
Abstract
Study Design
Observational Study.
Objectives
Surgical site infections (SSIs) are one of the major complications in spine surgery. Numerous factors that increase the risk of SSI have been widely described. However, clinical guidelines on antibiotic prophylaxis are usually common for all patients. There are no specific guidelines for patients with a high risk of infection. The aim of this paper is to create a specific protocol for patients at high risk of SSI.
Methods
This is a three-cohort study using a prospective database. Risk patients are those who meet at least two of the following criteria: obesity, diabetes, reoperation and immunosuppression. Between October 2021 and April 2023, 132 patients were recruited.
They were divided into three cohorts: cohort A, 46 patients, standard prophylaxis with cefazolin 2 g/8 h for 24 h; cohort B, 46 patients, cefazolin 2 g/8h and amikacin 500 mg/12 h for 24 h; cohort C, 40 patients, cefazolin 2 g/8h and amikacin 500 mg/12 h for 72 h.
Results
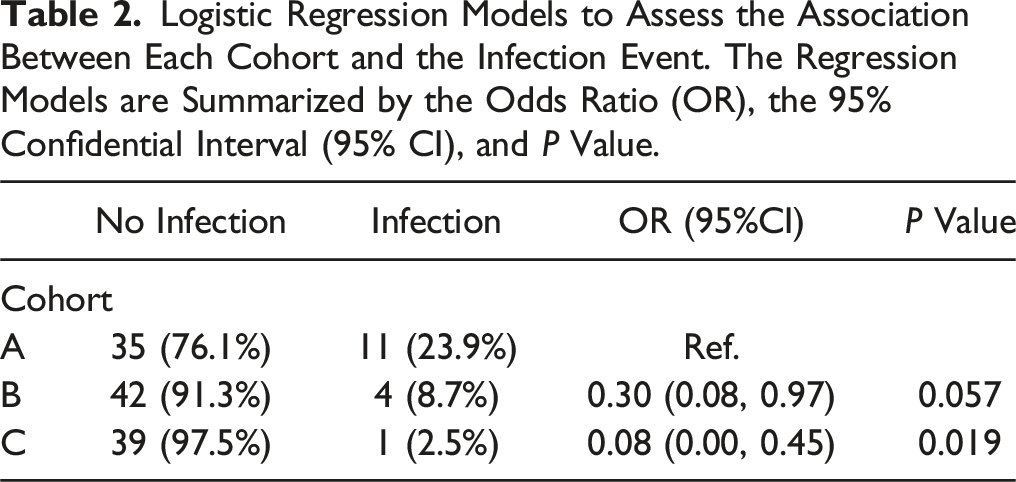
There was a significant decrease in the infection rate depending on the prophylaxis (23.9% in cohort A, 8.7% in cohort B, and 2.5% in cohort C). When logistic regression models were applied and cohorts B and C were compared with A, the following results were obtained: OR of 0.30 (CI: 0.08 – 0.97; P = 0.057) and 0.08 (IC: 0.00 – 0.45; P = 0.019), respectively.
Conclusions
Prophylaxis with prolonged double antibiotic therapy with cefazolin and amikacin is associated with a statistically significant decrease in the rate of SSI in patients with a high risk of infection.
Keywords
Introduction
Surgical site infections (SSIs) are one of the major complications in instrumented spine surgery, leading to an increase in the morbidity and mortality of patients as well as the associated costs. The rate of SSIs in this type of surgery is 1.4% - 13%; therefore, its prevention is a priority for any spine surgeon. 1
Numerous risk factors that increase the rate of SSIs have been widely described in the literature available2,3,4; consequently, surgeons are aware of the risks when dealing with different types of patients. Even though risk of SSI is much higher for some people than others, clinical guidelines on antimicrobial prophylaxis (AMP) are usually standard and common for all patients and there are no specific guidelines for high-risk patients (HRPs).
Most recommendations for AMP are based on 1-day or single-dose protocols and are aimed at the general population. However, there is no strong evidence of this efficacy.5–9 The North American Spine Society (NASS) guidelines recommend a single preoperative dose and as many intraoperative doses as may be required for uncomplicated procedures, although they recommend considering alternative prophylactic regimens for patients with comorbidities or who are undergoing complex surgery.
The aim of this paper is to determine if in HRPs the postoperative infection rate in instrumented thoraco-lumbar spine surgery is affected by AMP and to create a specific protocol for these targeted people.
Methods
The study design was carried out by a multidisciplinary committee made up of the Department of Microbiology, the Department of Preventive Medicine, and the Spinal Disorders Unit of two hospitals.
This study was approved by the Fundación Jiménez Díaz Ethics Committee (approval reference: FJD-UPC-23-01). Informed consent was not necessary to carry out this study.
This was a three-cohort study using a prospective multicentre database. We performed a retrospective analysis of prospectively collected data from patients with a high risk of SSI, who underwent instrumented thoraco-lumbar spine surgery between October 2021 and April 2023. A total of 132 patients were recruited. All the patients were included in the hospital’s database by means of a prospective and consecutive sampling process; patients were not randomised according to the type of prophylaxis received. STROBE guidelines were followed to report this study.
The inclusion criteria for determining an HRP is to meet at least two of the following criteria: (1) diabetes mellitus (DM). The criteria for diagnosing a patient with DM are HBA1c > 6.5% or fasting plasma glucose >126 mg/dL (7.0 mmol/L) or two-hour plasma glucose >200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test or, in a patient with classic symptoms of hyperglycaemia or hyperglycaemic crisis, a random plasma glucose >200 mg/dL (11.1 mmol/L); (2) obesity. Body mass index (BMI) > 30 Kg/m2; (3) revision surgeries; (4) immunodepression (immunosuppressive drugs, prolonged corticosteroid therapy, active cancer, immunosuppressive diseases, HIV infection, rheumatoid arthritis, etc.). The decision to choose these factors as criteria to determine whether a patient is at high risk of infection was based on bibliographic data (considering which factors are generally related to a higher rate of SSI) and on the authors’ clinical experience. 4
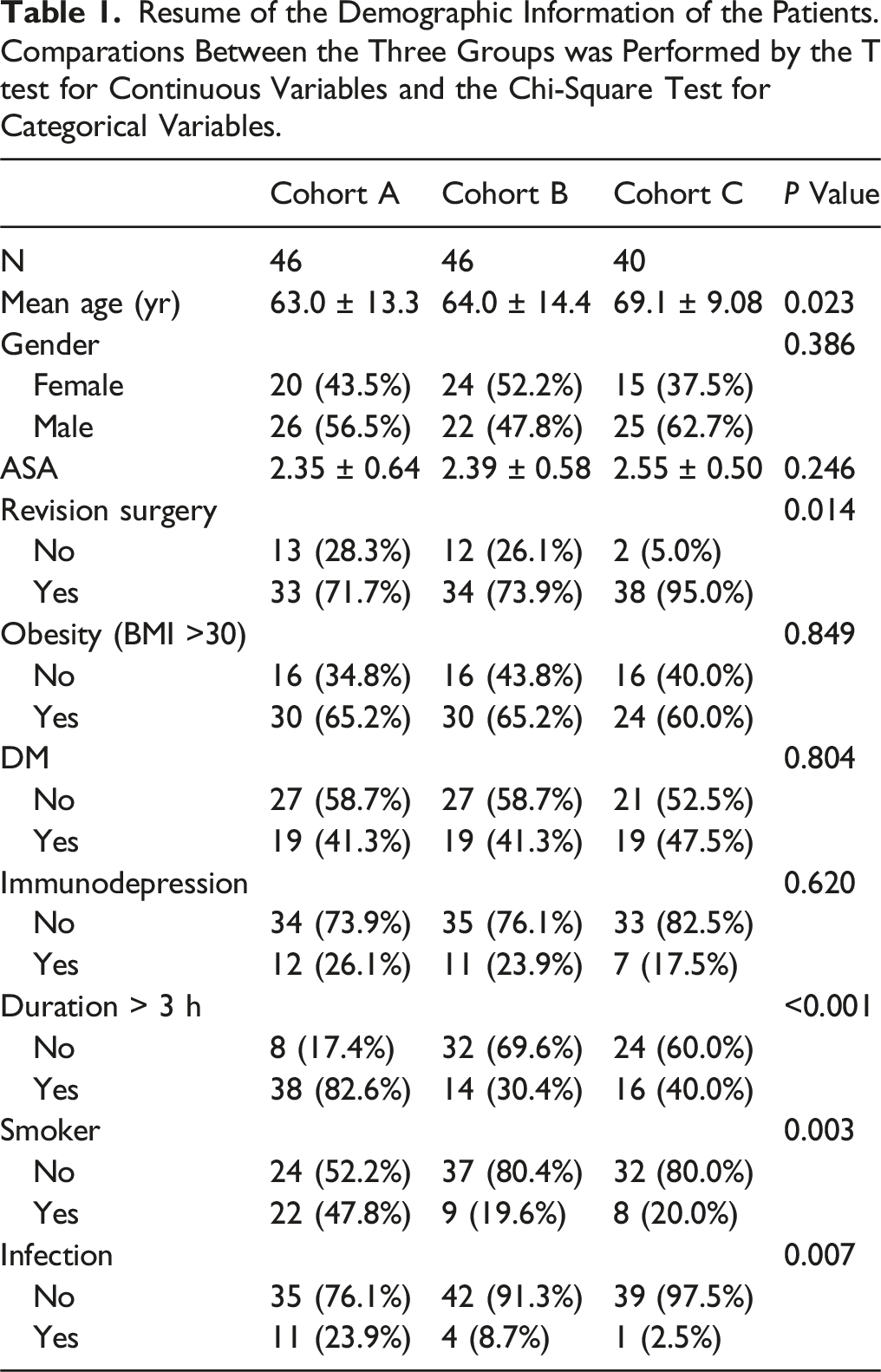
Resume of the Demographic Information of the Patients. Comparations Between the Three Groups was Performed by the T test for Continuous Variables and the Chi-Square Test for Categorical Variables.
Cohort A (46 patients) was administered AMP with intravenous (IV) cefazolin 2 g in the preoperative phase. Afterwards, we continued with the prophylaxis every 8 h for 24 h.
Cohort B (46 patients) was administered cefazolin 2g IV and amikacin 500 mg IV in the preoperative phase. The dose was repeated every 8 h for cefazolin and every 12 h for amikacin during the first 24 h.
Cohort C (40 patients) was administered cefazolin 2 g IV and amikacin 500 mg IV in the preoperative phase. The dose was repeated every 8 h for cefazolin and every 12 h for amikacin during the first 72 h.
In the three cohorts, preoperative antibiotics started within 30 minutes prior to skin incision. For prolonged surgeries, cefazolin was administered every 4 h during the procedure. In cases of allergy to cefazolin, as an alternative we used vancomycin 20 mg/kg for 24 h for cohorts A and B, and 72 h for cohort C. In patients with chronic kidney disease, the antibiotic dose was adjusted according to the glomerular filtration rate.
There was no intentional variation between the groups with respect to the surgical technique, preoperative disinfection protocol, surgical site preparation or postoperative wound care. Patients went for a routine follow-up appointment 6 weeks after they had been discharged from hospital. After that, every patient had regular follow-up appointments for at least 1 year. In the event of any wound-related issues between appointments, they were instructed to go to the ward via the Accident and Emergency Unit. Surgical site infection was diagnosed according to the definitions developed by the ECDC (European Centre for Disease Prevention and Control). 10
Statistics
Descriptive analyses were conducted using frequency distribution for categorical variables and central tendency measures for quantitative variables. Comparisons between the three groups were performed by the t test for continuous variables (age and ASA grade) and the Pearson’s chi-square test for categorical variables (gender, revision surgery, obesity, DM, immunodepression, duration of the surgical procedure > 3 h, smoker and infection).
A multiple logistic regression model was designed to obtain adjusted odds ratios (OR) with 95% confidence intervals (CIs) as estimations of the effect of the AMP regimens on SSI.
Results
The demographic information of the patients is summarised in Table 1. The mean age of our patients was 63.0 (±13.3), 64.0 (±14.4) and 69.1 (±9.08) years in cohort A, cohort B and cohort C, respectively. There was no significant difference between the cohorts regarding each variable, except for revision surgery, smoker, and duration of the surgical procedure > 3 h.
According to the statistical analysis of the study, there was a decrease in SSIs. The infection rate of cohort A was 23.9% (11 out of 46 patients), 8.7% in cohort B (4 out of 46 patients), and 2.5% in cohort C (1 out of 40 patients). There was a statistically significant difference in the number of SSIs between the three cohorts (P = 0.007) according to chi-square test. These data indicate that double-dose AMP and, to an even greater degree, prolonged double-dose AMP acts as a protective factor against SSI.
Logistic Regression Models to Assess the Association Between Each Cohort and the Infection Event. The Regression Models are Summarized by the Odds Ratio (OR), the 95% Confidential Interval (95% CI), and P Value.
Resume of Side Effects From Antibiotics.

Discussion
According to ECDC criteria, SSI is considered when it occurs at the site of the surgery within 30 days after the operation or within 90 days if the operation included placement of a foreign body, e.g. an implant. SSIs are undesired and troublesome complications after spinal surgery procedures. Reported rates of SSI vary widely and depend upon many factors. Generally speaking, the number of cases reported varies between 0.2% and 25% (although, most reports are between 2% and 5%). Indeed, spine surgery normally has a higher incidence of SSI than surgeries on another part of the musculoskeletal system.10–13
The medical, economic, and social costs of SSI are high. Whitmore et al. 14 estimated that the direct costs of SSI are $4067 per patient. Other studies suggest that the hospitalisation time of these patients increases by 6.5 days. In addition, there are indirect costs associated with the inability to work; patient satisfaction with the final clinical outcome of spine surgery is another important consideration.12,15
The main cause of SSI following operations is bacterial contamination of the surgical site during procedures. Krizek and Robson 16 demonstrated that contamination with >105 bacteria per gram of tissue significantly increased the risk of wound infection. The role of antibiotic prophylaxis is to keep the number of contaminating bacteria below a significant level to prevent infection. The concentration of antibiotics should be at the maximum when the skin is incised to control bacteria that could contaminate the wound. To achieve this, the antibiotics should be administered within 30 minutes prior to skin incision.6,17
The reported choice of AMP is varied. First-generation cephalosporin (normally cefazolin) is the most widely accepted choice in spine surgery. It is considered optimal because it is active against gram-positive species (Staphylococcus aureus is the most common bacterial isolate after SSI in spine surgery), it is relatively nontoxic and inexpensive, and it provides good soft tissue and bone penetration.5,18,19 However, in our hospital, 30% of the SSI samples we obtained were gram-negative. That is consistent with published data. Mackensie et al. 11 reported that 46.5% of SSI contained at least one gram-negative organism. From there arose the idea of associating an antibiotic that would cover this type of bacterium. After discussing it with the Department of Microbiology and the Department of Preventive Medicine, we decided to combine cefazolin with amikacin.
Despite the wide disparity of data available in the literature, it is accepted that preoperative AMP decreases the rate of SSI. However, the duration of this AMP in the postoperative phase is much discussed, and we can find very disparate data.5,6,12,18,20
The large discrepancies between AMP protocols and the SSI rate are at least partly due to differences in research methodology, types of spine surgery performed, differences between hospitals and countries, and the variability between patients (i.e. patients’ risk factors for SSI). Indeed, numerous risk factors for SSI are widely described in the literature. And, the higher a patient’s risk factor, the greater their risk of SSI. This subgroup of patients may benefit from a special AMP protocol given its high risk of SSI.2,3,8,9,12,13
Clinical guidelines on AMP are usually standard and/or common for all types of patients. There are very few protocols and studies specifically concerning HRP and yet they have the highest SSI rate. In our study, when comparing the three cohorts, the use of double AMP and, to an even greater degree, the use of prolonged double AMP is a protective factor that reduces the SSI rate. Statistically significant differences were observed when we compared cohorts C and A (P = 0.019). However, when cohort B was compared with cohort A, albeit the observation of diverse clinical conditions (OR 0.30, CI 0.08 – 0.97), the differences were at the limit of statistical significance (P = 0.057).
The reported side effects were few and reversible. We detected no increase in resistant organisms from wound cultures and no increased rates of C. difficile infection. These data are consistent with what has been described in the literature.18,21
It is important to consider the limitations of our research. As it was not a clinical trial, the main bias was the lack of randomisation between the cohorts. Indeed, the three groups were not fully comparable. The differences between hospitals and operations performed by different surgeons are also factors to consider.
Factors that are rarely considered are blood loss, blood transfusion and fluid administration, which can result in a decreased concentration of antibiotic in serum. In fact, to be effective for prophylaxis, AMP concentrations in serum, soft tissue, and bone must exceed the minimum inhibitory concentration (MIC) for a specific bacterium. The MIC must be maintained throughout the procedure in order to effectively control the bacterial burden.5,18,22,23
The lack of statistical significance between cohorts B and A can be due to the fact that our study was not adequately powered to detect differences between the groups. A large subject population would possibly prove statistical significance.
Conclusion
HRPs, due to their special characteristics, and a high SSI rate make up a separate subgroup of patients, and should be managed differently from the rest of the population.
In our study, AMP with prolonged double antibiotic therapy with cefazolin and amikacin was associated with a statistically significant decrease in the rate of SSI in patients with a high risk of infection.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.