
Abstract
Study Design:
Retrospective case series analysis.
Objective:
To identify relevant clinical and radiographic markers for patients presenting with infectious spondylo-discitis associated with spinal instability directly related to the infectious process.
Methods:
We evaluated patients presenting with de-novo intervertebral discitis or vertebral osteomyelitis /discitis (VOD) who initiated non-surgical treatment. Patients who failed conservative treatment and required stabilization surgery within 90 days were defined as “failed treatment group” (FTG). Patients who experienced an uneventful course served as controls and were labeled as “nonsurgical group” (NSG). A wide array of baseline clinical and radiographic parameters was retrieved and compared between 2 groups.
Results:
Overall 35 patients had initiated non-surgical treatment for VOD. 25 patients had an uneventful course (NSG), while 10 patients failed conservative treatment (“FTG”) within 90 days. Factors found to be associated with poorer outcome were intra-venous drug abuse (IVDA) as well as the presence of fever upon initial presentation. Radiographically, involvement of the same-level facets and the extent of caudal and rostral VB involvement in both MRI and CT were found to be significantly associated with poorer clinical and radiographic outcome.
Conclusions:
We show that clinical factors such as IVDA status and fever as well as the extent of osseous and posterior element involvement may prove to be helpful in favoring surgical treatment early on in the management of spinal infections.
Introduction
Infections involving the spine column can be life-threatening and highly disabling, with incidence ranging between 1:20 000 and 1:100 000 with accompanied mortality rates reaching as high as 20% in developed countries.1-3 Anatomically, bacterial spinal infections (SI) can attack a number of structures such as the vertebral body (osteomyelitis), the disc space (discitis), facet joints (infectious spondylitis), the epidural space (epidural abscess and/or phlegmon), paravertebral muscles in isolation or in any combination. 4 Excluding larger epidural abscesses, where surgery is more commonly indicated due to concern for neurologic decline, management of spinal VOD is primarily nonsurgical following well-established management paradigms 5 and aims at eradicating the pathogen and following healing is expected to result in pain relief and return to independent function. Regardless of the specific microorganism or the anatomic locations these tenets of nonsurgical care usually include the trifecta of: 1) targeted antibiotic therapy based on biopsy and/or blood culture proven specific pathogens isolated from the infectious source6,7; 2) some form of bracing 8 and 3) nutritional supplementation. 9 Unresponsiveness to antibiotic infection treatment, progressive neural element compromise and progressive spinal deformity usually suggests failure of nonsurgical care and may lead to considering surgical intervention in form of debridement, stabilization of the affected segment and even formal reconstruction.10-14
Although instability remains a major consideration in the decision making and timing of instrumentation surgery for spinal instability in nonsurgical versus surgical management of VOD, little has been published about variables which may predict such infectious spinal instability.
Hypothesis
We hypothesize that certain clinical and radiographic characteristics may be associated with late instability and predict failure of nonsurgical treatment for VOD.
The objective of the current study was therefore to expand the current knowledge on pending instability of a de novo spine infection (dnSI) by performing a pilot study, with the purpose of searching for clinical and radiographic markers that may be associated with late instability.
Methods
Authors declare that the research was conducted according to the principles of the World Medical Association Declaration of Helsinki “Ethical Principles for Medical Research Involving Human Subjects,” (amended in October 2013) and was approved by the Swedish Health services institutional review board (STUDY2017000146). Since this is a retrospective study, we have been deemed exempt from receiving informed consent. We retrospectively searched our computerized database for patients who presented to a single health network (Swedish, Seattle) over a course of 3 years (2017-2019) with dnSI who were initially treated nonsurgically. Patients were identified by retrieving those who underwent CT guided aspiration of dnSI with an underlying pathology inclusive of spinal osteomyelitis, discitis or a combination thereof. We intentionally excluded any patients from our analysis with intra-spinal or paraspinal abscesses as the major pathology as these are often regarded as indication for either interventional and/or surgical management and spinal stability is usually not compromised. Minor phlegmons and abscesses accompanying the major spondylo-discitis pathology were included. In addition, we excluded patients who underwent biopsy for relatively non-specific findings such as increased MRI contrast agent uptake around the facet joints or soft tissues as well as patients under the age of 18. Finally, for the purpose of focusing on factors that could be related to instability, we excluded patients who had previously received spine surgery in an area adjacent to the newly diagnosed VOD as their spinal biomechanics probably had been altered as a result of the previous spine surgery. Flow chart depicting the initial number of patients retrieved and the remaining after exclusions is presented in Figure 1. After agreeing on a clear group that met our PICO definitions, we divided the group into those who had an uneventful course, i.e. patients in which SI had resolved after completion of antibiotic and bracing, nutritional support treatment (non-surgical group “NSG”) and patients who due to clinical or radiographic deterioration, required surgical stabilization within 90 days of presentation (failed treatment group “FTG”). For all cases of Spondylo-discitis managed conservatively, bracing protocol was comprised of the following: In any involvement of mobile spine segments such as the cervical of lumbar regions and if the patient was ambulatory, an attempt was made to fit a rigid brace (rigid collar for the cervical spine or Thoracic Lumbar Sacral orthosis (TLSO) for involvement of the lumbar spine. In cases of poor tolerance for rigid bracing, management included soft bracing. In the few cases where the disease has resulted in patients being bed-bound, bracing was not required. In all cases, nutritional support consultation was requested. Main nutritional goal was mainly based per Albumin level and was set to be more than 3.5 g/dL, both pre-operatively as well as post operatively (in cases requiring surgery at a later stage).
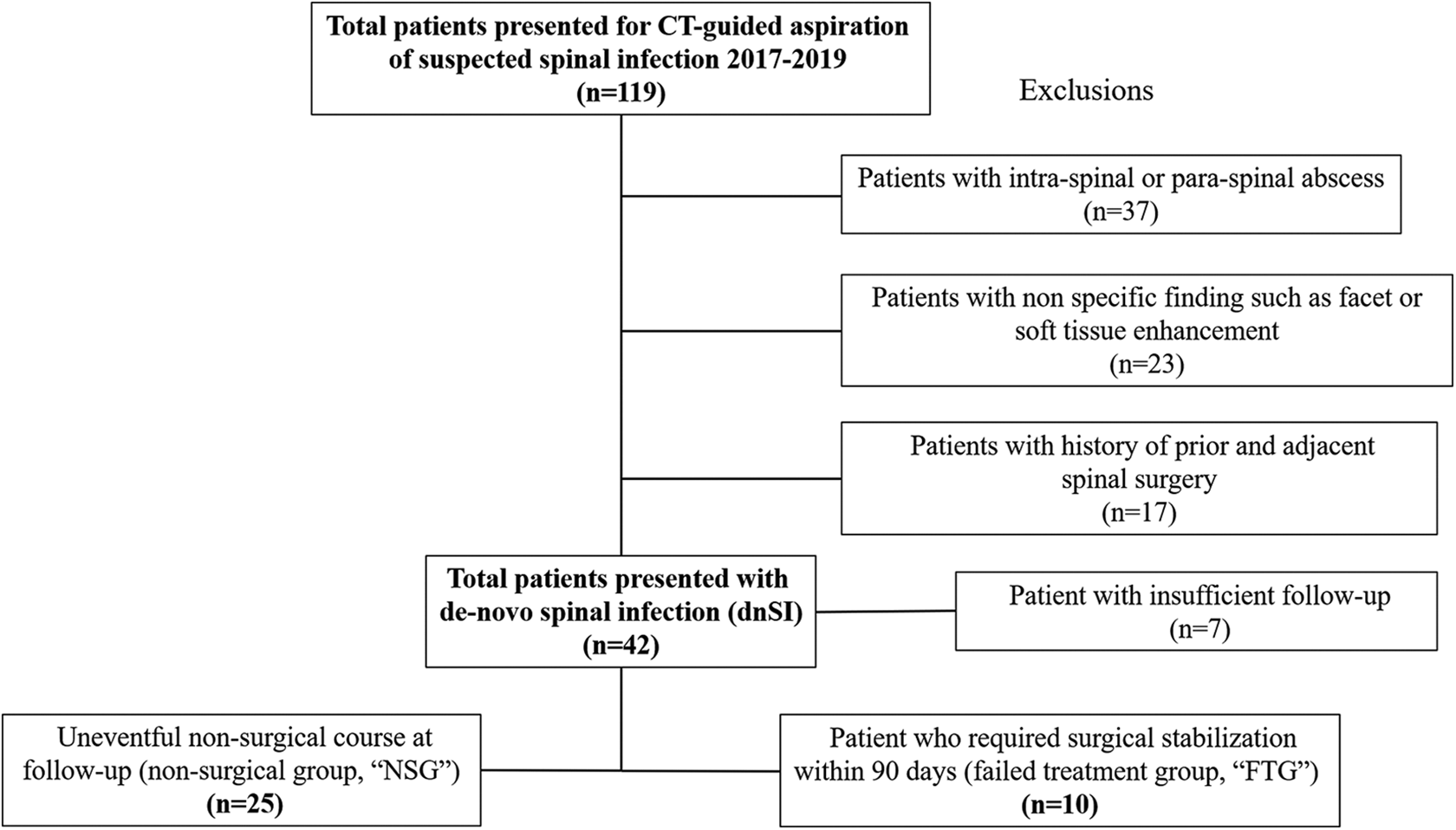
Flow chart depicting the initial number of patients retrieved and the remaining after the exclusions described above.
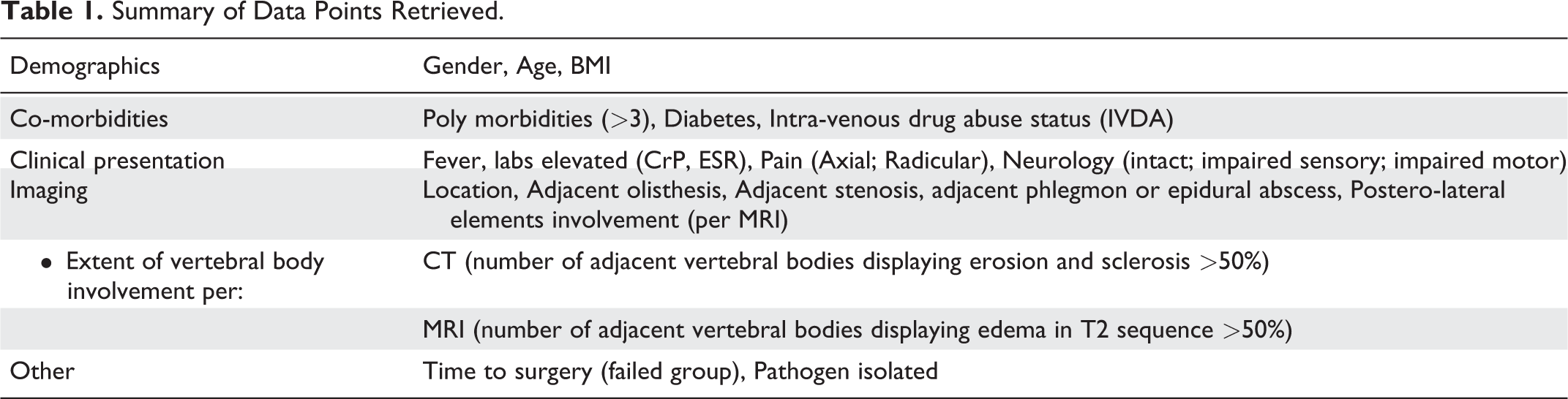
Demographic variables collected included gender, BMI, multi-co-morbidities (as in presence of more than 3 major co-morbidities), presence of diabetes mellitus (DM) and history of IVDA, presence of fever (>100.4 F), elevated inflammatory markers (CrP > 5 mg/L and/or ESR > 30 mm/hr), type of pain upon presentation (axial or radicular) and presence of a neurological deficit (intact, incomplete sensory or incomplete motor). Radiographic variables determined included location (based on both the anatomic segment and spine region affected) and the presence of the following adjacent findings: olisthesis, paraspinal phlegmon and/or abscess and central canal stenosis. Postero-lateral element disease involvement was defined by the presence of edema or increased MRI contrast uptake at the facet joint level itself and was graded according to number of facet joints involved (none, 1 or bilateral). The extent of adjacent vertebral body (VB) involvement (rostral and caudal VB) was measured independently both on CT (lytic, osteoblastic disease response or combination) and MRI (edema) as being less or more than 50% of VB height involved and was similarly graded (none, one VB > 50%, both VB > 50%). Finally, we retrieved the type of pathogen isolated and the time to surgery in the failed conservative group. A summary of the variables retrieved is shown in Table 1.
Summary of Data Points Retrieved.
For the purpose of statistically analyzing the difference in variables between the 2 groups we used the chi square test to compare categorical variables and the independent t-test to compare continuous variables. A P-value of less than 0.05 was defined as being statistically significant to reject the null hypothesis of lack of difference between the group which responded to conservative treatment and the failed group.
Results
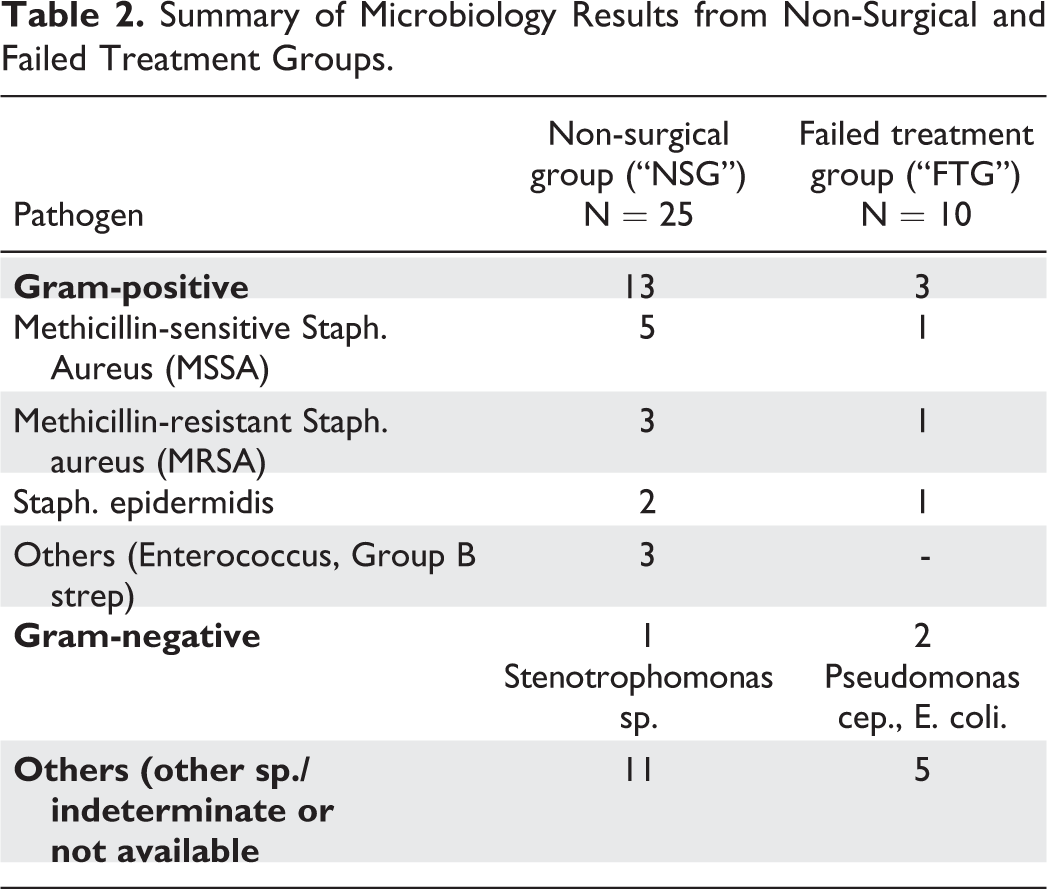
From January 2017 to June 2019, we retrieved a total of 119 patients who presented with radiographic findings suggestive of SI (vertebral osteomyelitis/discitis (VOD), intra- or paraspinal abscess or other non-specific finding) and received Interventional Radiology guided spinal biopsy to help in identifying the most appropriate antibiotic therapy. After excluding patients with soft tissue abscess, non-specific findings, prior adjacent spinal surgeries and insufficient clinical documentation or imaging studies at follow up (See flow chart; Figure 1), there were 35 patients remaining who presented with de-novo SI. In all patients, biopsy was followed by the initiation of nonsurgical management with targeted antibiotic management and some form of immobilization (rigid brace in the majority, soft brace and none in few cases where patients were bed-bound) and nutritional support. We found that 25 (71%) of our patients (13 males, 12 females, mean age 62 ± 14) concluded our nonsurgical treatment successfully as defined by satisfactory resolution of the active infection, return to independent preoperative function and without need for further spinal imaging, surgery or additional procedures during our 90-day observation window (non-surgical group; NSG). Conversely, in 10 patients (8 males, 2 females, mean age 58.8 ± 14.2) our nonsurgical treatment had failed (FTG) as identified on advanced re-imaging of the initially infected spinal segment. All patient but one in each group had initially presented with single level osteo-discitis (there was one case of 2-level discitis affecting contiguous levels in each group). Among additional symptoms leading to re-imaging was persistent back pain (n = 9), persistent fever (n = 4) or new hand or leg numbness (n = 3). Fortunately, no partial or complete motor deficits were noted. On re-imaging, we found progressive bony destruction and deformity in 9/10 patients, consisting of either kyphosis (n = 4), new olisthesis (n = 3) or both (n = 2). In one patient, the lack of adequate clinical response led to surgery in the absence of objective radiographic deterioration. Surgery consisting of uneventful debridement, neural decompression and spinal stabilization with fusion was performed at a mean follow up of 36.8 ± 20.7 days following the initial presentation. In terms of pathogens, all infections were primary with no clinical or pathologic evidence of secondary- or co-infections. Micro-organisms isolated were bacterial species alone, with the most common being Methicillin-sensitive Staph. aureus (MSSA). Microbiology culture results comparing patients in the NSG and FTG are summarized in Table 2.
Summary of Microbiology Results from Non-Surgical and Failed Treatment Groups.
After our analysis of clinical variables, we found that both IVDA use as well as the presence of fever upon presentation were found to be significantly associated with the “failed treatment group”(FTG). There was no association of poorer outcomes found in correlation to other clinical conditions such as morbid BMI, poly-morbid status, type of presenting pain or type of impaired neural elements at time of initial presentation. A summary of the compared demographic and clinical variables is presented in Table 3.
Comparison of Demographic and Clinical Variables between the Conservative vs. Failed Groups.
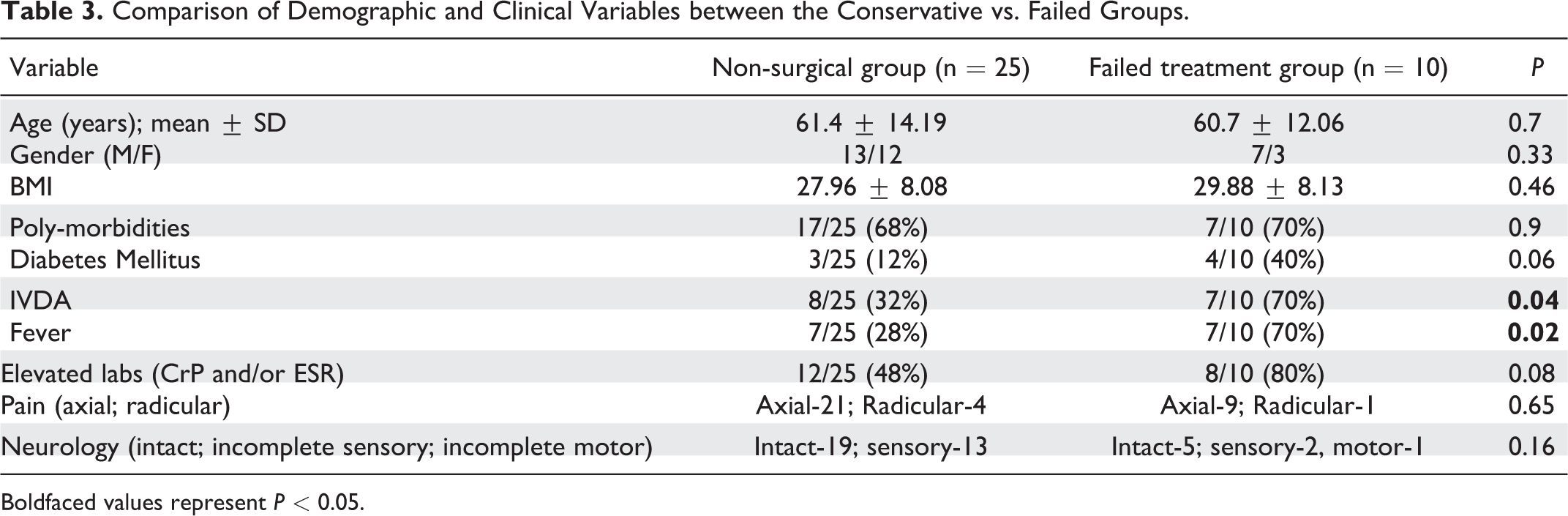
Boldfaced values represent P < 0.05.
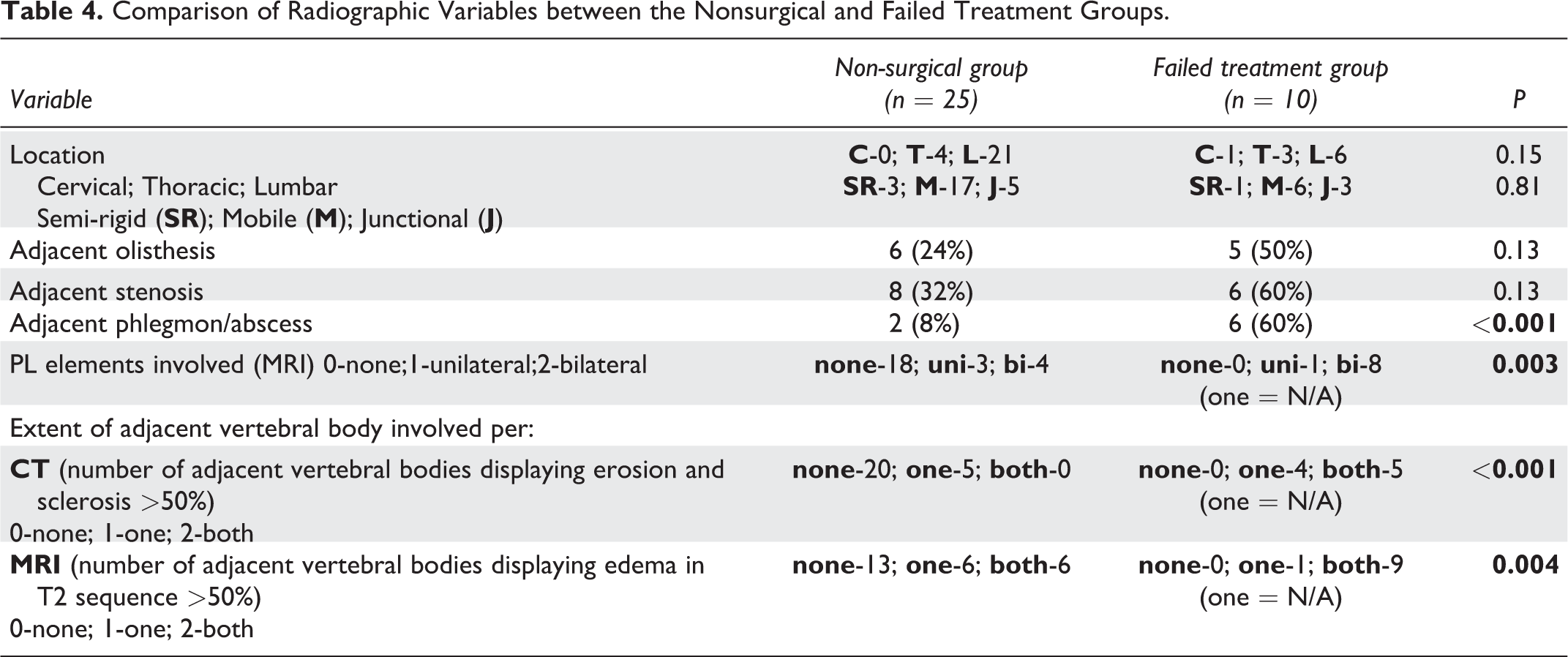
Radiographically, several variables were found to be significantly associated with a failed conservative treatment (Table 4). In terms of osseous elements, involvement of both same-level facet joints and the extent of caudal and rostral VB involvement were found to be significantly associated with poorer outcome in both MRI (increased contrast uptake and/or edema) and CT (osteoblastic and/or lytic disease response). In addition, adjacent peri-spinal abscess or phlegmon were also significantly more common in the FTG compared to the NSG. All olisthesis noted was grade 1 and no association was found between location or the presence of an adjacent olisthesis or central canal stenosis with the FTG. Three representative case each of the FTG and the NSG are presented in Figures 2 and 3, respectively.
Comparison of Radiographic Variables between the Nonsurgical and Failed Treatment Groups.
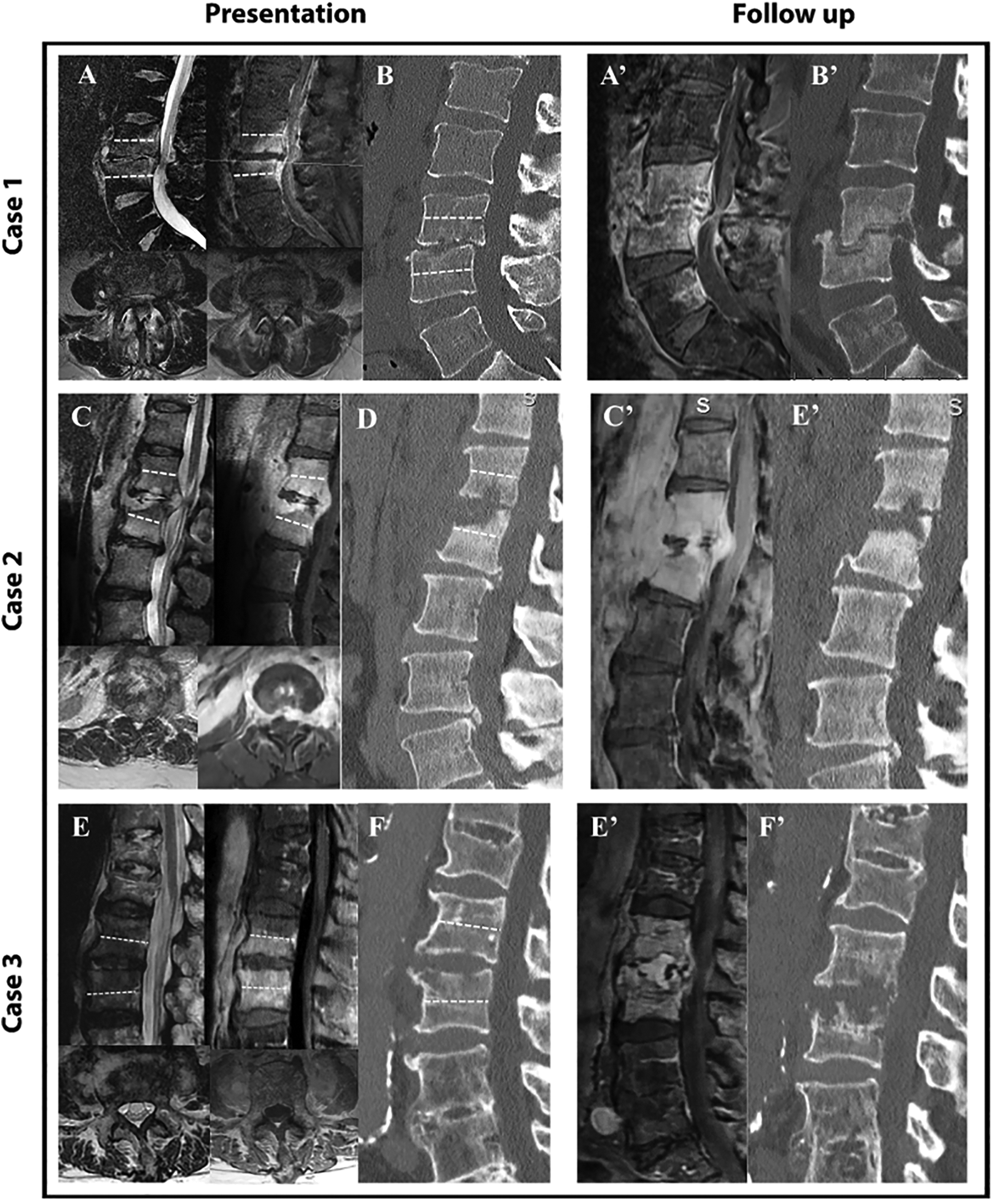
Three representative cases of the failed treatment group upon presentation (T2, T1 with contrast and sagittal CT; A + B, C + D and E + F) and follow up (T1 with contrast and sagittal CT; A’ + B’, C’ + D’ and E’ + F). Dashed white line marks 50% of VB height. In all cases upon presentation, osseous edema extends to more than 50% of vertebral body (VB) height as well as to both sides of the posterolateral elements. Bony sclerosis or resorption involved more than 50% of both rostral and caudal VB in cases 1 and 3 and the caudal VB of case 2.
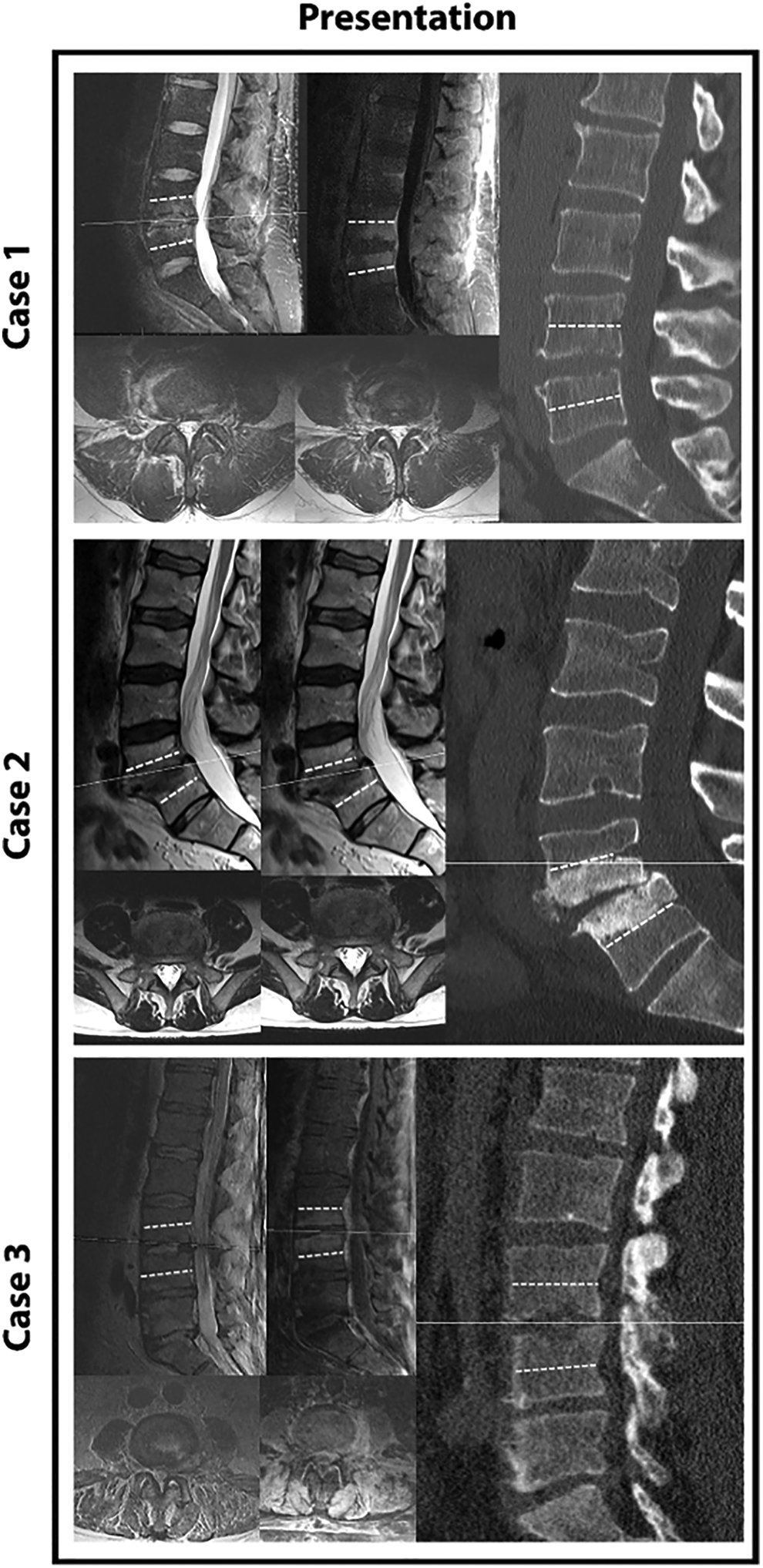
Three representative cases of the non-surgical group upon presentation (T2, T1 with contrast and sagittal CT; A + B, C + D and E + F). Dashed white line marks 50% of VB height. No case was found to display bilateral facet joint involvement with edema or contrast uptake. Also, the extent of VB findings (MRI or CT) was generally limited to less than 50% of adjacent VB height.
Finally, surgical treatment in the failed treatment group (FTG) included the following: In the one case of cervical infection that failed non-operative management, surgery consisted of an anterior cervical discectomy and fusion (ACDF). Longitudinal carotid approach was followed by discectomy using routine curettes and drill, placement of a allograft bone spacer and titanium screws and plate. In the thoracic (n = 3) and lumbar (n = 6) cases, standard posterior approach was followed by posterior instrumentation using pedicular screws. After debridement of the affected disc and phlegmon (where present), we supplanted the procedure by inter-body fusion using a poly-ether-ether-ketone (PEEK) cage inserted using a trans-facetal approach in the thoracic cases (in 1 out 3 cases) and a trans-foraminal (TLIF) approach in the lumbar cases (in 5 out of 6 cases).
Discussion
Growing evidence suggest that rate of dnSI is steadily on the rise with possible contributing factors such as increasing proportion of spinal procedures performed in the elderly and immune compromised, increasing rates of intra-venous drugs use and better diagnostic techniques.1,11,15,16 The inherent disease complexity and prerequisite interdisciplinary approach management of spinal infections as well as the associated direct and indirect clinical and human cost17,18 makes improved treatment algorithms of spinal infection care and complication avoidance clearly desirable.
Over recent years, 2 spine sub-specialties have provided scoring tools to facilitate decision making in the management process and provide some basis for predictive analytics in the future. In Spine Trauma, for instance, the TLICS 19 and SLIC 20 scores have gained increasing popularity with relatively clear and easily applicable parameters to help quantify the magnitude of thoraco-lumbar and sub-axial spine trauma incurred. Similarly, for Spine Oncology the Spine instability neoplastic score (SINS) with heavy emphasis on stability as well as others systems21-24 have provided helpful tools that can facilitate surgical decision-making and again quantify aspects of spinal stability to overall disease burden relative to outcomes. Surprisingly, in spite of similarity in complexity, equivalent scoring tools to guide surgical treatment or even prognostic factors in dnSI are still lacking. Our analysis provides some variables which, alongside additional studies, might be a helpful in suggesting which patients presenting with dnSI may benefit from early stabilization surgery.
In looking at clinical covariable for failed nonsurgical treatment, not surprisingly we found the presence of fever on presentation and intra-venous drugs (IVD) use to be predictors of failure. While the presence of fever on presentation may represent heavier systemic immunologic compromise or even sepsis our finding of active IVDA, while intuitively clear to some, stands in contrast to at least one study reporting favorable response to intravenous antibiotics. 25 Although underlying poly-morbid status was not found to be a significant risk factor, diabetes did approach significance (P = 0.06), suggesting that certain co-morbidities more than others may predispose the medically susceptible patient to poorer outcome. With respect to identified pathogens, only 32% of Interventional aspirations in the NSG and 20% of the FTG were positive for Staph. Aureus, which previously had been reported as causative organism in 55% of cases of spinal osteomyelitis. 26 Possible explanations for this disparity may lie in sampling variations from our relatively small study cohort. Radiographically, the extent of vertebral body involvement per both CT and MRI correlated significantly FTG. Interestingly, our findings that posterior facet joint disease involvement is similar to that of the SINS score formulated for stability determination in spinal oncologic patients.
Recently, Appalanaidu and colleagues have published a score that provides several clinical and radiographic predictors to guide surgical treatment of spondylodiscitis, 27 citing several shared factors including comorbidities such as DM and IVDA and abscess formation. In contrast, our radiographic analysis found additional, more detailed markers such as involvement of the vertebral bodies or posterolateral elements as key predictors for failure, providing higher resolution imaging findings that may help guide treatment better from a stability perspective. Counter to the study by Appalanaidu et al we found no differences in symptom duration or severity prior to initial presentation in our health care system in our 2 comparison groups.
Our study has a number of limitations. Of course, the retrospective nature of our study that used an institutional database and procedure codes for interventional radiology tissue biopsies may introduce elements of selection and retrieval bias.
Further key variables of adherence to 2 other factors of nonsurgical dnSI management could not be controlled for: 1) effectiveness and compliance with external immobilization to minimize mechanical factors in disease propagation; 2) participation in meaningful nutritional optimization with the goal of optimizing the immune system. From an antibiotic management standpoint, we could not control for changing resistance patterns and present or absent antibiotic adjustments relative to resistance patterns identified. We were, however, assured that all patients indeed were on intravenous antibiotic management by virtue of a controlled administration program suitable for all patients regardless of their psychosocial and payor specific circumstances. As desirable as regular tracking and representation of key inflammatory markers, like C reactive protein and erythrocyte sedimentation rate (ESR) might be, we had to resort to qualitative (elevated or not) rather than quantitative assessment of these due to changes in reporting quantities during our observation window.
Our study reflects a real-world experience largely dealing with pyogenic microorganisms seen in a developed nation. In contrast, the manifestations of mycobacterial and fungal infections seen in other parts of the world may indeed be very different and the tolerances to mechanical instability and derangement, may be very different.
Finally, the relatively small cohort size of our 2 comparison groups that had been selected for nonsurgical treatment raises the potential for small group variability variance and aberrations. From a statistical standpoint, this prevents from performing multivariate analysis and increases the likelihood of performing a type II error. We intentionally focused on patients who were selected as ideal candidates for nonsurgical infections management from our overall very large pool of spinal infections, where some form of interventional and surgical management is usually heavily preferred over purely nonsurgical care (in a random sample of 3 months during 2017, out of 24 patients who presented with SI to a single campus, only 3 were treated non-surgically). This choice of study design, while enabling analysis of variables associated with failed conservative treatment, resulted in relatively small sample groups. Therefore, this real-world efficiency study may have some foundational observational value in determining factors for success of nonsurgical management and predictors for failure.
The key insights in our study on nonsurgical management of VOD were that, aside from active IVDA, a previously reported but still debated clinical variable presentation with fever was a negative predictor for successful nonsurgical management. Moreover, we found mechanical stability to be a statistically important and previously not reported factor in determining success of nonsurgical management. The findings of our study hopefully will lay the foundation for a more focused assessment of relatively simple and reproducible parameters that may predict vertebral collapse and displacement in VOD and moreover its effect on management practices and correlation to eventual outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.