
Abstract
Study Design
Retrospective cohort study.
Objective
Investigate the patterns of fused lumbar alignment in patients requiring revision surgery for proximal junctional kyphosis (PJK).
Methods
Fifty patients (67.8 yo, 76% female) with existing thoraco-lumbar fusion (T10/12 to pelvis) and indicated for surgical correction for PJK were included. To investigate patterns of radiographic alignment prior to PJK revision, unsupervised 2-step cluster analysis was run on parameters describing the fused lumbar spine (PI-LL) to identify natural independent groups within the cohort. Clusters were compared in terms of demographics, pre-operative alignment, surgical parameters, and post-operative alignment. Associations between pre- and post-revision PJK angles were investigated using a Pearson correlation analysis.
Results
Analysis identified 2 distinct patterns: Under-corrected (UC, n = 12, 32%) vs over-corrected (OC, n = 34, 68%) with a silhouette of .5. The comparison demonstrated similar pelvic incidence (PI) and PJK angle but significantly greater deformity for the UC vs OC group in terms of PI-LL, PI-LL offset, pelvic tilt, and sagittal vertebral axis. The surgical strategy for PJK correction did not differ between the 2 groups in terms of approach, American Society of Anesthesiologists grade, decompression, use of osteotomy, interbody fusion, or fusion length. The post-revision PJK angle significantly correlated with the amount of PJK correction within the OC group but not within the UC group.
Conclusions
This study identified 2 patterns of lumbar malalignment associated with severe PJK: over vs under corrected. Despite the difference in PJK etiology, both patterns underwent the same revision strategy. Future analysis should look at the effect of correcting focal deformity alone vs correcting focal deformity and underlying malalignment simultaneously on recurrent PJK rate.
Keywords
Introduction
Proximal junctional kyphosis (PJK) after adult spinal deformity (ASD) surgery is a common form of adjacent segment disease. The reported rates vary from 5% to more than 40%;1-3 PJK has a spectrum of presentation, with some patients displaying no symptoms. In contrast, others can experience catastrophic clinical sequelae such as pain, neurologic deficit, ambulatory difficulties, and social isolation. 4 Patients with PJK have a compromised focal and potentially global alignment that can result in the need for revision surgery and therefore increase the costs of ASD management, in addition to the impact on the patient. 5 The specific etiology of PJK is not completely understood, with no isolated attributable factor for all occurrences. However, agreement generally exists on the underlying multifactorial pathophysiology involved, with consensus behind a combination of surgical, radiographic, malalignment, and patient-specific risk factors playing a role.6-9
Previous studies have demonstrated an association between over-correction in the sagittal plane and PJK development following ASD correction, regardless of patient age group.10,11 Over-correction, whether planned or inadvertent, puts the body at a disadvantage in terms of reciprocal malalignment, as confirmed by studies demonstrating that the need for revision for PJK correlates with excessive lumbar lordosis and overall sagittal correction.10-12 On the other hand, under-correction can also predispose patients to adjacent segment disease. In a degenerative spine population, an association has been reported between a lack of lumbar lordosis restoration and adjacent segment disease requiring revision surgery, similar conceptually to PJK. 13 Based on the existing literature, it appears that ASD surgery can result from 2 suboptimal surgical outcomes with opposing lumbar alignment (over-correction and under-correction). Collectively, both lumbar realignment outcomes are more likely to lead to the similar radiographic presentation of PJK.
Literature investigating PJK development and associated surgical risk factors has primarily focused on the effect of different lengths of fusion, surgical techniques, and the amount of correction obtained. Limitations of these studies include reliance on a relatively early follow-up (mostly 2 years), without accounting for patients who were lost to follow up.14,15 To our knowledge, the literature is lacking with regard to studies focused on the role of different lumbar alignment patterns following ASD surgery. The primary objective of the current analysis was to investigate the patterns of preoperative alignment in patients who were ultimately revised for PJK. As a secondary outcome, we sought to explore if the surgical procedure and post-operative radiographic outcomes were different between potential patterns of alignment prior to revision. We hypothesized that such an analysis could provide valuable insight into the variability of underlying malalignment in patients who develop PJK. Recognizing different alignment presentations is beneficial when planning ASD surgery, we argue that the same applies when revising patients who develop a PJK that warrants surgical treatment.
Methods
Cohort Definition
This study was a retrospective analysis of a multicenter database of ASD patients collected between 2009 and 2018. Institutional Review Board (IRB) approval at each of the 13 participating sites was obtained prior to conducting the study (IRB No. 2014-357). Informed consent was obtained from all participating patients. After querying the database, only patients undergoing revision surgery for PJK with a posterior fusion between the pelvis and the thoracolumbar (TL) junction were included in the current analysis. Figure 1 illustrates several case examples included in the present study. Examples of cases included in the analysis. Note that all patients have complete fusion of the lumbar spine from pelvis to the thoracolumbar area.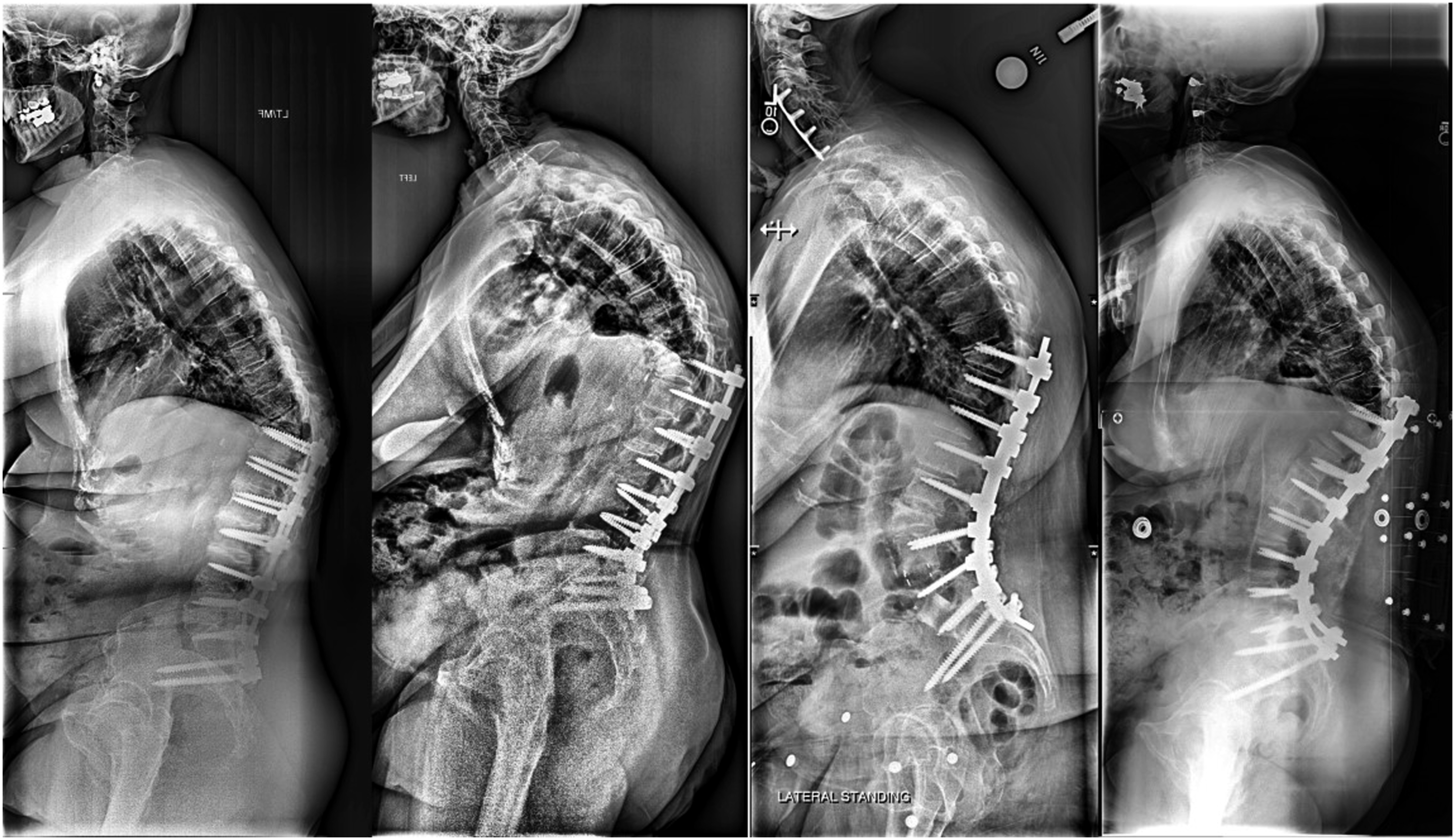
Data Collection
Demographic information collected included age, sex, and body mass index (BMI). Surgical characteristics, such as approach (anterior or posterior), American Society of Anesthesiologists score, decompression, use of osteotomy, interbody fusion, and fusion length were also recorded. Radiographic parameters of interest recorded pre- and post-revision are shown in (Figure 2). They included pelvic incidence (PI), pelvic tilt (PT), lumbar lordosis (LL), T1 pelvic angle (TPA), sagittal vertebral axis (SVA), and PI-LL mismatch (PI minus LL). Also, this study analyzed T2-T12 kyphosis (the angle between the superior endplate of T2 and the superior endplate of T12), T10-L2 kyphosis, PJK angle (Cobb angle between upper-most instrumented vertebra (UIV) and 2 levels above). Differences between current alignment values and age-adjusted alignment targets were also calculated.
16
A positive value denoted an over-correction/posterior alignment compared to the objective, while negative values denoted an under-correction/anterior alignment compared to age-adjusted objectives. Radiographic measurements were performed at a central location using a dedicated and validated software (Spineview, ENSAM laboratory of Biomechanics, Paris, France).
17
Radiographic parameters included in the current analysis.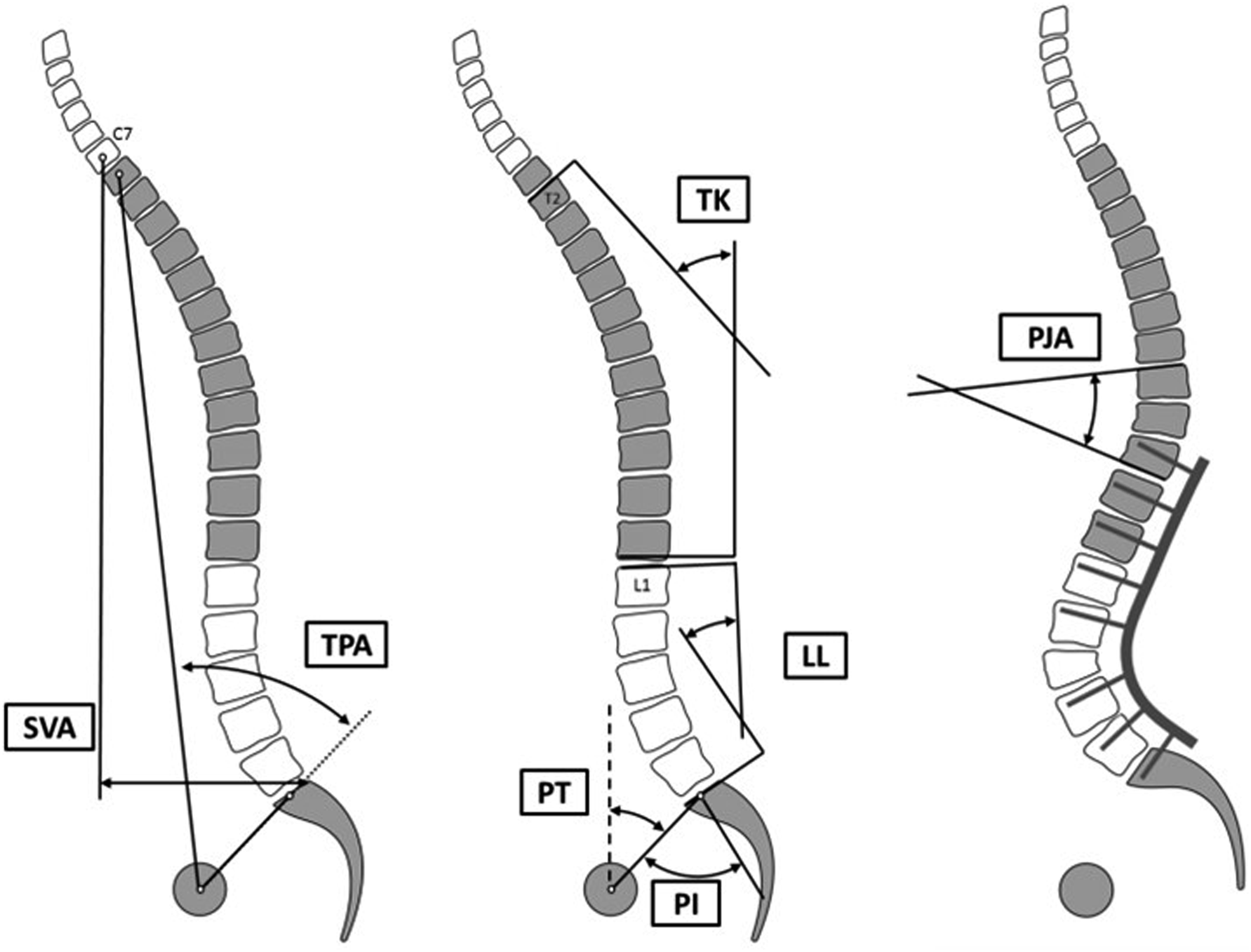
Statistical Analysis
General descriptive analysis of the entire cohort was conducted using mean values and frequencies as indicated. Patients were categorized based on pre-operative alignment of the fused lumbar spine before PJK revision using a hierarchical cluster analysis. By opposition to experience-based stratification, a hierarchical cluster is an unsupervised algorithm, a data-driven approach, with no assumption regarding the number of clusters nor the patient distribution. The endpoint is a set of clusters distinct from each other, while patients within each cluster are broadly similar to each other. The resulting groups were then compared in terms of demographic information, pre-operative alignment, surgical parameters, and postoperative alignment using the appropriate statistical test (unpaired t-test, Wilcoxon test, chi-square). Finally, associations between pre- and post-revision angles were investigated for the entire cohort as well as by type of pre-operative alignment using a Pearson correlation analysis. Statistical analysis was performed using SPSS 20.0 (IBM, Chicago, IL, USA).
Results
Cohort Description
Description of Radiographic Alignment Before PJK Revision for the Entire Cohort.
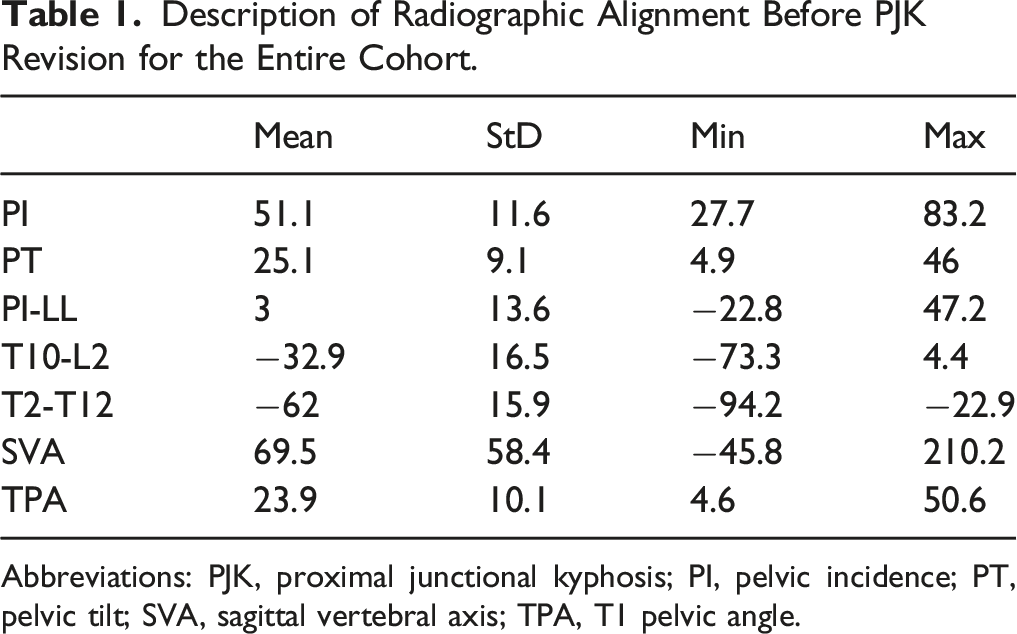
Abbreviations: PJK, proximal junctional kyphosis; PI, pelvic incidence; PT, pelvic tilt; SVA, sagittal vertebral axis; TPA, T1 pelvic angle.
Cluster Analysis
Unsupervised Cluster analysis using PI-LL value, PI-LL offset vs age-adjusted alignment goals, and PI demonstrated good results with a silhouette of .5 and identified two groups of lumbar curvature pre-revision surgery: one “over-corrected” with positive PI-LL offset form age-adjusted goals (n = 34, 68%), and one “under-corrected” with negative PI-LL offset from age-adjusted goals (n = 16, 32%). Comparison of these groups demonstrated significant difference in their PI-LL values (P < .001) (Figure 3) and their PI-LL offset from age-adjusted goals (14.0 ± 7.9 vs −9.7 ± 11.0, P <.001), but no significant difference was found in PI (50.7 ± 11.7 vs 52.4 ± 11.7, P = .626). Analysis of demographic information revealed no significant differences between “Over” and “Under” groups in term of age (Over: 67.9 ± 7.5 vs Under: 67.5 ± 8.3 P = .865), BMI (Over: 28.7 ± 5.2 vs Under: 29.9 ± 7.9 P = .590), sex (Over: 82.4% women vs Under: 62.5% women P = .125), or ASA grade. Results of the cluster analysis on PI-LL histogram. First group, associated to the left portion of the curve, had a mean PI-LL before PJK revision of −4.5° (“Over”) ranging from −22.8 to 6.9°. Second group, associated to the right portion of the curve, had a mean PI-LL before PJK revision of 18.9° (“Under”) ranging from 11.1 to 47.2°.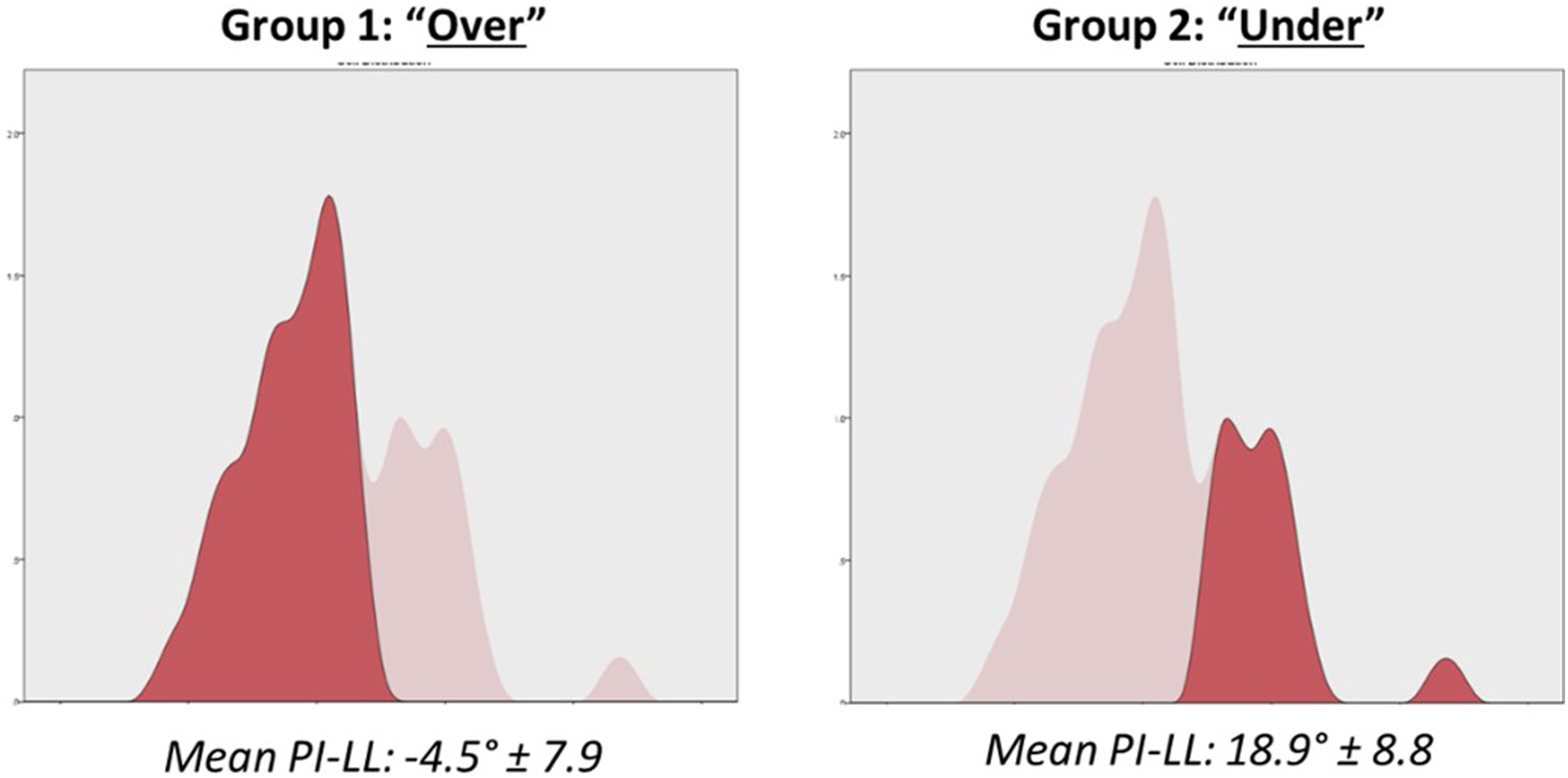
Comparison Between Cluster Groups
Comparison of Sagittal Alignment Before PJK Revision Between “Over” and “Under.”
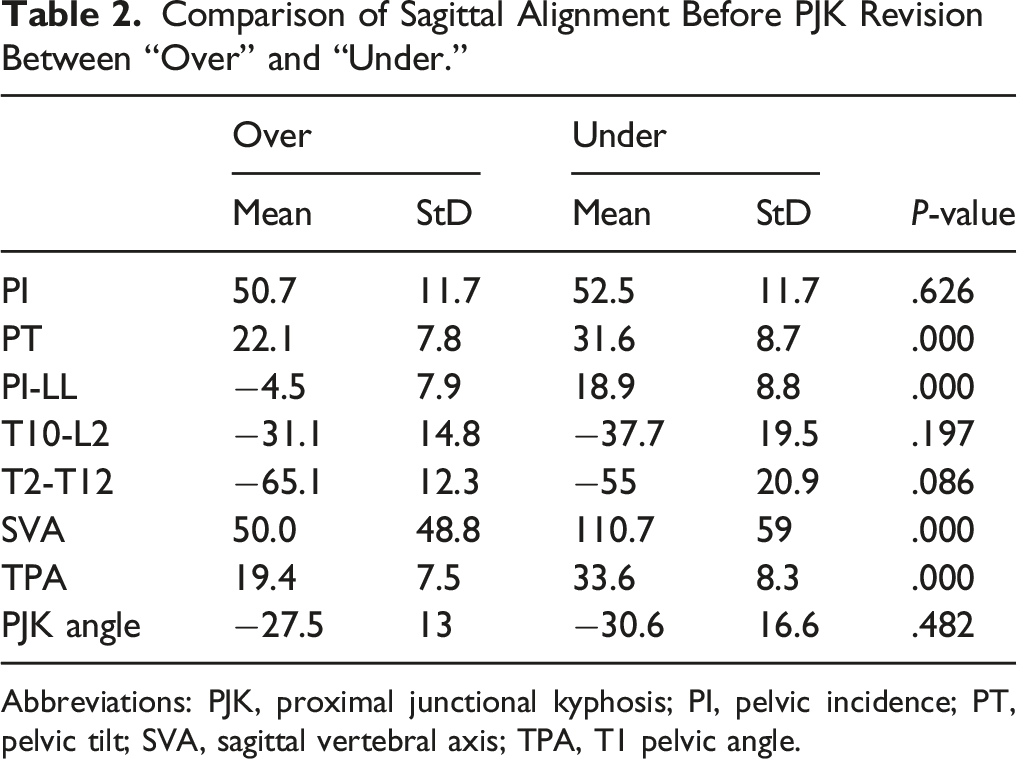
Abbreviations: PJK, proximal junctional kyphosis; PI, pelvic incidence; PT, pelvic tilt; SVA, sagittal vertebral axis; TPA, T1 pelvic angle.
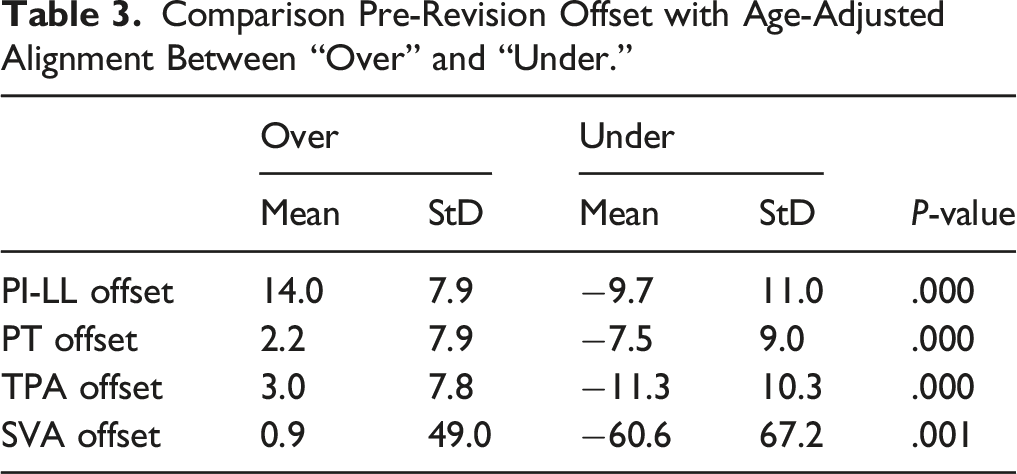
Comparison Pre-Revision Offset with Age-Adjusted Alignment Between “Over” and “Under.”
In terms of surgical information, there were no significant differences in approach, decompression, use of osteotomy, use of interbody fusion, or fusion length (all P > .05).
Comparison Post-Revision Sagittal Alignment Between “Over” and “Under.”
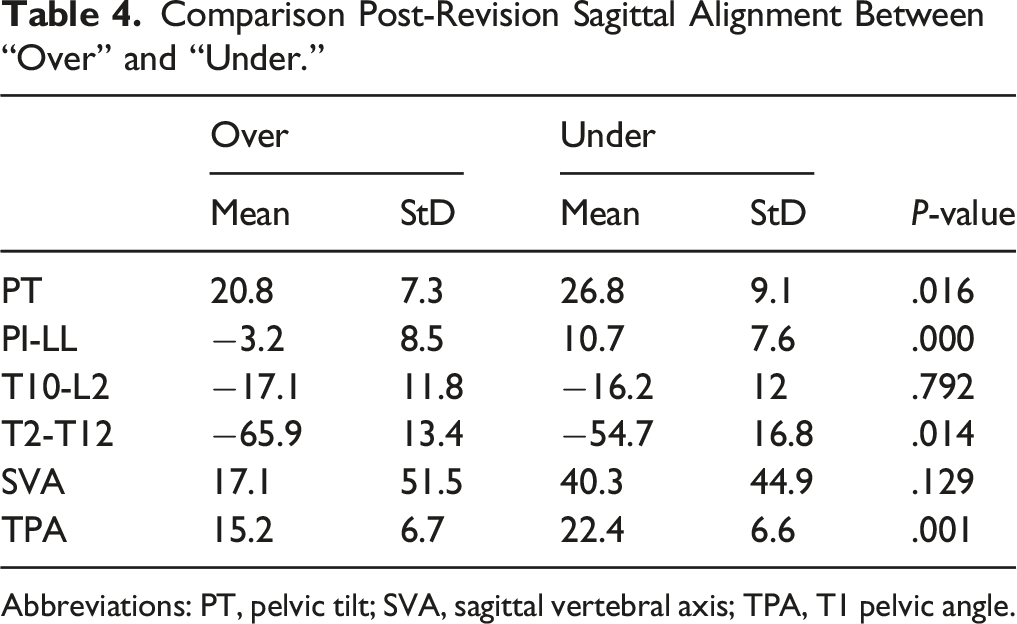
Abbreviations: PT, pelvic tilt; SVA, sagittal vertebral axis; TPA, T1 pelvic angle.
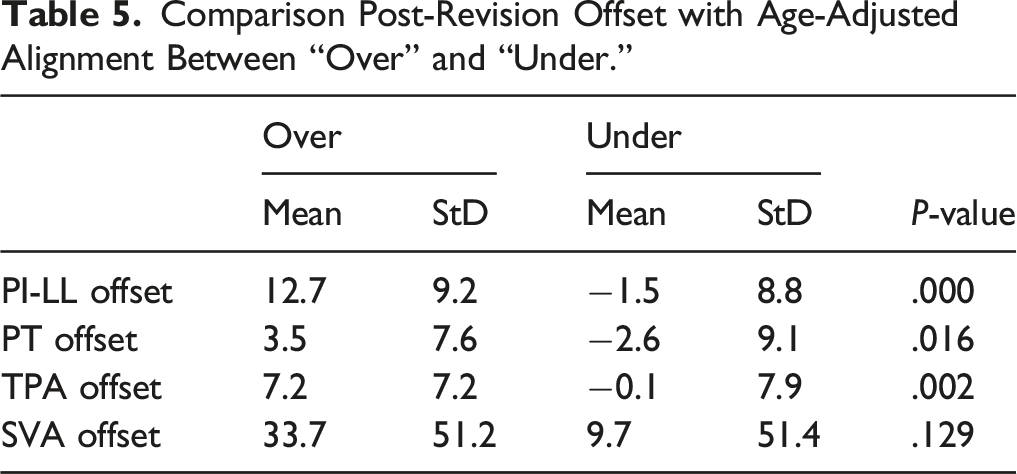
Comparison Post-Revision Offset with Age-Adjusted Alignment Between “Over” and “Under.”
PJK Angle Correction and New PJK Angle
Correlation analysis demonstrated a significant association between correction of the pre-operative PJK angle and the severity of the new PJK angle (r = −.359 P = .010). Both groups (“Over” and “Under”) underwent a similar correction of the PJK angle between pre and post (12.2° ± 12.2 vs 17.7° ± 21.1 P = .341). Similarly, both groups developed similar new junctional angle above the new UIV (−10.5° ± 10.1 vs −10.4° ± 12.1 P = .965). Correlation analysis within each group demonstrated a strong association between PJK angle correction and the new PJK angle (R = −.595 P < .001) for patients classified as “Over.” However, no significant association was found for patients classified in “Under” (P = .602). Comparison of the rate of new radiographic PJK demonstrated no significant difference between the 2 groups (41.2% vs 43.8% P = .863).
Discussion
Two patterns of lumbar alignment and shape were found to be associated with undergoing a revision for the treatment of the PJK. The first group corresponded to patients with an anterior alignment of the lumbar spine (a large PI-LL mismatch) as a result of being under-corrected with respect to their age-adjusted targets. The second group included patients with a posterior alignment of the lumbar spine (a negative PI-LL) as a result of an over-correction of the lumbar curvature compared to their age-adjusted targets. Despite the difference in lumbar curvature, both types underwent similar revision surgery with an emphasis on PJK angle correction (ie, a focal correction). Post-revision, in patients initially over-corrected, correction of the PJK without addressing the global deformity was subsequently associated with the development of a new PJK.
This study used unsupervised cluster analysis to identify the patterns of alignment within the fused segments. The main advantages of this approach compared to a classic hypothesis-based stratification are that cutoffs and group numbers are data-driven and represent the distribution within the data collection. A previous study used a similar approach to identify patterns of deformity or health care resources use.18,19 Due to the limited sample size, the cluster analysis was conducted on a limited set of parameters. With a larger dataset, future analysis may be able to investigate the shape of the fused spine with more detail (location of lordosis apex, distribution of the curvature, proximal rod bending, etc…).
In patients that were over-corrected, our hypothesis is that the creation of an excessive amount of lumbar lordosis initially led to a negative SVA, and therefore a posterior translation of the body’s center of mass (ie, gravity line). In this context, the development of PJK may be seen as a compensatory mechanism in an effort to restore a neutral global alignment (ie, truncal inclination). To achieve zero offset from their age-adjusted SVA target, over-corrected patients tended to recreate their SVA anteriorly using the unfused segments of the spine and developed a new PJK. While previously the practice of over-correction was advocated to mitigate the loss of correction in elderly patients, 20 recent findings from Lafage et al 21 showed that this approach may be harmful to elderly patients. Over-correction can be a driver of mechanical complications such as PJK.
The alignment of the under-corrected patients also lacked harmony. The failure to achieve sufficient correction left patients with an anterior alignment. As demonstrated by Elysee et al, 22 a positive SVA is associated with increased bending moments at the UIV junction. Our hypothesis is that this high mechanical loading at the junctional level led to the development of PJK. These findings are in line with those published in the degenerative population. Rothenfluh et al 13 found that patients with a residual PL-LL mismatch exhibit a 10-fold higher risk for undergoing revision surgery compared with controls in which sagittal alignment (PI-LL mismatch < 10°) was maintained after lumbar fusion surgery.
The etiology of PJK development for both over- and under-corrected groups can be explained as an opposite reaction generated to neutralize the initial force applied to the spine. 23 This is the body following the principles established by Isaac Newton’s third law. 23 Realignment goals in revision PJK surgery should be similar to the goals for primary surgery in adult spinal deformity patients. Identifying the factors that may have led to the development of PJK and optimizing them during the revision procedure are needed. Our results showed no difference in the surgical procedure between the two groups with different etiology.
Approaching revision PJK surgery as a focal mechanical failure may lead to suboptimal outcomes. A previous study by Kim and colleagues
24
looked at 32 patients treated with revision surgery after they developed PJK in the setting of a posterior fusion. The revision was successful in improving the proximal junctional angle (PJA); however, the global alignment that was present pre-revision was maintained. Patients with a pre-revision PI-LL mismatch < 11° had better post-operative outcomes than those with PI-LL >11. This supports the importance of matching PI to lumbar lordosis in terms of reducing the risk for recurrent PJK. This study is in line with our findings: addressing a PJK pathology by fixing the focal deformity only (ie, PJA) does not yield a sustainable solution. In other words, a posterior cranial extension without any change of PI-LL can “correct” the initial PJK but fails to address the root cause of the initial PJK. In this context, the outcome seems to be a new PJK as demonstrated by the linear association between PJK angle correction and post-operative new PJK angle in the current study. Planning for PJK revision surgery requires a deep analysis of the sagittal alignment by dissociating the driver of the deformity from the compensation. The ultimate goal of the body is to achieve an economical posture in terms of energy expenditure. PJK seen here is a compensatory mechanism in response to the underlying deformity. Figure 4 illustrates case examples of revision strategy in patients included in the analysis. In our series, no significant differences were found in terms of surgical information: no significant difference in approach, decompression, use of osteotomy, use of interbody fusion, or fusion length between the 2 clusters of patients. Being a retrospective study of a multicenter database, patients have been operated on by different surgeons, and variability in exact techniques used is probably present, but not statistically significant between these two groups of patients. Case examples: Patient on the left was classified in the “Over” group. This patient underwent a revision of the focal deformity above the construct without changing the lumbar alignment. Patient on the right was classified in “Under” group. This patient underwent a revision of focal deformity as well as correction of the loss of lumbar lordosis using a PSO at L4.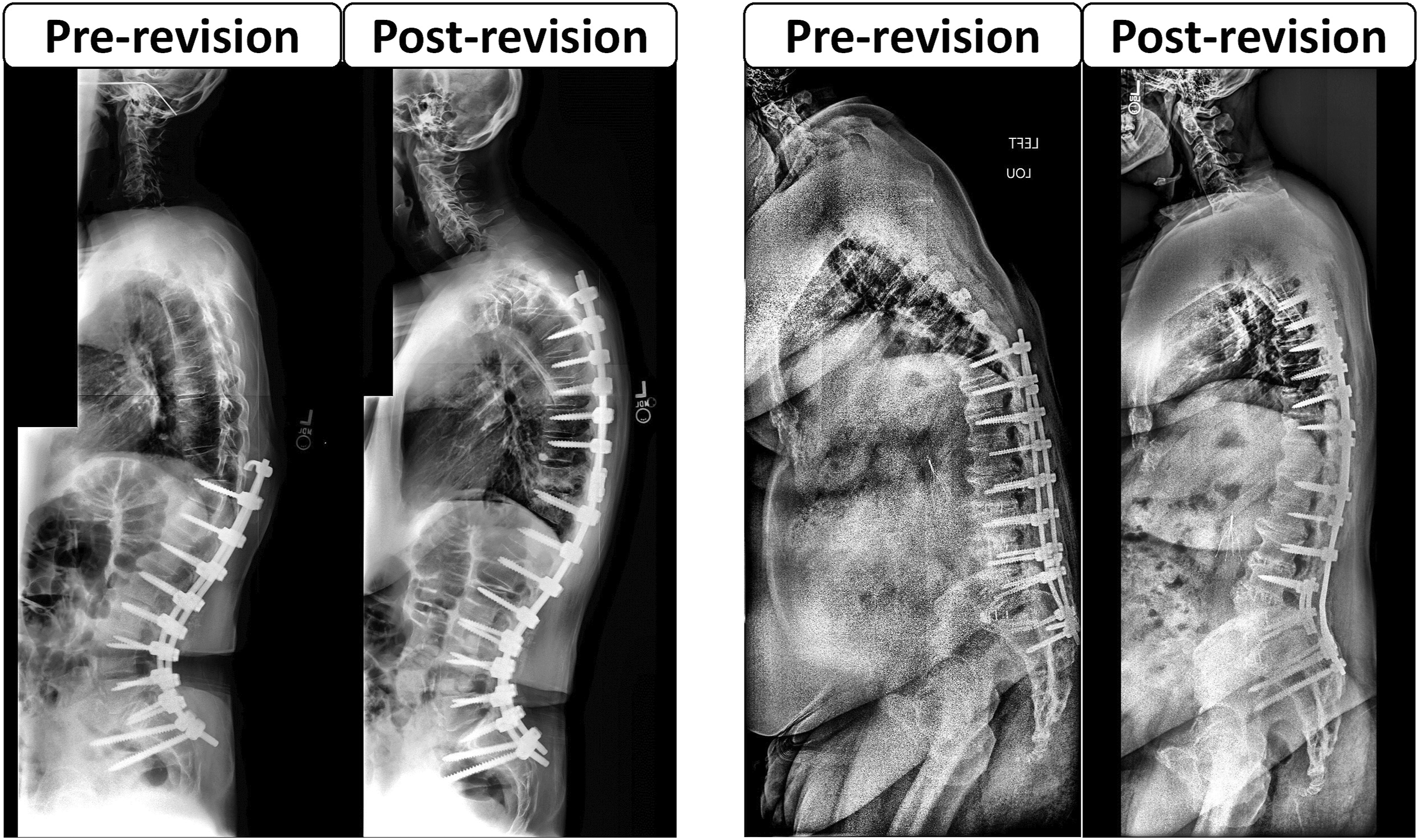
Our study has some limitations, the analysis included a relatively small cohort and which prevent a deeper investigation of pre-revision patient presentations in our clusters, including parameters commonly associated with PJK development, such as bone quality, location of correction, or rod contouring. The small cohort also limited the analysis of the optimal surgical strategy to address each of these 2 clusters of PJK patterns. However, a strong point of the study is having very strict inclusion criteria that included a single clinical presentation. In addition, this study did not have controlled planning for revision and did not account for variations in procedure due to an intraoperative event. Due to the retrospective nature of this analysis, functional outcomes were not available and could not be compared between these 2 groups of patients. Finally, a longer follow-up will be necessary to investigate the rate of recurrent PJK that required a revision, taking into consideration the type of preoperative alignment.
Conclusion
In the setting of PJK following posterior fusion surgery extended from the TL junction to the pelvis, 2 patterns of lumbar malalignment were identified: anterior and posterior malalignment. Etiology for PJK may be different based on fusion shape: PJK following over-correction may be a pathologic compensation to reach acceptable global alignment while PJF following under-correction may be due to excessive loading in an unfavorable position. Approaching PJK correction using a similar mindset as that used for correction of classic ASD, by correcting both focal deformity and the driver of malalignment, may lead to better outcomes and a lower PJK recurrence rate after revision surgery. However, a larger population and longer follow-up are needed to investigate the PJK recurrence on each of the observed groups based on surgical strategy and alignment correction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Spine Study Group (ISSG) is funded through research grants from DePuy Synthes (current), Nuvasive (current), K2M (current), Innovasis (past), Biomet (past), and individual donations.