
Abstract
Study Design
Retrospective review.
Objectives
The International Spine Study Group-AO (ISSG-AO) Adult Spinal Deformity (ASD) Complication Classification System was developed to improve classification, reporting, and study of complications among patients undergoing ASD surgery. The ISSG-AO system classifies interventions to address complications by level of invasiveness: grade zero (none); grade 1, mild (e.g., medication change); grade 2, moderate (e.g., ICU admission); grade 3, severe (e.g., reoperation related to surgery of interest). To evaluate the efficacy of the ISSG-AO ASD Complication Classification System, we aimed to compare correlations between postoperative length of stay (LOS) and complication severity as classified by the ISSG-AO ASD and traditional major/minor complication classification systems.
Methods
Patients age ≥18 in a multicenter ASD database who sustained in-hospital complications were identified. Complications were classified with the major/minor and ISSG-AO systems and correlated with LOS using an ensemble-based machine learning algorithm (conditional random forest) and a generalized linear mixed model.
Results
490 patients at 19 sites were included. 64.9% of complications were major, and 35.1% were minor. By ISSG-AO classification, 20.4%, 66.1%, 6.7%, and 6.7% were grades 0-3, respectively. ISSG-AO complication grading demonstrated significant correlation with LOS, whereas major/minor complication classification demonstrated inverse correlation with LOS. In conditional random forest analysis, ISSG-AO classification had the greatest relative importance when assessing correlations across multiple variables with LOS.
Conclusions
The ISSG-AO system may help identify specific complications associated with prolonged LOS. Targeted interventions to avoid or reduce these complications may improve ASD surgical quality and resource utilization.
Keywords
Introduction
Adult spinal deformity (ASD) is common, with reported prevalence rates as high as 68% among elderly patients. 1 Symptomatic patients may experience debilitating back pain and neurologic deficits, 2 resulting in levels of disability similar to other chronic diseases including diabetes, heart disease, and cancer. 3 Surgical advances have improved surgeons’ ability to correct deformities; however, ASD patients are frequently elderly with multiple comorbidities, 4 and surgery is associated with complication rates ranging from 37%–71%.5-9
Complications are an important metric for assessing and improving surgical quality and safety. Various complication classification systems have been implemented in ASD. Such classification systems include the widely used major/minor complication classification system,10,11 as well as the International Spine Study Group (ISSG)-AO ASD Complication Classification System. 12 In order to be useful, complication classification systems should be tied to clinically meaningful outcomes. Important outcomes include length of stay (LOS), which has been tied to readmission risk, 13 costs, 14 and satisfaction15-18 among patients undergoing spinal surgery.
While the traditional classification of complications as major/minor is useful for broadly defining complications, such broad definitions may not adequately allow for assessment of complications’ association with important outcome metrics including LOS. In contrast to the major/minor complication classification system, the ISSG-AO system was developed specifically for ASD to allow for more precise complication classification. The granular ISSG-AO complication classification system includes sub-classification of interventions to address complications by level of invasiveness, as follows: Grade zero (none); Grade 1, mild (e.g., medication change); Grade 2, moderate (e.g., ICU admission); Grade 3, severe (reoperation related to surgery of interest).
Given the substantial differences in the major/minor and ISSG-AO ASD complication classification systems, the purpose of this study was to compare whether complications classified by the major/minor and ISSG-AO ASD systems were associated with hospital LOS. We hypothesized that the disease-specific ISSG-AO ASD complication classification system intervention grade sub-component would demonstrate greater correlation with LOS as compared to broadly classifying complications as major/minor.
Materials and Methods
Patients and Covariates
Baseline, Surgical, and Perioperative Variables.
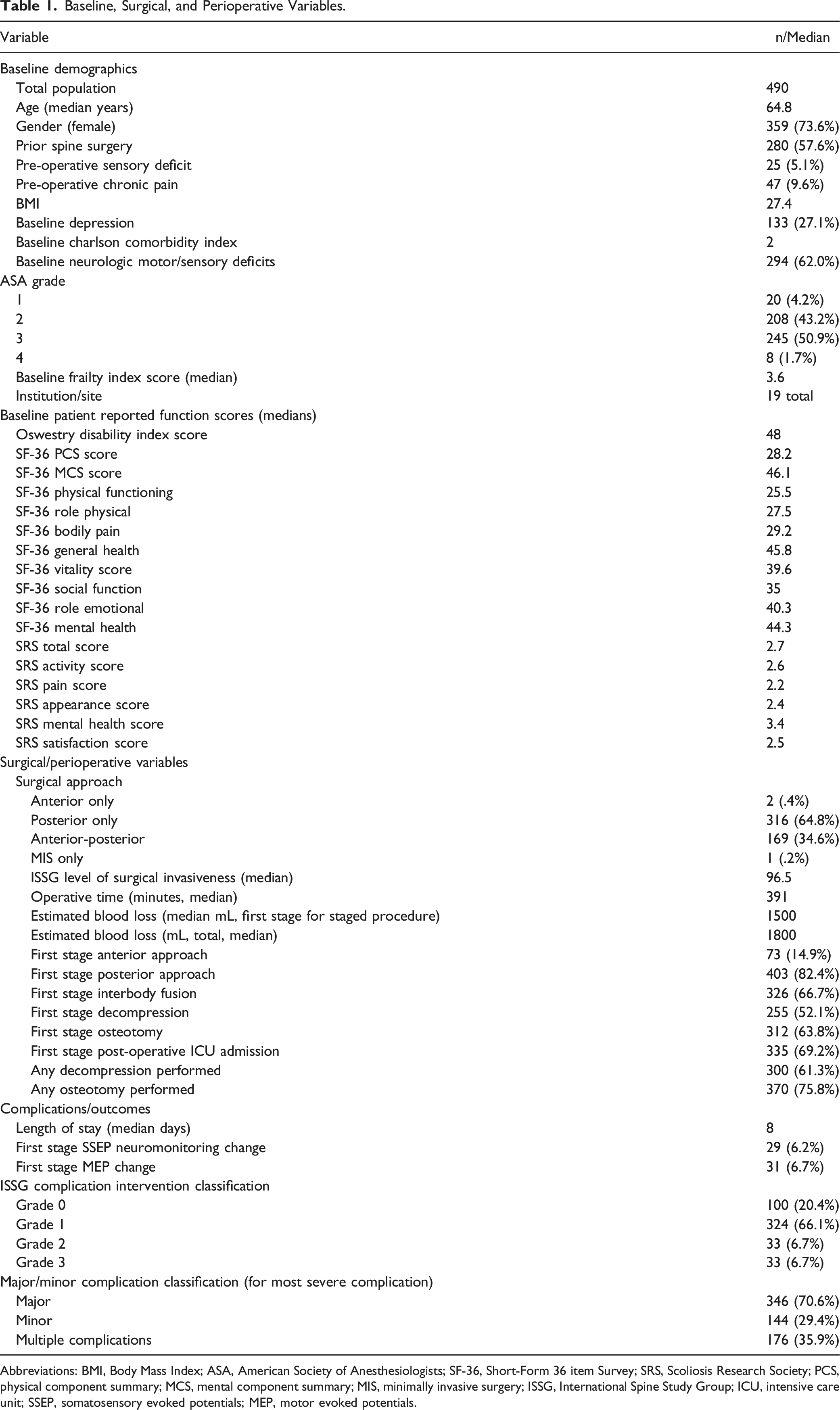
Abbreviations: BMI, Body Mass Index; ASA, American Society of Anesthesiologists; SF-36, Short-Form 36 item Survey; SRS, Scoliosis Research Society; PCS, physical component summary; MCS, mental component summary; MIS, minimally invasive surgery; ISSG, International Spine Study Group; ICU, intensive care unit; SSEP, somatosensory evoked potentials; MEP, motor evoked potentials.
Complication Grading
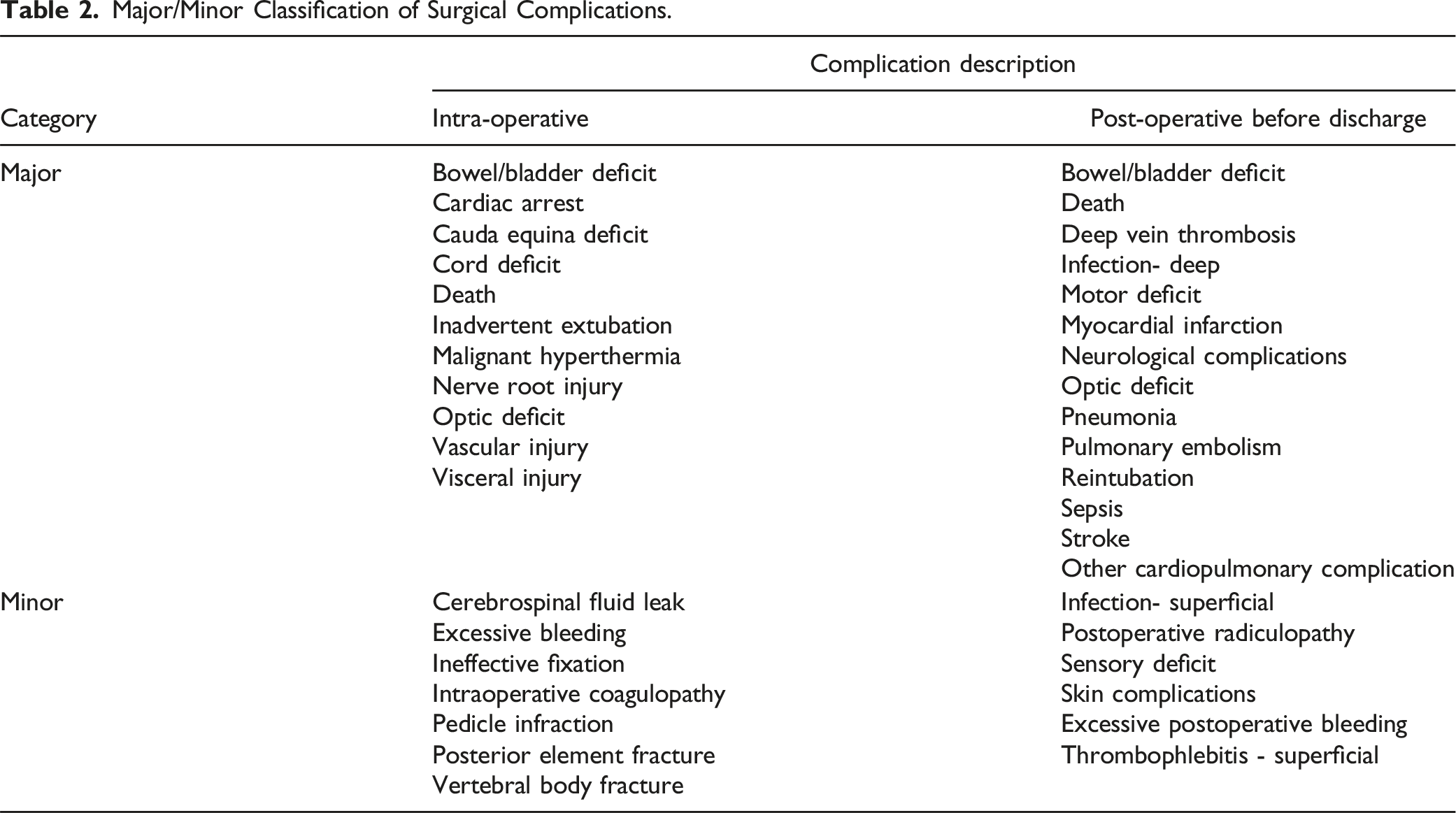
Major/Minor Classification of Surgical Complications.
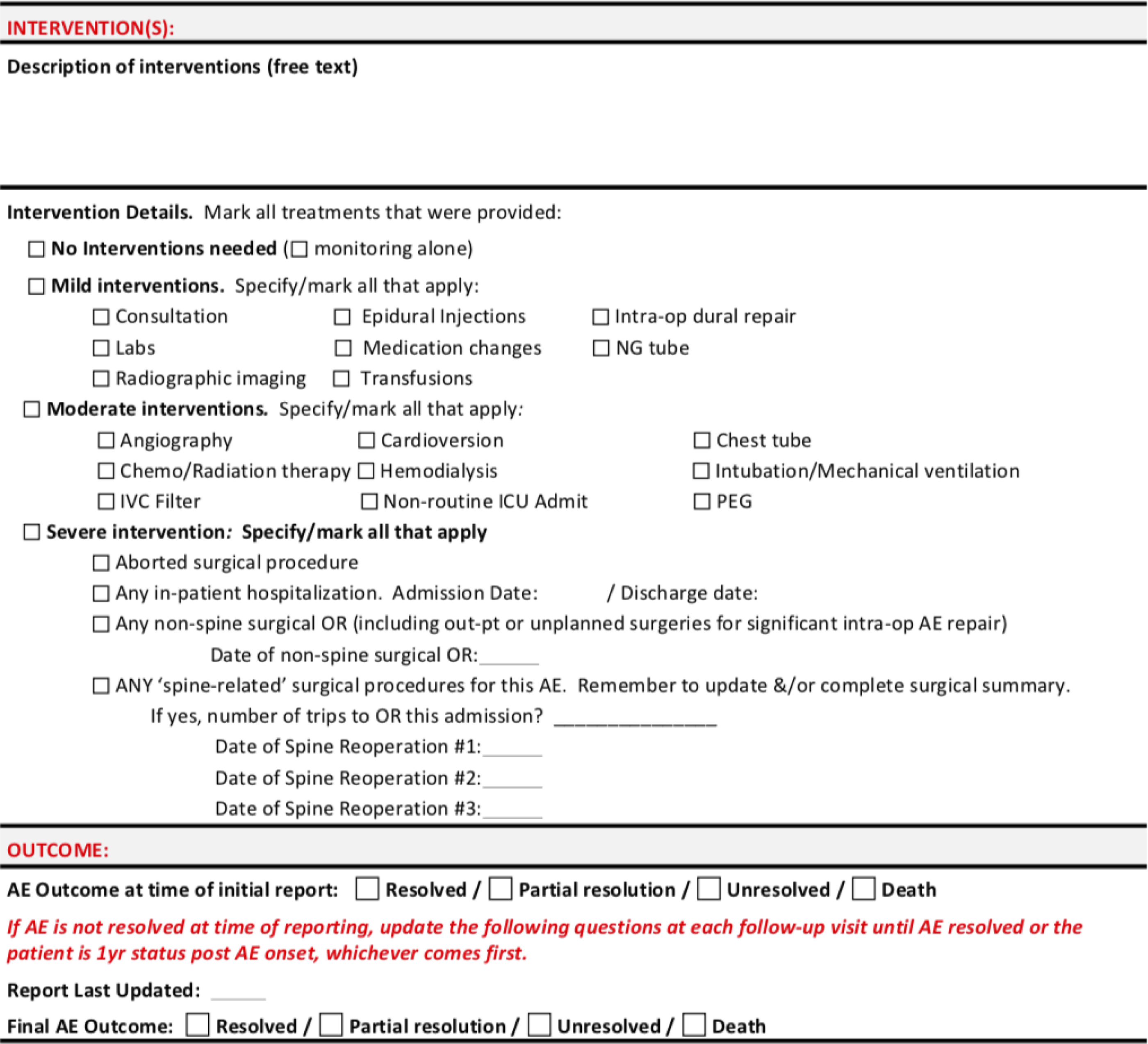
ISSG-AO complication classification system grading worksheet. The “Intervention Details” section was used to grade the intervention severity for each complication, as follows: No interventions = Grade 0, Mild interventions = Grade 1, Moderate interventions = Grade 2, Severe interventions = Grade 3.
Univariate Comparisons
Initial univariate analyses were performed to assess correlation of variables with LOS and to assess the effect of patients sustaining multiple complications. To assess the effect of multiple complications of varying severity on LOS, Kruskal-Wallis tests were used to compare LOS vs complication grade and LOS vs major/minor complications. Specifically, comparisons were performed between patients with and without multiple complications by evaluating patients based on their least severe, median severity, and most severe complications. Among those sustaining multiple complications, “median grade” and “median severity” were calculated for the ISSG-AO ASD complication classification system and the major/minor complication systems, respectively. For the ISSG-AO complication classification system, median complication grade was based on the median intervention grade of all complications sustained by the patient. Similarly, for the major/minor system, median complication severity was determined by whether patients sustained a greater number of minor or major complications.
Multivariate Comparisons
Two multivariate modeling approaches were employed to further assess associations with LOS. In the first model, a conditional random forest machine learning algorithm analyzed relative importance of each demographic, surgical, and perioperative variable in association with LOS. To account for patients sustaining multiple complications, the model was repeated to assess relative importance of ISSG-AO complication grade and major/minor classification in relation to patients’ least severe, median severity, and most severe complication. The conditional random forest model also included a “multiple complications” variable to account for patients who sustained more than one complication.
A generalized linear mixed model using a Poisson distribution with a log link was constructed. The hospital/participating center for each surgery was considered as a random effect to account for clustering of patients within the same hospital. Variables from the univariable analysis were included as potential confounders if their association with LOS was significant at P < 0.1. Separate generalized linear mixed models were constructed to assess fit for LOS against ISSG-AO grade and adjustment variables, as well as fit for LOS against major/minor and adjustment variables. For complication severity grade using the ISSG-AO system, additional pairwise comparisons were performed by grouping complication grades and comparing LOS between these groups.
All analyses were performed by an institutional statistician using R, version 4.1.2 (https://www.r-project.org). Level of significance was set at P = .05.
Results
Patients and Covariates
The ISSG database includes a total of 1999 participants. A total of 616 patients were identified in the database as having sustained one or more in-hospital complications and were reviewed for study inclusion (Table 1). Patients were excluded if they were missing complication status information, data necessary for complication grading, or if patients had incomplete hospital admission and discharge data precluding LOS calculation. Of the 616 patients, a total of 490 had complete data and were included in the final analysis. Among included patients, 73.6% were female, median age was 64.8 years, and 57.6% of patients had a history of prior spine surgery. Median LOS was 8 days. When classified by the ISSG-AO system, 20.4% of complications were Grade 0, 66.1% were Grade 1, 6.7% were Grade 2, and 6.7% were Grade 3. When classified by the major/minor complication classification system, 70.6% were major and 29.4% were minor. A total of 35.9% of patients sustained multiple complications.
Univariate Comparisons
Figure 2 shows results of Kruskal-Wallis comparisons between patients with and without multiple complications. Increasing complication severity as classified by the ISSG-AO system correlated with increased LOS regardless of whether patients sustained one or multiple complications. The strongest correlation was identified between LOS and most severe complication as classified by the ISSG-AO system, with P = 3.4 × 10−6. Kruskal-Wallis comparisons between patients with and without multiple complications, with comparisons performed for complications graded using the ISSG-AO ASD complication classification system (top row) and major/minor classification system (bottom row). For those sustaining multiple complications, “median grade” represents the median value of complication intervention severity of all complications sustained by patients, as determined based on the ISSG-AO complications classification system. “Median severity” represents the median value of all major/minor complications sustained by patients, as determined based on major/minor complications classification. KW value represents P-value, with level of significance at P = .05.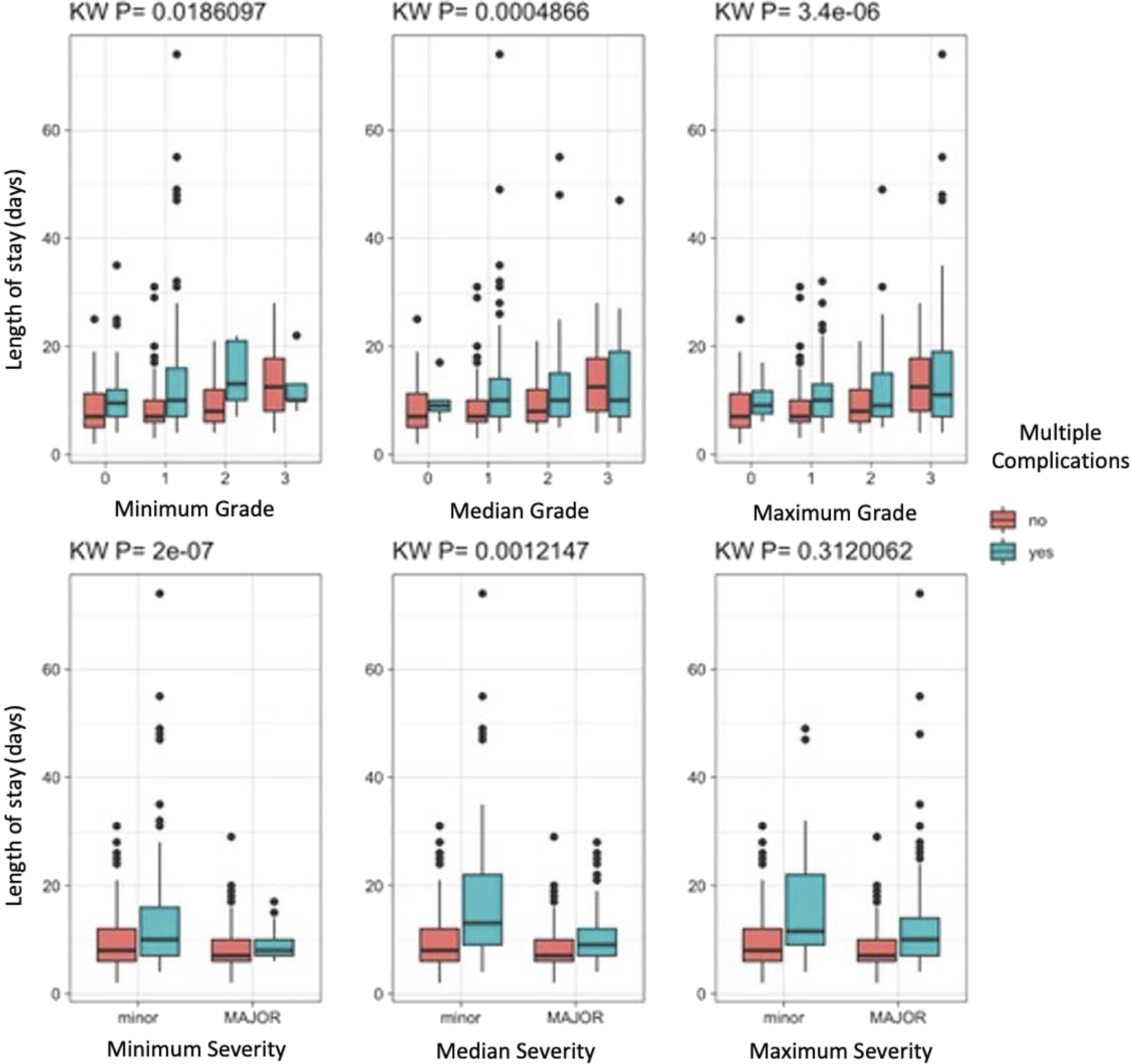
When classified as major/minor, longer LOS was correlated with minor rather than major complications when patients were assessed based on their least severe and median severity complication (p = 2 × 10−7 and P = 1.2 × 10−3, respectively). No correlation was identified between major/minor complication severity and LOS when patients were evaluated based on their most severe complication sustained.
Multivariate Modeling and Pairwise Comparisons
Figure 3 shows results of the conditional random forest machine learning algorithm analyzing relative importance of association between variables and LOS when patients were evaluated based on their most severe complication. For this analysis, ISSG-AO grade was found to have the highest relative importance, approaching 1.0 in relation to LOS, followed in decreasing order by multiple complications, posterior approach, and baseline disability. Classification of complications as major/minor had much less importance in relation to LOS, with a relative value of <0.1. Conditional random forest machine learning algorithm analyzing relative importance of association between variables and LOS when patients were evaluated based on their most severe complication. Abbreviations: ODI, Oswestry Disability Index; ISSG, International Spine Study Group; SRS, Scoliosis Research Society; SF-36, Short Form 36-Item Survey; BMI, Body Mass Index.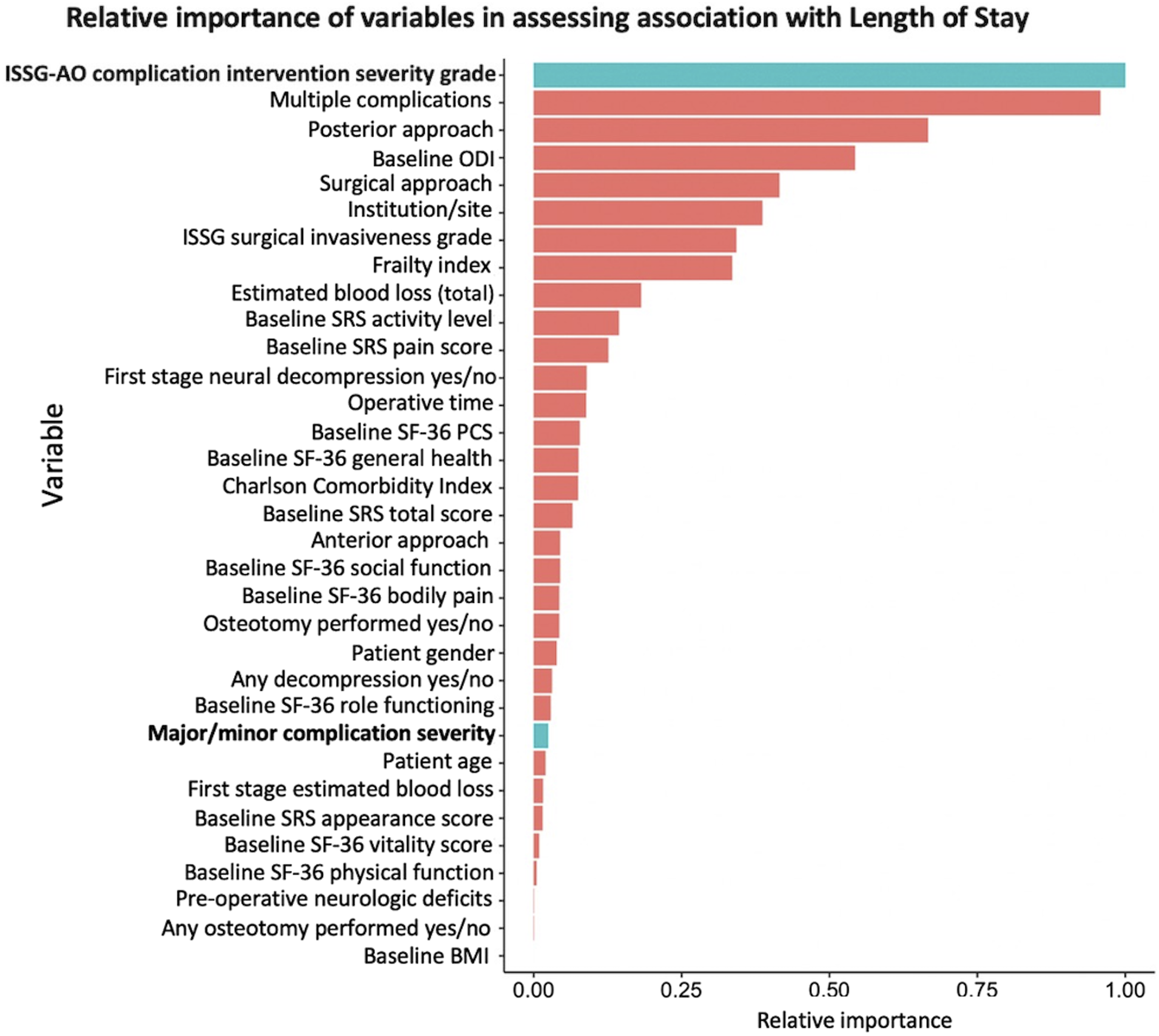
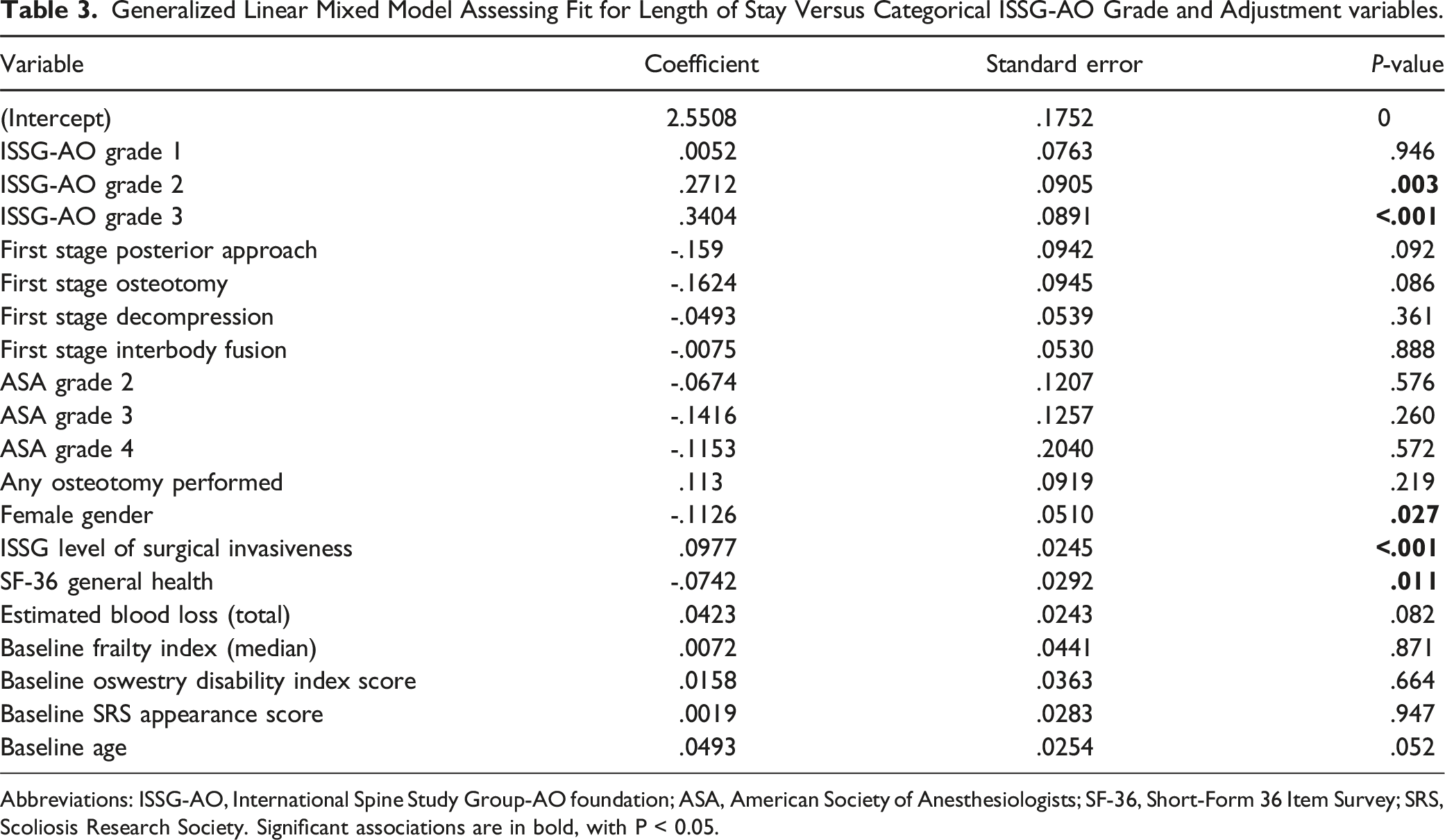
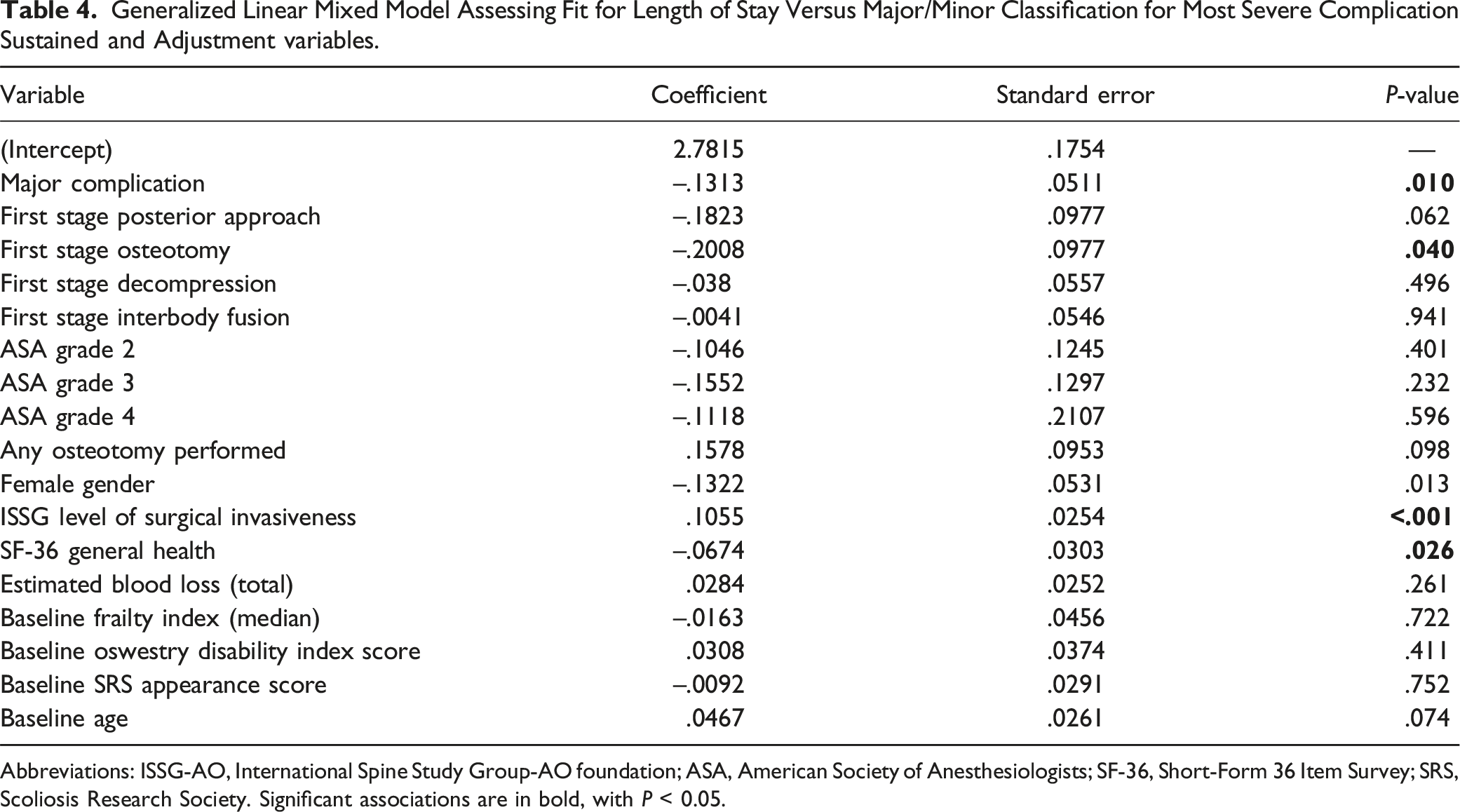
Figure 4 shows results of generalized linear mixed models. When fit for LOS vs ISSG-AO grade and adjustment variables (Table 3), the model demonstrated significant correlation between increased ISSG-AO complication grade and LOS, with P = .0027 for Grade 2, and P < .001 for Grade 3 complications. Female gender, level of invasiveness, and baseline general health were additionally found to correlate significantly with LOS. In contrast to ISSG-AO grade, general linear mixed model fit for LOS vs major/minor complication classification and adjustment variables (Table 4) found a significant, inverse correlation between increased complication severity (major complication as opposed to minor complication), with coefficient of -.1313 and P = .012. In this analysis, performance of an osteotomy during the first stage of surgery, level of surgical invasiveness, and baseline SF-36 general health were also found to correlate with increased LOS. Generalized linear mixed models fit for length of stay vs complication severity graded by major/minor classification (left panel) and ISSG grade (right panel). Fit for major/minor classification was repeated based on patients’ most severe and least severe complications. Abbreviations: ISSG, International Spine Study Group. Generalized Linear Mixed Model Assessing Fit for Length of Stay Versus Categorical ISSG-AO Grade and Adjustment variables. Abbreviations: ISSG-AO, International Spine Study Group-AO foundation; ASA, American Society of Anesthesiologists; SF-36, Short-Form 36 Item Survey; SRS, Scoliosis Research Society. Significant associations are in bold, with P < 0.05. Generalized Linear Mixed Model Assessing Fit for Length of Stay Versus Major/Minor Classification for Most Severe Complication Sustained and Adjustment variables. Abbreviations: ISSG-AO, International Spine Study Group-AO foundation; ASA, American Society of Anesthesiologists; SF-36, Short-Form 36 Item Survey; SRS, Scoliosis Research Society. Significant associations are in bold, with P < 0.05.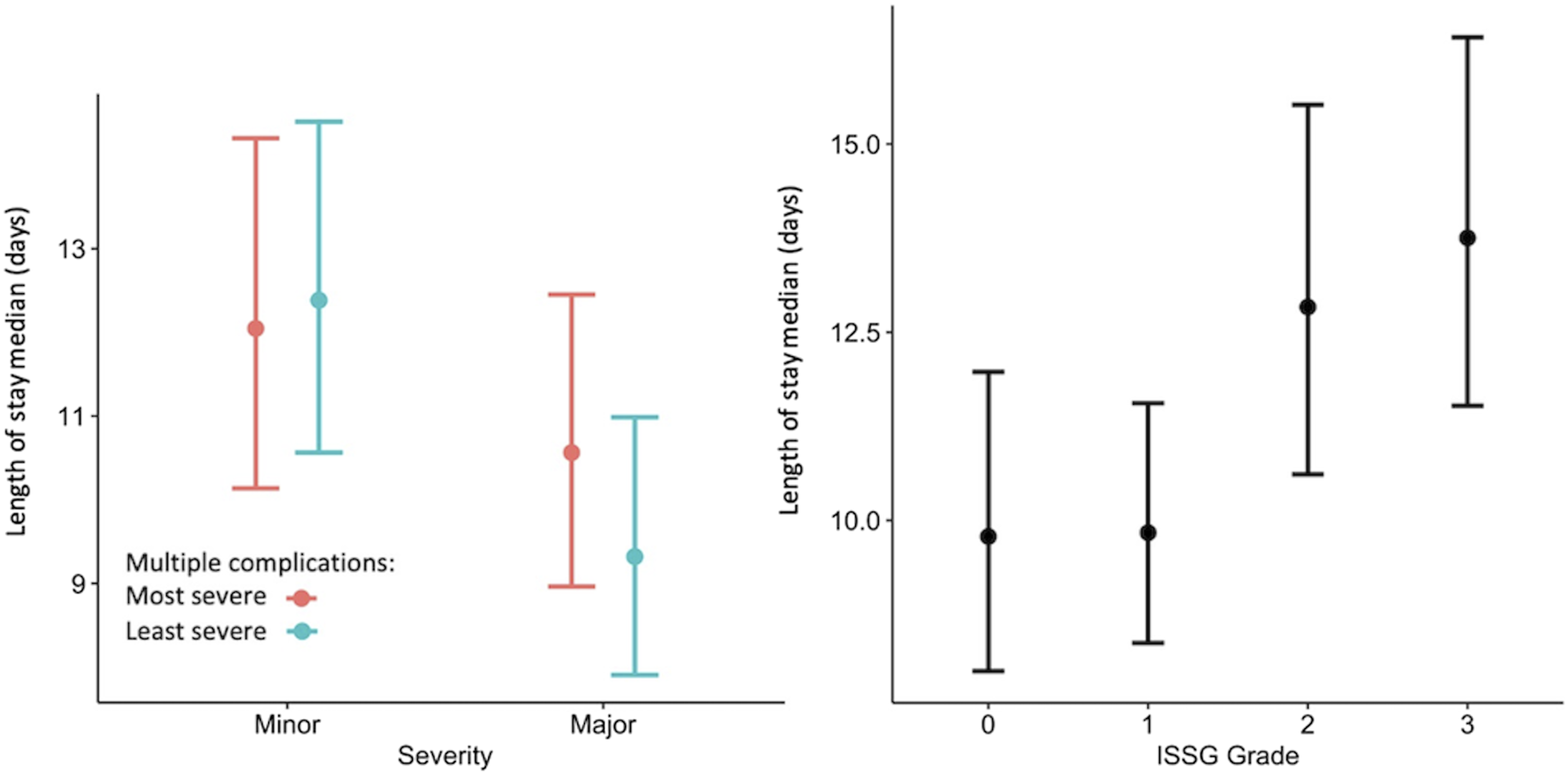
Pairwise Comparisons Between ISSG-AO Complication Grades and Association With Length of Stay.
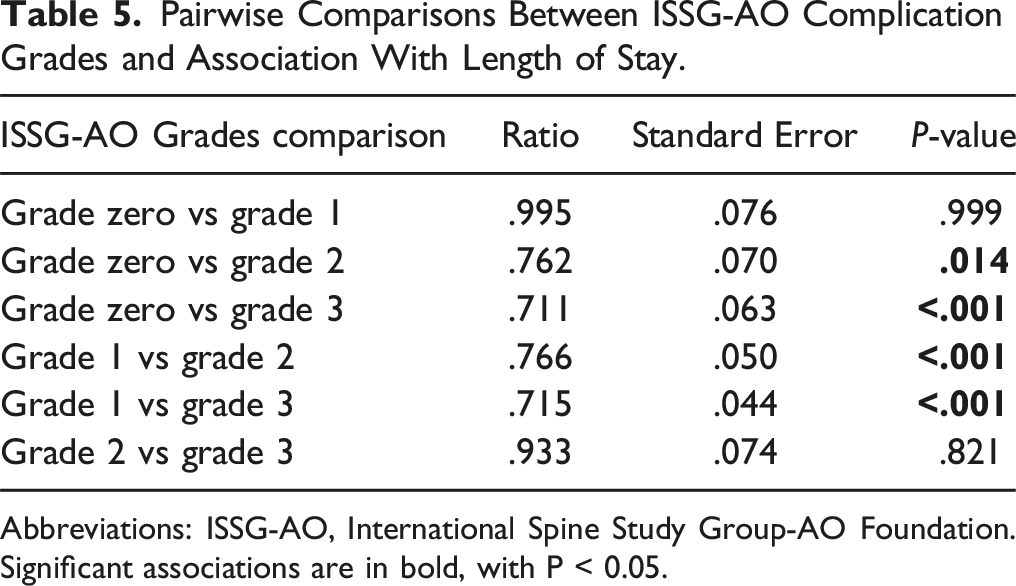
Abbreviations: ISSG-AO, International Spine Study Group-AO Foundation. Significant associations are in bold, with P < 0.05.
Discussion
The ISSG-AO ASD complications classification system was recently introduced to improve classification and understanding of postoperative complications specific to ASD patients. To assess the efficacy of the ISSG-AO classification system, we aimed to identify whether ISSG-AO complication intervention scoring correlates better with post-operative LOS as compared to the traditionally used major/minor complication classification system. Understanding associations with LOS is especially important, as increased LOS has been associated with higher readmission risk, 13 increased costs, 14 and diminished satisfaction15-18 among patients undergoing spinal surgery. We evaluated a large, multicenter cohort of 490 ASD patients sustaining in-hospital complications and classified the complications with both the ISSG-AO and major/minor systems. Multiple statistical approaches confirmed significant correlation between ISSG-AO complication severity classification and LOS, whereas the major/minor classification system showed an inverse relationship between complication severity and LOS.
Results of our study suggest that the ISSG-AO ASD complication intervention grading is a reliable means for identifying complications associated with prolonged LOS. This association was found to be independent of other factors, including staged surgery, patient frailty, and other comorbidities. Specifically, we found that the complication intervention sub-classification of the otherwise granular ISSG-AO classification system score strongly correlates with LOS, with grades 2 and 3 correlating most strongly with prolonged LOS in pairwise comparisons. Use of the complication intervention sub-classification may simplify evaluation of complications influencing LOS, especially as the ISSG-AO system’s 0-3 grading scale for complication intervention severity (Grade 0, none; Grade 1, mild; Grade 2, moderate; Grade 3, severe) is straightforward, with clear guidelines for each complication grade (Figure 1). 12 In addition, previous work has shown the ISSG-AO complication classification system to be highly repeatable, with good inter- and intra-rater reliability across varying levels of training, including those with and without surgical training. Indeed, overall intervention severity grading, or ability to correctly choose complication intervention severity grade, was 88.4% correct among all raters, including fellowship trained surgeons, residents/fellows, and research coordinators. 12 Furthermore, our results show that the widely used major/minor classification system cannot reliable correlate complication types with LOS, further supporting the need for an ASD-specific complications classification system. As such, the major/minor classification scheme appears to inadequately account for severity of complications and their implications as they relate to clinically meaningful outcomes such as LOS. For example, minor complications include cerebrospinal fluid leak and inadequate fixation, which may require additional procedures such as re-exploration or revision fixation. Such additional procedures may be expected to substantially prolong length of stay, and therefore may not be truly “minor” complications as they have meaningful implications for patients, payors, and other health care stakeholders.
To our knowledge, this is the first study to compare the correlation of the ISSG-AO ASD complications classification system grading to major/minor complication grading. We specifically chose to compare the ISSG-AO system to the major/minor system, as the major/minor system has been widely used for evaluating complications in ASD surgery. While our results show correlation between complication intervention severity and LOS, our study was not intended to provide a predictive model for LOS. Similarly, while previous studies have shown correlations between factors such as frailty and complications, 19 we were not specifically evaluating predictors of complications. Our results build on prior work by Le et al, who reported that increased ISSG-AO complication severity was significantly correlated with longer LOS among ASD patients. Similar to our study, Le et al found significant association between ISSG-AO complication grade and LOS after adjusting for multiple factors, including staged surgery and frailty. 20 In contrast, prior studies have not consistently correlated LOS and increased complication grade using alternative classification systems, such as the Clavien-Dindo (CD) grading system. 21 The CD system is similar to the ISSG-AO system in grading complications based on complication treatment intervention; however, the CD system was developed for in-hospital complications in general surgery rather than complications specific to ASD.20,22-24 Studies have also found no correlation between CD complication grading and LOS in patients undergoing surgery for cervical deformity, 24 further emphasizing the need for spine- and ASD-specific complication classification systems.
Disease-specific complication classification systems such as the ISSG-AO ASD system will likely play an increasingly important role in outcomes research with the aim of improving health care delivery. While the aim of the current study was validating the ISSG-AO ASD complications classification system and comparing the ISSG-AO system to the widely used major/minor system, it is important to note that other spine-specific complication classification systems have been validated, including the Spine Adverse Events Severity System (SAVES).25,26 Development and application of such systems is especially important as health care, and spine surgery in particular, faces increased pressure to improve costs, quality, and outcomes. 27 With our study, we have shown that ISSG-AO complication grading correlates strongly with LOS. Widespread implementation of accurate, disease specific complication classification systems such as the ISSG-AO system may facilitate communication between health care stakeholders and ultimately improve our understanding of complication risk factors and their consequences, including prolonged LOS. In turn, improved understanding of complications may help surgeons identify patients at risk for complications and diminished outcomes, improve preoperative patient selection and counseling, set appropriate expectations and surgical goals, including extent of surgery, and mitigate risks for poor outcomes by pursuing appropriate preoperative patient optimization. 28
This study was limited by its retrospective design, lack of a control group, and lack of a standardized discharge protocol among included centers. We also do not have data on the proportion of patients reported to the database from each center. We evaluated patients who underwent surgery between 2008 and 2020, and our data may be subject to changes in practices and protocols over time. In turn, this may limit generalizability of our results. We were also unable to include long-term outcomes or cost data. We did not account for time between procedures for staged surgery; however, we assessed and accounted for surgical approach including combined anterior-posterior approach, which may serve as a surrogate for staged surgery. Furthermore, while Klineberg et al found a high degree of complication intervention severity grading accuracy with the ISSG-AO system,
12
we were unable to assess the accuracy or reliability of data submitted from participating centers, or the accuracy of the complication intervention grading within our dataset. Despite these limitations, this is the first study to specifically compare the traditionally used major/minor complications classification system to the ASD-specific ISSG-AO complications classification system. We analyzed data from many patients and surgeons across 19 sites
Conclusion
Our findings demonstrate that the ISSG-AO ASD complications classification intervention severity grading correlates strongly with increased LOS, whereas the traditionally used major/minor classification system had an inverse correlation with complication severity and LOS. Widespread implementation of the ISSG-AO ASD complication classification system may help spine surgeons better understand complications, their risk factors, and clinical implications, ultimately helping surgeons mitigate complications and improve the overall value of ASD care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.