
Abstract
Study design
An ambispective, observational study of the prospective, institutional adult spine deformity (ASD) database.
Objectives
The study investigates the clinical and radiographic fusion rates with lateral interbody approach and rhBMP-2 in multiple-level lumbar fusion in the ASD population. Previous studies have reported over 10% pseudoarthrosis rate with multiple segment fusions. Lateral lumbar interbody fusion (LLIF) allows multiple-level, less-invasive access to the anterior lumbar spine. We hypothesized that fusion rates with lateral approach with rhBMP-2 use are superior to the published data on lumbar fusion in ASD patients.
Methods
The institutional ASD database was searched to identify eligible patients with two or more levels of LLIF (T12-L5), >4 levels of posterior instrumentations and >2 years of follow-up between the years 2010 and 2018. Antero-posterior and lateral 36-inch standing radiographs for each patient and computed tomography scans in select patients were studied to ascertain fusion status and patients were divided into two groups based on fusion status.
Results
The study included 179 patients with a mean age of 65.3 years and 74% female patients. The median number of interbody fusions was performed at 3 (IQR 3-4) levels. The mean follow-up duration was 4.4 years (SD = 1.9). 169 patients (94.5%) had successful arthrodesis, while 10 patients (5.5%) had radiological pseudoarthrosis at one level. Of the 10 patients, 8 (4.4%) were either clinically asymptomatic or had manageable back pain. Two patients (1.1%) required revision surgery for symptomatic pseudoarthrosis.
Conclusion
This is the largest known series of ASD patients investigating the fusion rates with multiple-level LLIFs. LLIF along with rhBMP-2 can achieve high fusion success across interbody fusion levels in multi-segmental ASD surgeries.
Keywords
Introduction
Spinal fusion for degenerative spinal conditions has been shown to improve health-related quality of life. 1 With the advent of improved spinal instrumentation and interbody devices, fusion rates have improved, but the optimal choice for graft material remains unclear. Iliac crest autologous bone graft (ICBG) is considered the gold-standard graft material, defined during the era of posterior-alone fusions. 1 However, concerns related to donor-site morbidity increased blood loss and operative time, and limited graft quantity compelled physicians to explore alternatives to the ICBG. 2 Since the U.S Food and Drug Administration approved rhBMP-2 for single-level ALIFs in 2002, 3 rhBMP-2 has been used as an alternative to ICBG and, as a result, its use in spinal surgery has increased substantially. Reported fusion rates with rhBMP-2 are equivalent to ICBG (94.1% with rhBMP-2 vs 89.5% with ICBG) in single-level transforaminal lumbar interbody fusion (TLIF) or posterior lumbar interbody fusion (PLIF) 4 and posterolateral lumbar fusions (PLF). 5 While the initial study recommended 20 mg rhBMP-2 use per level, 3 dosing recommendations remain inconsistent throughout the literature. Alternative biologic agents (e.g., Silicate calcium phosphate, allogenic morphogenic protein) have demonstrated modest success in comparison to the rhBMP-2.6,7,9
Superior fusions with rhBMP-2 were initially reported in short-segment constructs, but the fusion rate varies with the surgical approach and the choice of bone-graft material. 8 The addition of interbody spacers has increased the fusion success (89.5%-91%) as compared to posterior-alone fusion.4,7 Similarly, the fusion rates with ALIFs and rhBMP-2 are higher than with TLIF or PLIF procedure and rhBMP-2 (97.8% with ALIF vs 95.7% with TLIF or PLIF vs 93.6% with PLF). 8 In contrast to the short-segment constructs, fusion rates are reportedly lower in the long segment fusion constructs performed in adult spinal deformity (ASD) surgery; initial studies reported 85-90% fusion rates with PLF.10-12 Kim et al 13 reported an 83% fusion rate with PLF in the ASD population, utilizing local autogenous bone graft. 13 There is growing evidence to suggest that rhBMP-2 increases the fusion rate in PLF for ASD surgeries. A recent study reported a 95% arthrodesis rate with rhBMP-2 as compared to 72% with ICBG. 14
In recent years, lateral lumbar interbody fusion (LLIF) has been increasingly performed in ASD surgeries; potential benefits described are improved indirect decompression, higher segmental lordosis correction and improved sagittal alignment.15,16 Furthermore, multiple LLIFs may be a less-morbid alternative to formal osteotomy procedures for sagittal balance correction. 17 To the best of our knowledge, the arthrodesis rate utilizing rhBMP-2 and multiple-level LLIF in ASD surgeries has not been accurately described. The primary objective of our study was to report on the clinical and radiographic interbody fusion rate with multiple level LLIF using rhBMP-2 in ASD surgeries.
Methods
Study Design
An ambispective observation review of the institutional, prospective ASD database was conducted to identify patients treated for degenerative spinal deformity. Patients treated with two or more levels of LLIFs (between T12-L5 motion segments), >4 levels of posterior instrumentation and a minimum 2-year follow-up were included. Patients with stand-alone cages, single-level interbody fusion, smaller constructs (<4 levels), revision interbody fusion and inadequate follow-ups were excluded from the study. Data were extracted from hospital charts and diagnostic images of patients operated on between 2010-and 2018. A consent was completed before the procedure and Institutional review board approval was obtained before the start of the study. Patients were operated on in a lateral position using a lateral, retroperitoneal ante-psoas or trans-psoas approach. Multiple level LLIFs procedures were performed, and all patients were staged for posterior instrumentation within a week. Most patients also had L5-S1 interbody fusion and either ALIF or TLIF was performed at this level. rhBMP-2 was the only biologic agent used for interbody fusion and was strictly used within the interbody spacer devices; rhBMP-2 was not used in the posterolateral gutters to achieve PLF in primary surgeries. A low dose (3-4 mg) of rhBMP-2 was used at each LLIF level. A larger cantilever force due to long segment fusion alters the biomechanics and fusion success at the lumbosacral junction. Hence, pseudarthrosis at the L5-S1 level was not counted as an event in this analysis.
Radiographic Evaluation
Plain coronal and sagittal 36-inch standing radiographs were obtained pre-procedure and during follow-up. Computed tomography (CT) scans were obtained in select patients with suspicion of pseudoarthrosis or implant-related complications. Moreover, abdominal, and pelvic CT scans obtained for unrelated conditions during the follow-up period were available for review in several patients. All imaging studies obtained within the province of Alberta were available for review, ensuring high imaging capture rates. The upper instrumented vertebra (UIV) was categorized into three groups: upper thoracic (T1-T9), lower thoracic (T10-T12) and upper lumbar (L1-L3). Similarly, the lower instrumented vertebra (LIV) was categorized into three groups: lower lumbar (L4-6), sacrum (S1) and pelvis (Ilium). Coronal and sagittal alignment parameters [Coronal cobb angles, lumbar lordosis (LL), thoracic kyphosis (TK), sagittal vertical axis (SVA), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), PI-LL mismatch] were recorded on pre-and postoperative radiographs. Post-operative changes in alignment parameters were analyzed separately to measure the difference between the groups.
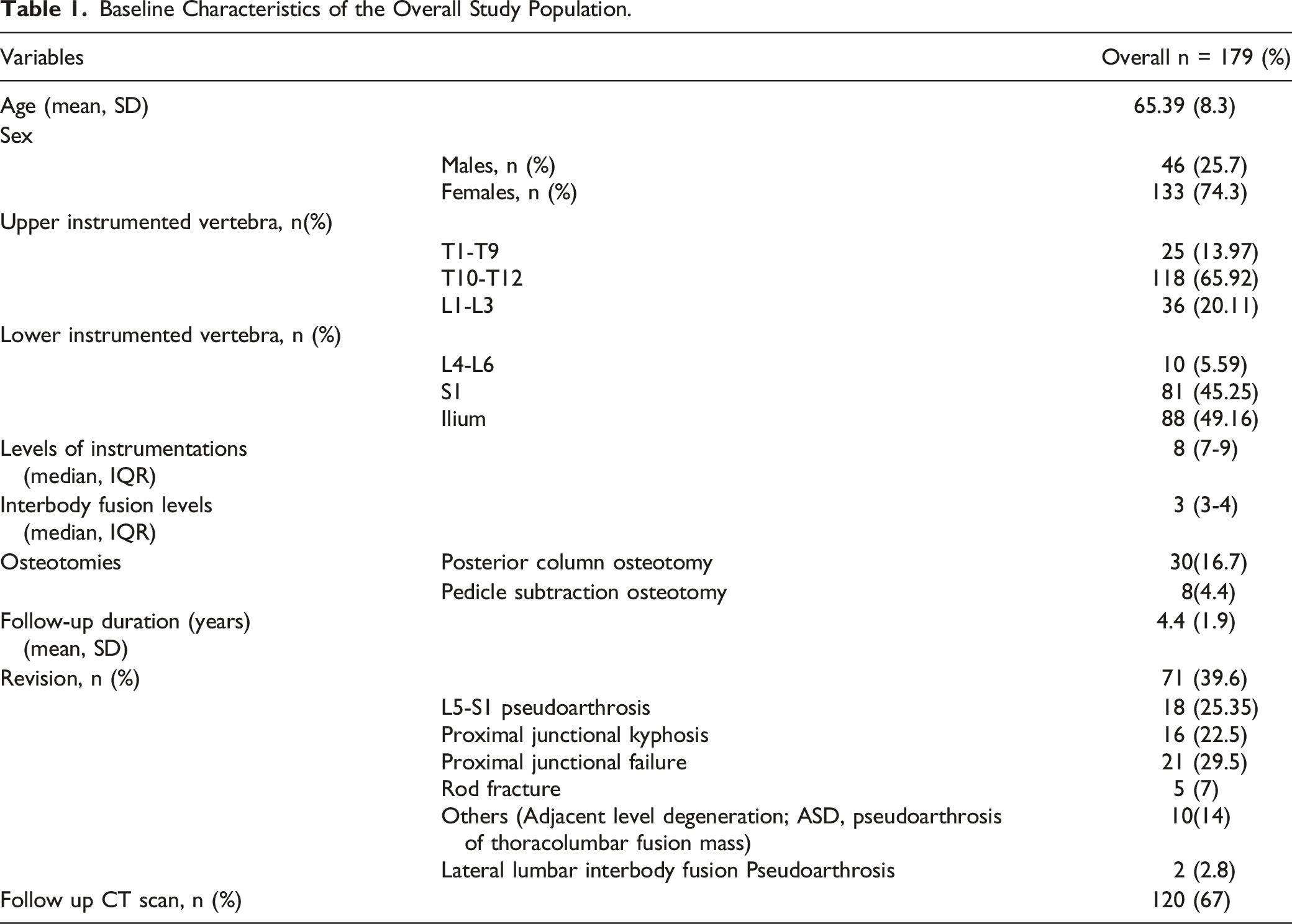
Baseline Characteristics of the Overall Study Population.
Radiographic findings suggesting pseudoarthrosis: 1. Inadequate consolidation of the disc space without bridging trabecular bone at the margins of the spacer or failure of graft incorporation into the vertebral endplates.18,19 2. Loss of fixation such as implant fracture, or a lucent halo around pedicle screws 3. Progression of radiographic deformity. 4. Progressive spacer device subsidence and spacer migration.
13
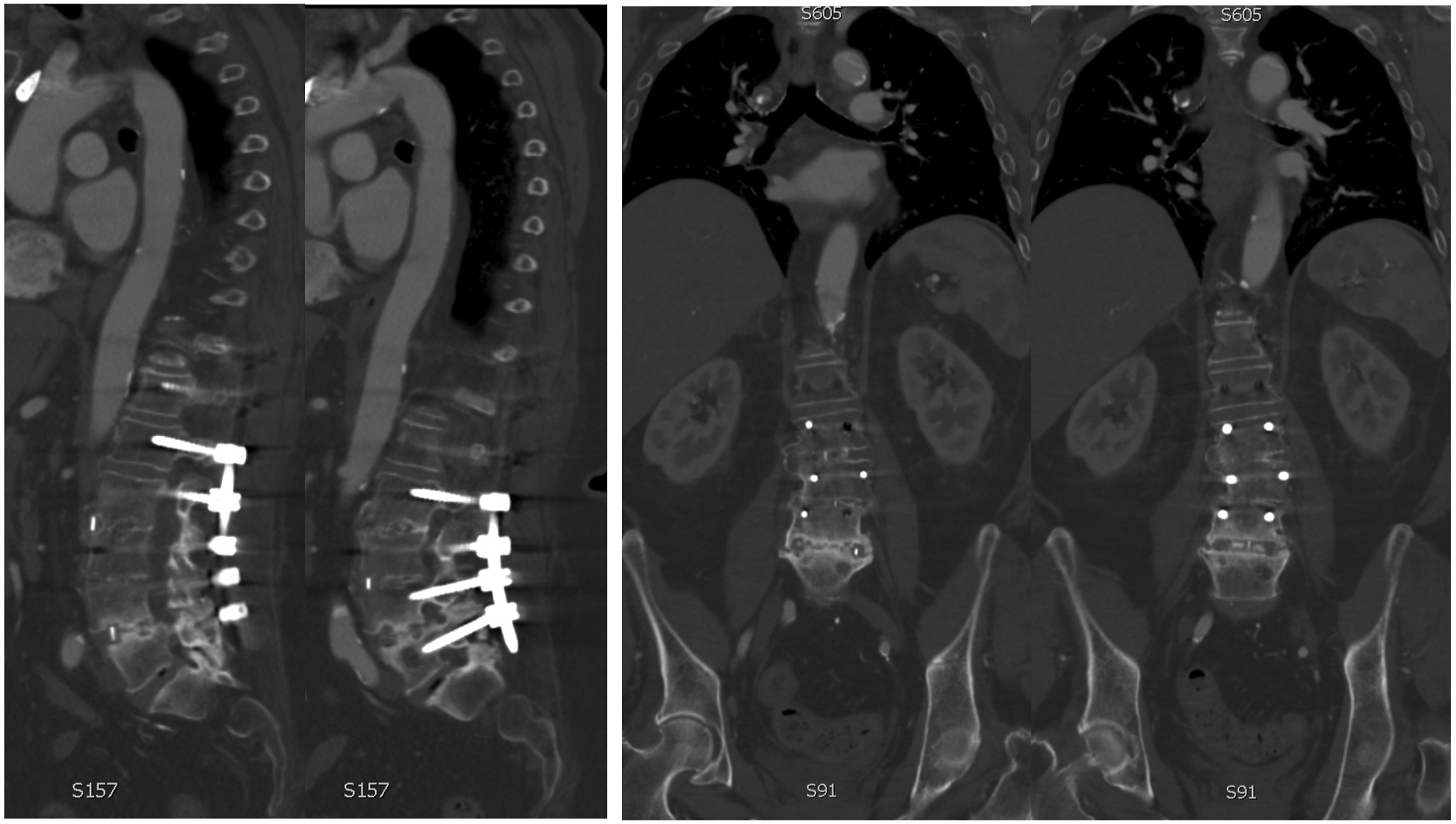
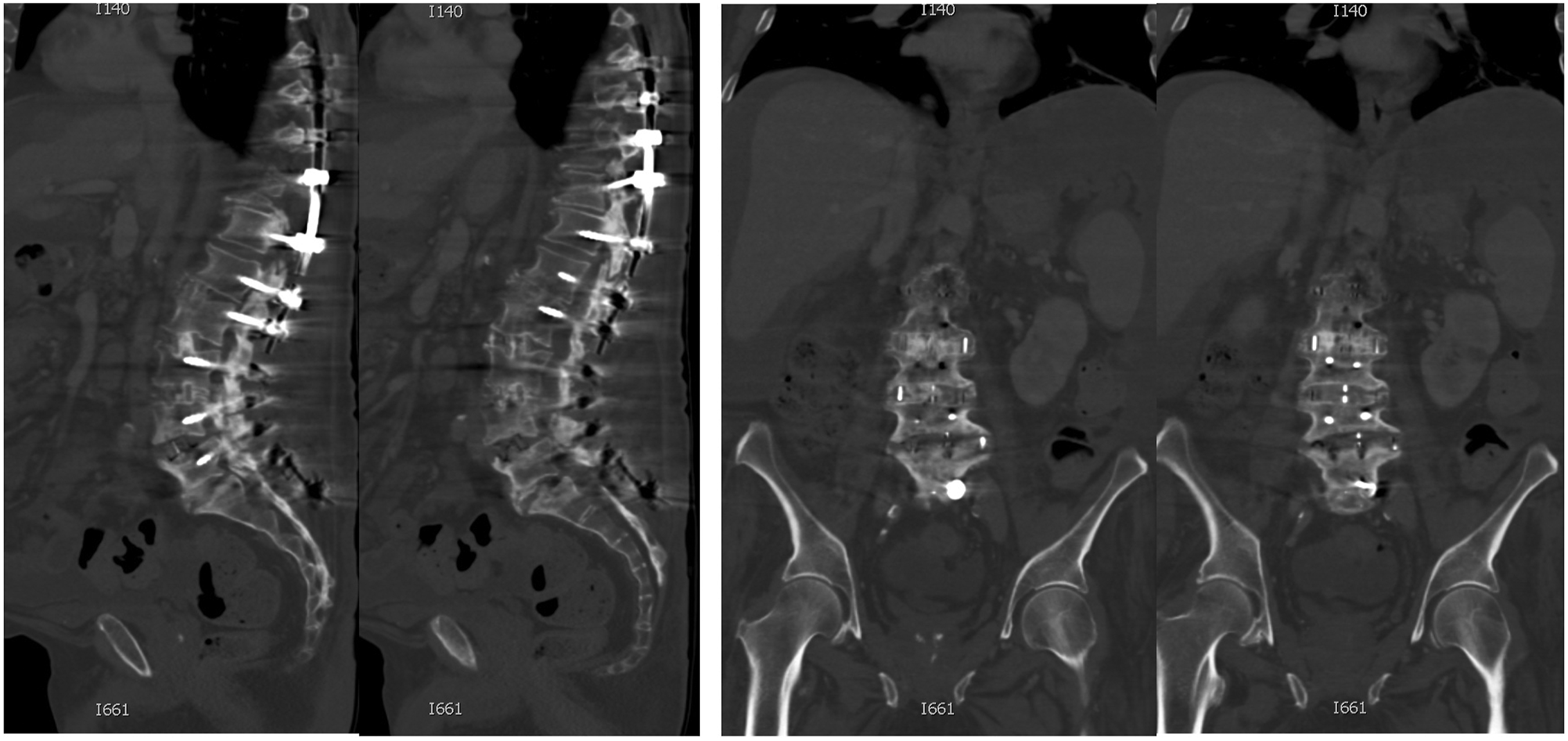
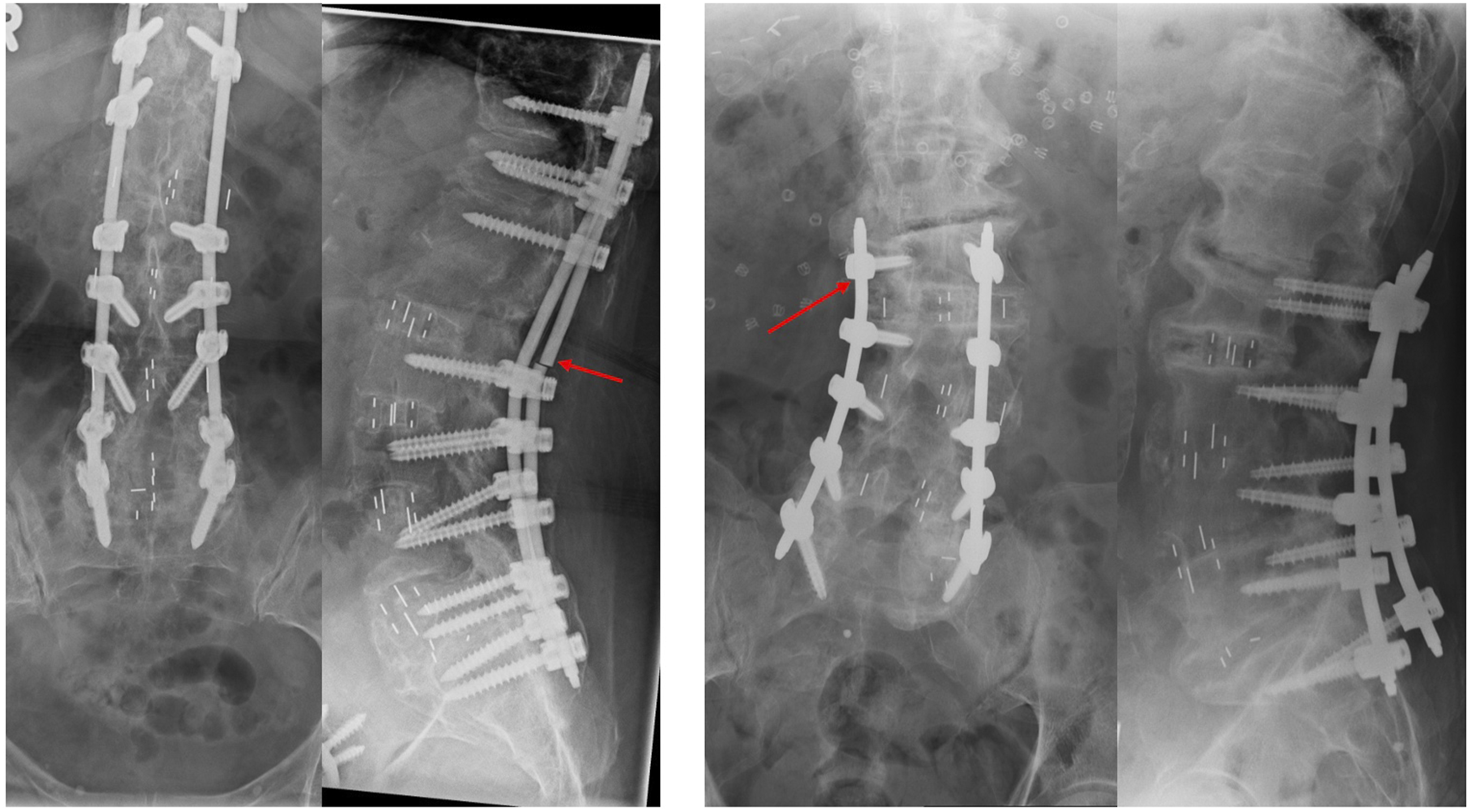
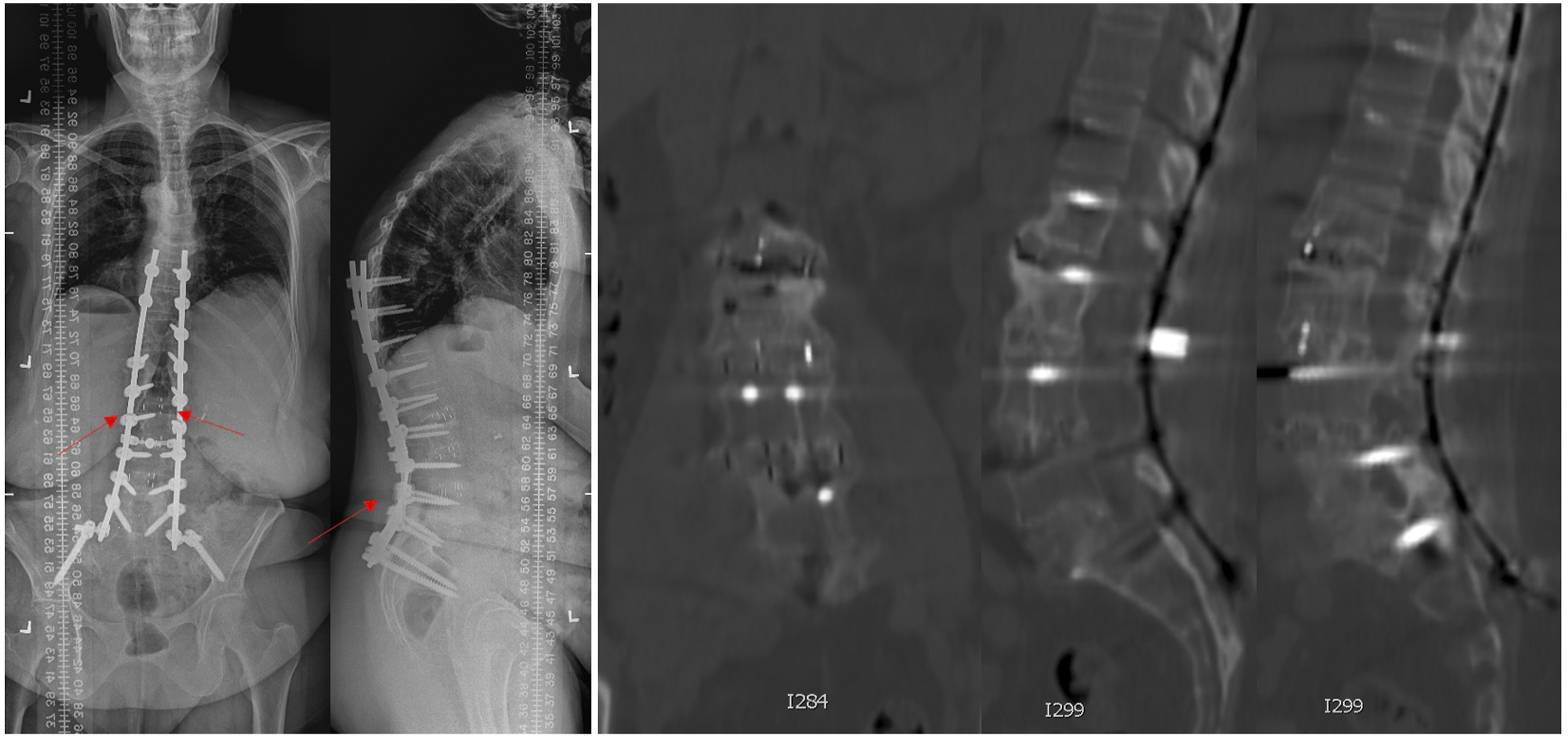
CT findings: 1. Absence of bone trabeculations across fusion levels 2. Bone lucency at graft-vertebral body junction. 3. Halo around pedicle screws or rod fractures, 4. Progressive spacer migration (rotation or translation)20-22(Figures 1-3) (Patient 5): 71 years female treated with L2-5 LLIF and T11-L5 posterior instrumentation. Sagittal computed tomography images (left) show inadequate consolidation and fragmented interbody fusion mass at the L4-5 level. Coronal images (right) also show an absence of bridging trabeculations across disc space. The patient was, however, asymptomatic at the final follow-up. (Table 3). (Patient 8): 72 years male underwent L1-5 LLIF and T10-S1 posterior instrumentation. A Follow-up computed tomography image obtained for workup of colorectal carcinoma 4 years after the surgery shows similar findings of inadequate bridging trabeculations across disc space and fragmented fusion mass at the L4-5 level. Bridging bone trabeculation can be noted at the adjacent L2-3 and L3-4 levels. (Patient 6): 72 years female underwent L1-5 LLIF and T10-S1 posterior instrumentation (left). Radiographs obtained at 3 years follow-up shows right rod fracture at L1-2 level (arrow). Although adequate consolidation across the disc space could be observed, findings were suspicious for radiological pseudoarthrosis. Significant subsidence was noted at the L4-5 level resulting in several foraminal narrowing and radiculopathy. 72 years Male (Patient 7) was treated with L2-5 LLIF and L2-S1 posterior instrumentation (right). Radiographs obtained 3 years after surgery demonstrate lucency in the anterior disc space at the L2-3 level and halo around the left L2 screw (arrow). The patient also had adjacent segment degeneration of L1-2 disc-space.
Statistical Analysis
Baseline characteristics and imaging features for the overall population were reported using descriptive statistics. Cases were binarized into fused vs pseudarthrosis. Differences in baseline characteristics of patients with successful fusion vs pseudarthrosis were assessed with Fisher’s exact test (categorical variables) and Wilcoxon rank-sum test (continuous variables). Two-sided P < .05 was considered statistically significant. Statistical analysis was performed with Stata/MP 16.1 (StataCorp LP).
Results
Demographic Data
Records of 345 patients were available in the institutional ASD database, and 179 eligible patients were identified after applying inclusion criteria (112 patients had either single-level LLIF, stand-alone LLIF or <4 levels of posterior instrumentation; 26 patients did not complete 2-year follow-up and follow-up imaging studies were not available for review in 28 patients and hence, these patients were excluded from the analysis) with complete 2-year follow-up. LLIF was performed at 637 levels. The mean patient age was 65.3 (SD 8.3) years; 74% of patients were females (46 males; 133 females). (Table 1)
Patient Characteristics
UIV was upper thoracic, the lower thoracic and upper lumbar vertebra in 25(14%), 118 (66%) and 36 (20%) patients respectively. LIV was L4-L6, sacrum and pelvis in 10 (5.5%), 81 (45.5%) and 88 (50%) patients respectively. The median length of instrumentation was 8 levels (IQR 7-9). Median interbody fusions were performed at 3 levels (IQR 3-4). The mean follow-up duration was 4.4 years (SD = 1.9). Osteotomies were employed in 38 (21%) patients; 30 (16.7%) patients had posterior column osteotomies (PCOs), and 8 (4.4%) patients had single-level pedicle subtraction osteotomy (PSO). Revision surgery was performed in 71 patients (39.6%); the cause of reoperation was proximal junctional kyphosis (PJK) in 16 (22.5%), proximal junctional fracture (PJF) in 21 (29.5%), rod fracture (other than LLIF-level) in 5 (7%), L5-S1 pseudoarthrosis in 18 (25.5%), thoracolumbar pseudoarthrosis in 3 (4.2%) and clinically significant pseudoarthrosis at LLIF-level in 2 (2.8%) patient.120 patients (67%) had postoperative CTs available for review during follow-up (Table 1). Of the 18 (25.5%) patients who were reoperated for L5-S1 pseudoarthrosis, 14 (78%) were without sacropelvic fixation and 17 (95%) had TLIF procedure at the L5-S1 level.
Group Characteristics
Baseline characteristics were similar in both fused and pseudoarthrosis groups. Three of the ten patients (33%) were obese (BMI>30) and 4/10 (40%) were smokers in the pseudoarthrosis group (Table 4). Both groups were similar in the number of interbody fusion levels (median = 3; IQR 3-4) and length of instrumentation (median = 8; IQR 7-9). All patients treated with osteotomies (n = 38) were in the fused group. Mean follow-up duration was not significantly different between the two groups (fused=4.4 years, pseudoarthrosis = 5 years; P = .266).
Comparison of the Variables Between Fused and Pseudoarthrosis Group.
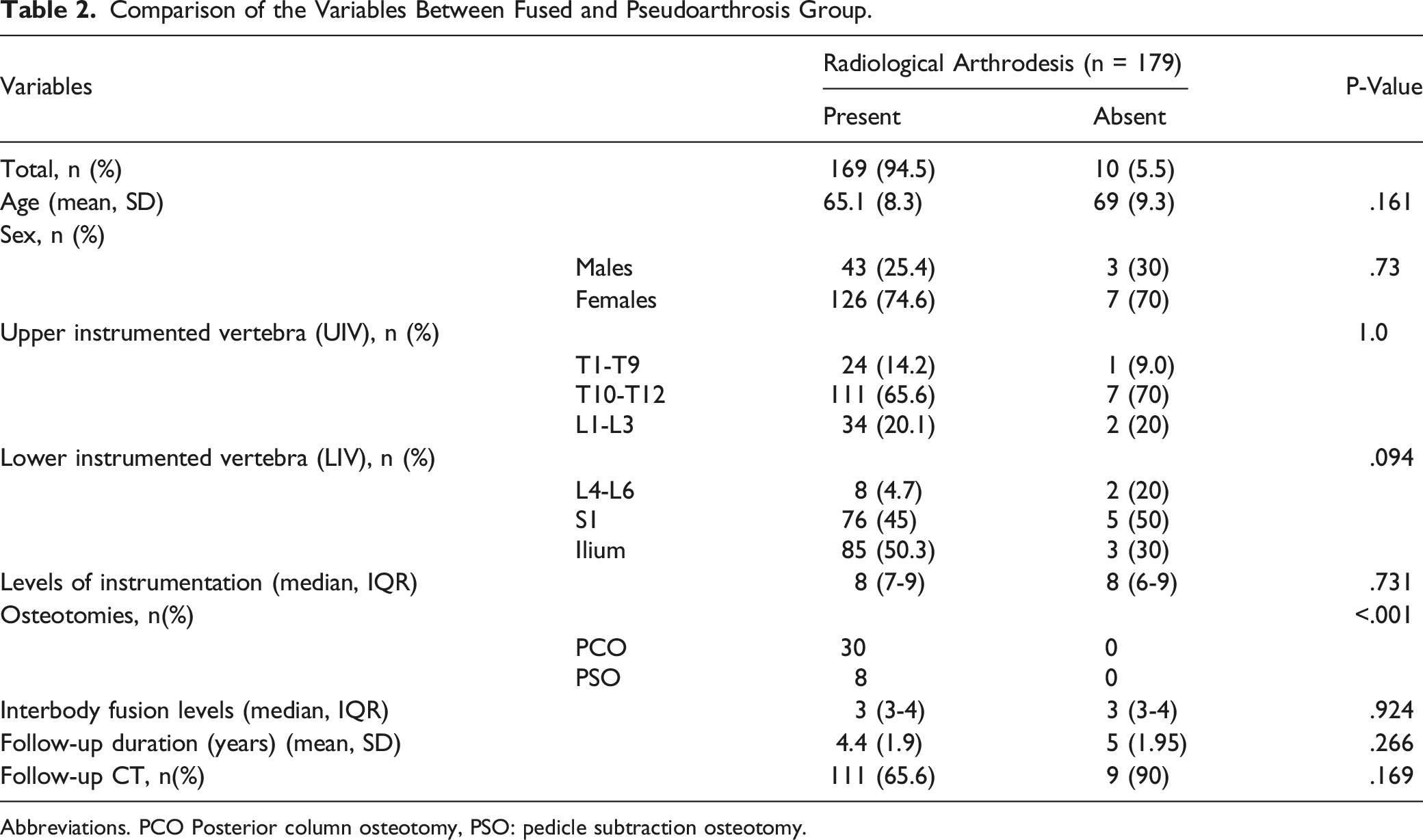
Abbreviations. PCO Posterior column osteotomy, PSO: pedicle subtraction osteotomy.
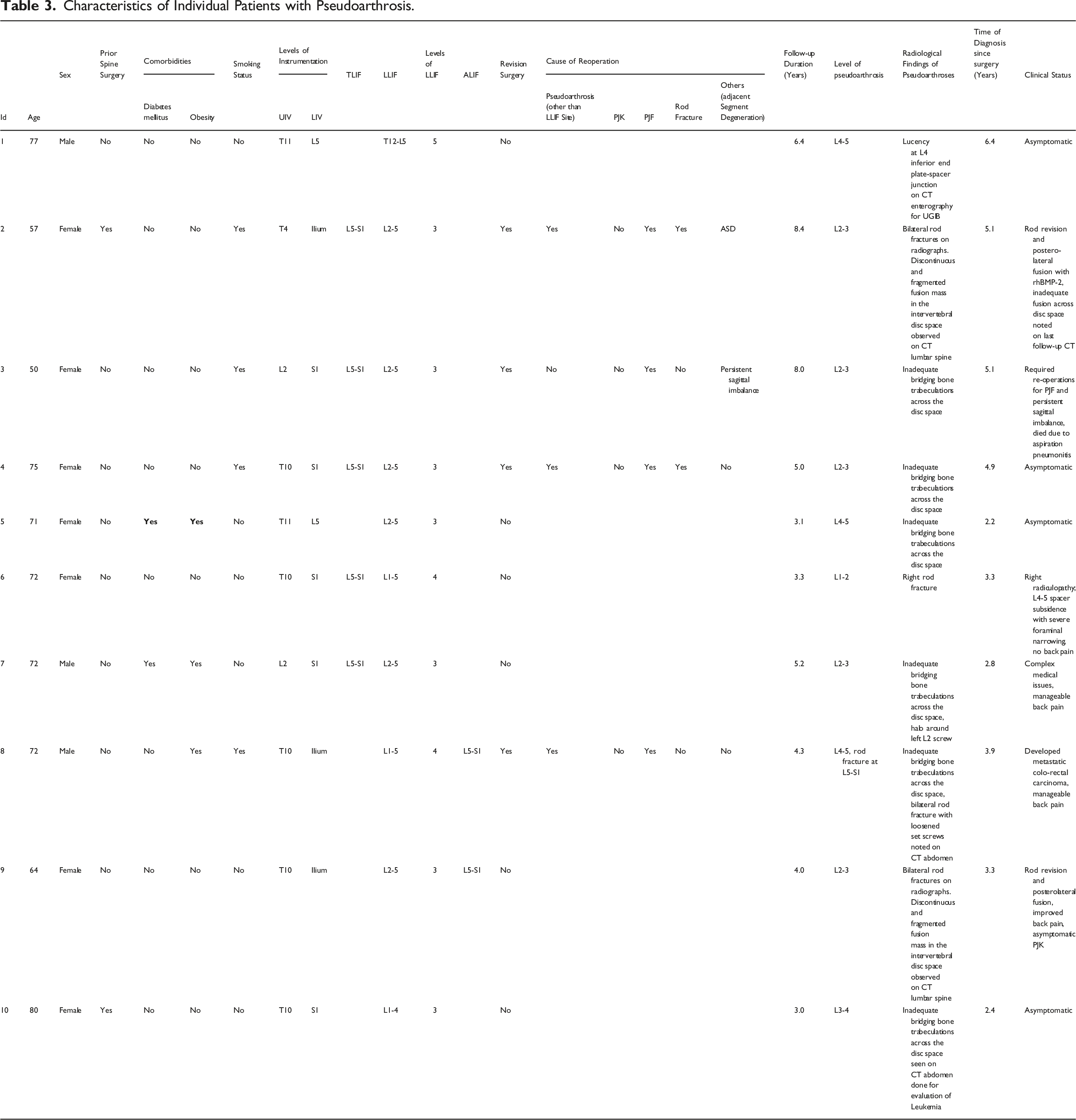
Characteristics of Individual Patients with Pseudoarthrosis.

(Patient 9): 64 years female with degenerative lumbar scoliosis (Pre-op coronal cobb:29, LL: 29, SS: 29, PI-LL mismatch: 31, SVA:84, PT:34) underwent L2-5 LLIF, L5-S1 ALIF and T10-Pelvis posterior instrumentation. Post-operative images (right) show restoration of lumbar lordosis and good correction of the sagittal alignment. The patient has mild persistent coronal imbalance to the right.
(Patient 9 continued): The patient presented with progressive mechanical back pain and follow-up radiographs demonstrated bilateral rod fractures (arrows)at the L2-3 level. (Post-op coronal cobb:9, LL: 54, SS: 35, PI-LL mismatch: 10, SVA:43, PT:32). Computed tomography images show lucency in the disc space and at the spacer-end plate junction (right). The patient underwent re-operation with rod exchange and postero-lateral fusion using rhBMP-2.
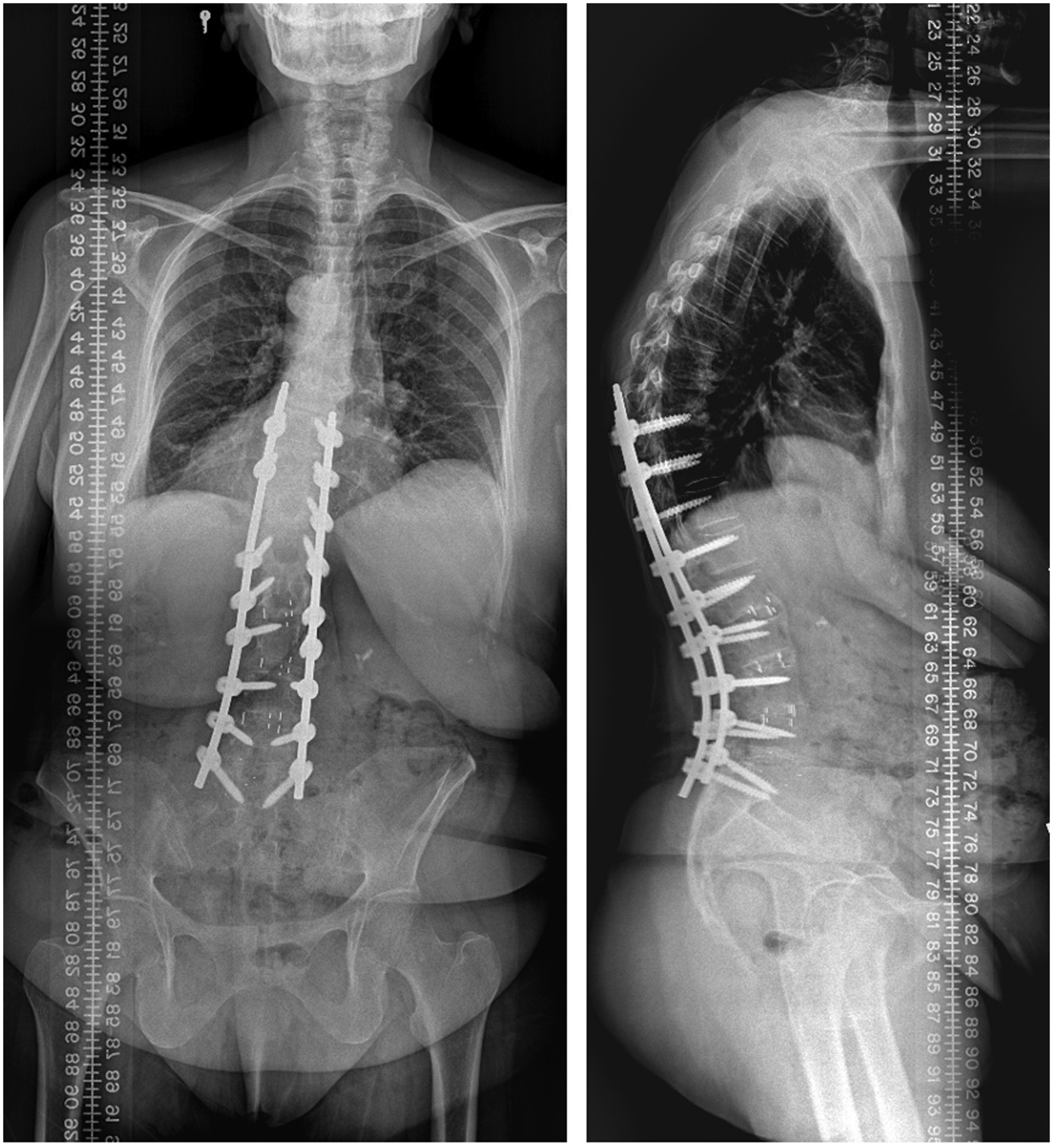
(Patient 9 continued): post-operative images obtained at 1-year follow-up after reoperation. The patient had excellent improvement in back pain symptoms. However, she persists to have asymptomatic proximal junctional kyphosis.
Radiographic Alignment Parameters
Comparison of Pre-Operative and Post-Operative Alignment Measures for the Overall Study.
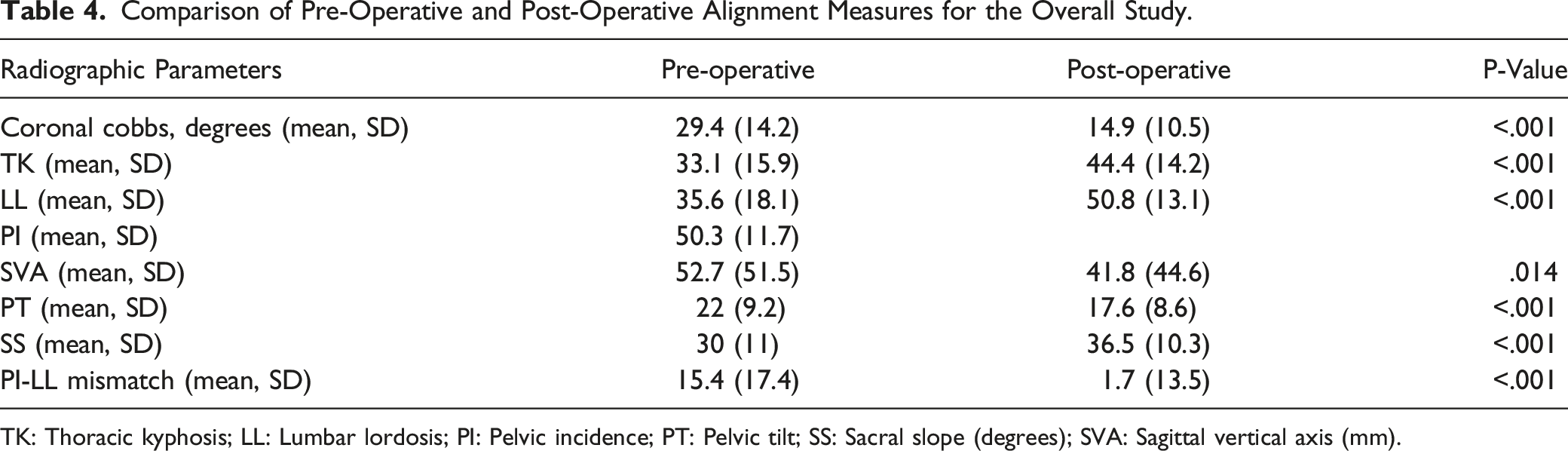
TK: Thoracic kyphosis; LL: Lumbar lordosis; PI: Pelvic incidence; PT: Pelvic tilt; SS: Sacral slope (degrees); SVA: Sagittal vertical axis (mm).
Comparison of Pre-Operative and Post-Operative Measurement Between Fused and Pseudoarthrosis Group.
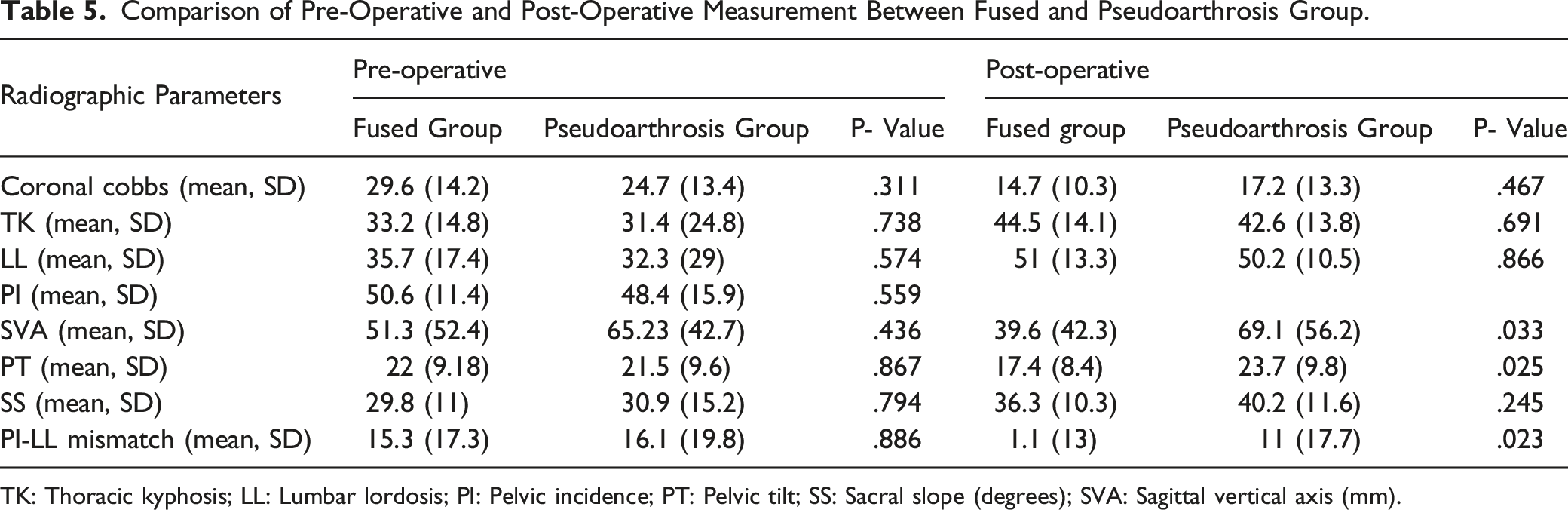
TK: Thoracic kyphosis; LL: Lumbar lordosis; PI: Pelvic incidence; PT: Pelvic tilt; SS: Sacral slope (degrees); SVA: Sagittal vertical axis (mm).
Discussion
Results from our study found a 94.5% arthrodesis rate for lateral lumbar interbody fusion (T12-L5) in the ASD cohort treated with multiple segment instrumentation. While 10 (5.5%) patients had radiological evidence of pseudoarthrosis, only two (1.1%) patients were significantly symptomatic requiring reoperation. Patients in the fused group achieved superior correction of SVA and PT and had lower PI-LL mismatch. Our results demonstrate that arthrodesis rates with multiple-level LLIF and rhBMP-2 in ASD are comparable to the previous studies of single-level LLIF. Retrospective reviews from prior studies have reported a 94%-96% arthrodesis rate with single level LLIF.23,15
Several authors have compared lumbar arthrodesis rates between rhBMP-2 and ICBG in prior studies.24,25 A recently published randomized control trial investigated the effect of rhBMP-2 in single-level PLIF procedure. 26 Forty patients were randomized in each group (rhBMP-2 and autograft) and patients achieved 100% arthrodesis in both the groups at 1-year follow-up. However, the authors noted a slower rate of trabecular bone formation and lower interbody fusion-mass density in the BMP group during the first year of surgery. 26 Multiple segment spinal fusion in ASD surgeries more frequently develops pseudoarthroses. Kim et al 13 reported 17% (39/232) pseudarthrosis in their series of spinal deformity patients treated with multiple segment instrumentation and autologous bone-grafting. 13 50% of the pseudarthroses observed in their study occurred at the junctional region (seven at thoraco-lumbar, eighteen at the lumbosacral region). In contrast, we encountered 21 (11.7%) symptomatic pseudarthroses at junctional levels in our series which required re-operation. Given the higher reported rates of lumbosacral pseudoarthrosis in comparison to the other levels of the lumbar spine, L5-S1 fusions were omitted from the primary analysis.27-30 Recently, Soroceanu et al 31 described an 11.4% incidence of radiological pseudarthrosis in an ASD cohort, although the levels of pseudarthroses, the use of LLIFs and reoperation rates were not defined. 31 How et al, in a recently published meta-analysis of 25 studies, reported a 6.3% combined revision rate for pseudoarthrosis in ASD patients. 32 The radiological pseudoarthrosis at the interbody fusion level in our study was 5.5% and clinically significant pseudoarthrosis requiring re-operation was even lower (1.1%). The use of rhBMP-2 is associated with the high direct cost of the index procedure. However, rhBMP-2 is cost-effective in ASD surgeries in preventing pseudoarthrosis and re-operation. 33 The mean 2-year direct cost for patients with pseudarthrosis ($138,000$ ± 17 000) was significantly higher than that of patients who did not develop pseudarthrosis ($61,000 ± $25,000). 34
CT scans and radiographs are the most commonly employed imaging studies to assess fusion status.35,36 Plain radiographs exhibit 89% sensitivity and 60% specificity for predicting solid arthrodesis in patients following PLFs. 37 Likewise, the sensitivity of CT scan to determine fusion status ranges from 70 to 90% and specificity ranges from 28 to 85% in patients with interbody fusion using metallic cages. 38 Peters et al, in a meta-analysis on assessment of fusion criteria, 39 demonstrated that CT-scan possessed the highest discriminant ability as against intra-operative exploration. Chun et al 40 performed a similar, yet a less-comprehensive review of imaging data and suggested that CT-scan has the highest sensitivity and specificity (53-63% and 86% respectively) among the imaging studies for the determination of arthrodesis. 40 While surgical exploration has historically been considered the ‘gold standard for the diagnosis of pseudoarthrosis 19 in the PLF-era, it is not a practical alternative to confirm the diagnosis.
Due to the higher radiation exposure with CT scans, multiple studies for long-term follow-ups are not warranted on asymptomatic individuals. Radiographs are cheaper, easily accessible and pose lesser radiation exposure. We relied on a composite radiographic criterion derived from the literature to determine fusion status in our patients. Assessment of arthrodesis solely based on radiographic findings might have overestimated the arthrodesis rates in our cohort as 35% of patients in the fused group did not have a follow-up CT scan. However, these patients did not exhibit clinical or radiographic suspicion during follow-ups to merit CT imaging. Meanwhile, we had access to the lumbar spine CT images of several patients obtained for unrelated conditions. Imaging studies of each patient within the province could be accessed with a high capture rate using the unique patient identifier. We feel that such a captive population allows for high follow-up rates and a higher precision estimate of the true arthrodesis rate.
The mean time from index surgery to pseudoarthrosis detection in our study was 4.1 years (range 2.2-6.4) (Table 4). The mean follow-up duration for both study groups is over 4 years and the length of follow-up is reasonable to detect most of the pseudarthroses, although seven years of follow-up has been recommended in literature. 41 Nevertheless, 8 patients (4.4%) with asymptomatic pseudoarthroses could become symptomatic in the longer term or these unfused segments with the potential fibrous union and radiologically demonstrable pseudoarthrosis could subsequently ossify into a stiff segment. A similar observation was made by Jung et al 41 in their study of 152 patients treated with single or two-level LLIF which reported a pseudarthrosis rate of 27.6% (42/152) at 1-year follow-up, which decreased to 12.5% (19/152) at 2-year follow-up. Fourteen of these patients had asymptomatic, radiological pseudoarthrosis and 5 (3.2%) were symptomatic requiring re-operation. These authors also described multiple-level LLIFs, diabetes and smoking status as independent risk factors for pseudoarthrosis development. 41 Five patients in the pseudoarthrosis group had posterolateral fusion despite the features of pseudoarthrosis at the interbody fusion level. This finding might explain the asymptomatic status of these patients and underlines the importance of meticulous PLF to supplement anterior interbody fusion.
Our strict definition of pseudoarthrosis identifiable at the interbody fusion levels could have resulted in a lower estimation of the pseudoarthrosis rate. We did observe five-rod fractures (2.42%) and junctional pseudoarthrosis but these rates are lower than that described in the literature. 27 Other limitations of the study were retrospective design, and lack of a control group to compare fusion rates with a fewer level of fusion or alternative biologics as described in the literature.36,42 The study results were focused on the radiological findings and failed to describe clinical outcome scores after the procedure. Radiological and implant-related complications poorly affect the HRQOL outcome scores, 31 and careful analyses of clinical outcomes would have helped to establish the impact of successful arthrodesis on quality of life. Lastly, the radiological criteria used in the study have not been validated to confirm pseudoarthrosis and CT images were available only for the two-thirds of the study cohort, which might have overestimated the true arthrodesis rate.
Despite these limitations, this study has notable strengths. It is the largest known series of ASD patients treated with multiple-level LLIFs. By limiting our definition to interbody fusion level, we have provided concise reporting of pseudoarthrosis at the lateral lumbar interbody fusion levels between the L1-L5 motion segment. Patients were followed prospectively with high image capture rates. The higher arthrodesis rate in our study could be attributed to the better disc space preparation and larger fusion surface provided by the lateral approach and rhBMP-2. A prospective study utilizing CT scans for evaluation of arthrodesis across fusion levels and longer follow-up data would be required to provide a precise estimate of the lumbar pseudoarthrosis rate.
Conclusion
LLIF along with rhBMP-2 can achieve high fusion rates in multi-segmental ASD surgeries. The pseudoarthrosis rate requiring reoperation in our study cohort was about 1%. Patients with persistent radiological signs of pseudoarthrosis may remain asymptomatic for several years.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB approval: REB19-0858, University of Calgary.