
Abstract
Study Design:
Retrospective upright MRI study.
Objective:
To validate the presence of positive and negative nerve root sedimentation signs on multi-positional MRI in the upright position and explore the relationship between negative nerve root sedimentation and gravity.
Methods:
T2-weighted axial multi-positional images in the upright position at the intervertebral disc levels from L1–L2 to L4–L5 in 141 patients with non-specific low back pain were retrospectively assessed. A positive sedimentation sign was defined as the absence of nerve root sedimentation or the absence of dorsal conglomeration of nerve roots within the dural sac. A negative sedimentation sign was defined as nerve root sedimentation dorsally or dorso-laterally like a horseshoe. Intra-and inter-observer reliability was evaluated. The relationship between sedimentation sign and dural sac cross-sectional area (CSA), anterior-posterior (AP) diameter was also explored.
Results:
The kappa value of intra-observer reliability was 0.962 and inter-observer reliability was 0.925. Both positive and negative sedimentation signs did appear at all 4 lumbar levels, including L1/2, L2/3, L3/4 and L4/5. A positive sedimentation sign was associated with significantly decreased dural sac CSA and AP diameter at L2/3, L3/4 or L4/5 level when compared to negative sedimentation sign.
Conclusions:
Both negative and positive sedimentation signs appeared at the L1/2, L2/3, L3/4, and L4/5 levels on the upright MRI, which suggested that the presence of nerve roots sedimenting dorsally in patients may not be associated with gravity. Moreover, the current study supports that sedimentation signs on multi-positional MRI images could have the same diagnostic functions as on MRI images.
Keywords
Introduction
Nerve root sedimentation sign was first described by Barz et al. 1 in 2010 and was easily observed on supine MRI axial views. A positive sedimentation sign is defined as the absence of sedimented nerve roots and is seen when the majority of nerve roots are located ventrally or centrally within the dural sac. In contrast, a negative sedimentation sign is seen when the majority of nerve roots lie dorsally in the dural sac. 1
Since the discovery of this sign, several studies have demonstrated the high sensitivity and specificity of the sedimentation sign for severe lumbar spinal stenosis (LSS).2-5 This sign is most often present in stenotic patients who need surgery. 6 A positive sedimentation sign may change to a negative sign following adequate surgical decompression of stenotic lumbar levels. 7 However, a persistent positive sign post-surgery may indicate inadequate decompression or surgical complications, such as a dural cyst. 7
There are few reports on the mechanism of the sedimentation sign formation. Gravity was thought to be responsible for the dorsal sedimentation of nerve roots (a negative sedimentation sign) in patients with no suspected LSS. 1 A positive sedimentation sign might be due to increased epidural pressure at the stenotic level, where inside the dural sac, the nerve roots are tethered centrally or ventrally, hence inhibiting the gravity-caused nerve sedimentation. 8 However, the exact mechanism of this sign still needs exploration.
In contrast to a supine MRI, in a multi-positional MRI a neutral, flexion, and extension image are taken while the patient is upright. 9 In the upright position, gravity creates a force in the superior to inferior direction, which differs from the anterior to posterior direction of force when a conventional MRI is taken in the supine position. Therefore, if gravity is the cause of a negative sedimentation sign in non-stenotic patients, sedimented nerve roots should not be seen in patients in the upright position. The aim of this study was to validate the presence of positive and negative nerve root sedimentation signs on multi-positional MRI in upright position. This will allow us (1) to better understand the mechanism of sedimentation sign and (2) to evaluate its eligibility as a valuable additional diagnostic test for LSS on images taken with upright positions.
Materials and Methods
Patient Population
Approval by the USC institutional review board was obtained prior to the beginning of this study. Lumbar multi-positional MRI images of 1320 patients referred for back pain with or without radiculopathy between September 2018 and June 2019 were evaluated. Patients aged 60 or older were included in the study. The exclusion criteria were previous history of spine surgery, infection, trauma, congenital anomaly, tumor, and inflammatory diseases of the spine. 141 consecutive patients (64 females, 77 males) with a mean age of 65.4 ± 5.1 years (range 60-80 years) were included in this study.
Multi-Positional Magnetic Resonance Imaging
Multi-positional MRI of the lumbar spine was performed using a 0.6-Tesla MRI machine (Upright Multi-Position, Fonar Corp., New York, NY, USA). The MRI unit uses a vertical orientation of the 2 opposing magnet doughnuts, allowing scanning of the patient in an upright, axially-loaded position. The imaging protocol included T1-weighted images (repetition time 671 milliseconds, echo time 17 milliseconds, thickness 4.0 mm, field of view 30 cm, matrix 256_224, NEX 2) and T2-weighted fast spin echo images (repetition time 3,000 milliseconds, echo time 140 milliseconds, thickness 4.0 mm, field of view 30 cm, matrix 256_224, NEX 2). T2-weighted axial images with patients scanned in neutral position were selected for analysis in this study.
From 3 slices of T2-weighted axial images at each lumbar intervertebral disc level between L1/2 and L4/5, mid-slice T2-weighted axial images were identified. Disc levels instead of mid-vertebral or pedicle levels were used to assess sedimentation sign because the disc level axial MRI images usually could demonstrate the most severe stenosis including structural changes such as disc degeneration, hypertrophy of ligamentum flavum and facet joints.10,11 Compared with Barz’s method of assessing the sedimentation sign at a level above or below the maximal stenosis, the current study assessed the sedimentation of nerve root at each disk level because we focused primarily on the presence of nerve root sedimentation between L1/2 and L4/5 to explore the mechanism behind the sedimentation phenomenon. Also, clinically for the diagnosis of LSS, the anterior-posterior (AP) diameter and cross-sectional area of dural sac, 12 are both measured at disc level.13,14 A total number of 564 T2-weighted axial images was evaluated for this study. L5/S1 disc level was not assessed because evaluation of this sign at L5/S1 would be misleading, according to Barz et al., 1 since S1 and S2 nerve roots leave the dural sac in a ventral position, which inhibits the dorsal sedimentation.
In the current study, a negative sedimentation sign was defined as the majority of nerve roots being located in the dorsal part of the dural sac, except 2 ventral exiting nerve roots (Figure 1A) 1 at the intervertebral disc level. In addition, nerve roots lying dorsally and laterally like a horseshoe were also identified as a negative sedimentation sign in the current study because this pattern complied with the definition of negative sign in the study done by Mannion et al. 11 showing this pattern indicated no stenosis (Figure 1B). A positive sedimentation sign was defined as an absence of nerve root sedimentation, with the majority of nerve roots located centrally (Figure 1C), ventrally (Figure 1D) or conglomerated (Figure 1E) in the dural sac. 1 A positive sedimentation sign could be subclassified into positive with room (empty space apparent in the dura sac, Figure 1C and D) and positive without room (no empty space in the dura sac, Figure 1E).2,15 This positive sedimentation sign classification has been used by Tomkins-Lane et al. 2 and Ko. 15 To explore the relationship between nerve root sedimentation sign and lumbar stenosis, 2 quantitative parameters, including dural sac cross-sectional area (CSA) and dural sac AP diameter were measured. CSA was measured with the method of Fazal et al. 6 using Image J Software (version 1.8, U.S. National Institutes of Health, Bethesda, Maryland, USA), while AP diameter was measured with the method of Fazal et al. 6 using the Lifetrack medical system (version 2, Lifetrack Medical Systems Pte. Ltd., Singapore, Singapore). Each parameter was measured twice by 2 researchers, the mean values were used for analysis.

Representative T2-weighted multi-positional MRI axial images to show a negative or positive sedimentation sign. (A) Negative. Nerve roots sediment dorsally. (B) Negative. Nerve roots lie dorsally and laterally in the dural sac like a horseshoe. (C) Positive. majority of nerve roots lie centrally. (D) Positive. Majority of Nerve roots lie ventrally. (E) Positive. Nerve roots and dural sac conglomerates, there is no empty room.
To determine the intra- and interobserver reliability of sedimentation sign, middle disc T2-weighted axial images were assessed by 3 researchers. Before the study rating, a set of 5 classic images (Figure 1A-E) was completed by each researcher. These images were then discussed among the researchers. Following the 5 test images, 20 patients with a total of 80 images were selected randomly from the 141 patients and assessed by 2 of the researchers twice with an interval of 2 weeks.
Statistical Analysis
The Chi-square test was used to evaluate the difference regarding the number of positive and negative sedimentation sign among different disc levels. The independent student t-test was used to evaluate the difference in dural sac CSA and AP diameter between positive and negative sedimentation signs. To assess the intra- and interobserver reliabilities, Cohen kappa values were calculated. All analyses were performed using SPSS computer software 21.0 (IBM Corp., Chicago, IL, USA) and a P-value < 0.05 was considered as statistically significant.
Results
Based on the randomly selected 20 patients with a total of 80 T2-weighted axial images, the intra-observer reliability was 0.962 and inter-observer reliability was 0.925.
Both positive and negative sedimentation signs were seen at levels L1/2, L2/3, L3/4 and L4/5 (Table 1); there was significant difference among 4 levels (χ2ᵪ2 = 10.680, P = 0.014). Positive sedimentation signs were most present at L4/5 (n = 50) and least present at L2/3 (n = 29) (Table 1).
Distribution of Sedimentation Signs at Disc Level from L1/2 to L4/5.

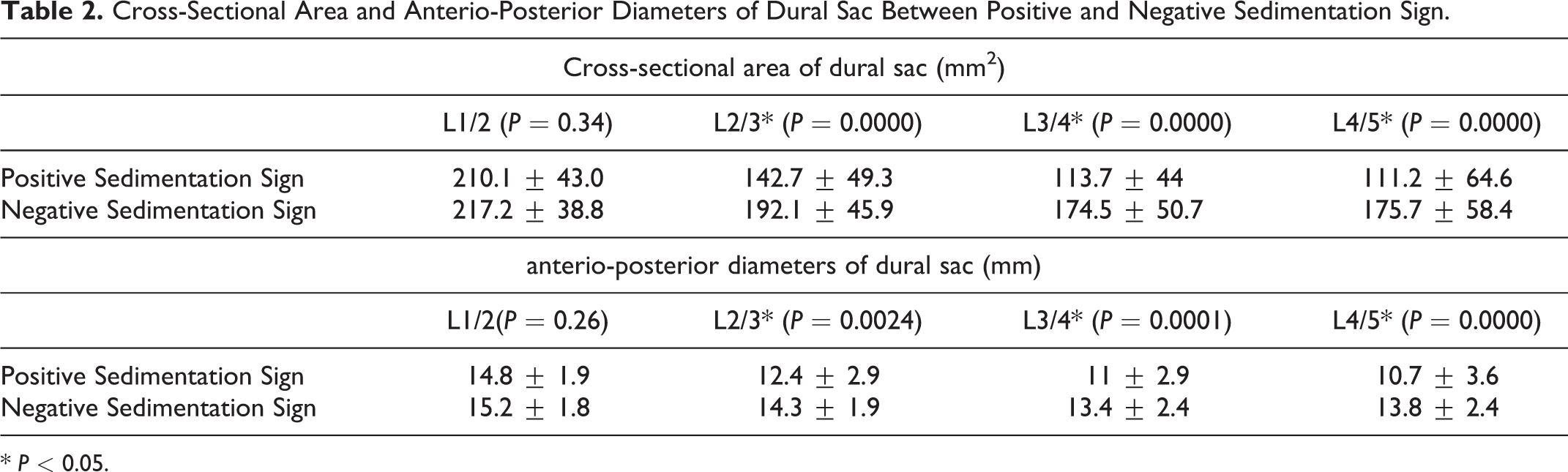
Compared to negative sedimentation sign, positive sedimentation sign was associated with a significantly decreased dural sac CSA at L2/3 (average from 192.1 ± 45.9 mm2 to 142.7 ± 49.3 mm2, P < 0.001), L3/4 (174.5 ± 50.7 mm2 to 113.7 ± 44.0 mm2, P < 0.001), and L4/5 (175.7 ± 58.4 mm2 to 111.2 ± 64.6 mm2, P < 0.001). Similarly, a positive sedimentation sign was associated with a significantly shorter dural sac AP diameter at L2/3 (average from 14.3 ± 1.9 mm to 12.4 ± 2.9 mm, P = 0.0024), L3/4 (13.4 ± 2.4 mm to 11.0 ± 2.9 mm, P = 0.0001), and L4/5 (13.8 ± 2.4 mm to 10.7 ± 3.6 mm, P < 0.001) (Table 2). However, at L1/2, there is no significant difference regarding either dural sac CSA or anteroposterior diameter between positive and negative sedimentation sign (P = 0.34, P = 0.26, respectively) (Table 2).
Cross-Sectional Area and Anterio-Posterior Diameters of Dural Sac Between Positive and Negative Sedimentation Sign.
* P < 0.05.
Discussion
The current study showed that both negative and positive sedimentation signs did appear on the upright MRI at L1/2, L2/3, L3/4 or L4/5 levels. Furthermore, a positive sedimentation sign was associated with significantly decreased dural sac CSA and AP diameter at L2/3, L3/4 or L4/5 level when comparing to negative sedimentation sign. However, no difference regarding dural sac CSA and AP diameter was noted between positive and negative sedimentation signs at L1/2 level.
The nerve root sedimentation sign was first described in LSS patients in the supine position by Barz et al. 1 The sedimentation sign could be used as a supplemental diagnostic method of LSS because it can differentiate patients with severe LSS from asymptomatic patients while having the strength of being easily observed on MRI images [1-3, 5]. In asymptomatic patients, gravity was thought to be responsible for the sedimentation of nerve roots to the dorsal part of the dural sac. 1 Since gravity has a downward force, this implies that in an upright MRI scan of asymptomatic patients, there would be no dorsal sedimentation of nerve roots within the dural sac. However, in the current study, at every intervertebral level, includingL1/2, L2/3, L3/4, and L4/5, a negative sedimentation sign did appear on the upright MRI. Also, the intra-and inter-rater reliabilities were excellent, similar to Barz’s report 1 . The current result is important because it shows that both positive and negative signs appear on multi-positional MRI, meaning that upright images could also be possibly used for sedimentation sign diagnostics. Secondly, the study results suggest that the presence of negative sedimentation signs might not be associated with gravity since negative sedimentation sign is present in both supine and upright position. Although the exact mechanism of the presence of negative sedimentation sign is still unclear, this study indicates that dorsal sedimentation of nerve roots (negative sedimentation sign) may be a function of normal anatomy rather than positional changes. For the mechanism of positive sedimentation sign, Barz et al. 8 demonstrated that patients with LSS and positive sedimentation signs had an increased epidural pressure when compared to patients without LSS and with negative sedimentation signs. Moreover, once adequate decompression was performed, a positive sedimentation sign could change to a negative one, 7 which further provided the evidence that increased epidural pressure was associated with positive sedimentation sign.
On supine MRI, Ko 15 and Fazal et al. 6 studied the correlations between the sedimentation sign and dural sac CSA at L2/3, L3/4 and L4/5 levels, and found that dural sac CSAs at L2/3, L3/4, L4/5 levels were significantly decreased in patients with positive sedimentation signs compared with those with negative signs. The current study showed similar results on upright MRI. All of the 3 studies found that positive sedimentation sign was associated with decreased dural sac CSA at L2/3, L3/4 or L4/5 level when compared to negative sedimentation sign. However, the averages of dural sac CSA in their studies for both positive and negative signs were smaller than in the current study. This may be due to a difference in patient population between the studies and ours: only patients with clinically diagnosed LSS were included in the previous studies while patients in the current study had non-specific back pain. Patient population in their study were clinically diagnosed LSS, while the patients in the current study only had non-specific low back pain symptoms. As sedimentation sign had a poor performance differentiating patients with moderate or mild LSS and low back pain,3,16 there may be intervertebral discs that are not stenotic but have positive sedimentation signs in the current study. The difference in patient population might explain the discrepancy in the values of CSA.
In addition to CSA, AP diameter of spinal canal is another parameter to help diagnose spinal stenosis.17,18 In the current study, we measured dural sac AP diameter, which could more accurately reflect stenosis than spinal canal AP diameter and found patients with positive sedimentation sign had smaller values of dural sac AP diameter than those with negative sedimentation sign, which was similar to the results from Fazal et al. 6 However, the average AP diameter of positive sedimentation sign was more than 10 mm in the current study, while less than 10 mm was used as a measure for central lumbar spinal stenosis. 19 This confirms that a positive sedimentation sign alone is not enough to diagnose LSS in unspecific low back pain patients and the sedimentation sign should be used only for supplemental diagnostics, similar to reports based on supine MRI.1,3,4,20 Also, when compared to the report from Fazal et al., 6 the values of AP diameter of both positive and negative sedimentation sign in the current study were larger than their report. The reasons might be due to the different patient population. Our patient population were those with low back pain, while their patient population were patients with clinically diagnosed central spinal stenosis.
An interesting finding in our study is that, at L1/2 disc level, both CSA and AP diameters of the dural sac in positive sedimentation sign did not have a significant difference compared with those with negative sedimentation sign. This might be due to that the nerve roots at this level are very close to the centrally locating conus medullaris, where the nerve roots are not allowed to travel in the dural sac like nerve roots at caudal level such as L2/3, L3/4 or L4/5 levels. This suggests that a sedimentation sign at L1/2 disc level might not imply the same result as the other 3 levels, and a positive sedimentation sign at L1/2 disc level might not reflect dural sac narrowness.
There is a limitation in the current study. Due to the lack of clinical diagnostic data, we could not determine the relationship between LSS in and sedimentation sign on upright MRI images in our study. However, the presence of positive and negative nerve root sedimentation sign at L1/2, L2/3, L3/4 or L4/5 provides a likely hypothesis that sedimentation sign on upright MRI images could have the same diagnostic value as on supine MRI images and further studies could be done to evaluate the relationship between LSS and sedimentation sign on images in upright positions. Despite this limitation, the current study still demonstrated that the gravity might not be the cause of the dorsal sedimentation of nerve roots, and positive sedimentation sign was associated with decreased dural sac CSA and AP diameter at level L2/3, L3/4 or L4/5 when compared to negative sedimentation sign. This is the first study that concerned nerve root sedimentation sign on upright MRI.
Conclusion
Both negative and positive sedimentation signs did appear at L1/2, L2/3, L3/4 and L4/5 levels on the upright MRI, which suggested that the presence of nerve roots sedimenting dorsally in patients without LSS might not be associated with gravity. Besides this, the current study supports that the sedimentation signs on multi-positional MRI images could have the same diagnostic functions as on supine MRI images although the clinical diagnostic value of sedimentation sign on multi-positional MRI images needs to be confirmed in further studies. Also, a positive sedimentation sign was associated with significantly decreased dural sac CSA and AP diameter at L2/3, L3/4 or L4/5 level compared to negative sedimentation sign on multi-positional MRI images, similar to the findings on traditional MRI images.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Disclosures outside of submitted work: JCW- Royalties – Biomet, Seaspine, Amedica, Synthes; Investments/Options – Bone Biologics, Pearldiver, Electrocore, Surgitech; Board of Directors – AO Foundation, Society for Brain Mapping and Therapeutics, Fellowship Funding (paid to institution): AO Foundation. ZB- consultancy: Cerapedics (past), The Scripps Research Institute (past), Xenco Medical (past), AO Spine (past); Research Support: SeaSpine (past, paid to the institution), Next Science (paid directly to institution), Motion Metrics (paid directly to institution); North American Spine Society: committee member; Lumbar Spine Society: Co-chair Research committee, AOSpine Knowledge Forum Degenerative: Associate member; AOSNA Research committee- committee member.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.