
Abstract
Study Design:
Review article.
Objectives:
A review of literature on the epidemiology, diagnosis, and management of spinal tuberculosis (TB).
Methods:
A systematic computerized literature search was performed using Cochrane Database of Systematic Reviews, EMBASE, and PubMed. Studies published over the past 10 years were analyzed. The searches were performed using Medical Subject Headings terms, and the subheadings used were “spinal tuberculosis,” “diagnosis,” “epidemiology,” “etiology,” “management,” “surgery,” and “therapy.”
Results:
Tissue diagnosis remains the only foolproof investigation to confirm diagnosis. Magnetic resonance imaging and Gene Xpert help in early detection and treatment of spinal TB. Uncomplicated spinal TB has good response to appropriately dosed multimodal ambulant chemotherapy. Surgery is warranted only in cases of neurological complications, incapacitating deformity, and instability.
Conclusions:
The incidence of atypical clinicoradiological presentations of spinal TB is on the rise. Improper dosing, inadequate duration of treatment, and inappropriate selection of candidates for chemotherapy has not only resulted in the resurgence of TB but also led to the most dreadful consequence of multidrug resistant strains. In addition, global migration phenomenon has resulted in worldwide spread of spinal TB. The current consensus is to diagnose and treat spinal TB early, prevent complications, promote early mobilization, and restore the patient to his or her earlier functional status.
Keywords
Introduction
The existence of tuberculosis (TB) in ancient times is evident from the fact that it was observed in mummies from Egypt and Peru (9000 BC) and has also been described as “Yakshama” in the oldest Indian medical treatises of Charaka Samhita and Sushruta Samhita, dating back to 1000 and 600 BC, respectively. 1,2 In 1779, Sir Percival Pott described tuberculous spondylitis and its clinical presentation of paraplegia in patients with kyphotic deformities in European population. 3 Significant progress has been achieved in 19th and 20th centuries including the discovery of the causative agent, Mycobacterium tuberculosis, development of Bacillus Calmette-Guerin (BCG) vaccine, invention of chemotherapeutic agents, advances in diagnostics, and improvement in surgical outcomes. 4,5
Once believed to be a health burden due to its endemic nature in underprivileged sections of developing countries, TB is now an international concern, as it has its footprints spread all over the world due to the global migration phenomenon. In spite of the major strides achieved in early diagnosis and efficient management of cases over the past 4 decades, increasing prevalence of immunodeficient survivors and the emergence of multidrug resistance (MDR) has resulted in resurgence of TB as a public health menace. 6
Epidemiology
The incidence of extrapulmonary TB (EPTB) is low at 3%, but there has been no significant reduction in incidence of EPTB when compared to pulmonary TB (PTB). 7 Skeletal TB (STB) contributes to around 10% of EPTB, and spinal TB has been the most common site of STB, amounting to around half of skeletal EPTB. Thoracolumbar junction remains to be the most affected region of the spinal column followed by lumbar spine and the cervical spine. 8,9
In 2016, there was an estimated incidence of 10.4 million new TB cases as per the World Health Organization (WHO). 10 While European region contributed only 3%, the South East Asian Region alone had 46.5% of the global TB burden. 11,12 The deaths related to TB remained to be one of the top 10 causes of death worldwide, despite the decline of TB deaths by 22% from 2000 to 2015.
According to the United Nations, the number of international migrants had grown rapidly from 173 million to 244 million from 2000 to 2015. The majority of migrants belonged to middle-income countries and most of them moved to developed nations. India, which contributed to around 23% of the global TB burden, also had the largest diaspora in the world in 2015. 13 This global migration phenomenon along with emergence of MDR strains pose new challenges to the global health care system. In addition, the ever-increasing incidence of chronic debilitating medical diseases and HIV-affected individuals further portend to the resurgence of TB. 14 Consistent efforts are being taken by the WHO, and the WHO End TB Strategy for 2030 has been adopted by its member nations, which aims at 80% reduction of TB incidence rate and 90% reduction of TB deaths. 15
Pathophysiology of Spinal TB
TB is caused by Mycobacterium tuberculosis complex, which has around 60 species. Among them only Mycobacterium tuberculosis (the most common), Mycobacterium bovis, Mycobacterium microti, and Mycobacterium africanum are known to affect humans. 16 It is a slow-growing fastidious, aerobic bacillus. The primary site of infections can be in the lungs, lymph nodes of the mediastinum, mesentery, gastrointestinal tract, genitourinary system, or any other viscera. The bacilli tend to remain dormant for prolonged periods and multiplies every 15 to 20 hours in aerobic conditions whenever favorable. Spinal infection is always secondary and is caused by hematogenous dissemination of the bacillus from a primary focus. 17,18
Anatomically the intervertebral disc is an avascular structure and the paradiscal arteries split on either side of the disc and reach the subchondral region of the upper and lower endplates of each disc. This arterial supply of the vertebra favors subchondral bone involvement on either side of the disc, “paradiscal,” which is the most common type observed. 19 The other patterns of involvement are “central,” resulting in vertebral body loss; “posterior,” when posterior appendicular structures are involved; and “nonosseous abscess” formation. TB results in granulomatous inflammation characterized by lymphocytic infiltration and epithelioid cells, which may merge to form the classical Langhans-type giant cells and end up in caseating necrosis of affected tissues forming cold abscess. With progressive destruction of the vertebral body, deformation of spine causes kyphosis. 20,21
Clinical Presentation of Spinal TB
The clinical picture of spinal TB is extremely variegated. Spinal TB usually is insidious in onset and the disease progresses at a slow pace. 22 The diagnostic period, since onset of symptoms, may vary from 2 weeks to several years. The manifestation of spinal TB depends on the severity and duration of the disease, site of the disease, and the presence of complications such as abscess, sinuses, deformity, and neurological deficit. 23 Spinal TB can either be complicated or uncomplicated. In complicated TB, patients present with deformity, instability, and neurological deficit. Uncomplicated spinal TB is one in which diagnosis is made prior to development of such complications. Backache is the most common of all symptoms. During the active stage, it is primarily due to inflammation of the bone and rarely can be radicular in nature. Rest pain at the involved level is pathognomic and the intensity is proportional to the amount of bone destruction and instability. 24 Constitutional symptoms such as loss of weight, loss of appetite, fever, and malaise are more frequently associated with PTB than spinal TB. 25
Cold Abscess
Cold abscess lacks inflammatory features and initially forms in the infective focus. Later, it takes the path of least resistance along the natural fascial and neurovascular planes as depicted in Figure 1. In the cervical spine, it can present as a retropharyngeal abscess or as a swelling in anterior or posterior triangle of neck or even in the axilla. Retropharyngeal abscess can produce dysphagia, hoarseness of voice, and respiratory stridor. 26 In the thoracic region, the cold abscess usually presents as a fusiform paravertebral swelling, seen radiographically, and it can track along the intercostal vessels and presents as a swelling in the chest wall. Thoracic cold abscess can track down through the arcuate ligament, or via the openings in the diaphragm. 27 The lumbar cold abscess usually present as a swelling in Petit’s triangle or in the groin and can track down along the psoas to cause pseudo-flexion deformity of the hip. Rarely they can track femoral or gluteal vessels to present as an abscess in Scarpa’s triangle or gluteal region. 28,29
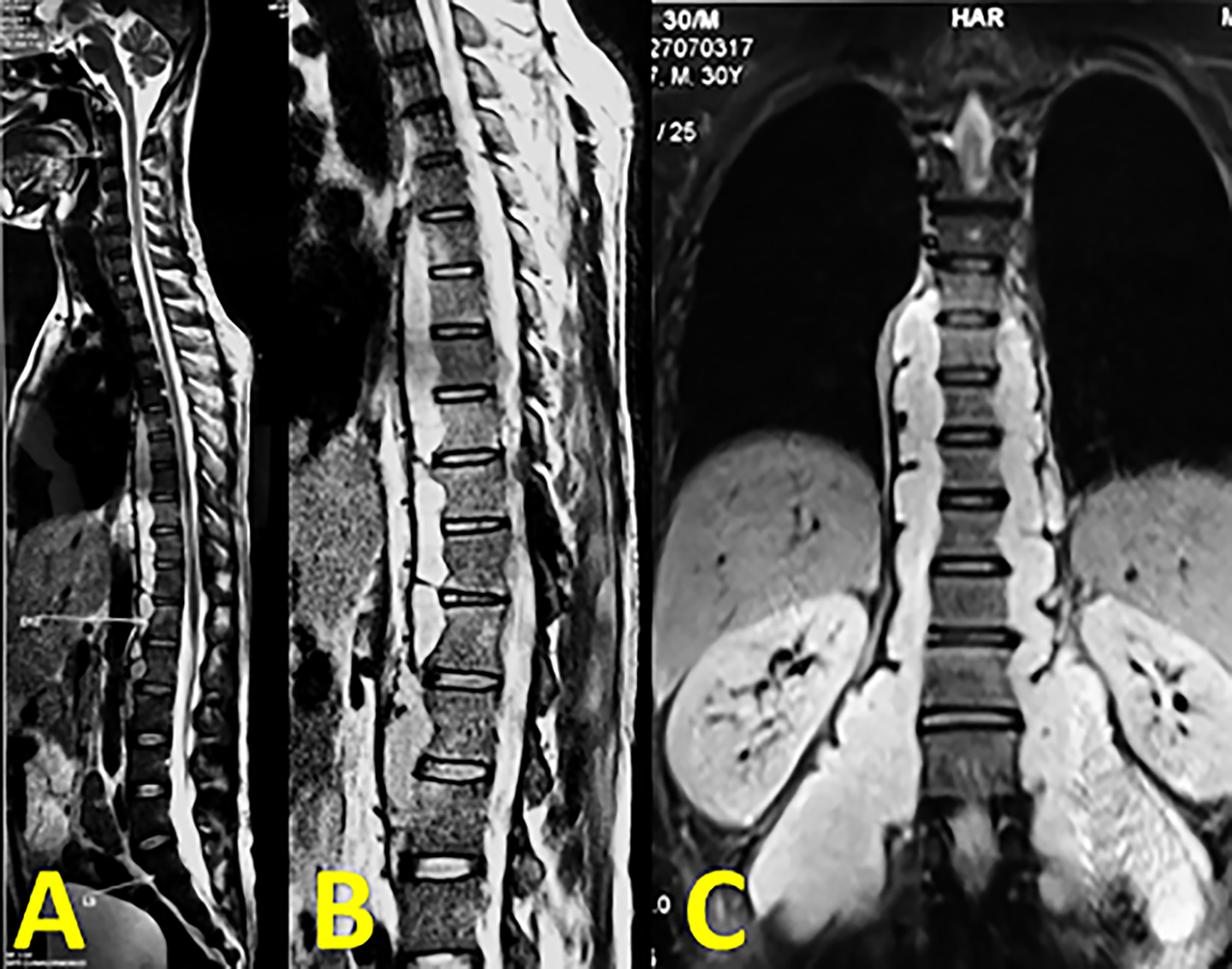
(A, B) Whole spine and focal T2 weighted sagittal MRI images of a 30-year-old individual showing unusually large prevertebral abscess with extensive tracking beneath the anterior longitudinal ligament. (C) Coronal image shows the abscess tracking along the psoas muscle to reach the anterior aspect of the thigh.
Deformity
Owing to the involvement of anterior column, progressive destruction results in kyphotic deformity of spine most often. The clinical appearance depends on the number of vertebrae involved causing “knuckle” (1 vertebra), “gibbus” (2 vertebrae), and “rounded kyphosis” (>3 vertebral collapse). Rajasekaran et al proposed a formula to predict the final kyphotic deformity in adult population affected with spinal TB: Y = a + bx, where Y is the final angle, “a” and “b” are constants, 5.5 and 30.5, respectively, and x is the initial loss of vertebral height in thoracic and thoracolumbar spine. 30 Jain et al later observed that it was possible to predict final kyphotic deformity using this formula with a variability of ±10°. 31 Jain et al believed that any kyphotic deformity of 60° or above is disabling and may increase the likelihood of developing neurological sequelae. 32 The vertebral loss is well tolerated in cervical and lumbar spine unlike thoracic and thoracolumbar spine due to the inherent lordosis. However, rarely with active ongoing infection, progressive cervical kyphosis may necessitate surgical intervention, as shown in Figure 2.
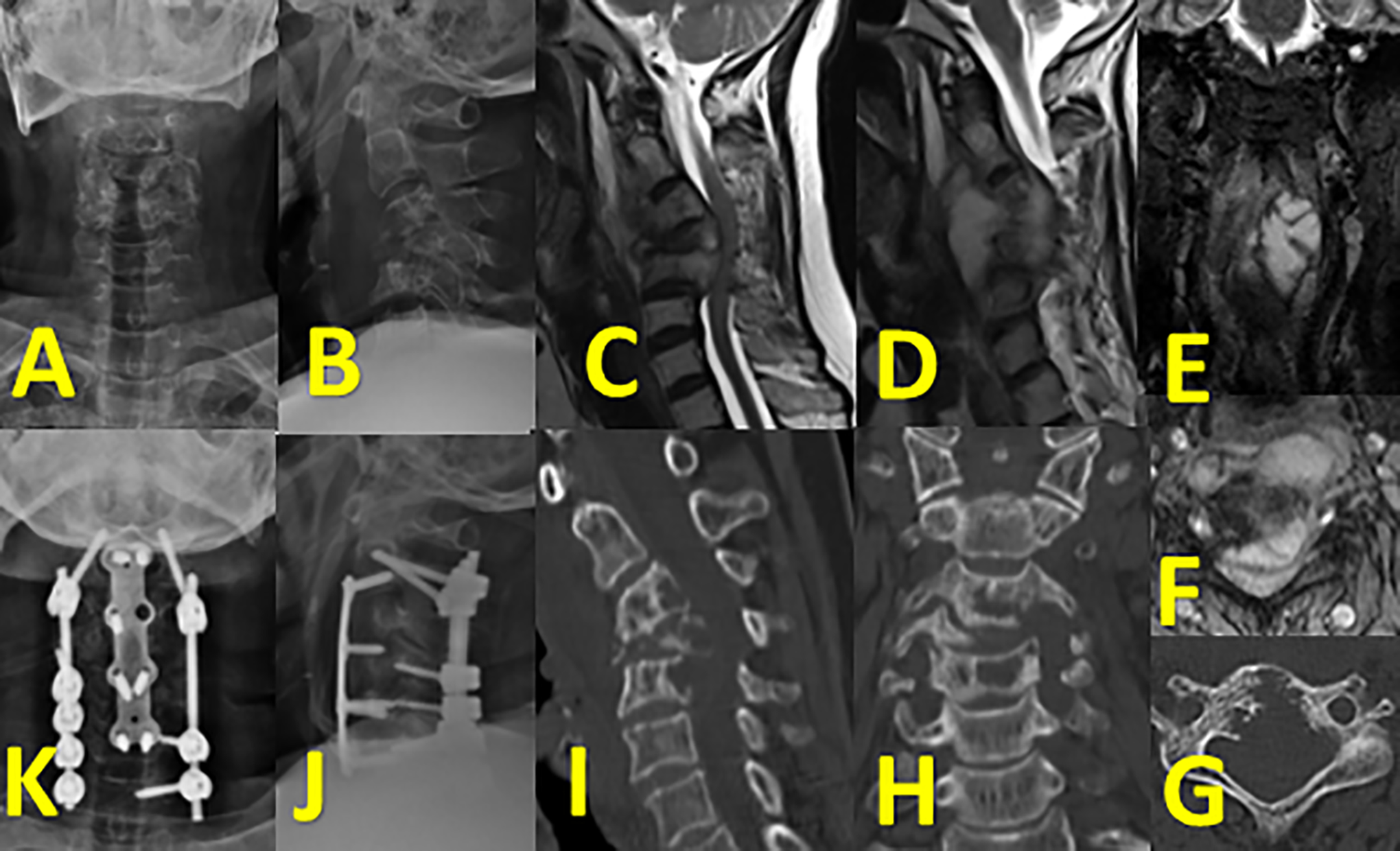
(A, B) Plain radiography of a 52-year-old female with active cervical spinal TB and cervical kyphosis. (C, D) T2 weighted sagittal and parasagittal image showing a huge prevertebral abscess and posterior abscess spreading along and confined within posterior longitudinal ligament with cord compression. (E, F) Coronal and axial trim images demonstrating asymmetrical paravertebral abscess more toward the left side. (G, H, I) Axial, coronal, and sagittal images showing fragmentary and osteolytic lesions with near complete destruction of C4 vertebra. (J, K) One-year follow-up lateral and AP X-ray following anterior corpectomy and iliac crest autografting with posterior instrumentation showing restoration of cervical lordosis and excellent healing.
Pediatric Spinal TB
The immaturity and flexibility of spine in children is the reason why they are prone to rapid and severe deformity progression following vertebral collapse. 33 In childhood TB, even after healing of the disease, deformity may progress due to the growing nature of spine. Rajasekaran described the signs of instability that he noted in a 15-year follow-up of children affected with spinal TB. The 4 “spine at risk” signs were retropulsion, subluxation, lateral translation, or toppling. 34 He suggested that children with instability score of 2 or more had disruption of the posterior facet and advised surgery in such situations. 35 One such situation, managed surgically is shown in Figure 3.
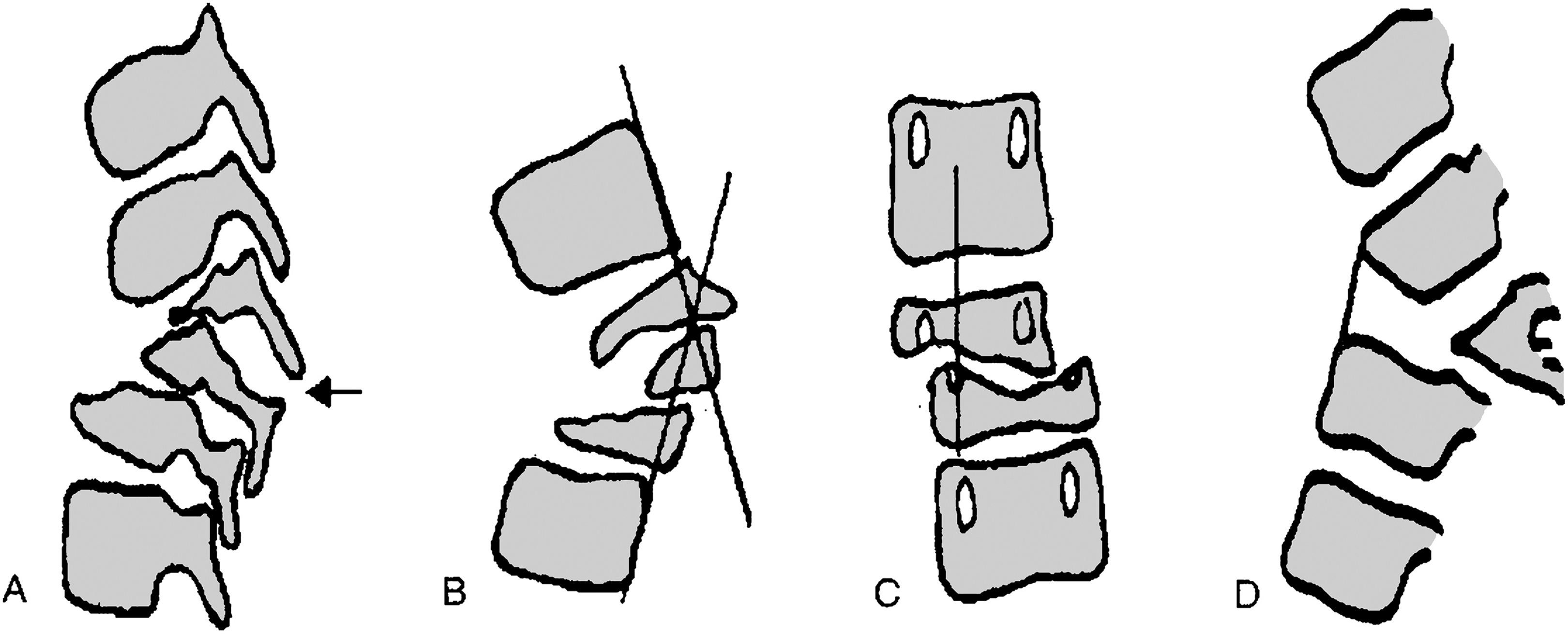
The “spine at risk” signs to identify children at risk for severe deformity include: (A) separation of facet joints in lateral radiographs which indicates instability, (B) retropulsion of the posterior part of affected vertebra, (C) lateral translation of vertebrae in the antero-posterior radiograph, and (D) toppling of one vertebra over the other vertebra. Here, a line drawn from the anterior surface of the caudal normal vertebra crosses the mid-point of the anterior surface of the cranial normal vertebra.
Neurological Deficit
Neurological complications can occur either during the early active disease or in the late healed stage. Direct compression due to abscess, inflammatory tissue, or sequestrum and instability are the usual causes for neural compromise in the active stage. 36 The mechanical stretch of cord over an internal gibbus results in delayed neurological issues even after the healing of TB. Late-onset neurological deficit due to ossification of ligamentum flavum proximal to the kyphosis is rare, but has been observed and believe to be due to exaggerated movements. 37
Atypical Spinal Tuberculosis
Patients without the typical clinical features of axial pain, constitutional symptoms, kyphosis, or typical radiological features (paradiscal) are considered as having atypical presentation. 38 Batson’s perivertebral venous plexus plays a role in skip lesions of spinal TB and is believed to be one cause for atypical presentations. Concentric vertebral collapse, isolated neural arch involvement, ivory vertebra, circumferential vertebral involvement, contiguous or skip vertebral lesions, and multifocal osseous involvement are some atypical radiographic patterns. Atypical clinical presentations such as prolapsed intervertebral disc as reported by Pande and Babhulkar, isolated cold abscess without bony involvement, and intraspinal pure soft tissue granulomas do occur. 39 Meningeal, neural, and perineural tissue involvement are rare, but easily identifiable in magnetic resonance imaging (MRI) and can cause features of compressive myelopathy without radiographic bony destruction. 40
Diagnosis
Growth of Mycobacterium in culture specimens obtained from the infected tissue is the single most confirmatory diagnostic test of spinal TB and is considered the gold standard method. However, due to its very poor sensitivity, histopathological studies demonstrating classical granulomas and staining of smears to identify acid fast bacilli (AFB) are considered as reference standards for all other diagnostic modalities. Apart from indirect serological markers of inflammation, immunological tests have also been used with varied results. Molecular diagnostics are frequently being used because of its rapidity and reliability.
Imaging
Plain radiographs have no role in early diagnosis of spinal TB. Disc space narrowing and rarefaction of vertebral end plates can be identified as the disease progresses and further destruction leading to kyphosis and instability can be made out only in late stages. It is useful in assessing coronal and sagittal alignment. Sixty percent to 70% of spinal TB may have an active pulmonary lesion, and thus chest radiography is essential. 41
Computed tomography (CT) demonstrates vertebral destruction well before plain radiographs and is extremely useful in identifying extent of bony destruction, posterior column involvement, junctional pathologies, joint involvement, and regional stability. 42 Four types of destruction have been noticed in decreasing order of frequency: fragmentary, osteolytic, subperiosteal, and localized sclerotic lesion. 43 CT is also of immense value in obtaining percutaneous CT-guided biopsy for establishing diagnosis. 44
MRI has been the imaging modality of choice as it has been able to detect earliest changes. Gadolinium-enhanced MRI further helps in differentiating TB from other causes of infective spondylodiscitis. 45,46 The extent of soft tissue involvement, spread of abscess, and neural compression are best visualized in MRI. Whole spine screening aids in identifying skip lesions (Figure 4). MRI is also of immense value in assessing the response to treatment. 47
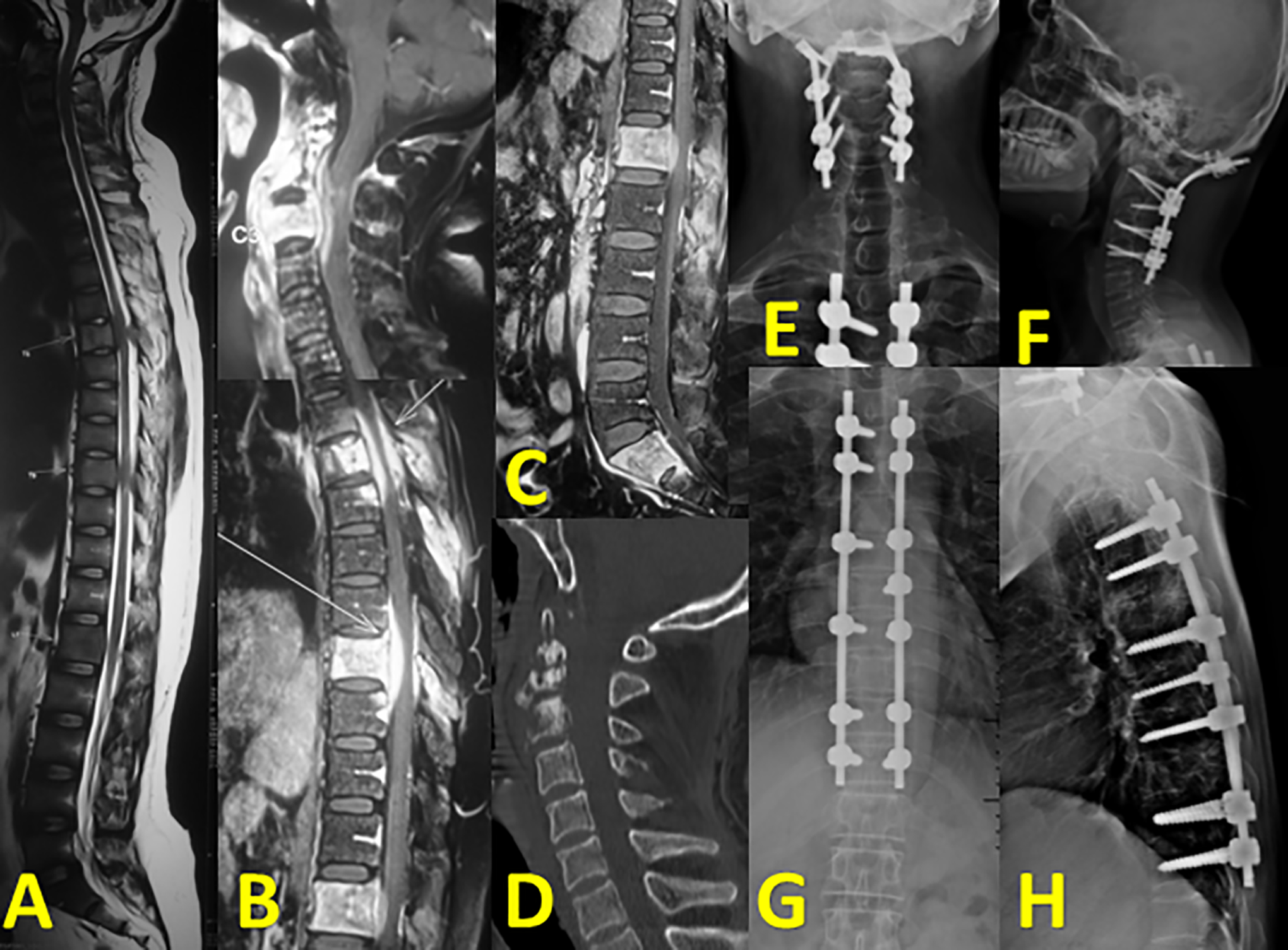
(A) Whole spine MRI screening showing multifocal lesions. (B, C) All suspected levels enhanced significantly with smooth uniform rims after contrast administration suggestive of TB. (D) Sagittal CT image with severe destruction of C1 and C2. (E, F) 1-year follow-up AP and lateral radiographs following occipitocervical stabilization. (G, H) Posterior thoracic stabilization done at the same stage.
Nuclear imaging by 18F-fluorodeoxyglucose (18F-FDG) labelled positron emission tomography (PET) scan helps in real-time assessment of disease activity, compared with CT and MRI, as 18F-FDG is known to accumulate in inflammatory cells such as neutrophils and activated macrophages at the site of inflammation. 48 However, none of the imaging options are reliable in distinguishing spinal infection and neoplasm, making histopathological examination mandatory to confirm the diagnosis or at least rule out neoplasm. 49
Laboratory Investigations
Erythrocyte sedimentation rate (ESR) is a sensitive marker of infection and can be used to monitor therapeutic response, but its low specificity is a concern. Usually in TB, ESR is >20 mm/h and decreases as healing progresses. C- reactive protein (CRP) is more specific for acute infection rather than TB. 50,51 Serological examination of IgM and IgG levels, which are high in active and chronic infective stages of TB, respectively, would not be able to differentiate between active and healed disease or between natural infection and BCG vaccinated individuals; thus, they are not recommended. 52,53
Though the WHO recommends usage of Mantoux tuberculin skin test in low-income countries, it is of no diagnostic value in endemic areas and may also be false negative in immunodeficient individuals and hence is of some use only in latent TB. Two other tests used in latent TB are interferon-γ (IFN-γ) release assays and whole blood-based enzyme-linked immunosorbent assays, measuring the amount of IFN-γ produced in response to Mycobacterium tuberculosis antigens. 54 Though they are specific and differentiate between natural TB and BCG vaccination, these tests cannot differentiate between latent TB and active TB. 55,56 The WHO has urged countries to ban inaccurate and unapproved blood tests and instead rely on accurate microbiological or molecular tests. 57
The significance of tissue diagnosis is well established and it would be ideal to subject tissue samples obtained to AFB staining, AFB culture and aerobic culture along with antibiotic sensitivity testing by line probe assays, polymerase chain reaction (PCR), and other molecular diagnostic tests apart from histopathological examination. 58 BACTEC radiometric culture takes 2 weeks, less than the 4 weeks of incubation time in standard AFB culture techniques. 59 Gene Xpert MTB/RIF test is a fully automated diagnostic test that yields results as early as 90 minutes, and has a sensitivity of 95.6% and specificity of 96.2%. 60,61 In addition, it also aids in identifying resistance to rifampicin.
In March 2017, the WHO recommended the use of a next-generation Xpert MTB/RIF assay, named Xpert MTB/RIF Ultra, as they found it, to have better detection rates of Mycobacterium tuberculosis in specimens with low numbers of bacilli, especially in smear-negative, culture-positive specimens, in pediatric specimens and in extrapulmonary specimens. 62 The classical histological features of TB are the presence of caseative necrosis, epithelioid cell granuloma, and Langhans giant cells and have been reported in around 72% to 97%. 63,64 To summarize, the diagnosis of spinal TB is based on correlating clinical and classical imaging findings on MRI and is confirmed by either culture and sensitivity, Gene Xpert PCR test, or by histopathological evidence. The diagnostic battery of investigation currently available and its usefulness in diagnosing or monitoring spinal TB is listed in Table 1 along with their reported sensitivity and specificity.
The Diagnostic Investigations Commonly Used in Spinal Tuberculosis.
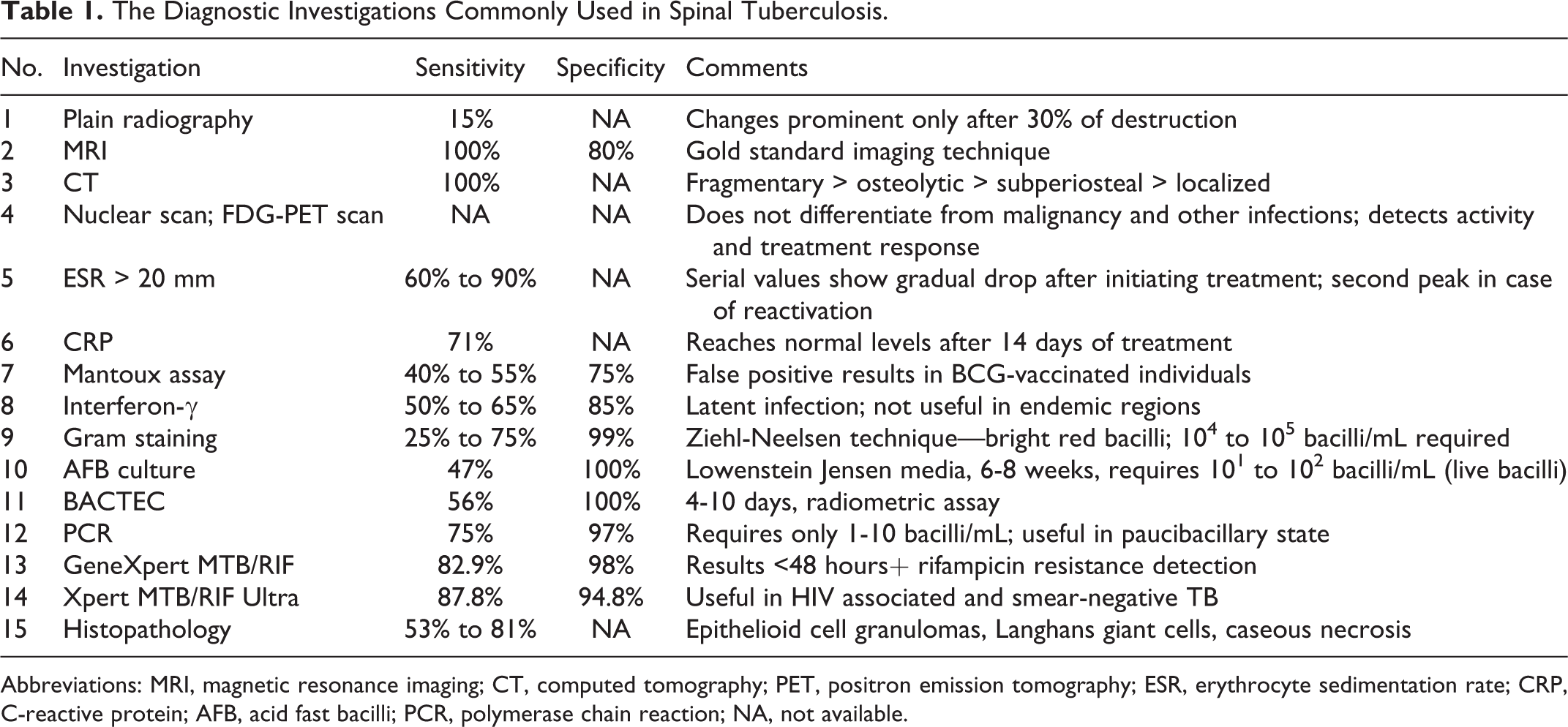
Abbreviations: MRI, magnetic resonance imaging; CT, computed tomography; PET, positron emission tomography; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; AFB, acid fast bacilli; PCR, polymerase chain reaction; NA, not available.
Management of Spinal TB
Chemotherapy
Multidrug antitubercular treatment (ATT) is the mainstay of treatment in both complicated and uncomplicated TB. 65 -68 Multidrug ATT is essential, as varying categories of bacilli exist in a lesion. They may exist as intracellular, extracellular, dormant, or rapidly multiplying forms and each has different growth and metabolic properties. 69 In addition, multidrug ATT reduces instances of drug resistance. 70 The duration of chemotherapy for spinal TB has been long debated, and the WHO recommends 9 months of treatment where 4 drugs—isoniazid, rifampicin, pyrazinamide, ethambutol, or streptomycin—are administered in the “initiation” phase for 2 months, followed by isoniazid and rifampicin for 7 months in the “continuation” phase. Again there is controversy over superiority of “daily dose” regime over alternate day “intermittent regime.” 71
The second-line ATT drugs (kanamycin, amikacin, capreomycin, levofloxacin, etc) have to be used judiciously as they have more side effects and are expensive than the standard first-line ATT drugs (isoniazid [INH], rifampicin, ethambutol, pyrazinamide). 72 A 2013 meta-analysis of both clinical trials and observational studies did not find any difference between Directly Observed Treatment, Short Course (DOTS) and self-administered therapy. 73 However, the WHO and all other TB programs continue to use DOTS as an important strategy in fear of drug resistance. 74 Uncomplicated spinal TB is a medical disease and can be effectively managed by chemotherapy alone, as evident in Figure 5. However, in patients with complicated TB, the combination of medical therapy and surgery will yield optimum results. 75
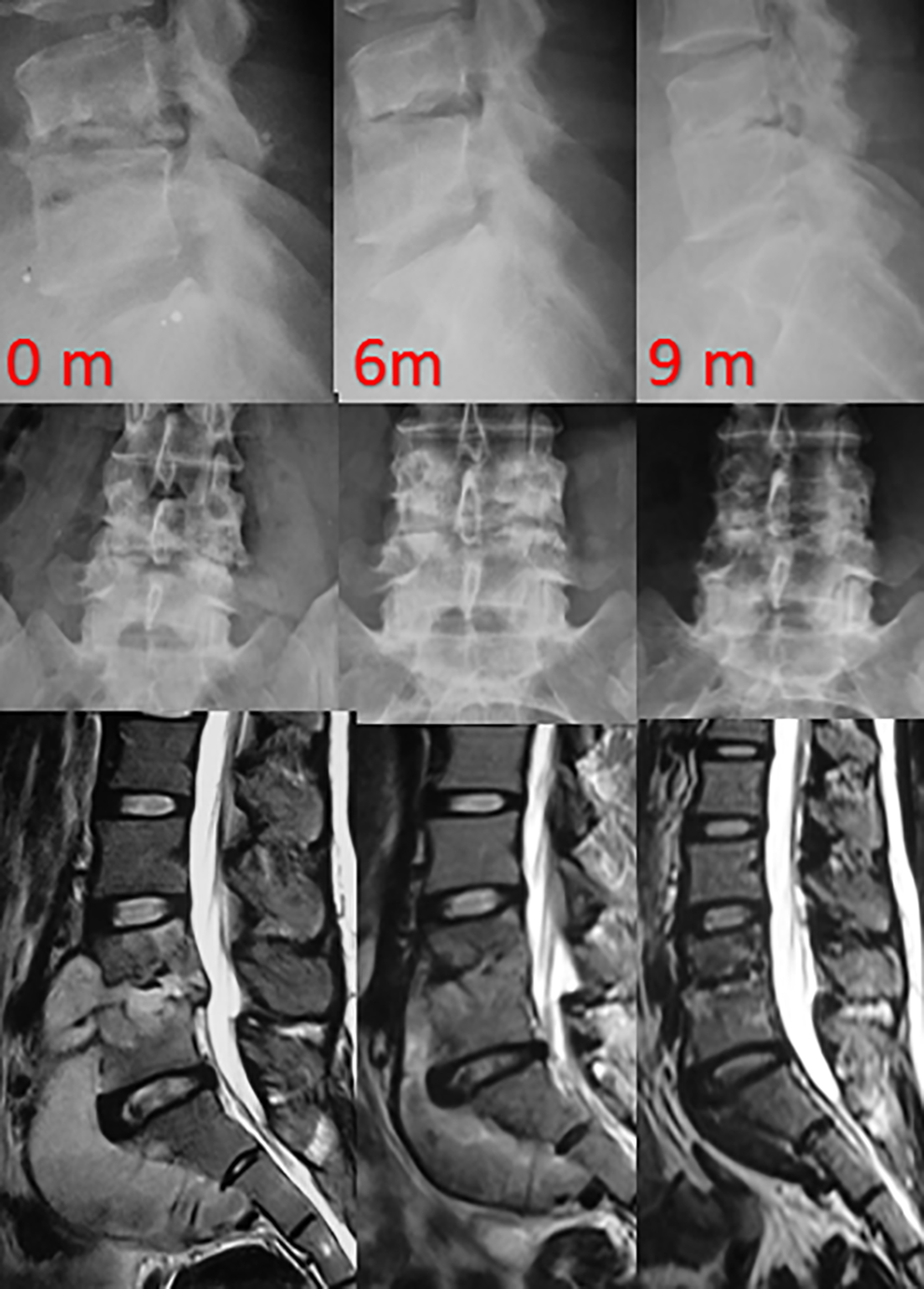
Serial radiographs and MRI images showing good progressive bony healing and complete resolution of cold abscess after receiving 9 months of ambulatory chemotherapy alone.
Drug-Resistant TB
MDR-TB is that which is resistant to INH and rifampicin. Primarily it occurs because of improper treatment, but resistant strains can also be communicable. Extensively drug-resistant TB (XDR-TB) is when there is resistance to INH and rifampicin, along with resistance to any fluoroquinolone and at least one injectable second-line anti-TB drugs. 76,77 Pawar et al suggested the following 5 predictors for successful outcome in MDR-TB: (1) progressive clinical improvement at 6 months following chemotherapy, (2) radiographic improvement during treatment, (3) disease with strains that are resistant to less than 3 ATT drugs, (4) use of less than 4 second-line drugs in treatment, and (5) no changes of regimen during treatment. 78 In 2009, the term “totally drug-resistant tuberculosis” (TDR-TB) for TB strains that showed in vitro resistance to all first- and second-line drugs tested was proposed by Velayati et al. 79 It would be more appropriate to get an opinion or refer such cases to an infectious disease specialist who is ought to have more experience in treating these resistant strains. Currently, new strategies and drugs (eg, delamanid, bedaquiline, SQ109, and sutezolid) are under trial to tackle these strains, which have been reported from India, Iran, Italy, and South Africa. 80,81
Surgical Management
Anterior debridement and radical excision of the disease foci along with ATT therapy was the choice of treatment initially, in spite of the associated high morbidities. 82,83 The Medical Research Council after randomly subjecting spinal TB patients to chemotherapy alone, debridement, and radical debridement along with fusion found out similar functional outcomes in all 3 groups. 84 Encouraged by excellent outcomes of multidrug ATT, Tuli introduced the “middle path” regime, where chemotherapy is the fundamental treatment and surgery was advocated only in certain scenarios. 85 This concept is widely accepted and practiced. Certain situations necessitating surgical management are as follows: lack of response to chemotherapy or recurrence, severe weakness at presentation, and static or worsening neural deficit even after initiating chemotherapy, instability, incapacitating pain, and deformities. 33
The advantages of surgical treatment include adequate sampling for histological confirmation of the diagnosis, early and better healing by removal of the disease focus, correction and prevention of the spinal deformity, reducing the rates of recurrence, and promoting early neurological recovery. Oga et al showed that tubercle bacilli, unlike pyogenic organisms, do not adhere to metal or form any biofilm and therefore surgical instrumentation is safe even in active disease. 86 The fundamentals of surgical management are adequate decompression and debridement, maintenance and reinforcement of stability, and correcting the deformity or halting the progress of deformity. 87
The surgical objectives are (1) abscess drainage, (2) debridement of the infected material, or (3) debridement and fusion with or without stabilization. 88 Chemotherapy alone resolves majority of the cold abscesses, and drainage is recommended only in certain scenarios such as respiratory distress or dysphagia, due to a large cervical paravertebral abscess and pseudo–hip flexion deformity due to a large psoas abscess. 26 Debridement alone does not prevent progression of deformity or improve healing rates, especially in children as it may lead to physeal damage and rapid deformity progression. 89,90 Debridement and fusion with or without instrumentation is performed by anterior approach, posterior approach, global reconstruction through posterior approach, or combined procedures.
Anterior Approach
Spinal TB mainly affects anterior column and thus anterior approaches enable adequate exposure, debridement, and reconstruction with ease. 91 Since anterior debridement alone failed to prevent deformity progression, Hodgson et al advocated radical debridement and arthrodesis. 91 -93 However, these results were not reproducible in other studies and were associated with respiratory failure, mortality, and graft-related complications. Rajasekaran in his study observed graft slippage, fracture, absorption, or subsidence in 59% of cases with anterior body fusion without instrumentation and these complications were common when the graft spanned 2 or 3 vertebral bodies. Addition of anterior instrumentation in the form of plates, rods, and screws is essential especially when significant kyphosis correction has been attempted. 94,95 Anterior procedure is recommended when posterior structures are intact, and are best avoided in panvertebral disease.
Posterior Approach
Nowadays posterior procedures are the most commonly performed, due to ease, familiarity of approach, and the lesser learning curve involved. The ability to achieve adequate exposure for circumferential spinal cord decompression, better deformity control through pedicle screws (Figure 6), and possibility of extension of instrumentation whenever required in addition to avoidance of thoracotomy-related complications through posterior approach is encouraging. 96 Transpedicular decompression and posterior instrumentation facilitates faster recovery and also prevents deformity progression and neurological sequelae in early disease. 97
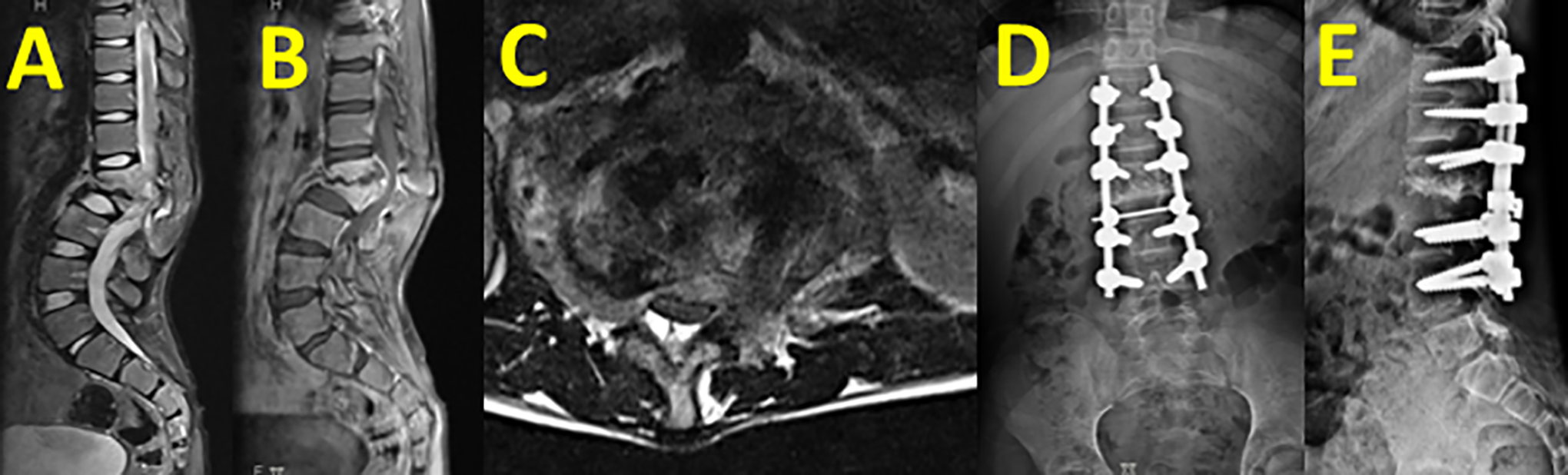
(A, B, C) MRI images of a 40-year-old with active TB and regional kyphosis with severe canal stenosis. (D, E) 1-year follow-up after posterior column shortening and decompression along with fusion procedure employed to achieve deformity correction by posterior approach alone.
Global Reconstruction by Posterior Alone Approach
Nowadays, global reconstruction is being advocated through posterior approach alone (Figure 7). Several posterior and posterolateral approaches have been described in the thoracic and lumbar spine where the anterior and lateral column can be reached safely. 98,99 They can be transpedicular, transfacetal, costotranversectomy, or extrapleural approaches. 100,101 Though transpedicular and transfacetal approaches can be used with ease in lumbar spine, reconstruction could be a challenge in thoracic spine without performing costotranversectomy. This approach is an extrapleural approach that allows decompression of spinal cord under direct vision and also allows placement of structural support anteriorly. 102 It can be done either by a posterior midline incision or with a T-shaped incision. 103
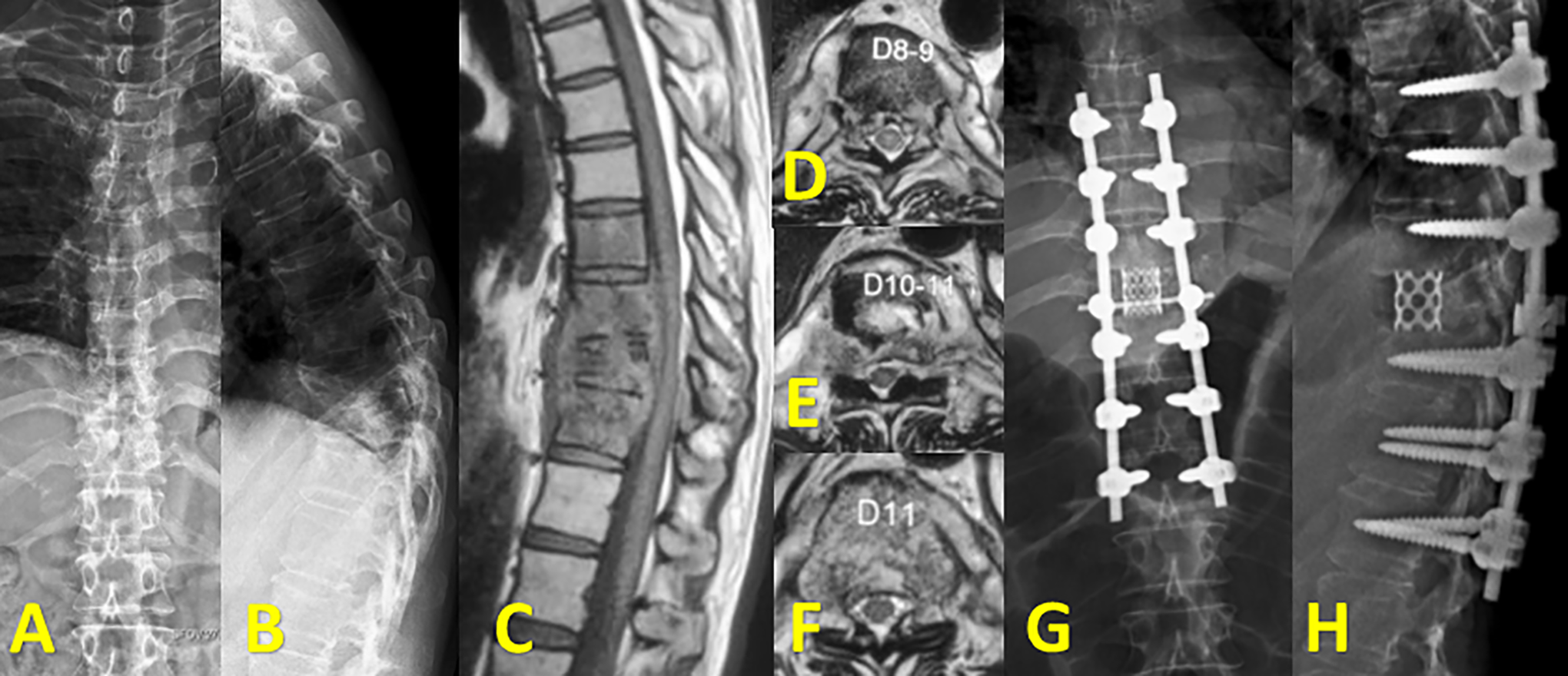
(A, B) AP and lateral radiographs of thoracolumbar spine with complete collapse of T10 vertebra resembling “vertebra plana.” (C, D, E, F) Sagittal and axial T2 weighted images of spine showing contiguous involvement of T8, T9, T10, and T11 with prevertebral abscess and concentric collapse of T10 vertebra. (G, H) AP and lateral postoperative radiographs following global anterior reconstruction through posterior-only approach.
Combined Approach
The combined approaches play a vital role especially in osteoporotic bones, multiple vertebral body involvement, and in severe kyphotic deformities. 104 Posterior instrumentation with anterior decompression and fusion can be performed in 1 or 2 stages. Anterior debridement removes infected foci and allows for direct neural decompression and rigid anterior reconstruction. Posterior instrumentation enables better deformity correction and reduces the stress on grafts placed anteriorly, thus helping in maintaining sagittal deformity correction. 105 However, due to the high associated morbidities, combined approaches are reserved only in severe destructive lesions and junctional pathologies that are inherently unstable. 106
Minimally Invasive Surgery
Recently, minimally invasive surgery (MIS) has been used either as stand-alone or in combination with open procedures. 107,108 The MIS procedures include thoracoscopic debridement, posterolateral endoscopic debridement, and MIS transforaminal interbody fusion. 109,110 Successful outcomes have been reported; however, their role in cases with severe neurological deficits and extensive osseous destruction is questionable.
Surgery in Healed Tuberculosis
Chemotherapy alone cures spinal TB; however, around 3% to 5% of cases progress to ≥ 60° kyphosis, requiring surgery. 111 Anterior procedures can be successfully employed in healed TB, but it becomes difficult to approach the apex of the curve in severe deformities. 112,113 Combined approaches employ anterior corpectomy, posterior shortening, and instrumentation and anterior and posterior grafting. 114,115 Due to the excess surgical duration, blood loss, and other morbidities, they are best avoided in moderate deformities. The options for posterior deformity correction procedures are transpedicular decancellation procedures, pedicle subtraction osteotomy and posterior closing wedge osteotomy, posterior vertebral column resection, and closing opening wedge osteotomy. 115 -117 Rajasekaran et al, in a series of 17 patients, reported that the average kyphosis improved from 69.2° preoperatively to 32.4° postoperatively by closing opening wedge osteotomy. 115,118
The surgical management of spinal TB should be tailored individually to achieve required outcomes. The factors to be taken into consideration are the age of the patient, location of the bony lesion, presence of medical comorbidities, severity of kyphosis, number of levels affected, region of the spine involved, and experience and preference of the surgeon. The recent trend is for all posterior global reconstruction in the thoracic and lumbar spine; however, anterior debridement and fusion remains the standard of care in lower cervical TB. Combined procedures becomes invaluable in patients with large vertebral defects involving 2 to 3 vertebrae, revision surgeries, and in thoracolumbar TB. 119
Conclusion
In spite of the advancements made in early diagnosis and effective management, spinal TB continues to haunt medical professionals especially in South East Asia due to parallel rise in drug-resistant strains. In addition, global migration phenomenon has now opened up the doors for this communicable disease in developed countries and the constant raise in survivors of chronic medical diseases, and HIV-infected individuals pose them at a high risk for clinically symptomatic disease as they are immunodeficient. The goals of treatment in spinal TB are to eradicate the disease and to prevent and/or correct spinal deformity and neurological deficits. Uncomplicated spinal TB is purely a medical disease. Surgery in spinal TB is directed toward achieving adequate decompression and debridement, maintenance, and reinforcement of stability and halting the progress of deformity or finally correcting the deformity in healed disease. The unrelenting efforts of the WHO and the improved compliance to multidrug chemotherapy bear credence to this amelioration and has paved way in reducing relapse rate to about 2%.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Supplement was supported by funding from AOSpine North America.