
Abstract
Study Design
Prognostic study.
Objectives
The objective of this study is to identify predictive factors for cloxacillin susceptibility in spinal infections.
Methods
A retrospective analysis was conducted using data from January 1, 1997, to December 31, 2021. The study included patients presenting with back pain and either a positive bacterial culture from the spine or radiological evidence of spinal infection (spondylodiscitis and/or epidural abscess) along with positive bacterial blood culture.
Results
Among 171 patients (127 males, 44 females), 53.2% had Staphylococcus isolates, with 40.4% showing cloxacillin resistance. Lower globulin levels (<33.5 g/L), recent hospitalization within 90 days, and residence in an old age home predicted gram-positive bacteria with cloxacillin resistance and gram-negative bacteria as causative organisms (P<.05). The 30-day and 1-year all-cause mortality rates were 0% and 8.2%, respectively. Higher red cell distribution width (RDW >16.1%) and Charlson comorbidity index (CCI) scores predicted 1-year all-cause mortality (P<.05). Intensive care unit admission was required for 9.9% of patients.
Conclusions
This study identified predictive factors for spinal infection by gram-positive bacteria with cloxacillin resistance and gram-negative bacteria. Patients with lower globulin levels (<33.5 g/L), recent hospitalization within 90 days, or residency in an old age home upon admission should avoid standalone cloxacillin therapy and consider antibiotics with gram-negative coverage. Higher RDW (>16.1%) and CCI scores were associated with increased 1-year all-cause mortality. These findings contribute to treatment decision-making and improving patient outcomes in spinal infections.
Keywords
Introduction
Spinal infections account for approximately 2%-7% of all musculoskeletal infections. 1 Bacterial spinal infections occur at a rate of .4-2.0 cases per 100,000 people each year, and this incidence is increasing due to improved life expectancy among patients with chronic diseases. 2
Diagnosing spinal infections is often challenging because back pain is frequently attributed to non-infectious causes. 3 However, delaying the diagnosis and treatment of spinal infections can lead to severe complications, including sepsis, neurological problems, spinal deformities, persistent pain, and even death. The primary approach to treating spinal infections involves medical treatment, such as administering appropriate antibiotics with or without the use of braces. Surgical intervention becomes necessary in cases where there are neurological deficits, spinal instability, failed conservative treatment, or when an open biopsy or culture is required. 4
According to existing literature, the most common cause of bacterial spinal infections is methicillin-sensitive Staphylococcus aureus. 5 Consequently, empirical antibiotic treatment with cloxacillin is recommended based on the Infectious Diseases Society of America (IDSA) clinical practice guidelines. 6 However, it is important to note that there are bacterial strains causing spinal infections that are resistant to cloxacillin. No studies have been conducted to investigate the effectiveness of cloxacillin as an empirical treatment for spinal infections.
The aim of our study is to identify predictive factors that can help anticipate cloxacillin resistance or treatment failure in spinal infections. This information will be valuable in guiding the selection of appropriate empirical antibiotic treatment options.
Materials and Methods
This study received ethical approval from the local institutional review board (HKU/HA HKW IRB, Reference number: UW 22-794). Given the retrospective nature of the study, informed consent was waived. A comprehensive review of medical records spanning a 25-year period (January 1, 1997, to December 31, 2021) was conducted. Patients were identified based on discharge diagnoses of spondylodiscitis and/or epidural abscess using the Clinical Data Analysis and Reporting System in the Hospital Authority. Inclusion criteria encompassed patients of all ages presenting with either back pain and positive bacterial culture from the spine, or back pain accompanied by radiological features of spinal infection (spondylodiscitis and/or epidural abscess) and positive bacterial blood culture. Patients with mycobacterial or fungal infections, incomplete records, absence of positive bacterial culture from the site of infection, or a history of spinal operation in the same region prior to infection were excluded from the study. Patient recruitment process was summarized in a flowchart of Figure 1. Flowchart of patient recruitment. 171 patients were included in the final analysis.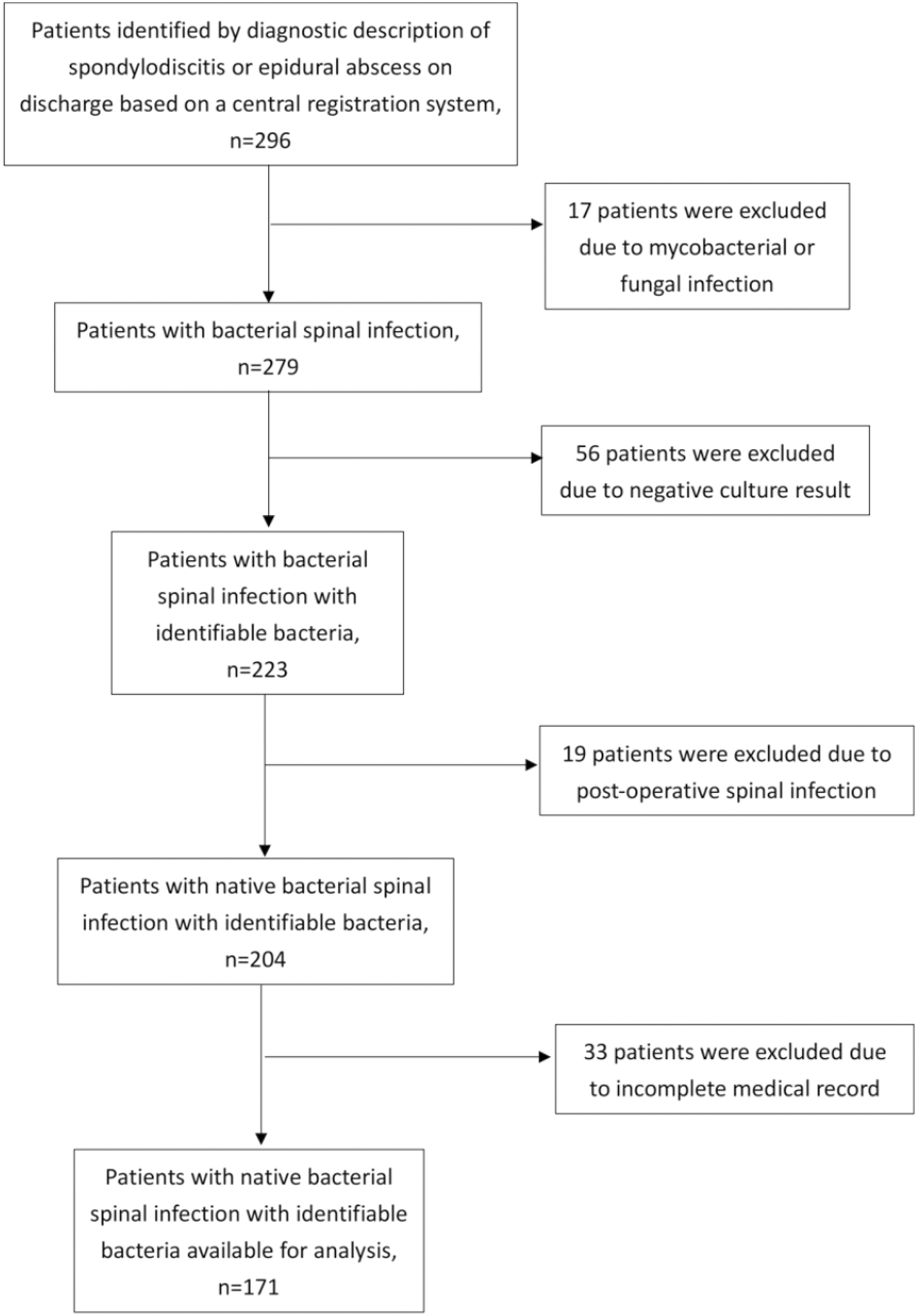
Patients’ demographic data including age, gender, presence of diabetes mellitus, comorbidities in terms of Charlson comorbidity index (CCI), 7 recent hospitalization within 90 days and status of old age home resident during admission were collected. Blood tests result (normal reference ranges are stated in Appendix 1) on presentation including white cell count (WCC), absolute neutrophil count (ANC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), albumin, globulin, bilirubin, alkaline phosphatase (ALP), alanine transaminase (ALT), aspartate aminotransferase (AST), sodium (Na), potassium (K), chloride (Cl), creatinine, hemoglobin (Hb), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), red blood cell (RBC) count, red cell distribution width (RDW), mean corpuscular volume (MCV), platelet count (Plt), international normalised ratio (INR) were collected. The first set of blood tests results on the date of admissions were used for analysis.
The primary outcome is cloxacillin susceptibility (using methicillin or oxacillin susceptibility as surrogate) in spinal infection and identification of any predictive factors that can predict cloxacillin susceptibility which in turn guides empirical treatment. If methicillin or oxacillin susceptibility was tested for the bacteria, it would be used as surrogate for cloxacillin. Otherwise, all gram-negative bacteria were regarded as resistant to cloxacillin and all staphylococci and streptococci (except methicillin-resistant staphylococci or enterococci) were regarded as sensitive to cloxacillin. In instances of polymicrobial infections, we assigned cases to the cloxacillin-sensitive group if all isolates from the patient were found to be sensitive to cloxacillin. Conversely, if any of the isolates were resistant to cloxacillin, the case was assigned to the cloxacillin-resistant group. Secondary outcomes included examining the gram stain characteristics of the organisms, assessing 30-day and 1-year all-cause mortality rates, as well as determining the rate of admission to the intensive care unit (ICU).
Statistical Analysis
Independent t test was used for continuous variables. Chi-squared test was used for discrete variables. Any independent variables that reached a statistical significance of <.05 were then included in the multivariate models, in order to investigate for the predictors for the outcomes. Receiver operating characteristics (ROC) curve was used to determine the optimal cut-off values for laboratory parameters. Data analysis was performed using the SPSS software version 22.0 (IBM®, Armonk, NY, US).
Results
Descriptive Characteristics
Patients Characteristics.

Bacteriology
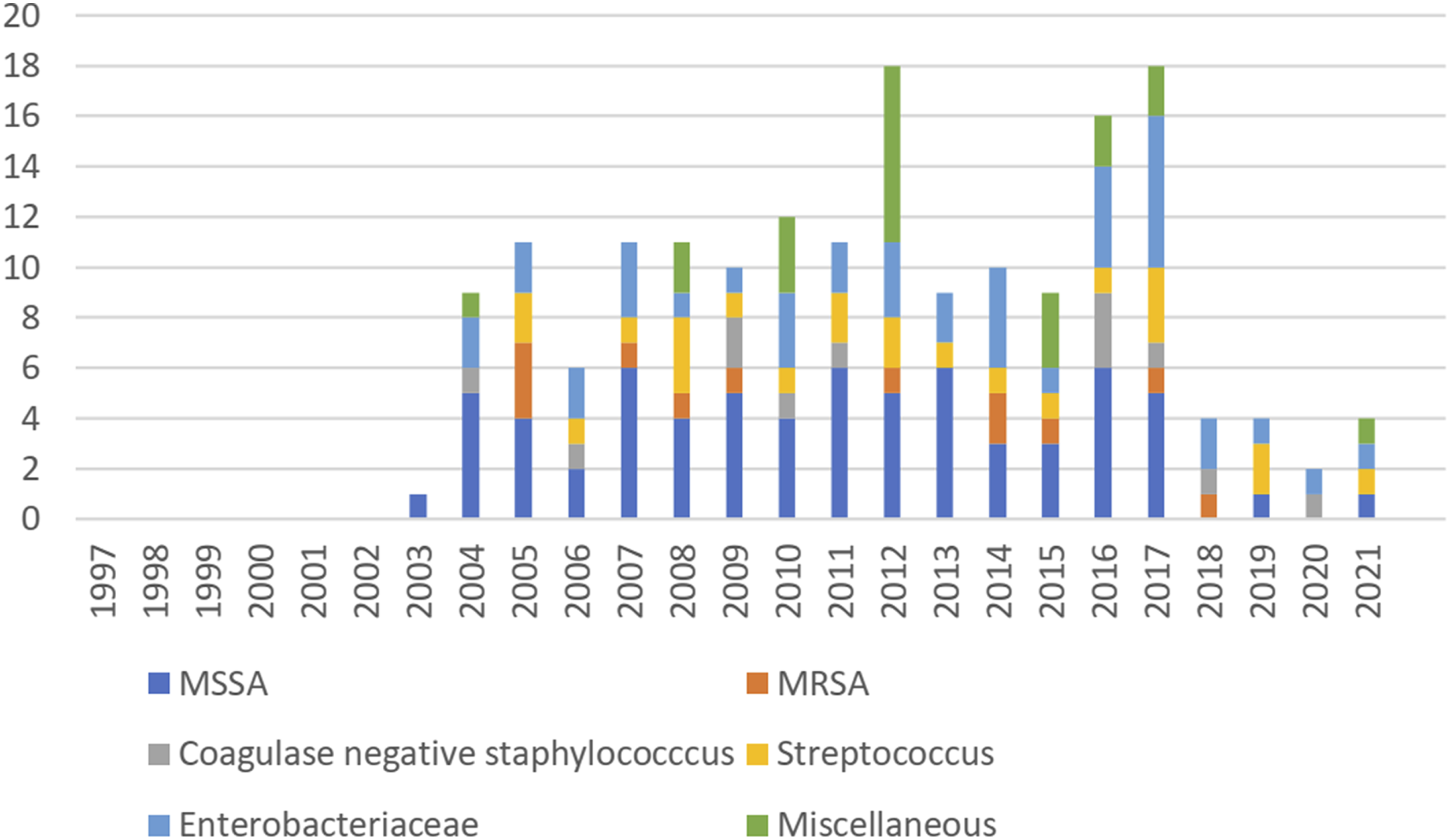
Among the 167 patients with monomicrobial infection, 70.7% (118/167) were caused by gram-positive bacteria, and 29.3% (49/167) were caused by gram-negative bacteria. Polymicrobial infection was observed in 4 patients. Staphylococci were the most commonly isolated bacteria, accounting for 53.2% (91/171) of cases, followed by Enterobacteriaceae (23.9%, 41/171), streptococci (13.5%, 23/171), and a miscellaneous group (12.2%, 21/171) (Figure 2). Staphylococcus aureus (86.8%, 79/91) and Escherichia coli (65.9%, 27/41) were the predominant species within the staphylococci and Enterobacteriaceae groups, respectively. Methicillin resistance was observed in 15.2% (12/79) of S aureus cases. The distribution of causative bacteria throughout the study period was summarized in Figure 3. Causative bacteria breakdown: majority of the infections were caused by staphylococci. Note: Since multiple bacteria were detected in the polymicrobial spinal infection, the percentages did not add up to a total of 100. Distribution of causative bacteria throughout the review period. Note: Most of the patients had incomplete records before 2004 and thus excluded from the study. MSSA, methicillin-sensitive Staphylococcus aureus; MRSA, methicillin-resistant S. aureus.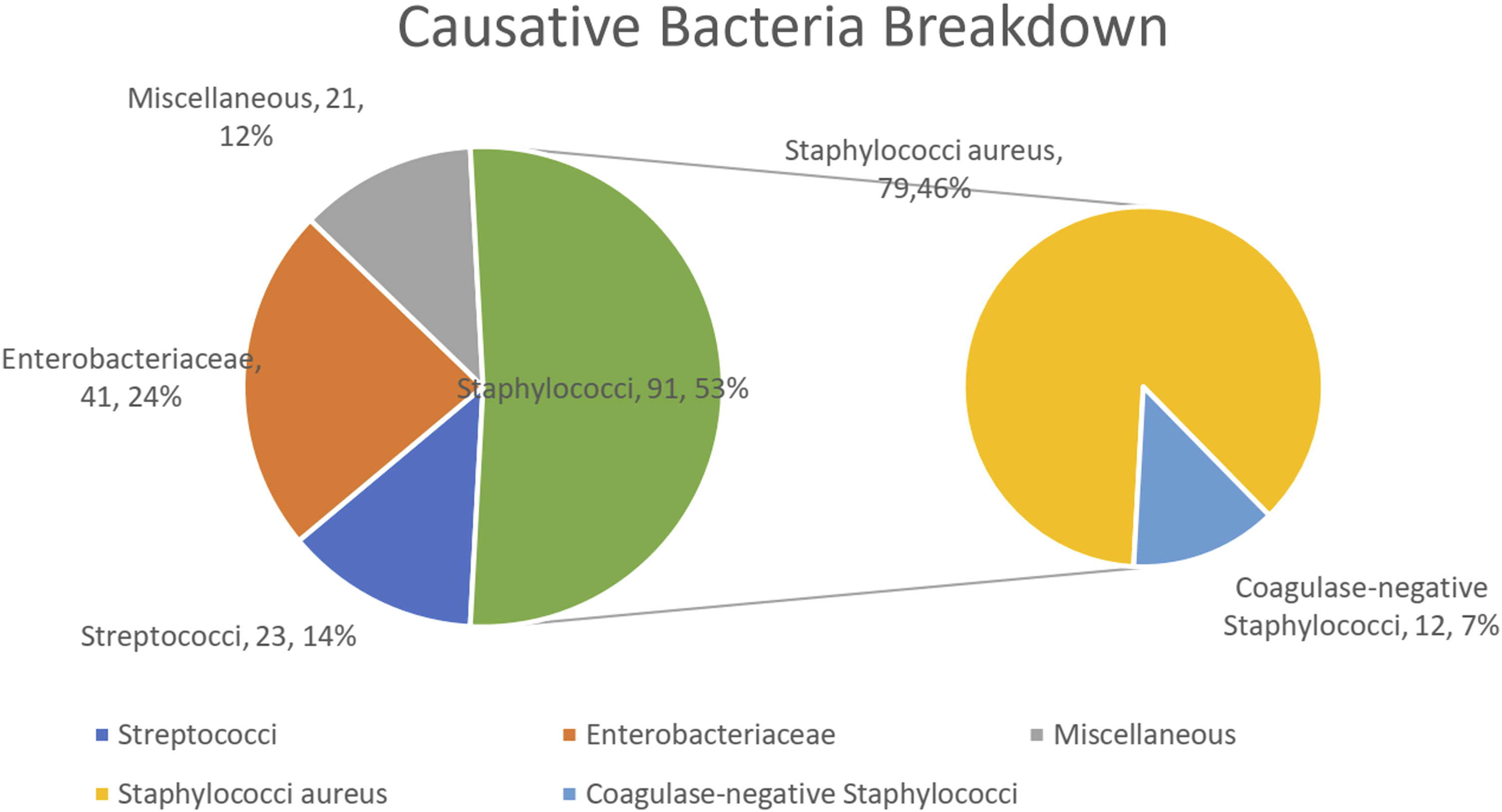
Cloxacillin Resistance and Predictors
Univariate Analysis for cloxacillin resistance.
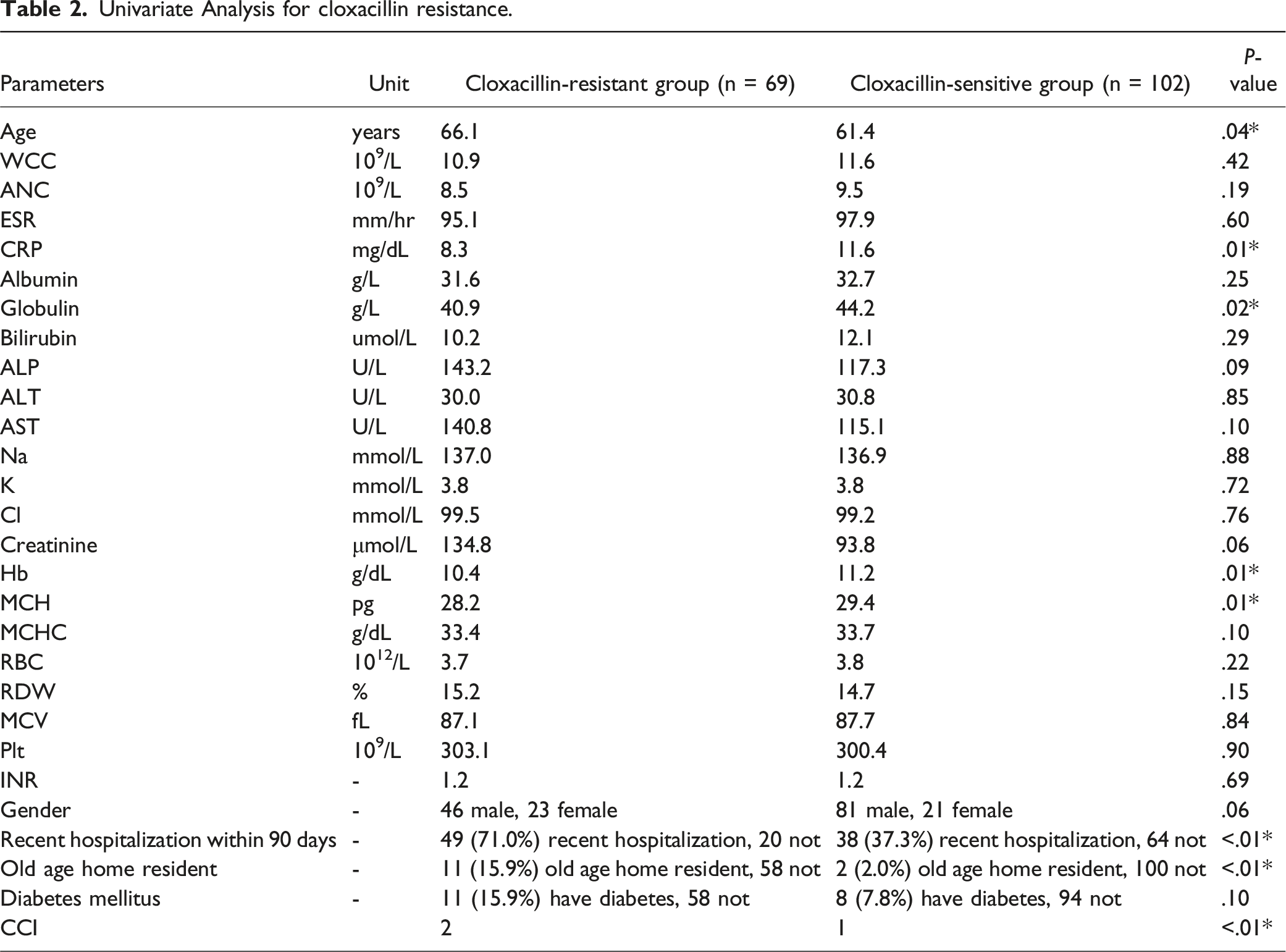
Seventy-one percent (71.0%) (49/69) of patients in the cloxacillin-resistant group had recent hospitalization within 90 days (vs 37.3% (38/102) in the cloxacillin-sensitive group, P < .01). Additionally, 15.9% (11/69) of patients in the cloxacillin-resistant group were residents of old age homes during admission (vs 2.0% (2/102) in the cloxacillin-sensitive group, P < .01). The cloxacillin-resistant group had a higher CCI when compared to the cloxacillin-sensitive group (P < .01).
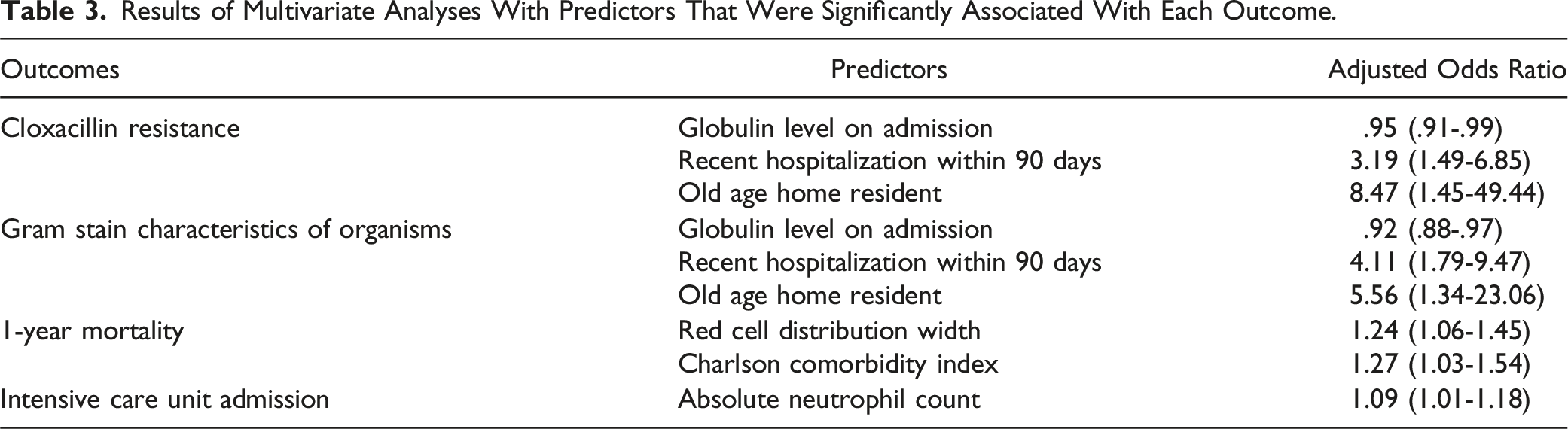
Further multivariate analysis found that the odds of cloxacillin resistance were higher with lower globulin levels (adjusted odds ratio [OR]: .95 (.91-.99), P = .02), recent hospitalization within 90 days (adjusted OR: 3.19 (1.49-6.85), P < .01), and being a resident of an old age home during admission (adjusted OR: 8.47 (1.45-49.44), P = .02). In ROC analysis, the cutoff value for globulin <33.5 g/L had a specificity of 91.2% (95% confidence interval [CI] 84.1%–95.9%) and a sensitivity of 14.5% (95% CI 6.8%–23.8%) for predicting cloxacillin resistance. (Figure 4). ROC curve for cloxacillin resistance (Area Under Curve (AUC) = .59).
Gram Stain Characteristics of Organisms and Predictors
Two of the 4 patients with polymicrobial infections had mixed gram-positive and gram-negative bacterial infection. Further analyses of the 167 patients who had monomicrobial infections were carried out to identify the gram stain characteristics of organisms and predictors. Lower levels of hemoglobin were associated with gram-negative bacterial infections, with a mean hemoglobin level of 10.2 g/dL in the gram-negative bacteria group compared to 11.1 g/dL in the gram-positive bacteria group (P < .01). Similarly, lower levels of globulin were observed in patients with gram-negative bacterial infections, with a mean globulin level of 39.6 g/L in the gram-negative bacteria group compared to 44.2 g/L in the gram-positive bacteria group (P < .01).
Seventy-six percent (37/49) of patients in the gram-negative bacteria group had recent hospitalization within 90 days (vs. 40.7%, 48/118) in gram-positive bacteria group, P < .01). Sixteen percent (8/49) of patients in the gram-negative bacteria group were old age home residents (vs. 3.4%, 4/118) in the gram-positive bacteria group, P < .01). Further multivariate analysis found that the odds of gram-negative bacterial infection was higher with lower globulin level (adjusted OR: .92 (.88-.97), P < .01), recent hospitalization within 90 days (adjust OR: 4.11 (1.79-9.47), P < .01) and old age home resident (adjust OR: 5.56 (1.34-23.06), P = .02) predicted gram-negative bacteria as the causative bacteria. ROC analysis found the cut-off of globulin <33.5 g/L had 91.7% (85.2%–95.9%) specificity and 16.1% (7.6%–28.3%) sensitivity to predict gram-negative bacteria as the cause.
30-Day and 1-Year All-Cause Mortality and Predictors
No patient passed away within 30 days of admission. Fourteen out of the 171 patients passed away within 1 year of admission, giving the 1-year all-cause mortality as 8.2%. Patients who had 1-year mortality had a higher RDW when compared to those who survived in 1 year (17.8% vs. 14.7%, respectively, P = .02). Residents of old age homes had a 23.1% (3/13) mortality rate within 1 year, compared to 7.0% (11/158) for those who did not live in old age homes (P = .04) Patients with diabetes mellitus had a 21.1% (4/19) mortality rate within one year, compared to 6.6% (10/152) for patients without diabetes (P = .03). A higher CCI correlated positively with 1-year mortality (P < .01). Higher RDW (adjusted OR 1.24, 95% CI 1.06-1.45, P < .01) and higher CCI (adjusted OR 1.27, 95% CI 1.03-1.54, P = .02) were found to predict 1-year all-cause mortality in multivariate analysis. In ROC analysis, a cut-off value of RDW >16.1% provided a specifity of 83.8% (95% CI 79.9%–91.2%) and a sensitivity of 43.8% (95% CI 19.8%–70.1%) for predicting 1-year all-cause mortality (Figure 5). In further division of CCI into four categories (0 points for none, 1-2 points for low, 3-4 points for moderate, and ≥5 points for high), moderate and high CCI categories were found to correlate with 1-year mortality (33.3% and 30.0%, respectively, vs. 4.2% and 2.1% for none and low CCI categories, respectively, P < .01). ROC curve for RDW to predict 1-year all-cause mortality (Area Under Curve (AUC) = .67).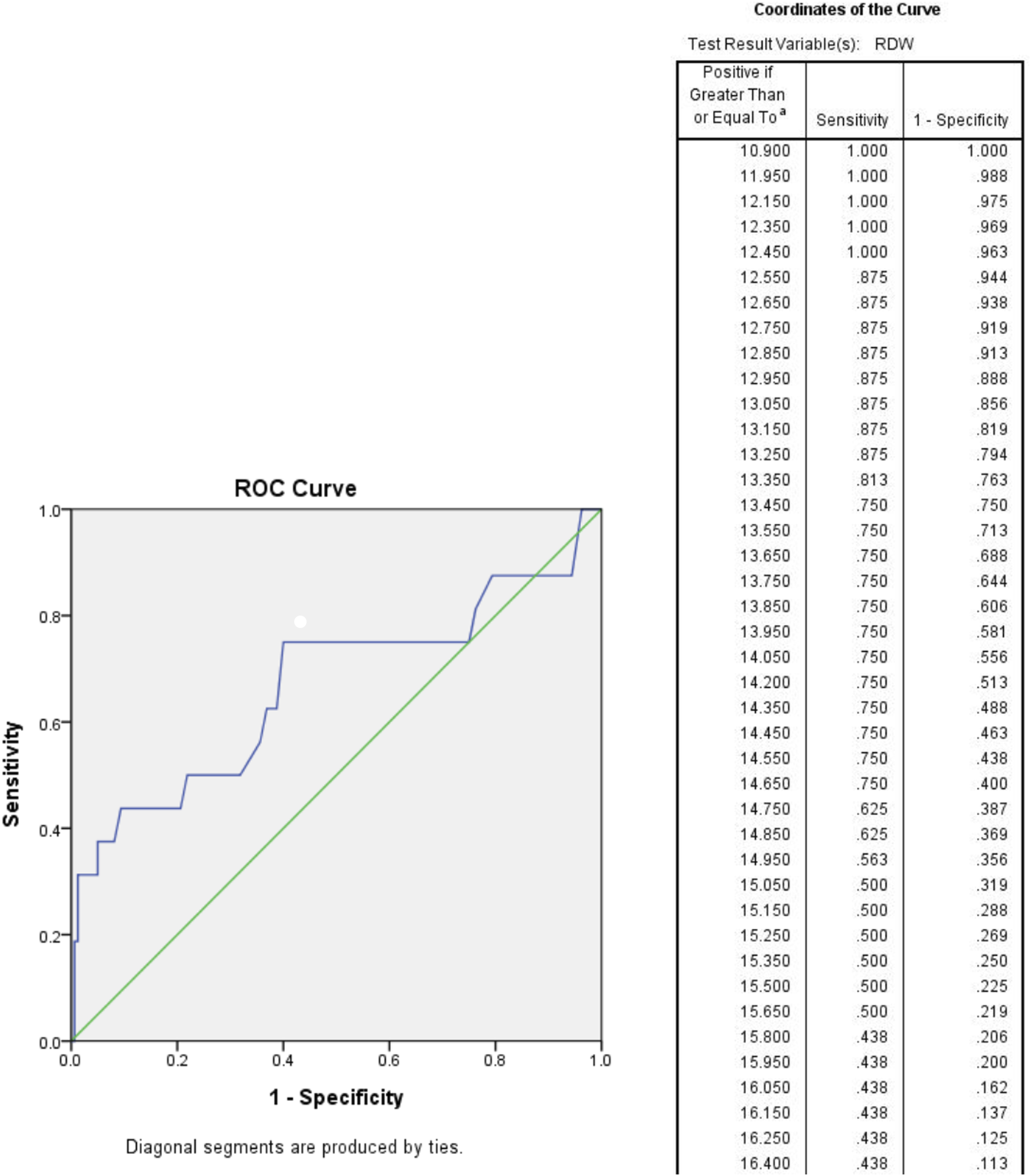
Intensive Care Unit Admissions and Predictors
Seventeen (9.9%) patients required ICU admission. This was associated with a higher ANC level (11.6 × 109/L in those admitted to the ICU vs 8.8 × 109/L in those not admitted). The OR for ICU admission based on ANC was 1.09 (95% CI 1.01-1.18, P = .04).
Results of Multivariate Analyses With Predictors That Were Significantly Associated With Each Outcome.
Discussion
Our study found that Staphylococcus was still the most prevalent pathogen group in bacterial spinal infections, with 53.2% of cases in our study population. The most frequently identified species within the Staphylococcus group was S. aureus. These findings align with existing literature references that report similar trends.5,8,9 Notably, 15.2% of the S aureus isolates in our series were found to be methicillin-resistant.
Empirical antibiotic therapy is commonly initiated to cover the likely pathogens in cases of bacterial spinal infection while awaiting definitive bacterial culture and antibiotic sensitivity results. Cloxacillin is the recommended first-line treatment for Staphylococcus infections. However, obtaining accurate culture and sensitivity results typically takes several days. It is important to avoid routine use of broad-spectrum antibiotics instead of cloxacillin, as this can contribute to unnecessary development of antibiotic resistance. To facilitate early and appropriate antibiotic treatment, it would be valuable to identify predictors for cloxacillin sensitivity or resistance based on patient characteristics and blood parameters upon admission. This approach aims to identify patients who are at risk of treatment failure with cloxacillin, which could be attributed to the presence of methicillin-resistant Staphylococcus species or other gram-negative bacteria that exhibit resistance to cloxacillin.
In our study, we observed that 40.4% of patients had bacterial isolates that were resistant to cloxacillin. Several predictors for cloxacillin resistance were identified, including lower levels of globulin, recent hospitalization within the past 90 days, and admission from an old age home.
Globulin is a group of serum proteins encompassing various components such as carrier proteins, enzymes, complement factors, and immunoglobulins. It is divided into different subfractions (α1, α2, β, and γ) based on their migration pattern during electrophoresis. Elevated globulin levels typically indicate an increase in immunoglobulins, often associated with infection or inflammation. 10 In the literature, globulin has been recognized as a potential diagnostic biomarker for conditions such as periprosthetic joint infection diagnosis, 11 a predictor for poor survival in cervical cancer patients treated with radiation based therapy, 12 and a predictor for mortality in patients undergoing peritoneal dialysis. 13 In our series, we found that lower levels of globulin were associated with cloxacillin resistance and the presence of gram-negative bacteria as the causative agents. Using a cutoff value of globulin <33.5 g/L, we achieved a specificity of 91.2% and sensitivity of 14.5% in predicting cloxacillin resistance, and a specificity of 91.5% and sensitivity of 18.4% in predicting gram-negative bacteria as the cause of infection. Recent hospitalization within the past 90 days and being a resident of an old age home were identified as predictors of cloxacillin resistance and the presence of gram-negative bacteria. These findings can be attributed to the different spectrum of bacteria encountered in healthcare settings like hospitals and old age homes compared to those in the community. Interestingly, a previous study demonstrated a higher prevalence of carbapenemase-producing Enterobacteriaceae carriers among individuals with these 2 risk factors. 14
The 30-day mortality and 1-year mortality were 0% and 8.2% respectively. A previous study found that hypoalbuminaemia was associated with a higher 30-day postoperative mortality and 90-day post-discharge mortality in spinal epidural abscess. 15 Our study could not find a statistically significant prediction of spinal infection outcome by albumin level. RDW is a measurement of variability of individual RBC volumes. The decrease in RBC clearance was an adaptation to subtle reductions in erythropoietic output to maintain circulating red cell mass in pathological conditions. 16 This in turn increased RDW. A previous study involved 15,852 adult participants showed that a higher RDW was associated with a higher all-cause mortality, mortality due to cardiovascular disease, cancer and chronic lower respiratory tract disease. 17 A recent study also found that a higher RDW at presentation was associated with higher mortality from COVID infection. 18 In our series, we found that a higher RDW and higher CCI predicted 1-year all-cause mortality. The original study from Charlson had already showed that a higher CCI correlated with a higher mortality rate. 7 Another study showed that CCI was associated with 1-year mortality in emergency department patients with suspected infection. 19 Our study showed that a cut-off of RDW >16.1% yielded 83.8% specificity and 43.8% sensitivity to predict 1-year all-cause mortality in patients with spinal infection.
Among the patients with spinal infection, 9.9% required admission to the ICU. These individuals presented with higher ANC, indicating more pronounced inflammatory responses to the infection and necessitating more intensive life support.
It is important to acknowledge the limitations of our study, primarily its retrospective design, which led to the exclusion of some records due to missing data. Also, we did not address the predictors of surgical treatment. Future prospective studies with larger sample sizes and improved record-keeping are warranted to further investigate these predictors. Nonetheless, our study provides valuable insights into predicting cloxacillin-resistant or gram-negative bacterial causative agents in spinal infection based on patients’ blood results and characteristics upon admission, thus influencing empirical antibiotic choices in clinical practice.
In summary, a lower globulin level on admission, recent hospitalization within 90 days and old age home resident status predicted cloxacillin-resistant or gram-negative bacteria as the causative organisms in spinal infection. A globulin level of <33.5 g/L upon admission showed high specificity in predicting such conditions. When selecting empirical antibiotics for spinal infection, it is advisable to avoid standalone cloxacillin therapy and consider antibiotics with gram-negative coverage when patients exhibit these risk factors. Higher RDW values (>16.1%) upon admission and a higher CCI were associated with increased 1-year mortality, while a higher ANC upon admission predicted the need for ICU admission.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.