
Abstract
Study design
Retrospective comparative study.
Objectives
The present study investigated radiographical changes in global spinal sagittal alignment (GSSA) and clinical outcomes following tumor resection using spinous process-splitting laminectomy (SPSL) approach without fixation in patients with conus medullaris (CM) or cauda equina (CE) tumor.
Methods
Forty-one patients with CM or CE tumor (19 males, 22 females, mean age at surgery of 52.9 ± 13.0 years) were included in this study. The variations of outcome variables were analyzed in various GSSA profiles using radiographic outcomes. The clinical outcomes were assessed using Japan Orthopaedic Association (JOA) score and JOA back pain evaluation questionnaire (JOABPEQ).
Results
In all cases, the various GSSA parameters (sagittal vertical axis, C2–7 lordosis, T1 slope, thoracic kyphosis, T10–L2 kyphosis, lumbar lordosis [LL; upper, middle, and lower], sacral slope, pelvic incidence, and pelvic tilt) did not significantly change in the 2-years postoperative period. Moreover, age at surgery, the number of resected laminae, preoperative T12–L2 kyphosis, or LL did not affect the postoperative changes in T12–L2 kyphosis or LL, and had no statistically significant correlation among them. The scores of each postoperative JOA domain and the Visual Analogue Scale included in the JOABPEQ were significantly improved. There was no statistical significant group difference in each sagittal profile or clinical outcomes between CM and CE groups postoperatively.
Conclusions
Tumor resection using SPSL approach did not affected the various GSSA parameters examined and resulted in satisfactory clinical outcomes, indicating that SPSL approach is a suitable surgical technique for patients with CM or CE tumor.
Keywords
Introduction
Surgical resection is the primary treatment for spinal cord tumors. In particular, as a technique of approaching tumors, laminectomy is a standard procedure for decompressing the spinal cord and directly removing tumors. Moreover, wide laminectomies are often required to open up enough space and resect the tumor safely.1-3 However, laminectomies have a risk of spinal deformities, which may cause instability and subsequent kyphosis due to damage to the posterior elements of the spinal column.4-8 In conventional laminectomy of the lumbar spine, intraoperative damage of posterior supporting structures can lead to irreversible atrophy of paraspinal muscles.7,8 Conversely, spinous process-splitting laminectomy (SPSL) helps to preserve spinal alignment by protecting posterior elements such as muscles, facet capsules, and interspinous and supraspinous ligaments.9,10 Because of these advantages, SPSL can be a useful alternative to conventional surgical decompression techniques to treat the entire lumbar spine.8-11
Recently, postoperative global spinal sagittal alignment (GSSA) has been regarded as an increasingly important subject, which may associate with clinical and functional outcomes in patients with spinal deformity or spinal cord tumor.12-17 Several reports showed that spinal deformity occurs at a rate of about 10% following surgery for spinal cord tumors (including intramedullary and extramedullary tumors) in adults.18,19 Postoperative kyphosis in the GSSA can lead to neurological deterioration, pain, and problems with posture, which may be related to the number and level of the resected laminae.15-17,20-23 However, no studies have examined radiographical changes in GSSA or the clinical outcomes after surgical resection for conus medullaris (CM) or cauda equina (CE) tumors in adults. Therefore, investigating the clinical association with these parameters is essential to identify the benefits of SPSL approach for patients with CM or CE tumors.
The purpose of this study was to examine the radiographical changes in various GSSA profiles and clinical outcomes following tumor resection using SPSL approach for patients with CM or CE tumor, and to evaluate whether any predictors were influencing postoperative GSSA.
Methods
Study Design, Patient’s Demographics, and Characteristics
A total of 41 patients (19 males (46.3%) and 22 females (53.7%) with ages at surgery ranging from 25 to 78 years (mean age 52.9 ± 13.0 years)) with intraspinal tumor at the level of CM (in which the central region of the tumor was located between T11 and L2 level) or CE (from L3 to 5) requiring surgical excision with SPSL approach at our institute between 2012 and 2018 were included in this study. The inclusion criteria were as follows: (1) diagnosed with CM or CE tumor at least at 18 years old, who did not have a facetectomy or fixation with spinal instrumentation; (2) absence of neuromuscular disorders, trauma, congenital vertebral deformity, or other pathological conditions; (3) absence of previous spine surgery; 4) clear visualization of the whole-spine on standing radiographs before surgery and at 2-years follow-up. Patients were excluded if they underwent postoperative radiotherapy/chemotherapy or had a dumbbell-shaped tumor, thoracic spinal cord tumors (in which the central region of the tumor was above the T10), and intramedullary and extradural spinal cord tumors, such as metastatic tumors. The subjects were divided into two groups, depending on the tumor location at the CM or CE level. All information on demographics (age and gender), imaging, and surgical data (estimated blood loss, time of surgery, number of resected laminae, and histopathology) were retrospectively obtained by collecting a review of the patients’ records and radiological images.
This study was approved by the Committee on Ethics and Institutional Review board (approval number: #20090042), and all subjects gave informed consent for inclusion prior to surgery.
Radiographical Data
All patients in the present study had a whole-spine radiological assessment at “preoperation” and “2-years postoperation” stages. X-ray findings involved examination of standing erect whole-spine posteroanterior and lateral radiographs. The patients stood while looking straight ahead for capturing the lateral films, feet shoulder-width apart, knees locked, and with their elbows bent and knuckles in the supraclavicular fossa bilaterally. 24
We examined various GSSA profiles as follows: sagittal vertical axis (SVA; plumb lines of C7 and the posterosuperior corner of S1), C2–7 lordosis, T1 slope, T5–12 thoracic kyphosis (TK), T10–L2 kyphosis, L1–5 lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), and sacral slope (SS). The LL was subdivided into three segments: T12–L2 upper lumbar lordosis (ULL), L2–L4 middle lumbar lordosis (MLL), and L4–S1 lower lumbar lordosis (LLL). Radiographs were measured by two authors of this study. Furthermore, they assessed the measurements independently. An experienced spine surgeon also reviewed the medical records and evident radiographs of all patients.
Clinical Outcomes and Functional Evaluation
We assessed the clinical outcomes and functional effectiveness of CM or CE tumor patients at “preoperation” and “2-years postoperation” stages using the Japanese Orthopaedic Association (JOA) scoring system (29 possible points) and the patient-reported outcomes, such as the JOA back pain evaluation questionnaire (JOABPEQ, the range of the score for each of the five domains is from 0 to 100, with higher scores indicating better condition). In addition, the degree of low back pain, pain, or numbness in the buttocks and lower limbs were assessed using the Visual Analogue Scale (VAS) included in the JOABPEQ (the range of the score is from 0 to 10, with lower scores indicating a comfortable condition without any pain or numbness).25,26 Japanese Orthopaedic Association score recovery rate was calculated as (2-years postoperative JOA score – preoperative JOA score)/(29 – preoperative JOA score) × 100 (%). Each scale was assessed by two or more orthopedic surgeons to decrease interobserver variation.
Statistical Analysis
All data are expressed as the mean ± standard error of the mean, and categorical variables were presented as percentages. Changes in various GSSA parameters were compared between “preoperation” and “2-years postoperation” stages using the Mann–Whitney test. A correlation analysis was performed using a Spearman test. A P value <0.05, <0.01, or <0.001 was considered to exhibit statistically significant difference. All statistical analyses were performed using SPSS version 26.0 (SPSS Inc., Chicago, IL).
Results
Demographics, Clinical Characteristics, and Surgical Data of All Patients.
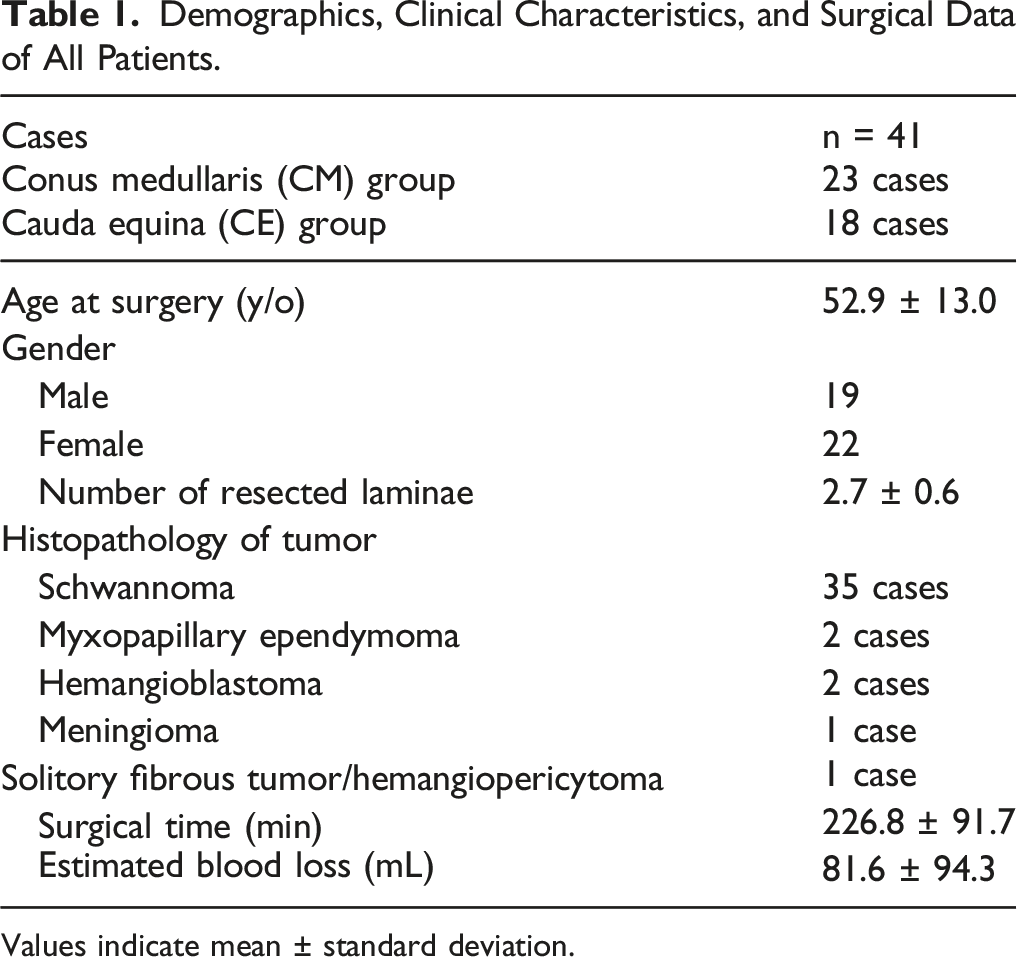
Values indicate mean ± standard deviation.
Comparison of Pre-Operative and 2-Years Follow-Up Spinal Sagittal Parameters Among All Cases.
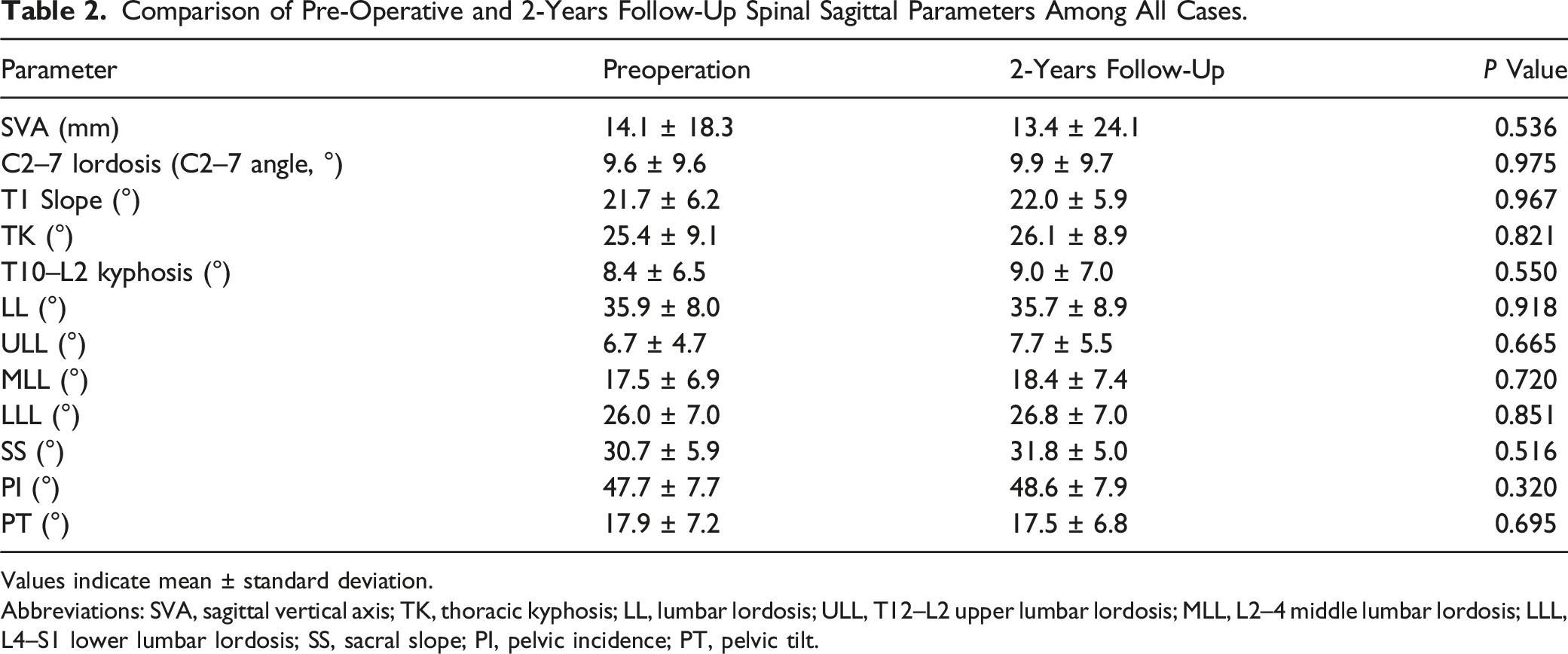
Values indicate mean ± standard deviation.
Abbreviations: SVA, sagittal vertical axis; TK, thoracic kyphosis; LL, lumbar lordosis; ULL, T12–L2 upper lumbar lordosis; MLL, L2–4 middle lumbar lordosis; LLL, L4–S1 lower lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt.
Correlation Analysis Between The Postoperative Changes For T12–L2 Kyphosis Or LL With Age, the Number Of Resected Laminae, or Preoperative T12–L2 Kyphosis or LL.
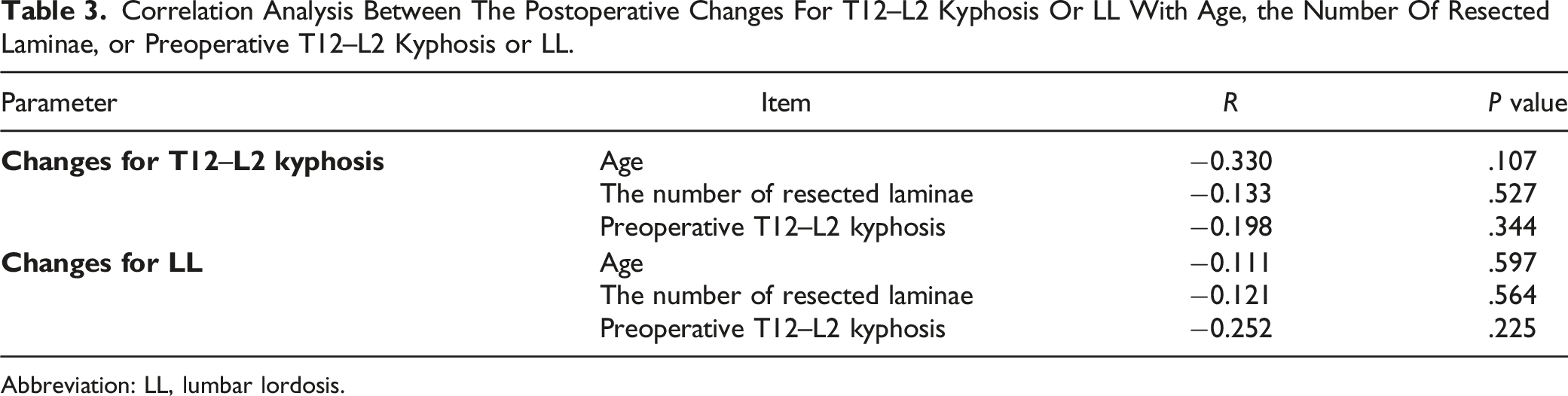
Abbreviation: LL, lumbar lordosis.
Comparison of Preoperative and 2-Years Follow-Up Clinical Outcomes Among All Cases.
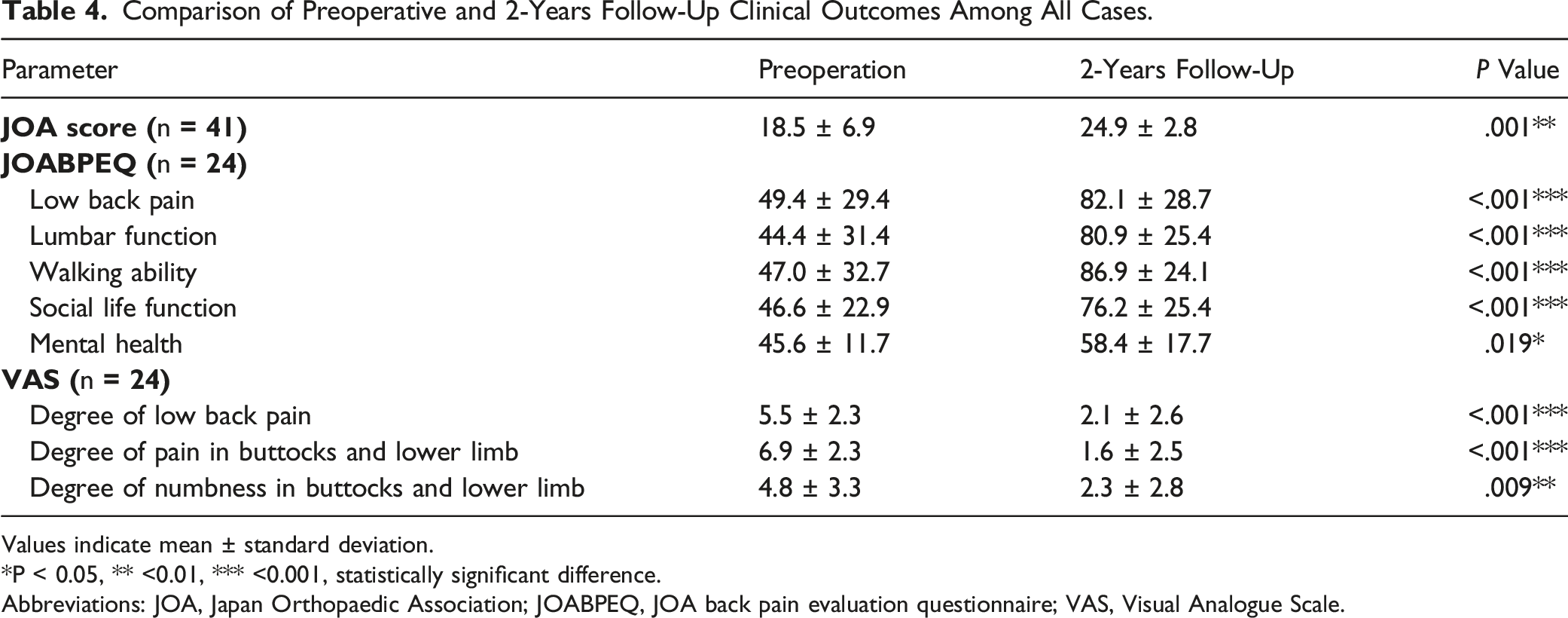
Values indicate mean ± standard deviation.
*P < 0.05, ** <0.01, *** <0.001, statistically significant difference.
Abbreviations: JOA, Japan Orthopaedic Association; JOABPEQ, JOA back pain evaluation questionnaire; VAS, Visual Analogue Scale.
Comparison of Each Sagittal Parameter Between CM and CE Groups.
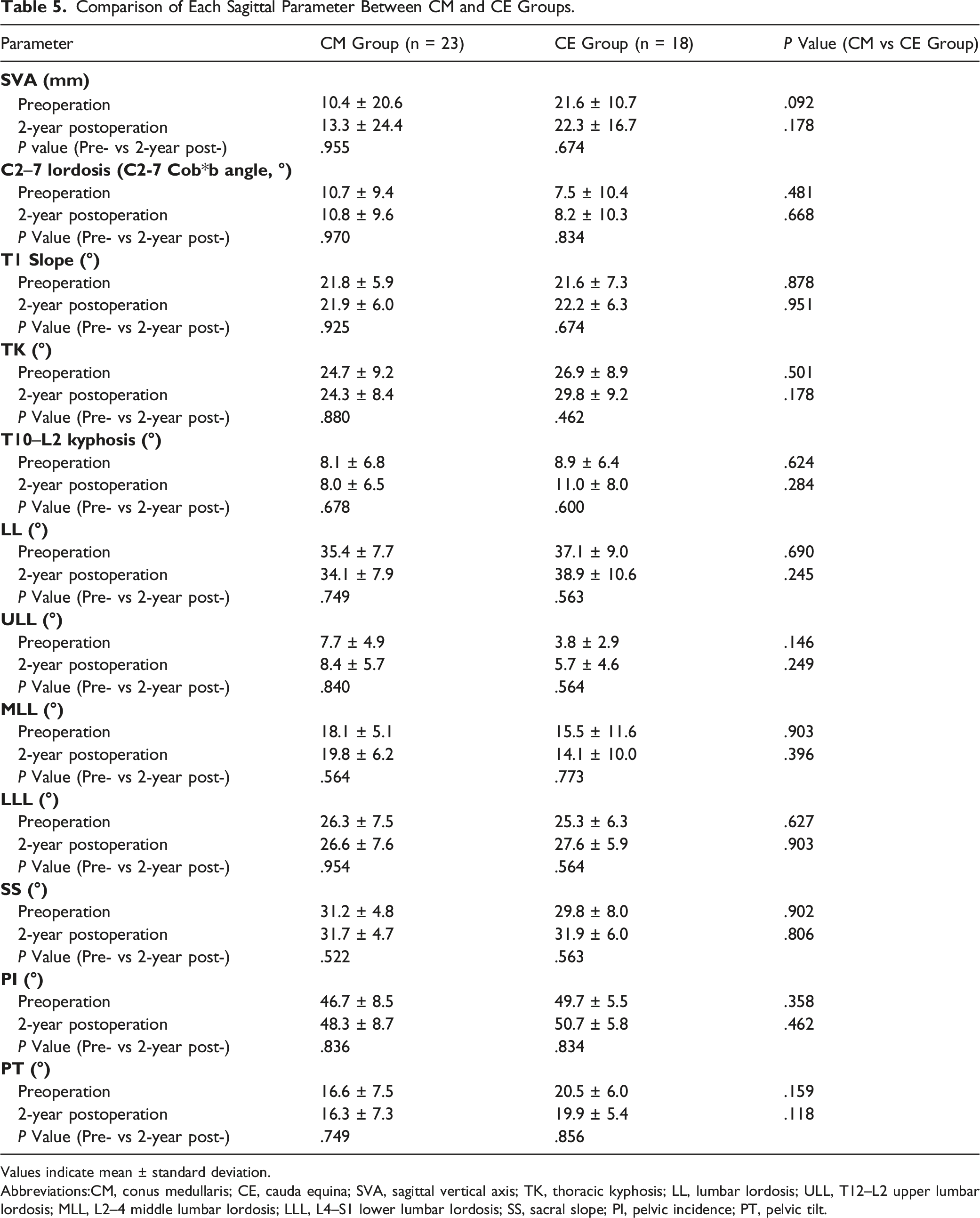
Values indicate mean ± standard deviation.
Abbreviations:CM, conus medullaris; CE, cauda equina; SVA, sagittal vertical axis; TK, thoracic kyphosis; LL, lumbar lordosis; ULL, T12–L2 upper lumbar lordosis; MLL, L2–4 middle lumbar lordosis; LLL, L4–S1 lower lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt.
Comparison of Each Clinical Outcome Between the CM and CE Groups.
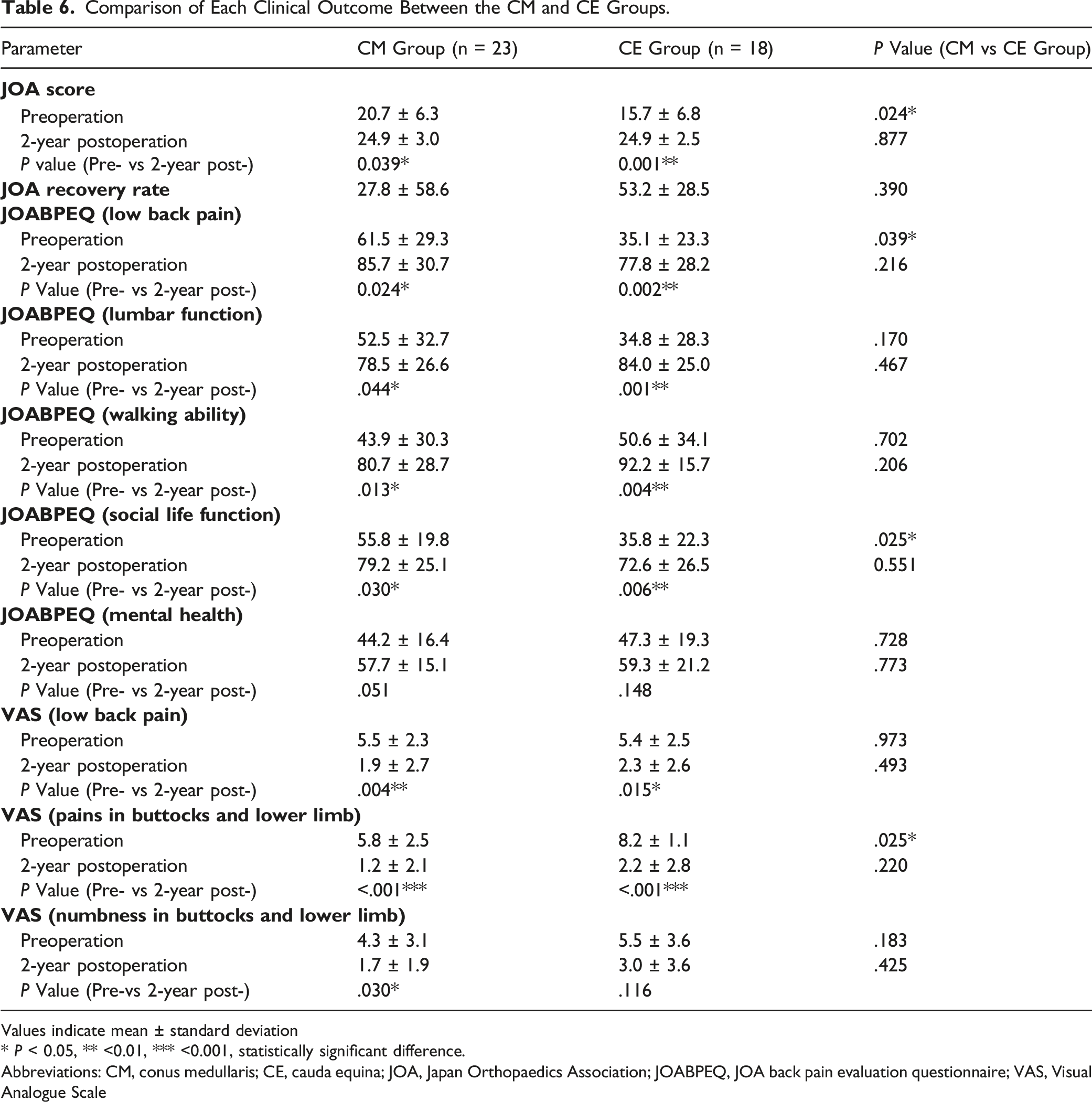
Values indicate mean ± standard deviation
* P < 0.05, ** <0.01, *** <0.001, statistically significant difference.
Abbreviations: CM, conus medullaris; CE, cauda equina; JOA, Japan Orthopaedics Association; JOABPEQ, JOA back pain evaluation questionnaire; VAS, Visual Analogue Scale
Discussion
The present study is the first to investigate how CM or CE tumor excision surgery using SPSL approach without spinal fixation affects postoperative radiographical changes in GSSA and patient-reported outcome measurements. Here, we indicated that various GSSA parameters were not influenced by tumor removal using SPSL approach, and postoperative clinical outcomes were significantly improved in CM or CE tumor patients in adults. Our findings have important implications for studies evaluating the utility of tumorectomy without fixation because only a few studies have examined the changes in postoperative GSSA in patients with CM or CE tumors.
Regarding surgical procedures for spinal cord tumors, there are two main categories: decompression with or without instrumentation. A mean follow-up period of 14 years allowed Paragelopoulous et al to show that six out of 36 patients (16.6%) had a spinal deformity, and four (11%) had spondylolisthesis after multilevel thoracolumbar or lumbar total laminectomy for removal of a benign intraspinal tumor. Moreover, there was an increased incidence of postoperative spinal deformity in patients who had more than two laminae removed or a facetectomy performed at the time of the initial operation. 23 To date, to prevent spinal deformity and instability after the excision of tumors, fusion surgery with spinal instrumentation was often required to correct postlaminectomy deformity and to stabilize the spine.27,28 Nevertheless, there were some disadvantages. First, metallic artifacts from the spinal instrumentation make it quite difficult to verify the status of the surgical site or to confirm tumor recurrence and regrowth by magnetic resonance imaging postoperatively. Second, postoperative radiotherapy is likely to be interfered by spinal instrumentation. 29 Third, using instrumentation has a possibility to cause meningitis if a cerebrospinal fluid leak occurs with wound infection. 30 Finally, the total cost of surgery and the expense of hospitalization will increase with instrumentation. 31 From these points of view, in our institution, patients with CM or CE tumor are treated with SPSL surgical technique for tumor removal without fixation whenever possible. In fact, as shown in the current study, the various GSSA profiles did not change after surgery, and good surgical results were obtained, indicating that this surgical technique is very useful and essential to improving patient outcomes.
In 2001, SPSL was developed as a new surgical procedure for lumbar laminectomy.8-11 In this new procedure, the spinous process is split longitudinally in the middle and then divided at its base from the posterior arch, leaving the bilateral paraspinal muscles attached to the lateral aspects. After successfully decompressing, each half of the split spinous process is reapproximated using a strong suture. 9 Thus, the supra- and interspinous ligaments are preserved, as is the spinous process, and damage to the paraspinal muscles is minimal. Kobayashi et al 17 compared postoperative spinal sagittal alignment changes in 32 patients with thoracic spinal cord tumors who underwent either conventional laminectomy or SPSL surgical approach, and found no significant differences between preoperative parameters and those measured at the final follow-up. In the present study, comparable postoperative results were obtained in patients with CM or CE tumor. Furthermore, comparing CM and CE groups according to tumor localization, each postoperative GSSA parameter was unchanged between the groups. Therefore, SPSL technique can be a valuable alternative to the conventional approach for CM or CE tumor resection, which suggests that fusion surgery with spinal instrumentation is not mandatory, even for patients with intraspinal tumors at the thoracolumbar or lumbar level.
Recently, several reports described that young age is one of the risk factors for spinal deformities after surgery for intraspinal tumors. Pediatric patients are suggested to be at the greatest risk for developing deformities, followed by young adults (<25 years old), who also have an elevated risk compared with that in older adults.22,23,27,28,32-34 However, in the current study, there were no postoperative local kyphotic changes of the area where the laminectomy was performed, which found no statistically significant correlation between age at surgery and postoperative sagittal alignments, such as T12–L2 kyphosis or LL. Because our study focused on adults with CM or CE tumor, only two young adult patients and no pediatric patients were included. This could explain why there was no significant correlation between age and the risk of spinal deformity at the resected site. Therefore, based on the results of this study, further research should be validated in the future, including pediatric patients, regarding whether each postoperative GSSA will be changed over long-term periods.
For dumbbell tumors, there is a substantial risk of spinal deformities due to the tumor invasion of the enlargement of the posterior arch and intervertebral foramina, as well as vertebral scalloping. In addition, during the surgical procedures, the facet joint must be occasionally sacrificed for intraspinal dumbbell tumor resection, which could be the cause of spinal malalignment after surgery.35-37 However, these reports are in patients with dumbbell tumors at the cervical or thoracic spine level. Ishikawa et al 38 showed that outcomes such as postoperative radiographic measurements and clinical evaluation were comparable in patients with dumbbell tumors at the thoracolumbar level to those at the middle thoracic level after tumor removal using laminectomy and unilateral total facetectomy without instrumented fusion. Unfortunately, because the present study excluded patients with dumbbell tumors and no reports evaluated whether spinal sagittal alignment changes after surgery in lumbar dumbbell tumors, this issue will still be controversial and will constitute the subject of future discussion.
In the current study, the neurological and patient-reported outcomes such as the postoperative JOA score, all domains of JOABPEQ, and VAS were significantly improved in patients with CM or CE tumor. Furthermore, there were no significant group differences in CM vs CE tumor groups at the 2-years postoperation. However, it remains unclear whether changes in GSSA on radiographs after tumor resection will be associated with corresponding clinical symptoms or age-related degeneration in CM or CE tumor patients over the long-term postoperative period. Unfortunately, this study was evaluated at 2-years postoperatively, and we do not have detailed data on long-term postoperative observation. Therefore, future investigations on the clinical correlations of surgical outcomes and preservation of physiologic GSSA would be helpful to validate our findings and identify the benefits of tumorectomy using SPSL approach for CM or CE tumor patients.
Our study has several important limitations that should be described. First, the present study had a retrospective design, which inevitably lowered the evidence level. Second, the sample size was relatively small, and the statistical power was not strong enough to provide conclusions about precise clinical outcomes for CM or CE tumor patients. Third, we did not have a control group, such as patients with spinal cord tumors who underwent tumor resection using a conventional laminectomy approach in this study. Finally, we assessed the standard standing erect whole-spine posteroanterior and lateral whole-spine radiographs, which are suboptimal as a measure of rotational deformity. Despite these limitations, this study presents important results concerning the absence of notable changes in various GSSA profiles in CM or CE tumor patients after tumor removal using SPSL approach over a 2-years follow-up. The major interest of this study is constituted by the unprecedented analyses focusing on the presence or absence of variations in each postoperative GSSA parameter in CM or CE tumor patients who underwent tumor resection using SPSL approach.
Conclusion
Here, we estimated the changes in various GSSA parameters and clinical outcomes after tumorectomy using SPSL approach without spinal fixation in CM or CE tumor patients. This surgical technique did not influence the individual GSSA profiles investigated and could maintain an excellent sagittal alignment with satisfactory functional and clinical outcomes during 2-years follow-up period. However, since the number of patients was relatively small in the current study, future studies with a larger sample size will be necessary to bring more precise conclusions.
Footnotes
Acknowledgments
The authors would like to thank Francois Renault-Mihara (ClearbioEditing) for the English language review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.