1) are author selected, and their significance per disease listed. $ Prevalence taken as cases of Acute Myocardial Infarction or First Time Ischemic Cerebrovascular Accident and £ At risk population as cases of Cardiovascular Disease from Global Burden of Disease Report 2015, and expressed as a proportion of global population in 2015. 81 DALY: All age, Disability Adjusted Life Years from Global Burden of Disease Report 2015. 82
What is Being Done to Address this in DCM?
Guidelines are an essential part of changing clinical practice. 23 Guidelines for the management of DCM were developed by AO Spine in 2017, 20 these have since been endorsed and extended with recommendations by the World Federation of Neurosurgeons Spine Committee.72-76 These primarily focus on the treatment of DCM, and not the detection or long-term management. The AO Spine guidelines introduced the use of the mJOA assessment tool, recognizing that different degrees of functional impairment appear to have a different disease trajectory.20,77 Although not suitable for disease screening, this is the first example of a decision algorithm based on an assessment tool in DCM. However, the mJOA does have certain limitations and a degree of inter-rater reliability error, which should always be considered in patients who have “borderline” assessment scores. 78
In the UK, the National Institute for Health and Care Excellence (NICE) has attempted to address early detection challenges with guidance for management of common neurological symptoms. 79 The guidance has received criticism in some quarters, 80 largely based on its breadth (eg, cervical myelopathy is poorly covered) but also the inconsistency of symptom-based categorization (eg, “slowly progressive limb weakness”) and disease-based categorization (eg, Bell’s Palsy), with the latter too reliant on professional knowledge which contrasts the aforementioned concerns. It is too early to evaluate the impact of such tools, but they are an important first step.
AO Spine RECODE-DCM has additional objectives. This includes the consensus selection of the condition name and its definition. 9 This will hopefully directly support efforts to ensure consistent messaging, important for awareness. It is of note in the aforementioned success stories, both MI and CVA have ubiquitous and lay terms; “heart attack” and “stroke”. This may be of significance for public awareness. However additionally, the priorities identified here also target key knowledge gaps to support awareness.
Myelopathy.org, a charity for DCM, was formed in 2017. It is the first, and so far, only charity specifically for DCM. Whilst there are many spinal cord injury charities, the majority have a focused remit on acute, traumatic injury and have considered DCM outside of this. Myelopathy.org, with a growing community of people living with DCM and also professionals, will hopefully serve as a focal point to advocate effectively for DCM.
Conclusions
DCM is a common and progressively disabling condition, for which awareness by the public, professionals, and funding agencies is low. Improving awareness could significantly improve outcomes, by ensuring timely diagnosis and treatment and minimizing chronic neurological disability. This was determined to be the number one research priority identified by AO Spine RECODE-DCM initiative. Further enhanced research and awareness of DCM is an urgent public health priority and a call to action is required!
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research priorities were organized and funded by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international Spinal Cord Injury experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department. MRNK is supported by the National Institute for Health Research (NIHR) Brain Injury MedTech Co-operative based at Cambridge University Hospitals NHS Foundation Trust and University of Cambridge, and BMD an NIHR Clinical Doctoral Research Fellowship. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, or the Department of Health and Social Care.