
Abstract
Study design
Retrospective study.
Objective
To evaluate the predictive effect of the 3 global sagittal parameters (Sagittal Vertical Axis [SVA], T1 Pelvic Angle [TPA], and relative TPA [rTPA]) in the surgical outcome of patients with adult degenerative scoliosis (ADS), then to define the optimum corrective goal based on the best of them.
Methods
117 ADS patients were included in this study and followed-up for an average of 3 years. Functional evaluation and radiographs were assessed preoperatively and postoperatively. The predictive accuracy of SVA, TPA, and relative TPA was analyzed through receiver operating characteristic (ROC) curve. The cutoff value of TPA was obtained at the maximal Youden index from ROC curve.
Results
TPA most highly correlated with postoperative oswestry disability index (ODI). The best cutoff value of TPA was set at 19.3° (area under curve =0.701). TPA >19.3° was the highest risk factor in multivariate logistic regression analysis (OR = 7.124, P = 0.022). Patients with TPA <19.3° at 3 months after operation showed a better ODI than those with TPA >19.3°. Correcting TPA less than 19.3° for patients with preoperative TPA >19.3° attributed to a better health related quality of life (HRQOL) and sagittal balance at last follow-up. The formula “Postoperative TPA = 0.923 × PI - 0.241 × postoperative LL - 0.593 × postoperative SS - 2.471 (r = 0.914, r2 = 0.836, P < .001)” described the relation between SS, LL, PI, and TPA.
Conclusion
TPA was a useful global parameter for the prediction of postoperative HRQOL for patients with ADS. Keeping TPA <19.3° could improve the postoperative HRQOL for ADS patients with preoperative TPA >19.3°, and TPA <19.3° could be an optimum correction target for patients with ADS.
Keywords
Introduction
Adult degenerative scoliosis (ADS) is a common spinal deformity faced by elderly people, 1 which leads to a decline in quality of life.2,3 As a main type of adult spinal deformity (ASD), 4 ADS occurs in patients with more than 50°years old and progressed with age. 5 The vertebral instability following osteoporosis and osteomalacia might be the initial factor for this deformity, 6 accompanied with degeneration in the intervertebral disks and facets. Patients with ADS might present with various symptoms, such as low back pain, neurologic deficits, and disability. 7 Conservative treatment is initially recommended for them, however, the therapeutic outcomes are usually dissatisfactory, and then surgical procedure is needed. For these patients, the objectives of surgery include an optimum correction of deformity; the improvement in health related quality of life (HRQOL) and the decompression of neural structures.8,9
Recently, the important role of sagittal balance in the management of adult spinal deformity has been widely recognized. There were proofs that the spinopelvic sagittal alignment, rather than coronal deformity, correlated closely with patients’ clinical outcome.10-12 Schwab et al13-15 demonstrated that sagittal vertical axis (SVA), pelvic tilt (PT), and pelvic incidence minus lumbar lordosis (PI-LL) were critical parameters for surgical plan and developed a classification of adult spinal deformity centered around these parameters to guide the correction surgery. But as SVA could be easily influenced by patient’s posture and modulated by compensatory mechanism,16,17 judging the whole sagittal balance simply based on SVA might be inaccurate and misleading. Therefore, Protopsaltis et al 18 developed the T1 pelvic angle (TPA), which accounted for both truncal inclination and pelvic retroversion, could measure the global sagittal balance and less influenced by the postures. Then a few studies reported that this new parameter could more effectively predict the surgical outcomes than classical sagittal parameters.19-21
However, there were still some deficiencies in previous studies. First, as proposed by Banno, 20 reaching TPA <20° was the proper corrective target, but as the normal value of TPA varied with PI, 22 TPA >20° could be normal in a patient with large PI, and for patients with small PI, keeping TPA <20°might not be enough. Therefore, defining the TPA-based corrective target might be related to PI. 23 Therefore, based on our previous study of the sagittal alignment in normal Chinese population 24 and Yilgor’s study, 25 we developed the conception “relative TPA” (relative TPA =actual TPA—ideal TPA, Ideal TPA = 0.407 × PI + 0.104 × Age - 16.1 [r2 = 0.328, P < .001]). As a novel parameter including PI, age and TPA, relative TPA might become important reference for corrective surgery.
Thus, the goals of this study were to evaluate the predictive effect of the 3 global sagittal parameters (SVA, TPA, and relative TPA) in the surgical outcome of patients with ADS, then to define the optimum corrective goal based on the best of them.
Materials and Methods
Study Design
This study was a single-institution retrospective study which was conducted in the light of the principles of the Declaration of Helsinki and got approved by the relevant institutional Ethics Committee with the requirement for informed consent being waived. The IRB approval number is IRB00006761-2014200.
Patients
Initially, the data of patients with ADS who underwent corrective surgery in our hospital from January 2010 to September 2016 were reviewed. Based on the following inclusion criteria, 117 patients were included to assess the effect of TPA, SVA and rTPA in postoperative evaluation. The functional status was evaluated by using Visual Analog Scale (VAS), the Oswestry Disability Index (ODI), and Japanese Orthopaedic Association (JOA) Scores.
Inclusion Criteria
Location in lumbar spine and Cobb angle >10°. The age >50 years old at the time of operation. No history of scoliosis up to adolescence, neuromuscular diseases and primary spinal surgery. Long instrument with fusion >4 vertebral levels With complete preoperative and postoperative data Had >2 years follow-up
Radiographic Measurements
All patients underwent standard standing posteroanterior and lateral whole spine X-ray before surgery, 3 months after surgery, and last follow-up. Two experienced orthopedic surgeons measured the following parameters by using the PACS system (Picture Archiving and Communication System, GE health care, Mount prospect, IL, USA) and the average of their results was recorded. The parameters included SVA, lumbar lordosis (LL), thoracic kyphosis (TK), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), Cobb angle of the curves, and TPA (the angle subtended by the line from the femoral head axis to the centroid of T1 and the line from the femoral head axis to the middle of the S1 endplate) (Figure 1). Measurements of sagittal parameters.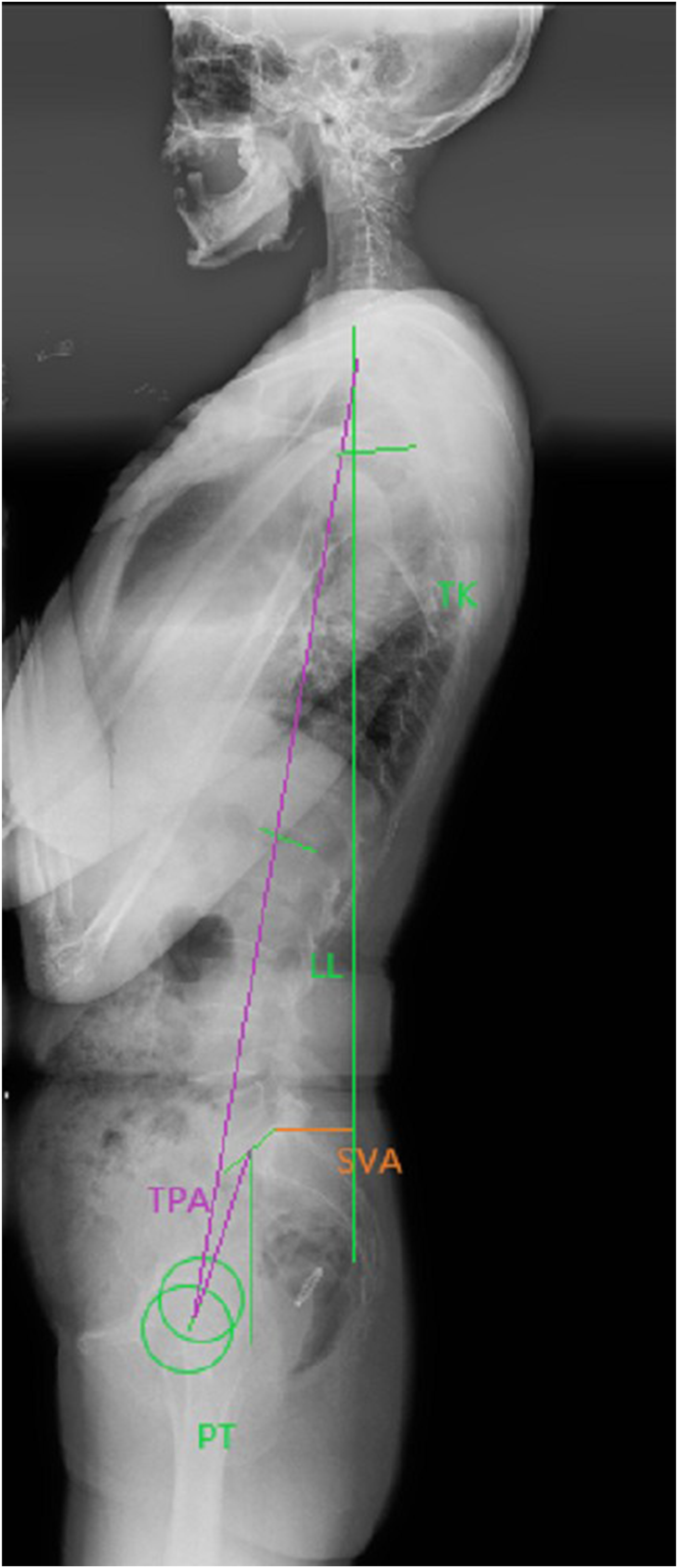
Statistical Analysis
SPSS version 19.0 (SPSS Inc, Chicago, IL, USA) was used to analyze the collected data. Pearson correlation analysis was used to evaluate the relationship between HRQOL and sagittal alignment. Receiver operating characteristic (ROC) curve was used to evaluate the predictive effect of SVA, TPA, relative TPA and to find out the most optimum cutoff point of TPA to predict a good clinical outcome (ODI <40). Logistic regression model was used to identify the independent risk factors of a bad clinical outcome (ODI >40). Comparison between 2 groups was performed by using the student t-test. Multifactor regression analysis was conducted to determine the relationship between postoperative TPA and other parameters. Statistical significance was set at P-value < .05.
Results
General Profiles
The basic information of the ADS patients
Preoperative and Postoperative Radiographic Data and Functional Evaluation
Preoperative SVA (r = 0.301), SS (r = −0.198), LL (r = −0.261) were all significantly related with the patient’s preoperative functional evaluation (P < .05), and SVA showed the highest relationship with ODI among all parameters (r = 0.301, P < .01).
The preoperative and postoperative sagittal parameters and health related quality of life (HRQOL) in patients.
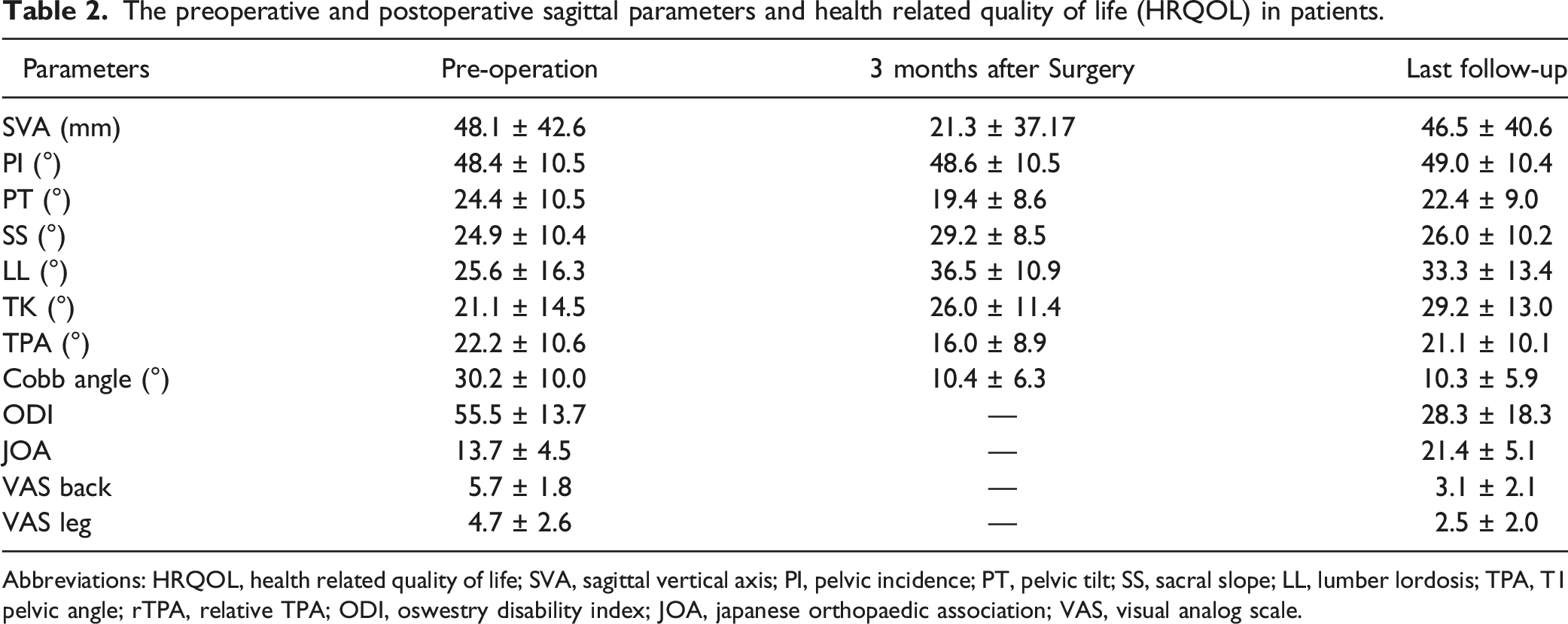
Abbreviations: HRQOL, health related quality of life; SVA, sagittal vertical axis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; LL, lumber lordosis; TPA, T1 pelvic angle; rTPA, relative TPA; ODI, oswestry disability index; JOA, japanese orthopaedic association; VAS, visual analog scale.
Correlations between sagittal alignment at 3 months after surgery and functional evaluation at last follow-up.
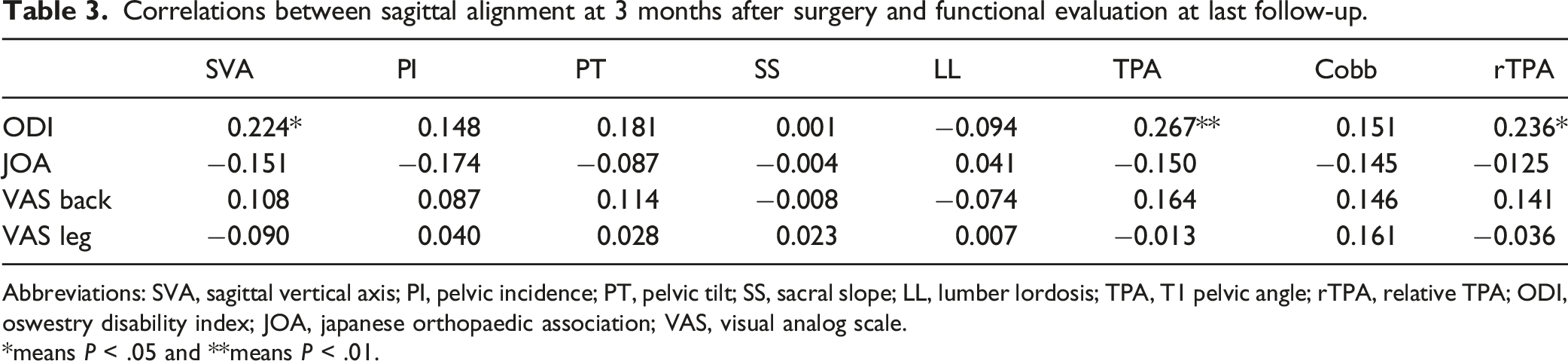
Abbreviations: SVA, sagittal vertical axis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; LL, lumber lordosis; TPA, T1 pelvic angle; rTPA, relative TPA; ODI, oswestry disability index; JOA, japanese orthopaedic association; VAS, visual analog scale.
*means P < .05 and **means P < .01.
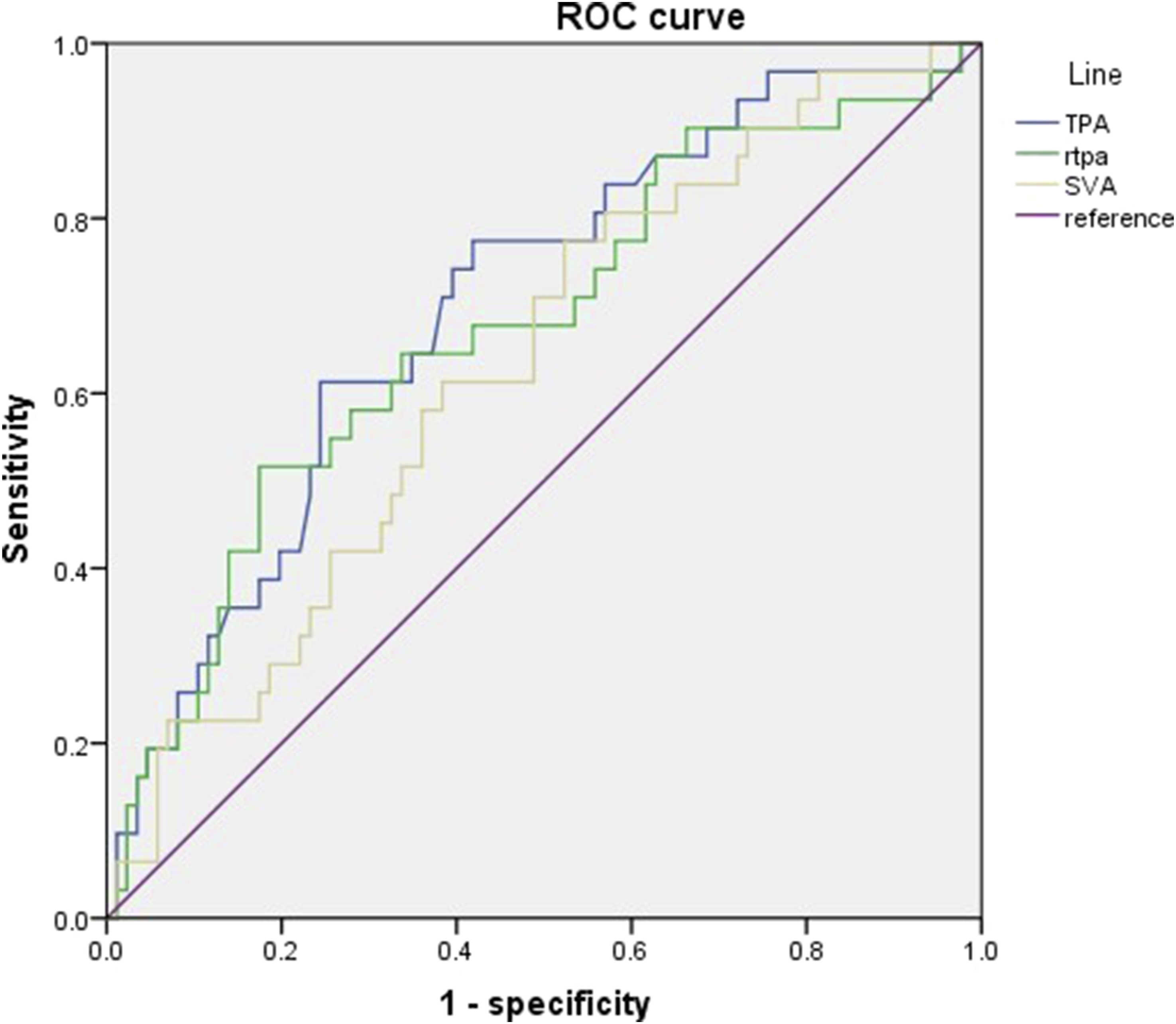
ROC curve to compare the predictive effect of SVA, TPA, and rTPA for a good clinical outcome (ODI <40). Abbreviations: ROC, receiver operating characteristic; SVA, sagittal vertical axis; TPA, T1 pelvic angle; rTPA, relative TPA; ODI, oswestry disability index.
Univariate and multivariate analysis for bad clinical outcomes (ODI>40) in 117 ADS patients by logistic regression.
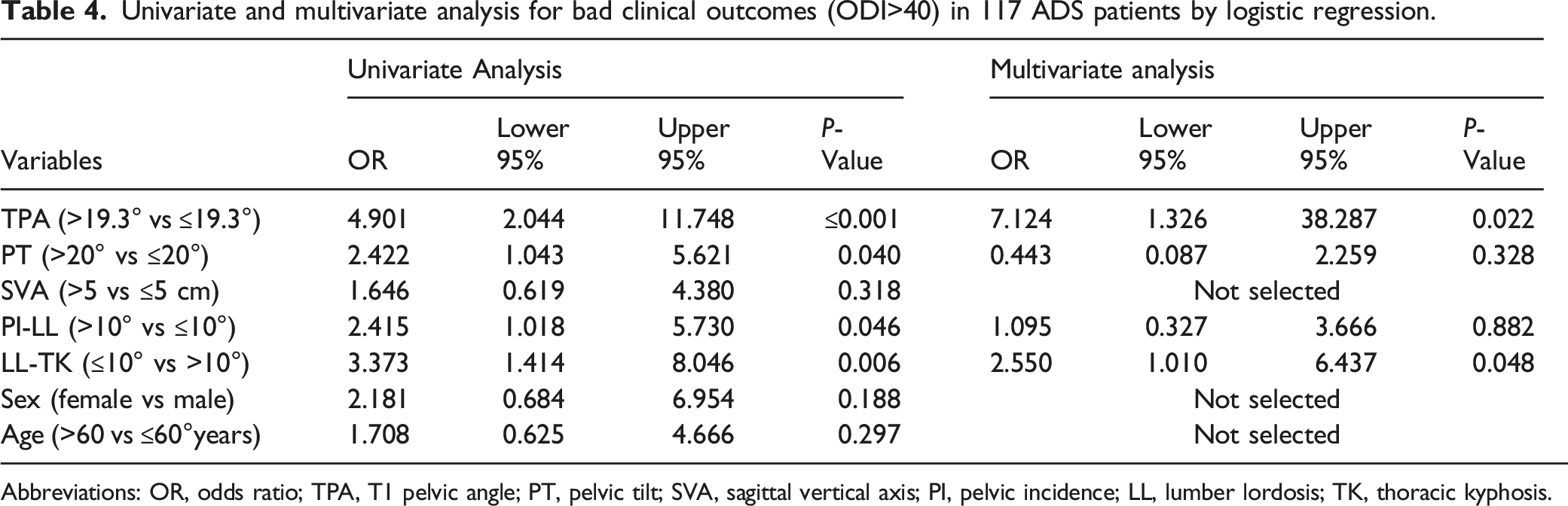
Abbreviations: OR, odds ratio; TPA, T1 pelvic angle; PT, pelvic tilt; SVA, sagittal vertical axis; PI, pelvic incidence; LL, lumber lordosis; TK, thoracic kyphosis.
The comparison between group A and group B.
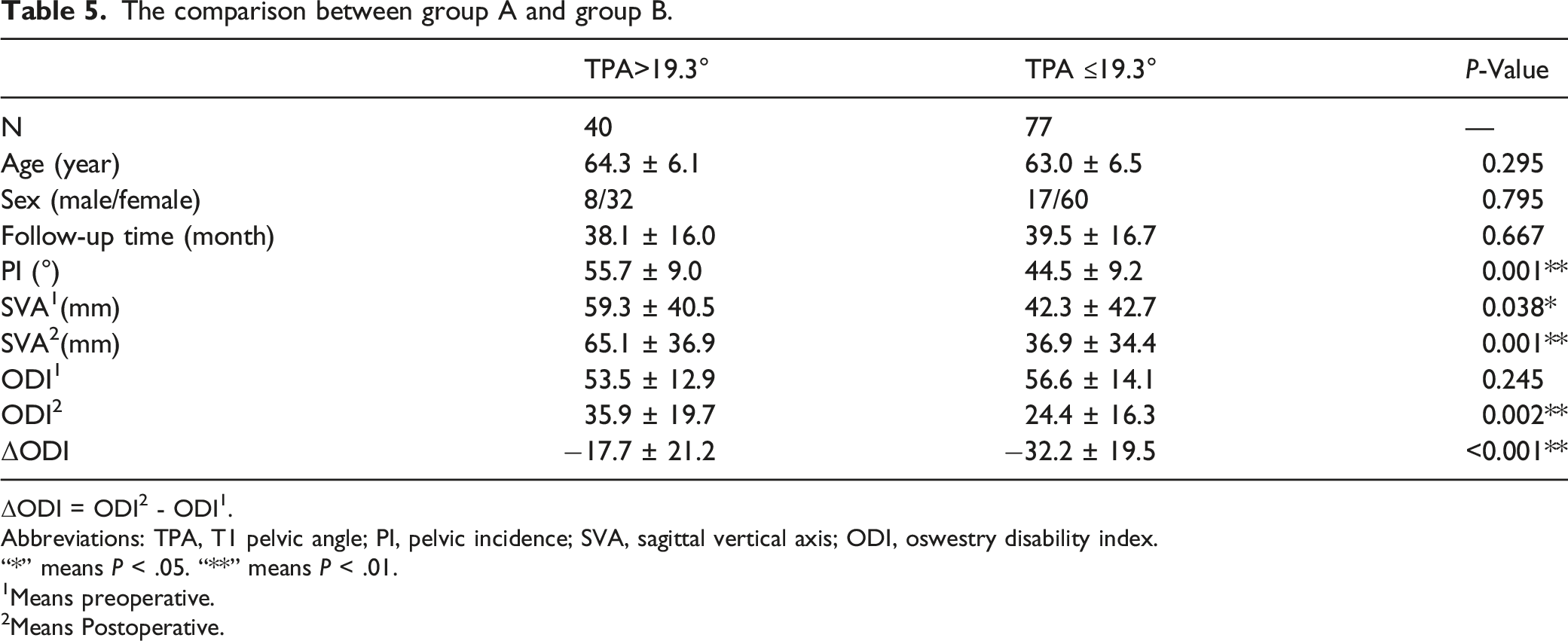
ΔODI = ODI2 - ODI1.
Abbreviations: TPA, T1 pelvic angle; PI, pelvic incidence; SVA, sagittal vertical axis; ODI, oswestry disability index.
“*” means P < .05. “**” means P < .01.
1Means preoperative.
2Means Postoperative.
The comparison between group C and group D.
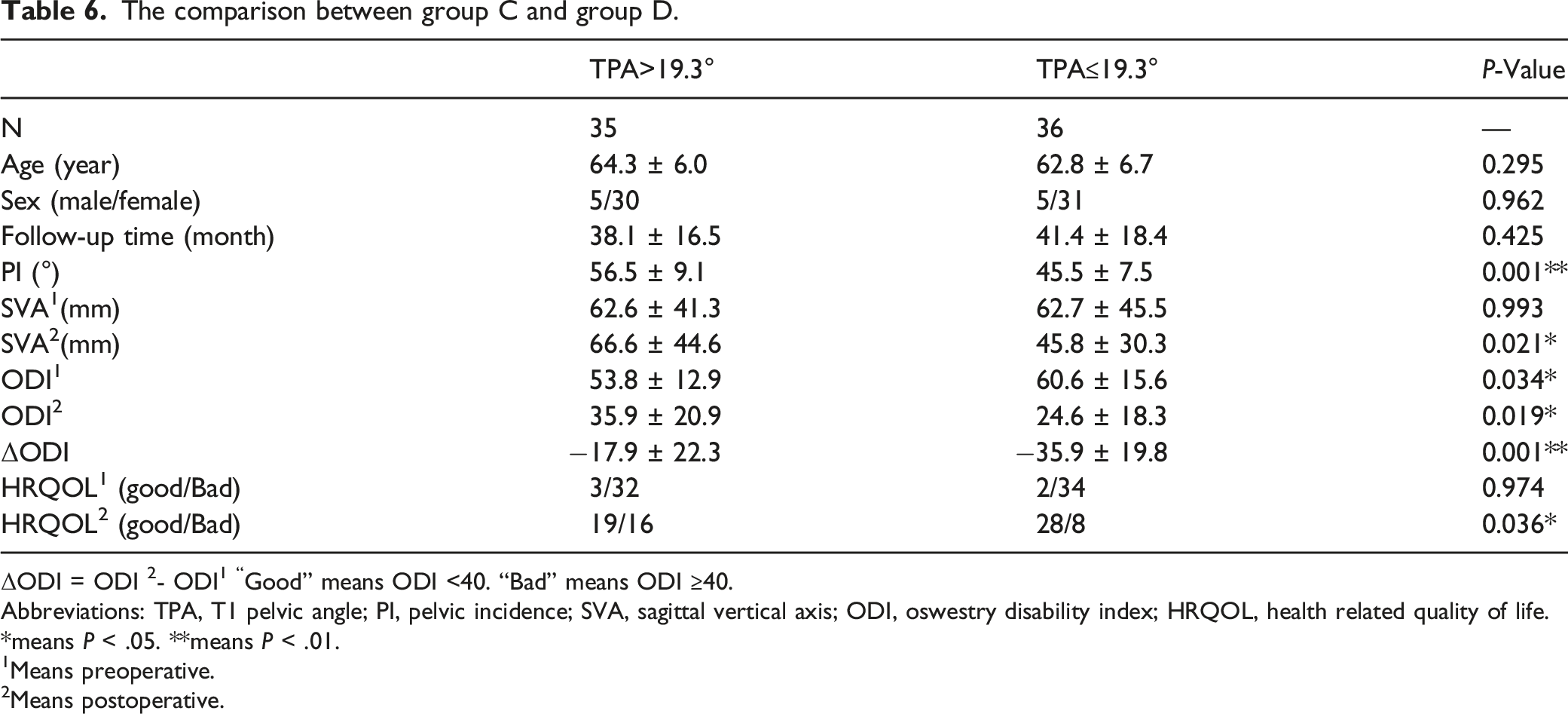
ΔODI = ODI 2- ODI1 “Good” means ODI <40. “Bad” means ODI ≥40.
Abbreviations: TPA, T1 pelvic angle; PI, pelvic incidence; SVA, sagittal vertical axis; ODI, oswestry disability index; HRQOL, health related quality of life.
*means P < .05. **means P < .01.
1Means preoperative.
2Means postoperative.
These findings indicated that correcting TPA less than 19.3° for patients with preoperative TPA > 19.3° attributed to a better HRQOL and sagittal balance at last follow-up.
The Formula to Predict the Postoperative TPA
According to previous research23,28,29, a formula based on PI and postoperative LL and SS was established to predict the postoperative TPA by using a multifactor regression analysis based on the radiographic data of 117 ADS patients, and the relationship between TPA and LL, PI was presented as:
Postoperative TPA = 0.923 × PI − 0.241 × postoperative LL − 0.593 × postoperative SS − 2.471 (r = 0.914, r2 = 0.836, P < .001).
Discussion
Spinopelvic sagittal parameters have been widely used to evaluate the severity of ASD and guide the surgical procedure. As Schwab proposed SVA, PT, PI-LL as 3 key parameters which were most significantly related with HRQOL of ASD patients, 14 SVA less than 5 cm, PT less than 25°, PI-LL within ± 10° were extensively accepted correction goals for ASD patients.15,30 However, some problems existed in this evaluation system. First, SVA were easily influenced by patient’s posture, 31 which could interfere the accuracy of preoperative and postoperative evaluation of sagittal balance, so judgement based on TPA could be more effective.19,20 On the other hand, as proposed by Yilgor et al, the sagittal parameters should be evaluated in relation to PI, we developed the conception named “relative TPA”, which is defined as actual TPA minus ideal TPA. Relative TPA could take personal pelvic morphology and age into consideration during the judgement of sagittal balance. But whether relative TPA could predict the clinical outcomes more effectively should be further explored. So we made detailed comparison for the 3 parameters. TPA was most correlated to ODI at last follow-up (r = 0.267, P < .01) and presented the largest AUC among them. For patients with long fused spine after correction surgery, TPA which combined the information of truncal inclination and pelvic retroversion was less influenced by posture. So TPA could more precisely reflect the real global sagittal balance of these patients, and this was also why TPA most highly correlated with postoperative HRQOL. Although including some individual parameters, relative TPA was not better than actual TPA in the prediction of clinical outcomes for patients with ADS. This might be caused by the inaccuracy of the current formula for ideal TPA (r2 = 0.328). Meanwhile, relative TPA might fit the patients with extreme PI values, but for most patients, the actual TPA could already be a useful parameter to predict their clinical outcome.
Prior studies have also evaluated the predictive effect of TPA on the postoperative sagittal balance and HRQOL in adult scoliosis.18,19,21 TPA combines both the information of SVA and PT, which might simplify the correction goal proposed by Schwab. Banno et al 20 reported that TPA was most closely associated with postoperative HRQOL, which was in keeping with our study, and they proposed that TPA <20° should be the target of corrective surgery for patients with ASD. Yang et al 32 demonstrated that TPA <20° could be used to judge the sagittal balance for patients with unspecific low back pain. However, the previous studies ignored something important. Yang and Banno quoted the TPA cutoff value proposed by Ryan et al 21 directly and made the group comparison of parameters and HRQOL by this value. These could only illustrate patients with early postoperative TPA <20° presented better clinical outcomes, which lacked comparison of preoperative and postoperative changes. In addition, Ryan et al 21 obtained the threshold for TPA by the regression formula (TPA = 8.647 + 0.273 × ODI, r2 = 0.19). It was not accurate enough to get a cutoff value for using the formula with r2 = 0.19. Instead, we used ROC curve with high AUC and set the cutoff value of TPA at 19.3° (61.3% for sensitivity, 75.6% for specificity) to predict a good clinical outcome (ODI <40). Furthermore, TPA >19.3° was the highest independent risk factor according to the logistic regression (OR = 7.124, P = .022, Table 4). Compared to other predictors, TPA contained more information about both truncal inclination and pelvic retroversion. This might be why TPA stood out in multivariate regression.
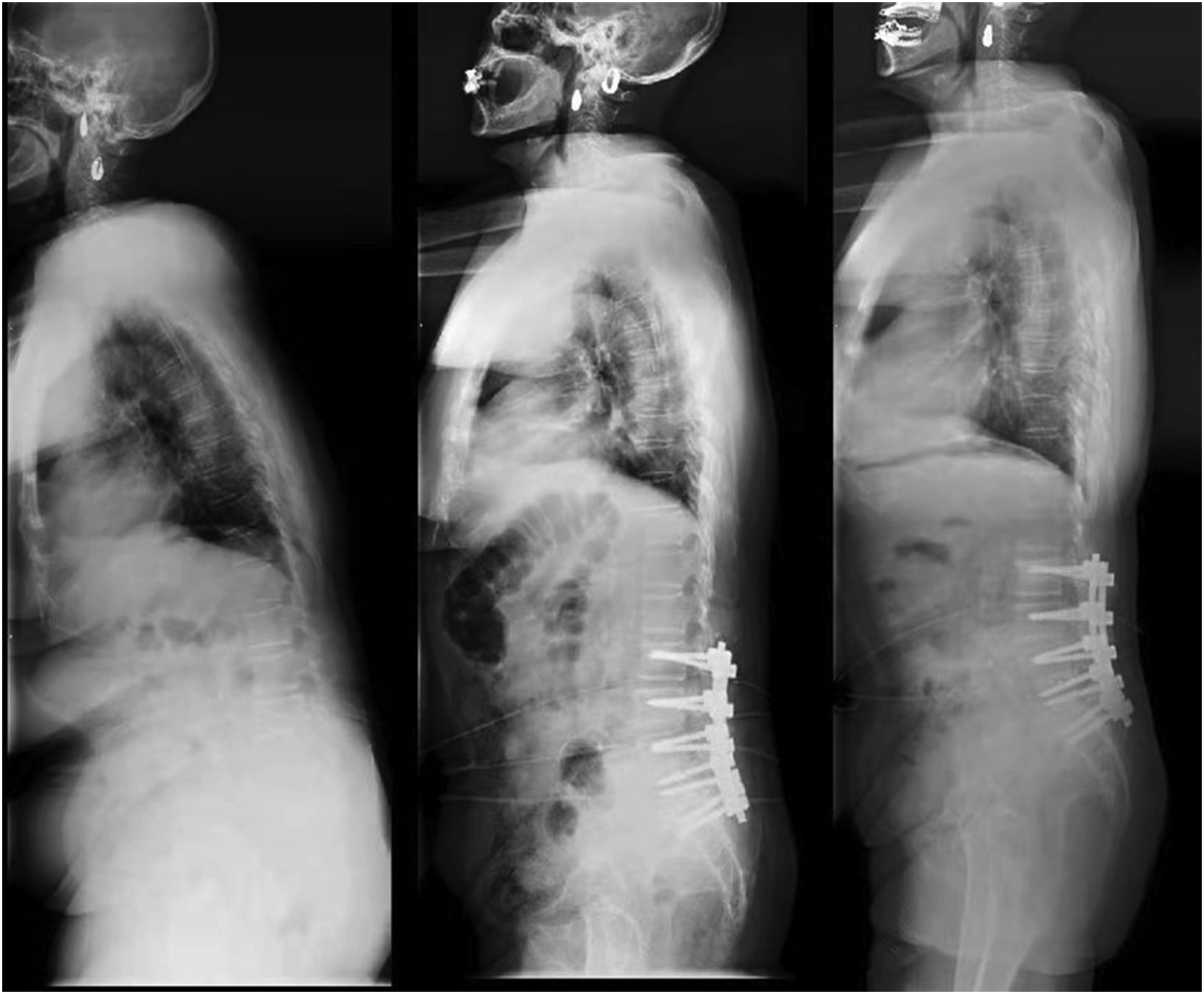
As presented in Table 5, patients with relative TPA <19.3° showed a significantly better ODI and SVA at last follow-up than those with TPA >19.3°. Afterward we selected 71 patients with preoperative TPA >19.3° and Divided them into 2 group (group C with postoperative TPA ≤19.3°, group D with TPA >19.3°) to explore the surgical outcome by correcting TPA above 19.3°. Interestingly, the group D presented higher preoperative ODI than group C but showed lower postoperative ODI, SVA at last follow-up. Therefore, we proposed that keeping TPA <19.3° should be the optimal correction goal for patients with ADS (Figures 3 and 4). Although our result was close to previous research, it was reached through a more accurate and rigorous method. Sagittal parameters of a 61 years old female ADS patient who reached ideal TPA with good prognosis. Pre-operation (left): SVA = 23.4 mm, TPA = 24.4°, VAS back = 8, VAS leg = 4, ODI = 70, JOA = 12; 3 months after surgery (middle): SVA = 28.9 mm, TPA = 12.0°; last follow-up (right): SVA = 9.4 mm, TPA = 15.1°, VAS back = 1 VAS leg = 0, ODI = 4, JOA = 29. Abbreviations: ADS, adult degenerative scoliosis; SVA, sagittal vertical axis; TPA, T1 pelvic angle; ODI, oswestry disability index; JOA, japanese orthopaedic association; VAS, visual analog scale. Sagittal parameters of a 71 years old female ADS patient who did not reach ideal TPA with bad prognosis. Pre-operation (left): SVA = 179.3 mm, TPA = 54.8°, VAS back = 5, VAS leg = 5, ODI = 68, JOA = 6; 3 months after surgery (middle): SVA = 82.8 mm, TPA = 36.6°; last follow-up (right): SVA = 66.8 mm, TPA = 31.0°, VAS back = 6 VAS leg = 0, ODI = 58, JOA = 10. Abbreviations: ADS, adult degenerative scoliosis; SVA, sagittal vertical axis; TPA, T1 pelvic angle; ODI, oswestry disability index; JOA, japanese orthopaedic association; VAS, visual analog scale.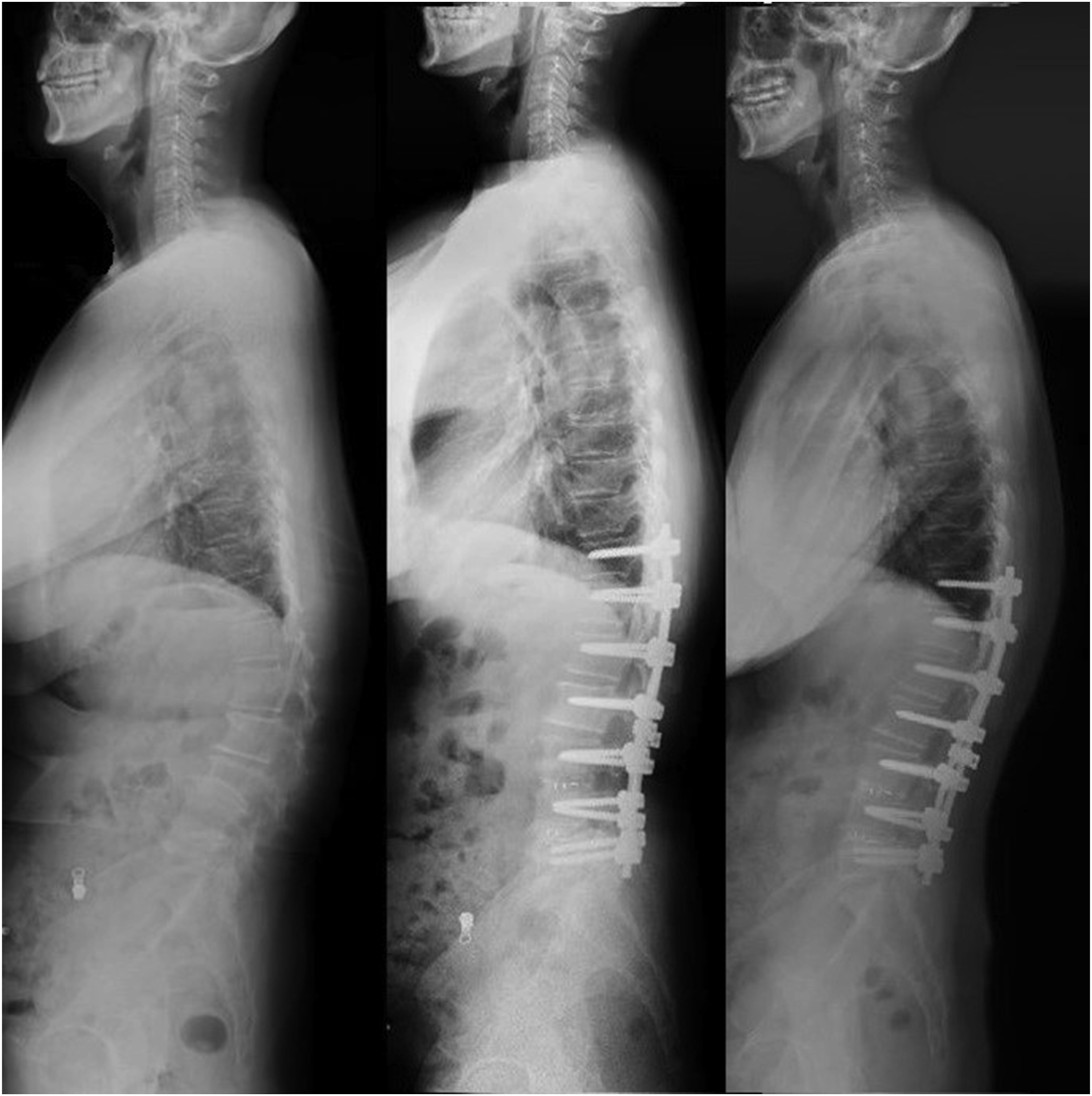
In order to better apply our results to clinical practice, we put forward a formula based on PI and postoperative LL and SS to predict the postoperative TPA, presented as postoperative TPA = 0.923 × PI − 0.241 × postoperative LL − 0.593 × postoperative SS − 2.471 (r = 0.914, r2 = 0.836, P < .001). As LL and SS could be remodeled or measured during surgery and PI was a fixed value in adults, this formula with high r2 gave us a direct access to achieve the ideal postoperative TPA value through corrective surgery.
There were still some limitations in this study. First, this was a single-center retrospective study, which might cause selection bias. The power analysis was not done for all factors so the sample size might need to be expanded. Second, our study only included Chinese population, so the threshold of TPA and the predictive formula should be carefully applied in other races. Third, a few references were not from high-standard literature. Despite these limitations, our study was the first to propose the correction goal for Chinese population based on TPA.
Conclusion
This study demonstrated that TPA was a useful global parameter for the prediction of postoperative HRQOL for patients with ADS. Keeping TPA <19.3° could improve the postoperative HRQOL for ADS patients with preoperative TPA >19.3°, and TPA < 19.3° could be an optimum correction target for patients with ADS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Natural Science Foundation of China (Grant No.81871807).
Ethics Approval
Ethics Committee of the Peking University Third Hospital approved this study. The IRB approval number is IRB00006761-2014200.