
Abstract
Study Design:
Case studies.
Objectives:
To demonstrate that muscle generated pain (MGP) may be a cause of pain in patients who have undergone minimally invasive spine surgery (MISS).
Methods:
A physical examination including electrical stimulation of putative pain generating muscles to identify the presence of lowered thresholds for depolarization of muscle nociceptors, and an examination of strength and flexibility of key muscles in the upper and lower body, may identify multiple etiologies of MGP. Treatment of identified muscles consisted of muscle/tendon injections to identified sensitized muscles followed by exercises incorporating relaxation limbering and stretching.
Results:
Postsurgical pain was eliminated and mobility restored in both presented cases replicating success in prior published studies.
Conclusions:
Understanding the pathophysiological mechanisms of muscle pain may facilitate the evaluation and treatment of MGP in MISS patients diagnosed with failed back surgery syndrome.
Introduction
Soft tissue pain may be related to muscle, fascia, ligaments, and tendons. Muscles will be used in this article to represent soft tissue recognizing that other soft tissue may be important pain generators as well.
Muscles represent 40% to 45% of the body by weight. They are thought to be a source of nonspecific low back pain in as many as 85% of patients with complaints of nonradiating low back pain. 1 In an ambulatory setting, 70% of patients presenting with acute low back pain were diagnosed with nonspecific low back pain, defined as sprains and strains of soft tissue. 2
Until now, the role of muscles in the etiology of common pain syndromes has been overlooked in traditional medical education. This is despite a large body of literature explaining the pathophysiology of muscle pain and the possible interventions to evaluate and treat muscles as a source of pain. 3
The landmark Quebec Workmen’s Compensation Board study, 4 looking at the disparate treatments rendered to patients presenting with back pain, found that the presentation itself did not determine the patient’s treatment, but rather the discipline that evaluated the patient. Thus, patients being seen in an interventional pain center for back pain will frequently get epidural steroid injections. The patients presenting to a surgical center will often get surgery. Even when patients present with valid indications for a spine surgery, suboptimal results may occur. Self-retaining retractors may produce muscle atrophy 5 -7 and associated decreases in force production capacity. 8 Trunk muscle strength has been found to be greater in patients undergoing MISS versus open procedures. 9 MISS emphasizes muscle sparing to improve rates of recovery and functional outcome but does not yet show convincing superior outcomes to open surgical approaches. However, no studies on spine surgery have addressed the possibility that pain produced by muscle in the low back and buttock is a possible confounding contributor to the clinical presentation of patients presenting with nonradiating back and back and leg pain. A review article on failed back surgery syndrome (FBSS) and a study on animal models of low back pain do not mention muscle or fascia as possible sources of ongoing pain. 7,8 An unpublished literature review done at Weill Cornell Medicine Comprehensive Center for Spine Care (WCM-CCSC) of 2700 papers on muscle tissue, back pain, and spine surgery found no studies of outcomes of MISS or open surgical procedures addressing muscle generated pain (MGP).
We present 2 cases of patients with persistent pain following MISS who were successfully treated by identifying and treating sensitized muscles. The case presentations are complex, reflecting the multifaceted approaches necessary to identify and treat MGP.
Case Reports and Methods
Case 1
Mr X is a 64-year-old executive, status post 2 spine surgeries for low back and leg pain. He developed low back pain in 2006 after lifting a heavy object, and a routine X-ray revealed a malignant tumor that was successfully resected, but his back pain persisted. In 2013, he had an L3-L4 and L4-L5 laminectomy/laminotomy. He had partial relief of pain, but in 2016, he developed right leg pain and foot drop, which was relieved by an L5-S1 micro-discectomy in 2016. However, he had persistent low back pain with impaired gait. He had unsuccessful trials of epidural steroid injections. He had some relief with Pilates. His pain intensity was 4/10. His medications were buprenorphine, medical marijuana, and trazodone for sleep. His Beck Depression score was 4. His Tampa Kinesiophobia scale was 48, suggesting some fear of movement that could interfere with rehabilitation.
Although a technically successful spine surgery was performed on a patient with valid indications for surgery and relief of radicular pain, there remained residual pain in his low back/buttock and leg and a diagnosis of FBSS.
In August of 2016 his physical examination revealed SLR (straight leg raise) at 65° left and 60°, and distance of 10 inches from finger tips to floor with legs straight. Tenderness was identified with the use of an electrical instrument in the following muscles: bilateral abdominal obliques, adductor magnus, iliacus, iliopsoas, quadratus lumborum, vastus intermedius, vastus lateralis, and right gluteus medius, gemellus, obturator, and piriformis.
These muscles were injected with needles of varying length, 22g × 1 1/2 - 20 g × 3 1/12 inches into the attachment sites and the muscle tissue. The purpose of the injection is to traumatize the muscle at its attachment sites and the muscle tissue itself to produce a traumatic inflammation. The injectate, 0.5% lidocaine, is used only for comfort. These injections are followed by 3 days of physical therapy, which include passive electrical contraction of the muscle and gentle limbering exercises to normalize strength and flexibility of the treated muscles and to correct the stiffness identified on his physical examination. After treatment of all the identified muscles, his pain was eliminated and his gait normalized. All these results are sustained as of phone follow-up in September of 2018.
Case 1 represents many of the patients seen in a practice specializing in the identification and treatment of MGP. A retrospective pilot study 10 of 97 patients who had failed one or more interventions for the back pain including spine surgery, epidural steroid injections, facet blocks, radiofrequency ablations, trigger point injections, and prolotherapy, were evaluated for the presence of specific sensitized muscles that could be the source of their ongoing pain. A sensitized muscle is defined as one whose nociceptors have a lowered threshold for depolarization, thereby allowing that sensitized muscle to produce pain with normal activity. Such pain would be called mechanical or muscle allodynia. Fifty-six patients who had no additional treatment and agreed to participate were evaluated by phone at an average of 77 weeks following their last treatment day. Fifty-six percent of patients continued to report >50% reductions in pain and interference in function.
Case 2
A 37-year-old lawyer and avid weightlifter developed bilateral shoulder and neck pain with radiation into the right upper arm. MRI (magnetic resonance imaging) revealed HNP (herniated nucleus pulposus) at C3-C4 and MISS was performed on May 18, 2019. His pain was unchanged postoperatively. He continued to have bilateral shoulder pain, right greater than left, and was evaluated for the possibility of muscle related pain on June 1, 2019, after he reported that his pain was worsening and interfering with sleep. He acknowledged that as an avid weightlifter he never warmed up or stretched prior to a workout. He had intermittent aches and pains that did not interfere with functioning. His disabling pain had begun in 2017 in his neck and interscapular region. MRI and neurological evaluations were unrevealing of any evidence of nerve root compression. His pain increased over time and did not respond to physical therapy and trigger point injections, and in 2019, a C3-C4 disc was found on MRI. Two surgeons had suggested a fusion and one a foraminotomy, which the patient chose. The MISS did not relieve his pain. Botox injections were done postoperatively and were ineffective. He was told that he needed 1 year of injections to achieve adequate results. A facet block produced 50% reduction in pain that lasted 1 week and a subsequent radiofrequency ablation was ineffective. He was referred for the possibility of MGP as a source of his persistent complaints. He was distraught over his persistent pain. Although he continued to work full-time as an attorney, his score on the Brief Pain Inventory was high with 8/10 in pain severity and 7/10 in interference in activities of daily living and a Tampa Kinesiophobia scale of 42.
Physical Examination
There was a 7-inch deficit in internal rotation of the right shoulder versus the left. Examination of the cervical spine revealed diminished range of motion with full flexion and extension but with lateral bending 15° bilaterally with pain and rotation 60° to the left and 70° to the right. Examination of the musculature with the aid of an electrical instrument producing a stimulus so small it is undetectable to a normal nonsensitized muscle (see below), revealed tenderness in the following muscles: bilaterally deltoids, latissimus dorsi, longissimus, posterior cervicals, rhomboids, scalenes, serratus anterior, subscapularis, suboccipitals, supraspinatus, teres minor, trapezius, and in the left triceps, teres major, and in the right infraspinatus, and pectoralis minor.
Because of the diffuse tenderness in his upper body and his dysphoria, it was suspected that he had central sensitization (CS). We routinely treat CS with low-dose naltrexone to block toll like receptor 4 on microglia, which are implicated in CS mediated pain 11 and suppress secretion of interleukins 1 and 6 thought to be causing dysphoria and hyperalgesia. 12,13 His dose was titrated to 0.9 mg/day and he was also placed on sertraline 50 mg HS for anxiety. He reported diminished generalized upper body discomfort and improved mood. The following muscles were then injected with the same protocol as in Case 1: bilateral levator scapulae, posterior cervicals, serratus anterior, and right omohyoid with total relief of his pain and normalization of range of motion in his cervical spine now 6 weeks following his last treatment.
If putative muscle pain generators could be successfully treated postsurgery might they also be present and treatable presurgically? Kaiser Permanente’s (KP) rate of spine surgery for patients with low back pain is among the lowest in the United States. A pilot study was done at KP in San Diego in the Department of Orthopedic Spine Surgery on patients with long-standing back and leg pain who were scheduled for spine surgery and reported in the same paper noted above for post failed treatment back pain patients. 10 Patients were told that it was possible that their pain was related to muscles that were not identified as part of their evaluation, and if so, treatment might avoid the scheduled surgery. Eleven patients volunteered. Seven were found to have sensitized muscles, and 4 of the 7 completed treatments as described above and cancelled their surgery. One patient was lost to follow-up. Three patients were still improved at 77 weeks and did not undergo surgery.
Understanding the pathophysiological mechanisms of muscle- and fascia-generated pain would facilitate the exploration of their role in patients presenting as possible candidates for spine surgery.
Neuroanatomy and Neurophysiology of Muscle Pain 14
Muscles contain high threshold mechanoreceptors and chemoreceptors (nociceptors) that are located close to arterioles in the muscle tissue and respond to potential or actual tissue damage. They are identified as group 3 (analogous to A delta cutaneous fibers) and group 4 (analogous to C cutaneous fibers) neurons. The high threshold allows the individual to only feel pain appropriately where there is a threat of tissue damage, for example, attempting to lift an object beyond one’s capacity, or after a tissue damaging event has occurred. Stimulation of the nociceptors causing pain is the signal to stop the activity consciously and through inhibitory mechanisms (see pain adaptation model below).
Neuropeptide Content of Nociceptors
Multiple neuropeptides are released from varicosities on muscle nociceptors’ nerve endings. Substance P (SP) and calcitonin gene related peptide (CGRP) cause vasodilation and vessel permeability resulting in localized edema. They are neuropeptides most characteristic of nociceptors. 15 Prostaglandin E2 is released from endothelial tissue, serotonin from platelets, and bradykinin is cleaved from plasma protein. These molecules stimulate respective receptors and lower the threshold to depolarize the nociceptor. This process is known as sensitization.
Brief noxious stimulation of nociceptors may only produce transient pain. Sensitized nociceptors, which are easily activated now, release, without a potentially damaging stimulus, neurovasoactive substances (SP, CGRP, histamine, bradykinin, serotonin, prostaglandins, and somatostatin) into the surrounding tissue creating an “inflammatory soup, and ongoing pain.” 16,17
Sensitization
If a noxious stimulus is transient the changes induced are reversible. Repeated subclinical or significant muscle trauma, however, can result in a sustained decrease in the threshold to depolarize a nociceptor (peripheral sensitization), and almost immediately by sensitization of dorsal horn neurons (central sensitization) resulting in consistent pain to normal use of a muscle. This means that the mere contraction of a muscle in the course of simple movements may be sufficient to initiate an impulse from the nociceptor that can be perceived in the brain as pain. Therefore, what should be an otherwise painless movement of the muscle is perceived as painful and may be termed mechanical or muscle allodynia. This process may go on for an indefinite period of time resulting in chronic pain in a region of the body such as the low back. Central sensitization is associated with spread of pain to adjacent and distal tissue through opening of previously ineffective pathways in the central nervous system. 18
Pain Adaptation Model
Muscles producing pain will be inhibited from maximum voluntary contraction and their antagonist(s) will have enhanced motor activity, which may result in spasm in the antagonist and problems in coordinated movement patterns. 18 Therefore, finding a muscle in pain and spasm may be misleading since it may represent dysfunction in the antagonist.
Chronic Pain and Effects on Coordinated Patterns of Muscle Activity
Persistent muscle pain and alterations in contractile forces in agonists and antagonists can produce uncoordinated muscle activity and may lead to additional overt and subclinical soft issue injury. Experimental and clinical muscle pain influences muscle activity during gait. Increased muscle activity was found in phases where there is normally no activity and no or decreased activity was recorded in movement phases where pain-free subjects had strong activity. 19 Induced pain in low back muscles reduces activity in abdominal muscles possibly impairing spinal stability. 20
Muscle Generated Pain and Neurogenic Inflammation (NI)
A strong noxious stimulus producing an action potential in a muscle nociceptor is transmitted in an anterograde fashion to dorsal horn neurons and ultimately to the cerebral cortex where it may be perceived as pain. The origin of the stimulus in this case would be in MGP (see Figure 1).
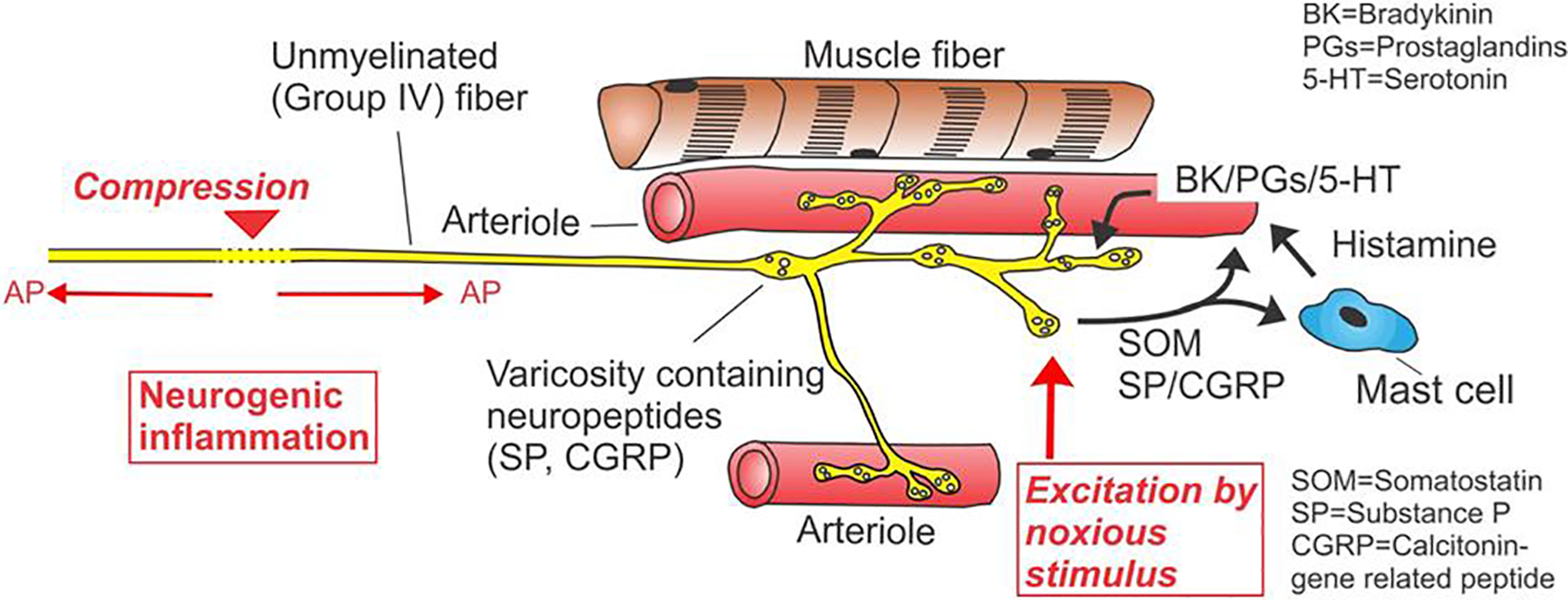
Schematic of group 4 muscle nociceptor. Neurogenic and Myogenic Pain. Structure of a muscle nociceptor and events occurring around the receptor during noxious stimulation. The nociceptor has several branches close to arterioles. The noxious stimulus (filled upward arrow) excites the nociceptor, leading to the release of neuropeptides from the ending, such as substance P (SP), calcitonin gene-related peptide (CGRP), and somatostatin (SOM). SP and CGRP cause vasodilation and increased capillary permeability in the small blood vessels in the vicinity of the ending. SP also degranulates mast cells; the released histamine is likewise a vasodilator. The release of neuropeptides from nociceptive endings can also occur when action potentials invade the ending retrogradely (against the normal direction of propagation) in neuropathy or radiculopathy (left part of figure). At the site of a nerve compression, action potentials originate in the nociceptive fiber and propagate both anterogradely (to the CNS, causing pain) and retrogradely (to the receptive ending, causing neurogenic inflammation through the release of neuropeptides). The neurogenic inflammation is a sterile inflammation around the nociceptive ending due to an increase in blood vessel permeability followed by plasma extravasation. The plasma extravasation leads to the formation of bradykinin and other agents that sensitize the nociceptor. The result of a neurogenic inflammation is a local edema with sensitized nociceptors (modified after Mense and Gerwin 21 ).
The stimulus may also be initiated proximally in the afferent neuron. Compression of a nociceptive neuron along its course in the periphery or the dorsal root may produce an action potential. The action potential travelling back to the dorsal horn would be the source of neuropathic pain. If the action potential travels in a retrograde fashion to the muscle, it will produce NI by stimulating free nerve endings to release neuro-vasoactive substances, as they would be released with trauma to the muscle. NI may compound neuropathic pain. 13
It is difficult clinically to determine if pain in soft tissue is MGP, NI, 22,23 or other soft tissue. Schilder et al 23 demonstrated that an electrical stimulation of fascia and skin produces stinging sensations and therefore may present a diagnostic challenge to identify neuropathic (related to compression of the dorsal ramus of the spinal nerve) versus fascial back pain. The transitional mechanism of fascial excitability and its possible clinical presentation, however, are not clearly understood. 24
A clinician may typically perform range of motion in the lumbar and cervical spine, straight leg raising test, reflexes and sensory examination, muscle strength, and evidence for spasms, all done generally to establish the presence of nerve root compression or structural abnormalities related to the spine. However, specific assessment of soft tissue dysfunction as a source of spine related pain is not done.
Functional Muscle Pain
Kraus postulated 4 causes of muscle dysfunction causing pain 25 :
Deficiency or deconditioning—defined as weakness and/or stiffness of muscle and tendon from lack of use or use of a muscle in a limited range. 26
Tension—inability to relax muscle related to emotional tension causing abnormal patterns of muscle contraction (dysponesis).
Muscle spasm—involuntary contraction of a striated voluntary muscle fiber.
Altered muscle tissue—typically referred to as trigger points. 27
An easily performed test of trunk muscle strength and flexibility is the Kraus-Weber test. Palpation for increased sensitivity as determined by pain to a discrete amount of pressure is the community standard to determine trigger points (with associated findings including taut band-like muscle fibers and pain radiating to other muscles) but this construct has been challenged. 27 Muscle dysfunction may present as difficulties in performing coordinated muscle movements, interfering with activities of daily living.
Various exercises have been proposed to treat back pain but generally are predicated on non-muscular source of the pain. 28 Studies of comparative effectiveness of exercise programs have not demonstrated superiority of any but the studies are confounded by non-homogeneous patient selection. 29 Various injections with a variety of injectates are performed for trigger point pain but the validity of this approach is lacking based in part on inconsistencies in applying diagnostic criteria, injection techniques, and postinjection protocols. 26
Other approaches include use of shockwave therapy, photobiomodulation (formerly known as low-level laser treatment), and varieties of massage, all of which are not yet supported by rigorous randomized controlled trials.
Discussion
We have reviewed the pathophysiology and functional aspects of muscle-related back pain. Our case presentations demonstrated the utility of evaluation and treatment of sensitized muscles to eliminate pain in FBSS patients post-MISS. In our quest to improve outcomes for MISS, muscle and fascia are unexplored pain-generating tissue. The role of muscle in possibly causing postoperative pain is not simply the effect of sparing of soft tissue. It requires recognizing the possibility that MGP was a contributing factor presurgically as well as postsurgically and also has effects on muscle function. The absence of the study of the pathophysiology of muscle pain in medical education impairs the appreciation of the presence of MGP as an important etiology in assessing surgical candidates. The few existing approaches to evaluate and treat soft tissue pain deserve to be systematically studied to determine if inclusion of muscle assessment as a source of pain may lead to better selection criteria for patients being considered for MISS and in the treatment of those patients with persistent postoperative pain. To that end, the WCM-CCSC has included weekly sessions on the evaluation and treatment of muscle pain for Pain Medicine fellows and initiated a study to determine if identification and treatment of MGP can reduce morbidity in patients with persistent pain post-MISS. We plan to do an additional study to determine if identification and treatment of pain generating muscles can be utilized to refine our inclusion and exclusion criteria in selecting patients for spine surgery.
Conclusion
Muscle evaluation and treatment protocols should be but are not a standard part of the assessment of patients with putative spine related pain pre- and postsurgically.
Based on the pathophysiological understanding of sensitized nociceptors as the foundation for MGP, we were able to electrically identify specific muscles as the source of pain in the cases presented above. The treatment provided, namely, thoroughly injecting a sensitized muscle with particular attention to the attachments as well as the muscle tissue, is based on the pioneering work of Hans Kraus, MD. Kraus also postulated 4 basic reasons for functional muscle pain. We successfully utilized the exercise programs developed by Kraus 28 on both patients and in the patients in our study, 9 to restore normal strength and flexibility and to teach relaxation skills to deal with tension related pain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from the Carl Zeiss Meditec Group.