
Abstract
Objective
To critically analyze the evidence and efficacy of cannabis to treat surgical and nonsurgical back pain via a Systematic Review.
Methods
We conducted a systematic review to investigate the efficacy of cannabis to treat non-surgical and surgical back pain. A literature search was performed with MEDLINE and Embase databases. Only RCTs and prospective cohort studies with concurrent control were included in this study. Risk of bias and quality grading was assessed for each included study.
Results
Database searches returned 1738 non-duplicated results. An initial screening excluded 1716 results. Twenty-two full text articles were assessed for eligibility. Four articles ultimately met pre-determined eligibility and were included in the study. Two studies addressed post-SCI pain while other two studies addressed low back pain. No studies specifically examined the use of cannabis for surgical back pain. The type of cannabis varied between study and included THC, dronabinol, and Nabilone. A total of 110 patients were included in the four studies reviewed. In each study, there was a quantifiable advantage of cannabis therapy for alleviating back pain. There were no serious adverse effects reported.
Conclusions
In all articles, cannabis was shown to be effective to treat back pain with an acceptable side effect profile. However, long-term follow up is lacking. As medicinal cannabis is being used more commonly for analgesic effect and patients are “self-prescribing” cannabis for back pain, additional studies are needed for healthcare providers to confidently recommend cannabis therapy for back pain.
Study Design
Systematic review.
Background
While the understanding regarding back pain has improved, the ongoing lack of successful and lasting treatment modalities remains an overarching problem. In particular, the struggle of managing non-surgical back pain has been identified as a primary contributing factor to the current opioid epidemic, despite substantial legislative efforts to curb these trends. 1 For patients who do undergo spine surgery, management of post-operative pain is an additionally difficult challenge. As is the case with most surgeries, spine surgery can be associated with musculoskeletal tissue damage, in addition to some expected post-operative neurologic manifestations associated with disabling pain perceptions. Inadequate pain control not only causes patients substantial distress but can also significantly inhibit early and optimal post-surgical recovery. It is the current consensus that adequate pain relief measures are best achieved when applying some form of “Enhanced Recovery After Surgery” through a combination of multi-modal therapies. 2 Unfortunately, most back pain management regimens rely heavily on opioid analgesics. The long-term usage of opioids often leads to various well-documented and undesirable side-effects, the most prominent of which are drug habituation, abuse, and addiction. 3 With the rising opioid crisis in the United States and elsewhere, clinicians are hopeful to find alternative pain management modalities for both surgical and nonsurgical back pain.
The utilization of cannabis to improve back pain is steadily increasing throughout the general population. The mechanism of endocannabinoid pain modulation is independent from that of the opiate pathway, making cannabinoids a potentially attractive adjunct therapy for back pain management with the goal of actually decreasing reliance on opiate medications.
4
Cannabis acts through the endocannabinoid system, which employs two different receptors: CB1 and CB2. CB1 receptors are present on both central and peripheral neurons (Figure 1). CB2 receptors are present on immune cells. It is hypothesized that CB1 receptors modulate neurotransmitter release and pain transduction, while CB2 receptors modulate cytokine release. This cytokine release is primarily thought to modulate peripheral neuropathic processes.5,6 Delta-9-tetrahydrocannabinol (THC) is the major psychoactive component of cannabis and activates CB1 receptors in the central nervous system.
7
Animal studies have provided evidence supporting the suppression of nociceptive transmission by endocannabinoids and exogenous cannabinoids.
8
This effect is thought to occur both peripherally and centrally, specifically at the posterior horn of the spinal cord.
8
A total of 66 different cannabinoids have been isolated. In addition, several synthetic cannabinoids such as nabilone and dronabinol have been produced.
9
Of these cannabinoids, THC has been the most widely studied and is currently the most highly utilized in the population. Mechanism of action of the endocannabinoid system. Cannabinoids bind to CB1R on the presynaptic neuron blocking neurotransmitter release.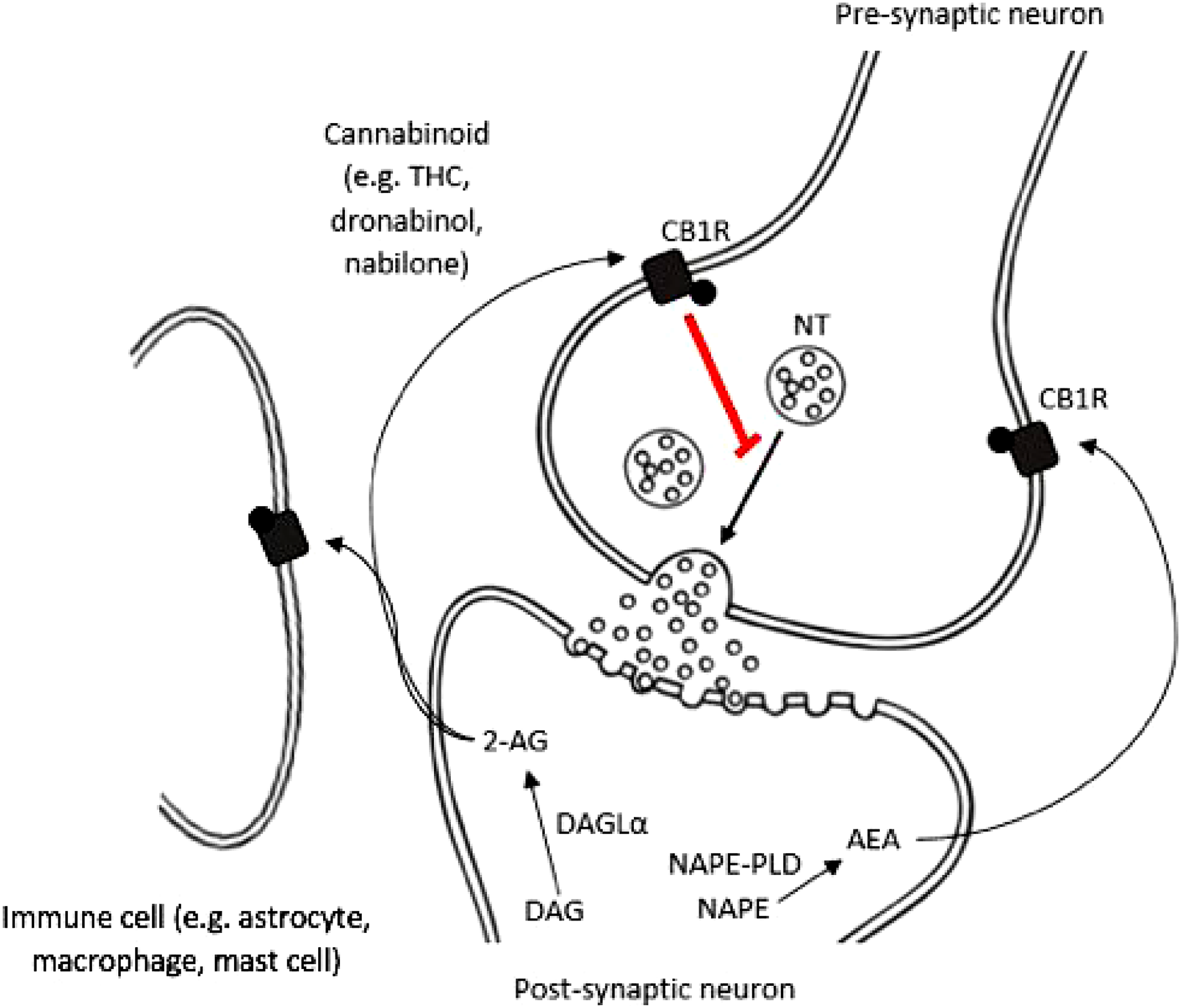
While the utilization of cannabis for analgesic therapy was first reported in 1975, the recognition of its medicinal properties was recorded as early as 400 AD. California was the first state in the United States to legalize medicinal cannabis in 1996. To date, a total of 35 states in the United States have since legalized medicinal cannabis, and a growing number of countries are following suit. The growth in widespread acceptance of medicinal cannabis by both clinicians and patients corresponds with an increasing interest to understand its analgesic properties for therapeutic utilization. 10 A recent meta-analysis showed evidence that in most randomized control trials (RCTs) there was a significant analgesic effect favoring cannabis over the placebo for non-cancer pain management, without any serious adverse events. 11 Cannabis has been further reported as efficacious in reducing pain in several disease processes including cancer, rheumatoid arthritis, multiple sclerosis, and fibromyalgia.12-14 Additionally, there is growing evidence supporting its ability to mitigate nonsurgical back pain. 15 However, there have been mixed results for post-operative pain relief from cannabinoids. 6 Given the increasing success of medicinal cannabis in alleviating pain as seen through the literature, we hypothesized that cannabis is an effective therapy for both nonsurgical back or neck pain management and post-operative pain management following spinal fusion surgery. To assess the potential for cannabis in spine-related pain management, we performed a formal Systematic Review. Our goal was to evaluate the efficacy of medical cannabis in reducing pain in patients following spine surgery, for patients suffering from chronic low back or neck pain, and patients affected by previous spinal cord injury pain (SCI-pain).
Methods
We conducted this systematic review using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 16
Identification of Studies
We searched MEDLINE (PubMed), EMBASE (Ovid), Cochrane Central Register of Controlled Trials (CENTRAL), and Cochrane Database of Systematic Reviews (CDSR) from inception to Dec 31, 2020. The search strategies are included in Supplemental Table S1 in the supplemental material. We reviewed reference lists of included studies and systematic reviews for additional articles.
Assessment of Eligibility
We established a priori criteria for study eligibility. We included studies of adults undergoing spinal surgery (acute pain), those with chronic low back or neck pain (chronic defined as ≥12 weeks), and those with chronic neuropathic pain following a spinal cord injury. Included were all concurrent comparative studies (randomized and nonrandomized) comparing medical cannabinoid use, any dose, and any administration to any non-cannabinoid treatment. We excluded case series, case reports, case-control studies, cross-sectional studies, conference proceedings, abstracts, editorials, letters, and white papers. We did not limit the search with respect to the English language.
Two review authors (RNP, JRD) independently screened titles and abstracts to identify articles for full text review. Any citation deemed appropriate for inclusion by at least one of the reviewers was retrieved. Each full-text article was independently reviewed for eligibility by the same two team members. Any disagreements were resolved by consensus. One German language study was included in this study. It was reviewed by two authors who are native German speakers.
Data Abstraction and Data Management
Two review authors extracted data from each study into a spreadsheet (Microsoft Excel). Data included the author’s last name, publication year, study design, country, sample size, population characteristics, conditions studied, length of follow-up, treatment characteristics (type of cannabinoid and comparator, dose, route of administration), pain outcome scale (primary outcome), function/quality of life (secondary outcome), results (baseline and follow-up mean scores and standard deviations if reported) and any adverse events reported.
Assessment of Methodological Risk of Bias of Individual Studies
Predefined criteria were used to assess the quality of each study. Randomized and nonrandomized trials were assessed by a team of three independent reviewers using the criteria and methods developed by the Cochrane Back Review Group.17,18 Studies were given an overall rating of “good”, “fair”, or “poor” quality. 19 Studies rated “good” were considered to have the least risk of bias and their results were generally considered valid. “Good” quality studies included clear descriptions of the participant population, study setting, interventions implemented, comparison groups, a valid method for allocating patients to each treatment group, low dropout rates, clear reporting of dropouts, appropriate means for preventing bias, and appropriate measurement of outcomes. Studies rated “fair” were susceptible to some bias, though deemed not enough to invalidate the results. These studies did not meet all the criteria for a rating of good quality, but no flaw or combination of flaws was deemed likely to cause major bias. The study may be missing information, making it difficult to assess limitations and potential problems. The “fair” quality category was broad, and studies with this rating varied in their strengths and weaknesses. The results of some “fair” quality studies were likely to be valid, while others may could have been only possibly valid. Studies rated “poor” had significant flaws that implied various types of biases which could invalidate their results. They had a serious or “fatal” flaw (or combination of flaws) in design, analysis, reporting, large amounts of missing information, discrepancies in reporting, or serious problems in the delivery of the intervention. The results of these studies were equally as likely to reflect flaws in the study design as they were to show true difference between the compared interventions.
We also assessed the overall quality of evidence using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach. 20 This approach quantifies potential limitations in five domains: risk of bias, inconsistency, imprecision, indirectness, and publication bias.
Results
Study Selection
Our search identified 2141 citations. We excluded 2121 from screening titles/abstract after applying the exclusion criteria listed above, resulting in the evaluation of 20 full texts. Four studies21-24 assessing 110 participants met our inclusion criteria (Figure 2). The studies excluded from full text review can be found in Supplemental Table S2 in the supplemental material. Preferred reporting items for systematic reviews and meta-analyses flow diagram.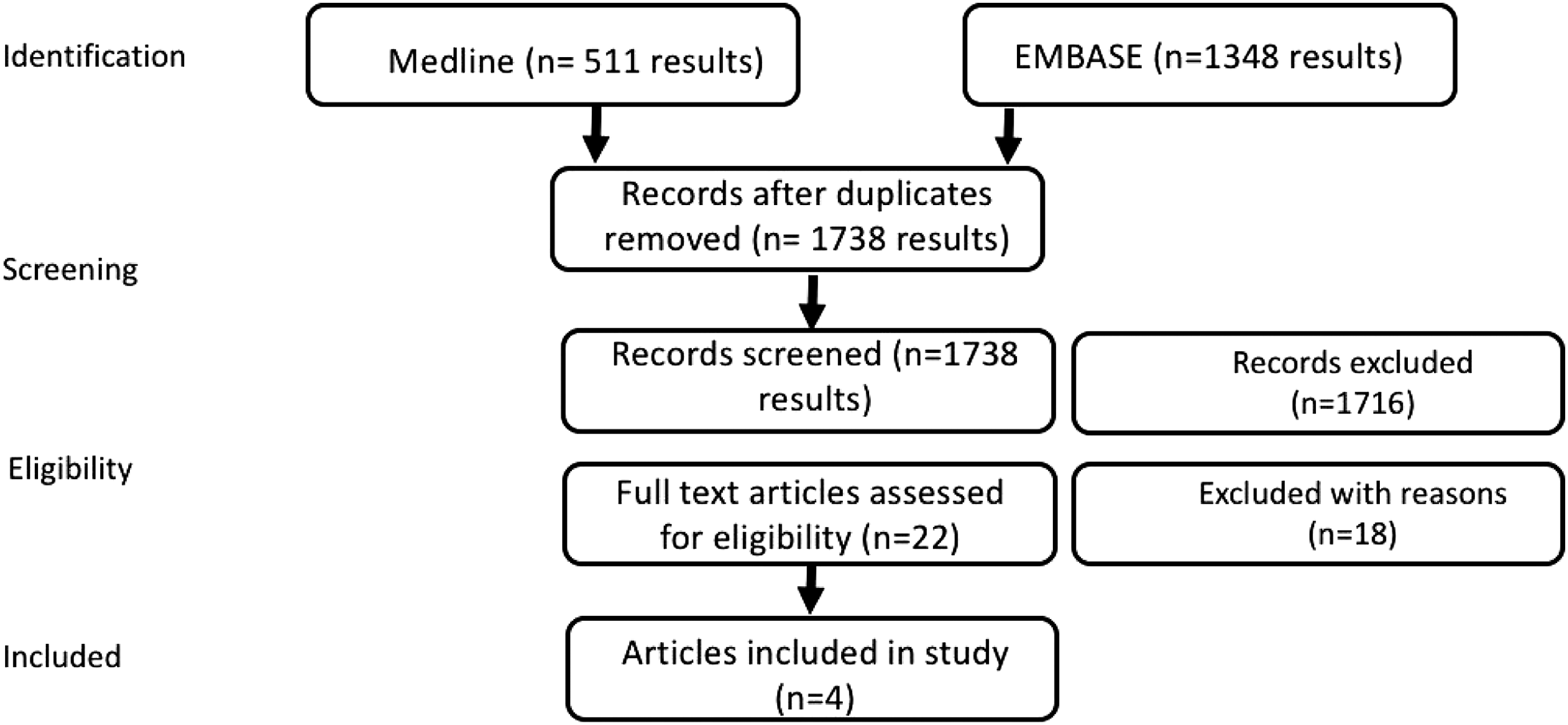
Study Characteristics
Three studies were RCTs21,23,24 and one was a prospective cohort study. 22 All were designed as cross-over studies. Three of these studies were conducted in the United States22-24 and one in Austria. 21 The average age of the participants was 45 years. Most participants were females (86%). Two studies administered the cannabinoids orally21,23 and the other two administered cannabinoids via inhalation, either smoking or vaporizing.22,24
Study Quality
One study was judged as “good” 24 and three as “fair” quality.21-23 Concerns regarding bias in the three “fair” quality studies were related to high attrition, 23 unclear randomization and treatment concealment, 21 and the observational design (Supplemental Table S3). 22
Efficacy in Assessing Pain Following Spinal Surgery
We found no studies meeting our inclusion criteria that assessed the effect of cannabis in managing pain following spinal surgery.
Efficacy in assessing pain in patients with chronic low back or neck pain
One cross-over RCT and one observational cross-over study assessed the effect of cannabis on chronic back pain. The first, a Germain-language cross-over RCT performed in Austria, investigated the efficacy in adding Nabilone to a baseline pain medication regimen for treating chronic back pain. 21 In this study, the baseline medication consisted of opioids and antirheumatic agents. A total of 30 patients participated in this trial. Participants were randomized and received either Nabilone (.25 mg) or a placebo (mannitol 270 mg). Participants were allowed to take up to four doses per day of their designated medication based on their symptom severity. The study medication was taken for four weeks followed by a five week washout period before starting the complementary study medication that was also taken for four weeks. Relevant study protocol violations were found in nine patients. Two patients changed their baseline medication and seven patients were found to have prematurely terminated their drug, leading to a 30% attrition rate. Despite the high attrition rate, there was a statistically significant decrease in reported spinal pain intensity at the end of the study in both the intent-to-treat and the per-protocol analysis. Additionally, there was a statistically non-significant decrease in the average spinal pain intensity and improvement in reported quality-of-life over the final 4 weeks of the study. The cross-over period was followed by a 16 week medication switch period with free choice, in which the number of study participants who favored nabilone was over four times higher than those who were assigned the placebo.
Study characteristics.
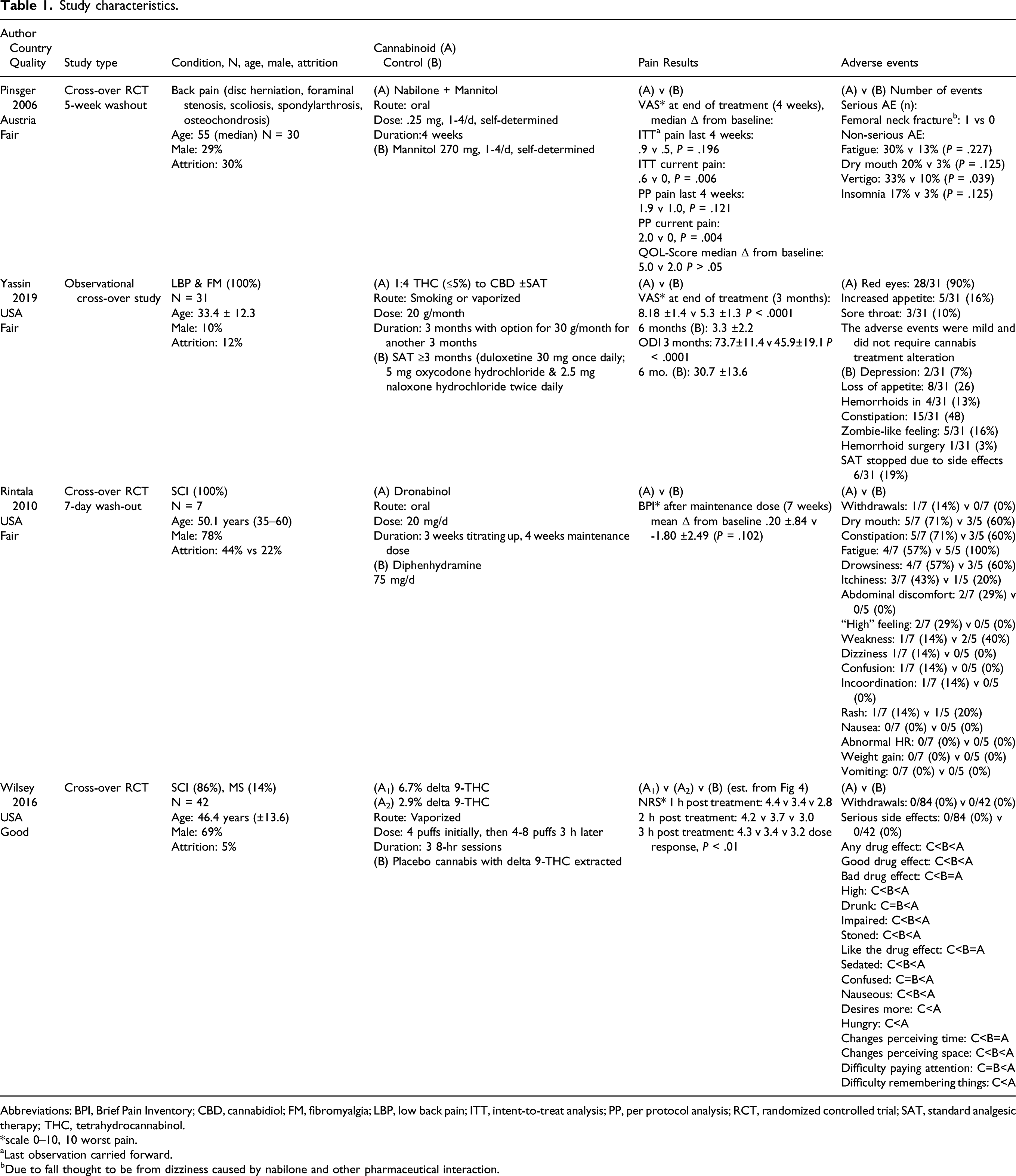
Abbreviations: BPI, Brief Pain Inventory; CBD, cannabidiol; FM, fibromyalgia; LBP, low back pain; ITT, intent-to-treat analysis; PP, per protocol analysis; RCT, randomized controlled trial; SAT, standard analgesic therapy; THC, tetrahydrocannabinol.
*scale 0–10, 10 worst pain.
aLast observation carried forward.
bDue to fall thought to be from dizziness caused by nabilone and other pharmaceutical interaction.
We rated the overall quality of evidence for the efficacy of cannabinoid treatment in those with chronic back or neck pain over short-term treatment (1-3 months) as VERY LOW (Supplemental Table S4).
Efficacy in assessing pain in patients with chronic pain post SCI
Two RCTs assessed cannabinoid usage for chronic pain caused by SCI. The first was a “fair” quality randomized, controlled, double-blind, crossover pilot study published by Rintala et al. 23 This study examined the effects of dronabinol, a synthetic derivative form of THC, on central neuropathic pain after a SCI in seven patients. Study participants were recruited by word of mouth at a Veterans Affairs Medical Center. All participants sustained a SCI at least 12 months before the study with at least six months of chronic neuropathic pain rated at least “5” on a scale of 1 to 10. There was no differentiation between transitional zone and peripheral neuropathic pain. Participants were started on either 5 mg of dronabinol or 25 mg diphenhydramine. Their doses were titrated up over 12 days to a total dose of 20 mg/day of dronabinol and 75 mg/day diphenhydramine. The titration phase was then followed by a 7 day stabilization phase to a balanced dosage based on pain relief and side effects. This was further followed by a 28 day maintenance phase of stable dosage. This was finally followed by a 9 day downward titration, and 7 day washout period prohibiting any therapeutic use before starting the other medication. Change in pain intensity using the Brief Pain Inventory (BPI) scale was the primary outcome of the study. They found no statistically significant advantage of using dronabinol compared to diphenhydramine for relieving chronic neuropathic pain related to SCI.
The second was a “good” quality crossover RCT which evaluated the efficacy of inhaled THC for managing neuropathic pain also resulting from a SCI. 24 Participants (n = 42) were recruited from a Spinal Cord Injury Clinic and were between the ages of 18 and 70 who rated their pain intensity greater than 4 out of 10. Patients were screened for bipolar disorder, schizophrenia, and major depressive disorder, as cannabis has been shown to exacerbate these conditions. Each participant was scheduled for three 8 hour experimental sessions with at least a 3 day washout period in between. Participants received either a placebo, 2.9%, or 6.7% THC per session in a random sequence. The study medication was administered via a Volcano vaporizer (Storz and Bickel America, Inc., Oakland, CA). Four 5 second puffs were administered at the first time point. Three hours later, participants could choose to inhale anywhere from four to eight puffs.
The primary outcome was pain intensity measured on an 11-point numerical rating scale (0–10). At all time-points during the 8 hour session, there was a statically significant reduction in pain in both THC groups when compared to the placebo group. There was no statistical difference between the two THC doses, suggesting the lower dose is just as effective as the higher dose. Psychoactive and other subjective side-effects were dose dependent. The number of puffs needed-to-treat to achieve a clinically significant reduction (30% or more) of pain intensity during the 8 hour period was determined to be four. Additional neuropsychological performance measurements were attempted, but were inconclusive given the range of disabilities throughout the study participants.
The overall quality of evidence for the effect of cannabinoid treatment in chronic pain following spinal cord injury was rated as LOW for its immediate effect (1–3 hours), and VERY LOW for its short-term effect (7 weeks), Supplemental Table S4.
Adverse Events
AEs were reported in all studies, and most were categorized as non-serious. With respect to cannabinoid use, one serious AE was reported: one participant sustained a femoral neck fracture following a fall thought to be due to an interaction between nabilone and a separate pharmaceutical agent. 21 One participant receiving dronabinol withdrew from their study due to self-reported unacceptable side effects. 23 No other withdrawals were noted among cannabinoid users. Other non-serious side effects varied among studies and are listed in Table 1.
Discussion
In this Systematic Review, we evaluated the efficacy of cannabis as an analgesic for surgical and non-surgical back pain. Exhaustive database searches for RCTs and cohort studies revealed only four studies that formally studied cannabis use for nonsurgical back pain. Two studies each focused on general back pain or post-SCI back pain. No studies specifically evaluated cannabis utilization for post-surgical back pain. Overall, the studies were well-performed. No studies demonstrated excessive or outright bias. A total of 110 participants were involved in the four studies. In three out of four studies, there was a statistically significant reduction in pain reported in the cannabinoid group when compared to the control group. The singular study which found no difference between cannabinoid versus control pain management included only seven patients. While there was a positive trend supporting pain improvement in the cannabinoid group, the study likely lacked significant power to prove statistical significance. Given the heterogeneity of the included studies, a meta-analysis of cannabis efficacy for treating back pain could not be performed.
Several different cannabinoids used in the studies were included in this review. Nabilone and Dronabinol are synthetic cannabinoids available via prescription. Typically prescribed for their anti-emetic properties, over the recent years they have gained wider indications for their potential ability to manage neuropathic pain. With regards to pharmaceutical delivery systems, there have been well-documented deleterious effects of inhaled cannabis preparations on the respiratory system, resulting in many experts recommending against such applications. 25 Thus, oral synthetic cannabinoids appear to be a more appealing delivery approach. There remains a debate regarding whether the inhalation delivery of whole plant cannabis produces superior analgesic effects when compared to ingesting oral synthetics. 26 In addition to these differing routes of administration, synthetic compounds may lack certain key chemicals present in whole cannabis plants which aid in its absorption and the activation of cannabinoid receptors. 27 Some studies suggest that self-titrating cannabis through inhalation may result in more potent dosages, thus optimizing pain control. To our knowledge, there have been no studies which directly compare oral versus inhaled cannabis for pain control. Establishing a deeper understanding regarding the pharmacokinetic differences between oral and inhaled forms of cannabis is necessary to provide the most accurate formal recommendations towards a preferred mode of delivery for pain control.
The duration of follow-up for these studies was also quite varied and ranged from 4 weeks in the 2006 Austrian study by Pinsger to 6 months in the study by Yassin et al from 2019, but also charted hourly changes in the study by Wilsey et al from 2016. Longer term treatment benefits or adverse side effects beyond the 6 month paradigm can therefore not be inferred, these follow up ranges, however, are very much within the typical range of pharmaceutical analgesics studies. No serious adverse events directly attributed to cannabis use were reported in the four studies analyzed in this review. While the lack of serious short-term side effects is encouraging, long-term follow-up would be necessary to document any long-term side effects of cannabis use. The longest study follow-up in the studies utilized for this Systematic Review was 6 months. Clearly longer-term follow-up of sequelae such as opiate recidivism and functional recovery would be very desirable in the context of a general overhaul of post-operative pain management. There have been some concerns raised regarding the growing utilization of cannabis throughout the population. The legal status of Cannabis varies heavily among countries around the world, and remains heavily stigmatized and sometimes actively prohibited even for medicinal use in many legal codes even beyond the actively restricted status of opiate analgesics present around the world. Some longer-term adverse side effects of more open access to cannabis may still be emerging as further experience with its wider spread use in the United States is still emerging. For instance, in Washington State, an increase in the rate of de novo spinal infections has been reported since the legalization of recreational cannabis, which may have directly or indirectly resulted in growing substance abuse. 28 Patients should be extensively counseled by care provider on the potential risk of abuse of cannabis if used to treat back pain. Cannabis use has also been associated with higher suicide rates in individuals with depression, increased risk for psychosis, and rates of other affective disorders, again increasing the onus on medical professionals to raise awareness of such undesirable side effects in general and specifically in case of medical applications. Thus, assessing possible cognitive effects of long-term cannabis use would be useful.29,30 Cannabis is not recommended for patients with mental health disorders. 31 As such, we recommend screening for mental health disorders and/or suicidal ideation before recommending cannabis for back pain management.
Back pain is understood as a multi-faceted condition and is difficult to manage. Novel therapeutic approaches are highly sought after, including a reappraisal of pharmaceuticals used, to improve the wellbeing of the affected population. Conventional wisdom which heavily relied on opiate analgesics has clearly been an unfavorable option with severe downsides. Indeed cannabis, with its alternate neurochemical transmitter pathway may provide a compelling alternative. Three out of the four studies in this Systematic Review showed significant back pain improvement in patients who utilized cannabis instead of a placebo. Interestingly, cannabis remains more heavily stigmatized than opiates in the eyes of many patients, medical providers and legislatures around the world. As the legalization of both medicinal and recreational cannabis continues expanding worldwide, the use of cannabis as an adjunct for back pain management is likely to increase as well. Coupled with an acceptable side effect profile and low addiction potential, cannabis could become a preferable alternative over other types of medications, including opiate analgesics. This is further supported by recent data which suggests cannabis use for pain management leads to decreased opiate utilization. 32 Opiates and cannabis operate through distinctly different neurochemical pathways, providing a physiologic explanation which supports the addition of cannabis as an adjunct to opiates for pain management. 33
Reducing opiate use is a strongly pursued goal in the context of the United States opioid epidemic. Overall, there is growing evidence that cannabis may be efficacious in managing back pain, however, given the current level of evidence, a conclusion recommending the routine utilization of cannabis as an alternative to opioids cannot be made at this time. We were disappointed to have found no studies that met our search criteria regarding cannabis use in post-surgical back pain. Therefore, we are not able to assess efficacy in this population. There has been no direct evaluation of the efficacy of different routes of cannabis administration or related dosing with respect to its analgesic properties. Studies that address possible combination multimodality therapies, which could include the addition of cannabis to conventional pain management regimens to decrease opiate analgesic usage, are certainly of future interest. As the legalization of cannabis continues to evolve alongside its steadily diminishing social stigma, we anticipate more studies will emerge, further advancing our understanding regarding the potential for cannabis to manage back pain.
Supplemental Material
sj-pdf-1-gsj-10.1177_21925682211065411 – Supplemental Material for The Efficacy of Cannabis in Reducing Back Pain: A Systematic Review
Supplemental Material, sj-pdf-1-gsj-10.1177_21925682211065411 for The Efficacy of Cannabis in Reducing Back Pain: A Systematic Review by Richard L. Price, Kaarina V. Charlot, Sven Frieler, Joseph R. Dettori and Rod Oskouian in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.