
Abstract
Study Design:
Retrospective study.
Objective:
Current studies suggested that the posterior cervical deep muscles should be preserved during the atlantoaxial posterior approach. This study aimed to modify the conventional temporary posterior fixation by preserving the semispinalis cervicis and to evaluate the radiographic and clinical outcomes compared with the conventional technique.
Methods:
Applied anatomical and imaging study were assessed prior to the clinical studies. Thirty patients with odontoid fracture were enrolled. 12 patients underwent modified operation with preservation of semispinalis cervicis (Group P-SSC), and 18 patients underwent conventional approach with detachment of the semispinalis cervicis (Group D-SSC) as controls. Clinical and radiological assessments were evaluated postoperatively, including activities of daily living (ADL), axial symptom scoring system (Ass), cervical range of motion (ROM), and the average atrophy rate of muscles.
Results:
All patients experienced fracture healed within 10 months after temporary fixation. At early follow-up, ADL accompanying extension and flexion were significantly different between the two groups. The Ass scores in the Group P-SSC were constantly higher than that in Group D-SSC. Flexion-Extension ROM in Group P-SSC was significantly larger than that of Group D-SSC. The average atrophy rate at the C3 and C5 level in Group P-SSC was 7.62±3.38% and 7.55±3.89%, repectivcly, while 15.67±5.97% and 8.56±4.76% in Group D-SSC, respectively. Significant differences in the atrophy rate were found between groups at C3 level.
Conclusions:
Compared with the conventional technique, the modified surgical technique with preservation of semispinalis cervicis was effective in improving axial symptoms, decreasing the atrophy rate of muscles, and increasing the cervical ROM.
Introduction
Anderson-D’Alonzo type
Over recent years, axial symptoms have received a lot of attention as postoperative complications which adversely affect patients’ quality of life after posterior cervical fixation.
6
Although the causes of axial symptoms remain uncertain, many studies have shown that when C-2 and C-7 spinous processes are preserved, the frequency of persistent postoperative axial neck pain is reduced.6-9 The semispinalis cervicis (
Methods
Applied Anatomy and Imaging Study
To safely perform this modified surgery, the approach was assessed by applied anatomy prior to clinical studies. Anatomical observations were performed in 6 fresh cadavers (3 females and 3 males) aged between 55 to 75 years at the time of death, with no evidence of spinal pathology. The cadaveric dissections were performed with the cadavers in the prone position. The skin and the nuchal fascia were opened. The lateral edge of the trapezius muscle was seen and retracted medially. The fibers of the splenius capitis muscle run cranial and lateral below the nuchal fascia. This muscle was split, and down below we found the fibers of the semispinalis capitis muscle. To observe the axial lamina, this muscle was also detached and retracted. The obliquus capitis inferior muscle was found running across the surgical field. The obliquus capitis inferior muscle and semispinalis cervicis muscle could be mobilized and retracted without damaging the attachments to the C2 spinous process. The entry points for the C1 lateral mass screws and C2 pedicle screws were identified (Figure 1). Anatomical observation in cadavers: (A). Cadaveric dissections (B). Anatomic locations of C2 in the cadaver. SSCa: semispinalis capitis; Trap: trapezius; OCi: Obliques capitis inferior; RCpm: Rectus capitis posticus major. The black circle indicates the insertion points for the C2 screw; the black star indicates the C2 spinous process.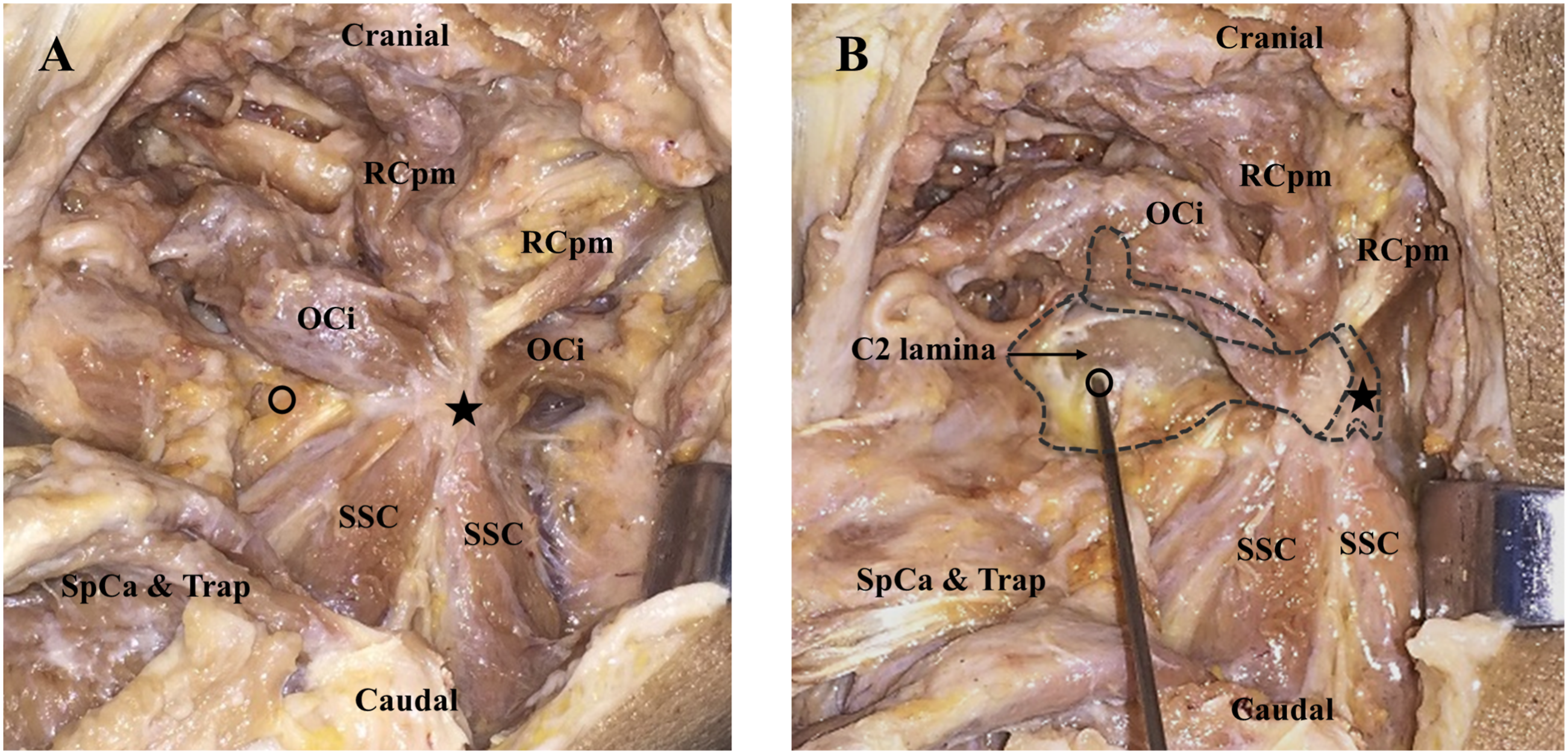
To ensure that the operation was performed according to preoperative plans, the cervical posterior muscles were assessed using Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) images. The main planned parameters of screws insertion points, direction of screws trajectories, and intermuscular space were studied on preoperative cross-sectional images (C1-C2 level) of patients (Figure 2). The cross-sectional images on C2 level. Picture (A) shows the MRI image; Picture (B) shows the CT image. SSCe: semispinalis cervicis; M: multifidus; SSCa: semispinalis capitis; SpCa: splenius capitis; Trap: trapezius; LgCa: longissimus capitis; LgCe: longissimus cervicis; The black circle indicates the insertion points for C2 screw; the arrows indicate the screw trajectory for C2 screw.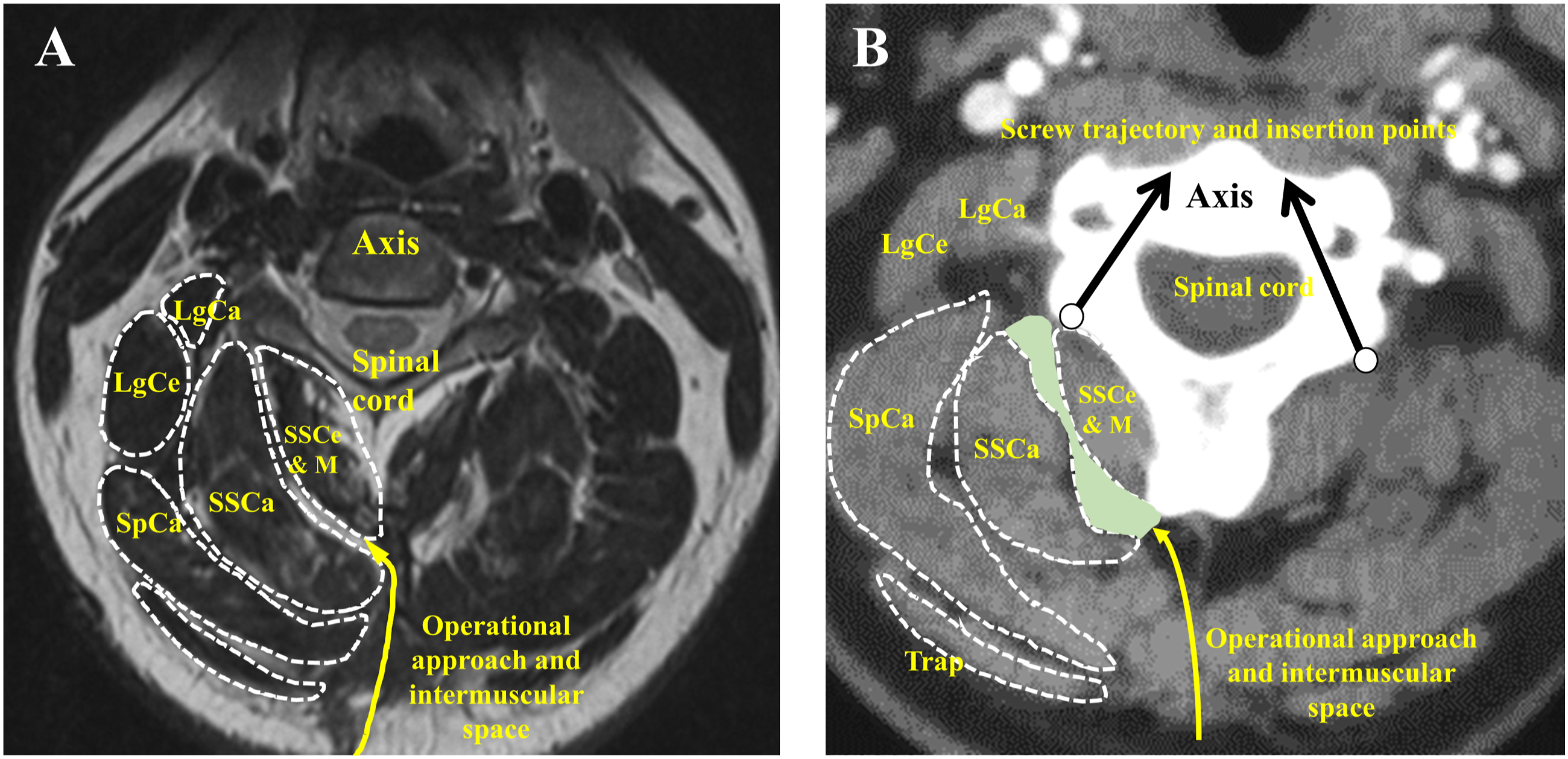
Patient Population
From June 2015 to January 2017, we conducted the conventional fixation with detachment of the SSC (Group D-SSC), and from February 2017 to December 2018, we conducted the temporary posterior fixation by modified fixation with preserving the SSC (Group P-SSC). Therefore, 35 consecutive patients diagnosed with odontoid fractures who met the inclusion criteria were divided into two groups. All procedures were performed by the same surgical team, with the same operator and assistant. The study has been approved by the Ethical Committee of our hospital. Every patient gave informed consent.
The inclusion criteria were: (1) Grauer typeⅡA fractures with fragmentation but displacement less than 1 mm, which could not be reduced by external fixation; (2) Grauer type ⅡB fractures with displaced transverse fractures that could not be fixed by the anterior approach; (3) Grauer typeⅡC fractures that manifested with anterior inferior to posterior superior or comminuted fractures; (4) Patients with Grauer type Ⅲ fractures could not tolerate long-term external fixation; (5) Postoperative follow-up was at least 2 years. The exclusion criteria were: (1) Aged 65 or older or with severe osteoporosis or tumor; (2) Poor physical status, unable to tolerate the second surgery; (3) Grauer type Ⅰ and Ⅲ fractures that was expected to have predictabley good results with external immobilization; (4) Odontoid fractures with atlantoaxial instability or disruption of the transverse atlantal ligament, or atlantoaxial subluxation with atlantodens interval more than 3 mm, for whom posterior C1-C2 fusion has to be conducted. (5) History of anterior or posterior cervical fusion surgery.
Operative Technique
All patients underwent nasotracheal or fiberoptic endotracheal intubation. After induction of general anesthesia, the patients were placed in prone position with a Mayfield head clamp with a slight degree of cervical hyperextension. A gauze roll was placed in the mouth to permit an unobstructed anteroposterior view of the odontoid process.
The surgical procedure for Group P-SSC included the SSC insertion that was completely preserved in C2. After a midline incision, the nuchal fascia and trapezius muscle were dissected. Off the midline, splenius capitis and semispinalis capitis were dissected to expose the deep cervical muscles. The C2 lamina and pedicle were exposed by blunt dissection through the intermuscular plane between the SSC muscle and the obliquus capitis inferior muscle without damaging the attachments to the C2 spinous process. Then, the suboccipital muscles and obliquus capitis inferior muscles were detached and the entry points for the C1 lateral mass screw were identified (Figure 3). The insertion points for the C1 and C2 screws were located at the position described by Harms and Melcher.
4
The surgical procedure in Group D-SSC included the conventional temporary fixation technique previously described, in which the SSC was detached from the C2 spinous process.
5
Picture A and B shows the operative field in Group D-SSC and Group P-SSC respectively. (A) The conventional surgery detaching SSC attaching to the C2 spinous process; (B) The modified surgery preserving SSC.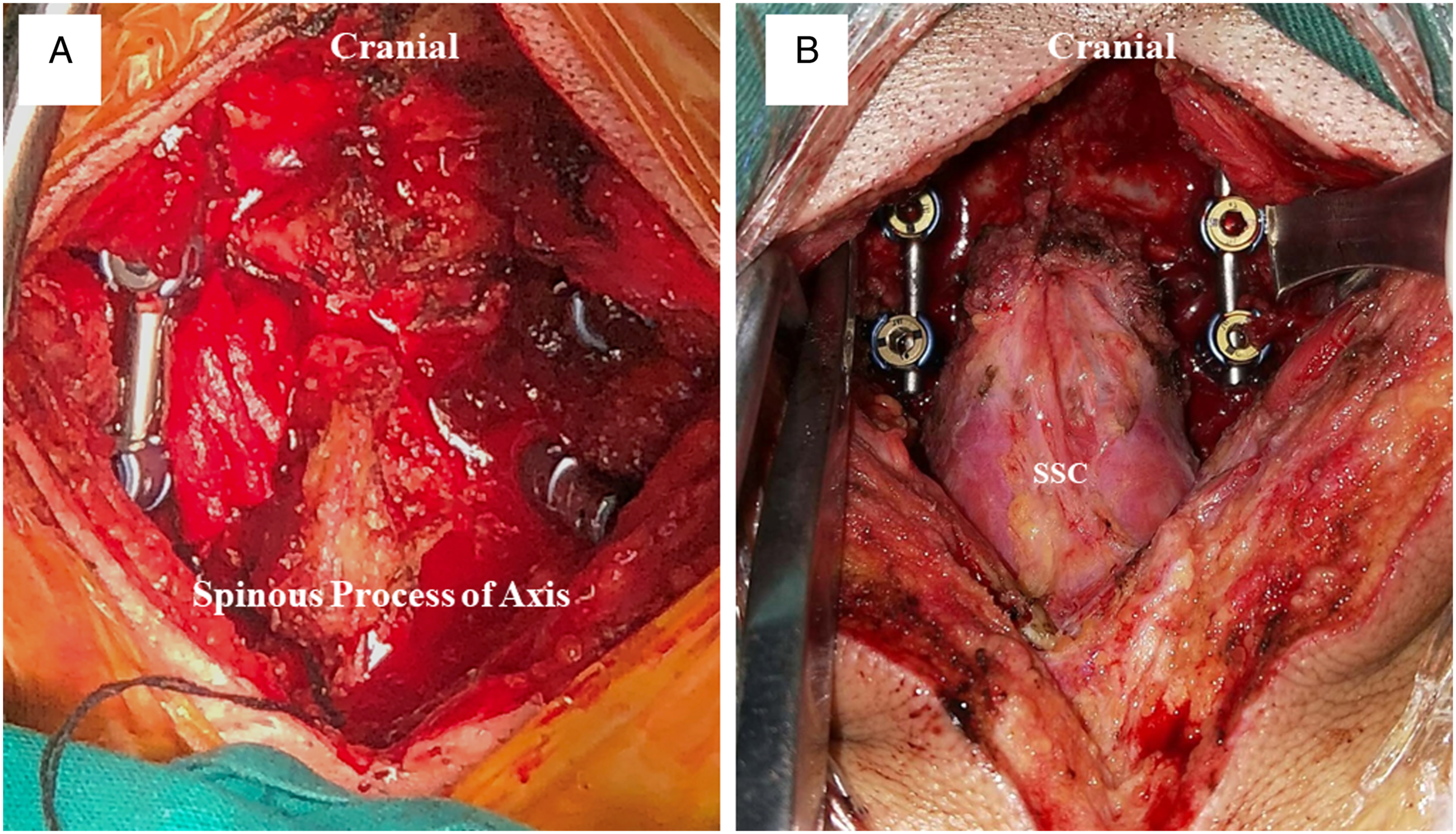
The postoperative collar period was 6-8 weeks. Cervical CT scan and image reconstruction were performed at 3-6 months postoperatively or later to evaluate fracture healing which was defined as evident bridging bone across the odontoid fracture site. Once fracture healing was observed, the removal of instrumentation was performed as described in previous studies. 4 The routine of the second surgery was to reuse the previous incision and remove the hardware via a posterior approach. The SSC and its attachment were carefully retained in Group P-SSC.
Radiological and Clinical Assessment
Plain radiographs were taken before surgery, and at 3, 6, and 12 months after the first surgery and after instrumentation removal. Clinical and radiological assessments after the first surgery and removal of instrumentation were listed below.
Measurements of flexion to extension ROM (F-E ROM) and rotation ROM (R-ROM)
The postoperative O–C7 angles on cervical flexion and extension position were measured using the McGregor line and the posterior tangents of the C7 vertebral body on lateral cervical extension and flexion radiographs, respectively. Then the F-E ROM was calculated as the difference between the two angles (Figure 4). The postoperative R- ROM of the patients were photographed in the cranial view using a digital camera ,with spectacles as the measurement lines (Figure 4).
11
Measurements of rotation ROM (A & B) and O–C7 angle at F-E ROM (C & D). (A&B) The lines for measurements were obtained using the glasses and the pattern of clothes. The total of the left and right rotation angles was calculated as rotation ROM (α + β). (C&D) The lines for measurements were obtained using McGregor line and posterior tangents of the C7 vertebral body on lateral extension or flexion radiographs. The F-E ROM was calculated as (β - α ).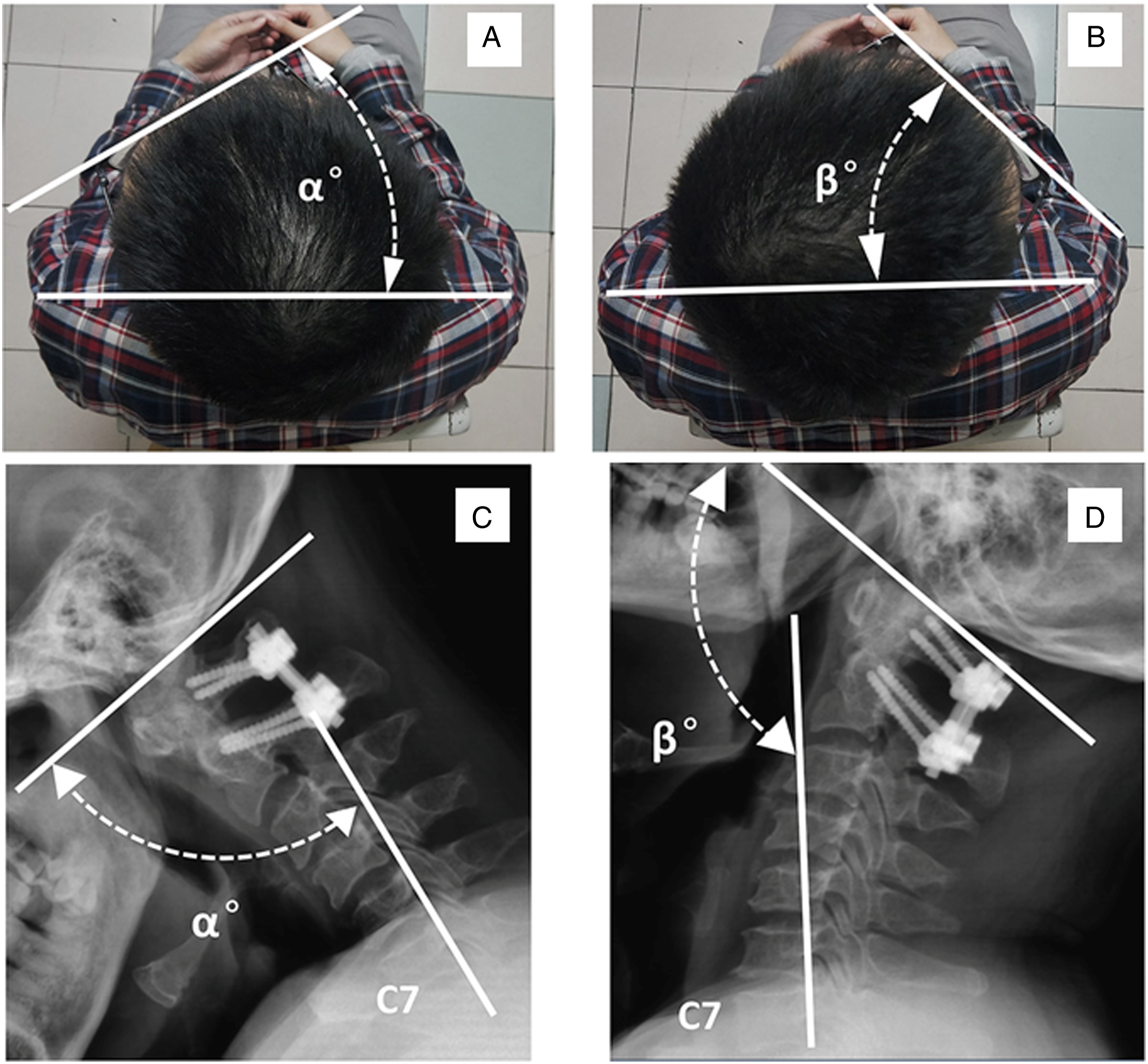
Measurements of Cross-Sectional Areas (CSA) of the Cervical Posterior Muscles
The cervical spine was examined by CT before surgery and 3 months postoperatively. The CSA at the C3-4 and C5-6 levels was measured for evaluation. The preoperative and postoperative CSA of the posterior cervical muscles, including the trapezius, splenius capitis, semispinalis capitis, SSC, and multifidus muscles were measured on axial CT scanning with soft-tissue window at C5, while SSC and multifidus muscles were measured at C3 level (Figure 5). The rate of muscle atrophy was calculated at each level using the following formula7,12: Atrophy rate (%) = (1 - postoperative area/preoperative area) * 100%. The measurement was performed using ImageJ imaging software (version 1.43, National Institutes of Health, Bethesda, Maryland). Outline of the cervical extensor muscles. (A) Posterior extensor muscles visualized on axial CT images at the C5–C6 level. a multifidus, b semispinalis cervicis, c semispinalis capitis, d splenius capitis. (B) Outline of the semispinalis cervicis and multifidus at the C3-C4 level.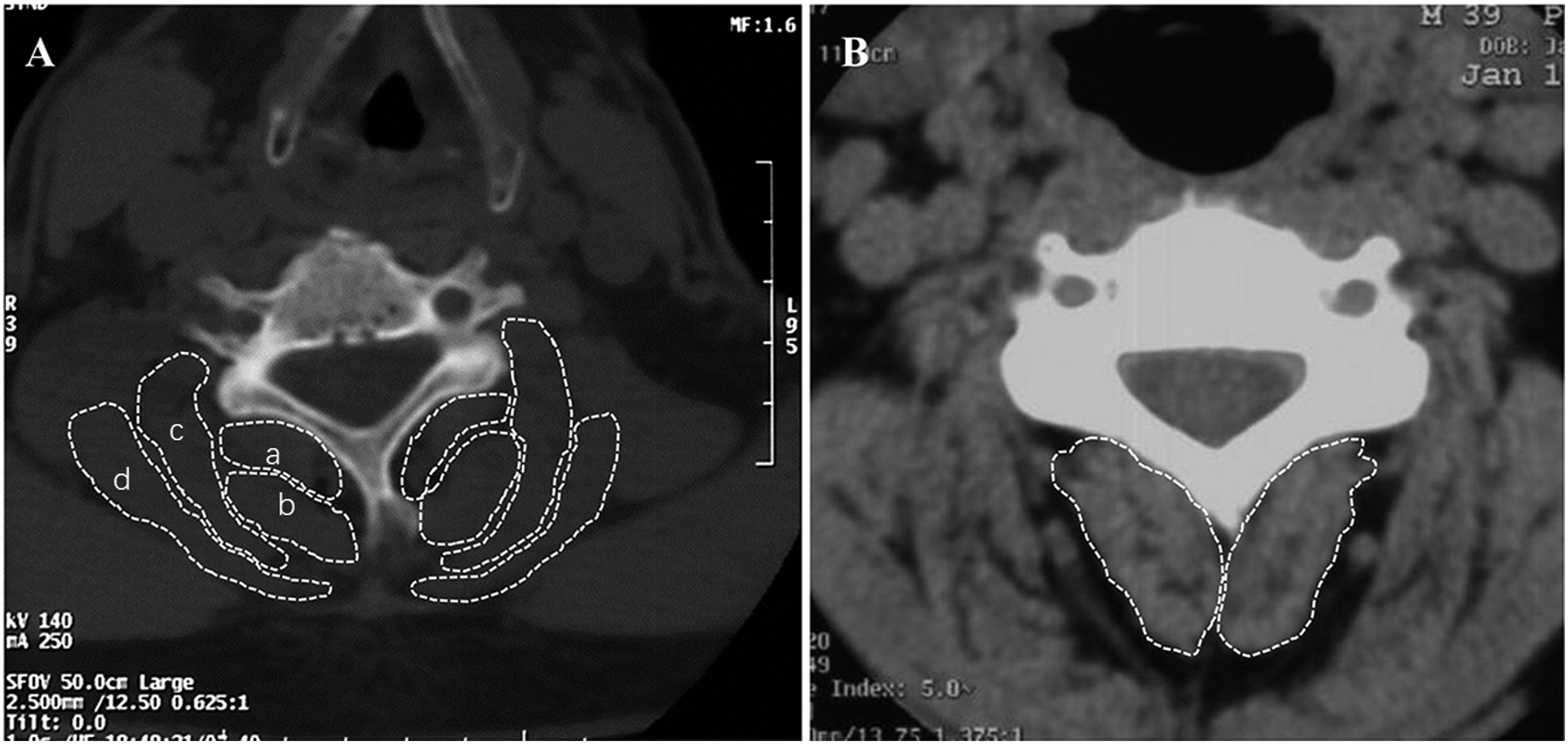
All measurements were performed independently by two researchers who were blinded to the operative method. Analysis performed using the average values of the two observations at each level.
Evaluation of ADL
Activities of Daily Living Index for Neck Mobility in Daily Living.
Abbreviations: ADL, activities of daily living.
The Severity of the Limitation of ADL.
Abbreviations: ADL, activities of daily living.
Evaluation of axial symptoms
Axial symptoms were evaluated using the Axial Symptom Scoring System (
Statistical Analysis
The SPSS statistical software (Version 25; IBM Corp., NY, USA) was used to complete the statistical analyses. Continuous variables were presented as mean with standard deviation, and categorical variables as total number and percentage. Continuous variables were compared using Student's t-tests including patients’ age, healing time, CSA, ROM, and atrophy rate. ADL scores and Ass scores were compared using Spearman’s rank correlation test, and Mann-Whitney U tests. Comparisons of categorical variables were performed with the Chi-square test or Fisher test, including gender, fracture classification. A P < .05 was considered statistically significant.
Results
Patients’ General Information.
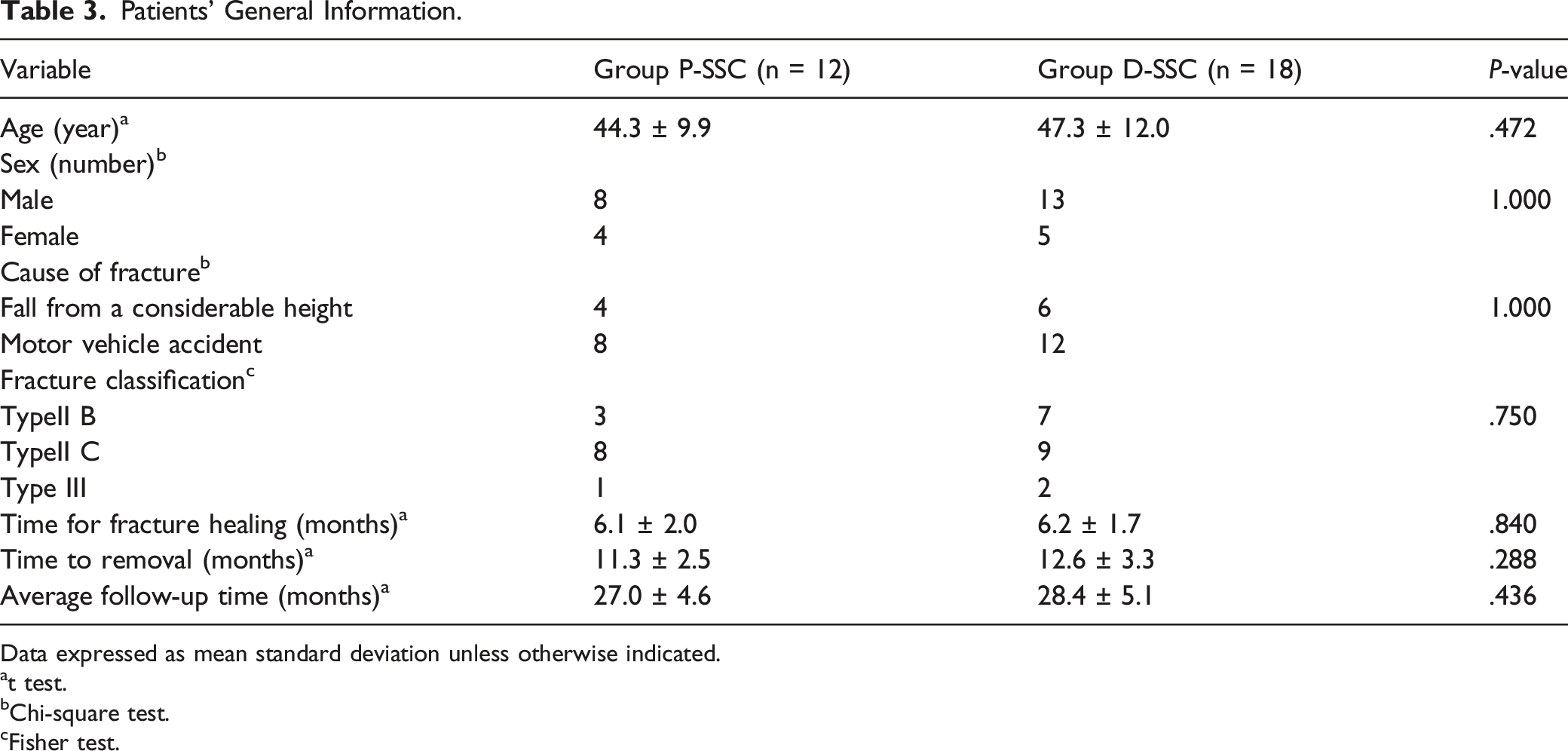
Data expressed as mean standard deviation unless otherwise indicated.
at test.
bChi-square test.
cFisher test.
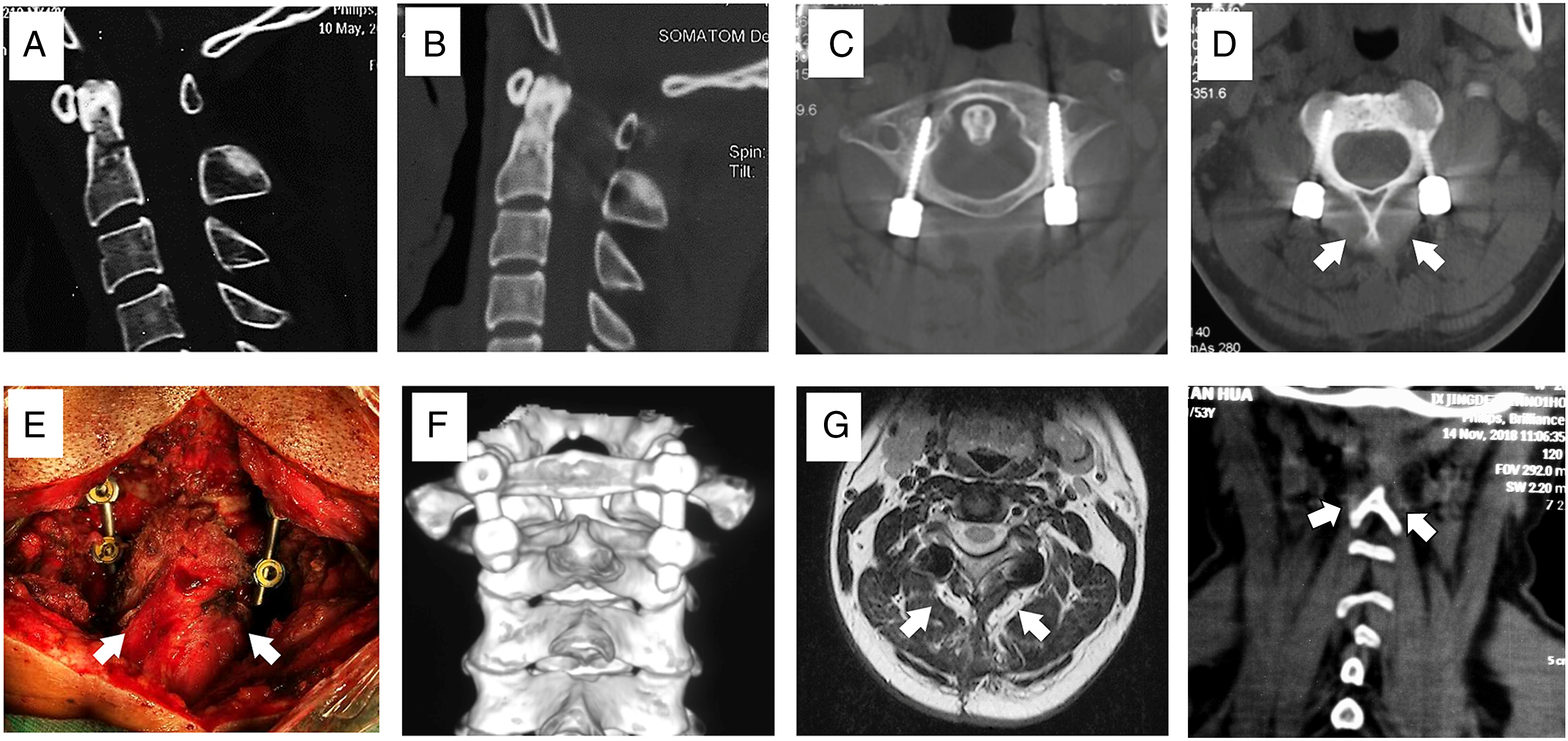
A type II C odontoid fracture managed with temporary posterior fixation (A) Preoperative CT scan; (B) postoperative sagittal view of CT scan; (C) axial view of CT at the C1 level; (D) axial view of CT at the C2 level; (E) preserved SSC attached to the C2 spinous process; (F) postoperative CT scan and reconstruction; (G) postoperative Magnetic Resonance Imaging; (H) postoperative coronal view of CT showing the intact signal of SSC.
Limitations of Activities of Daily Living
Postoperative ADL, Axial Symptom Score, and ROM in Two Groups.
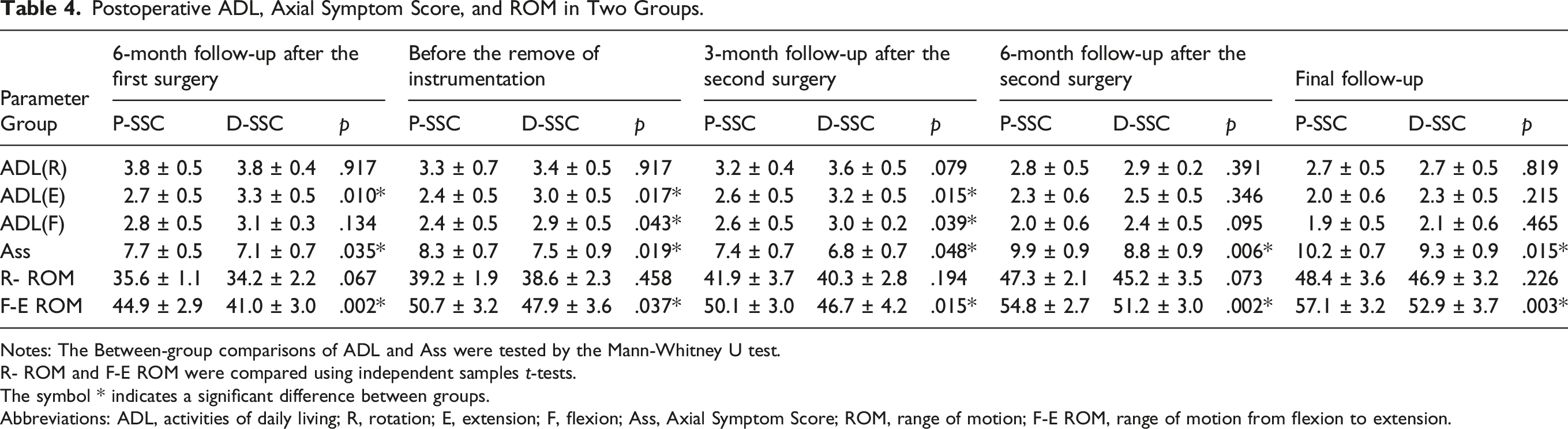
Notes: The Between-group comparisons of ADL and Ass were tested by the Mann-Whitney U test.
R- ROM and F-E ROM were compared using independent samples t-tests.
The symbol * indicates a significant difference between groups.
Abbreviations: ADL, activities of daily living; R, rotation; E, extension; F, flexion; Ass, Axial Symptom Score; ROM, range of motion; F-E ROM, range of motion from flexion to extension.
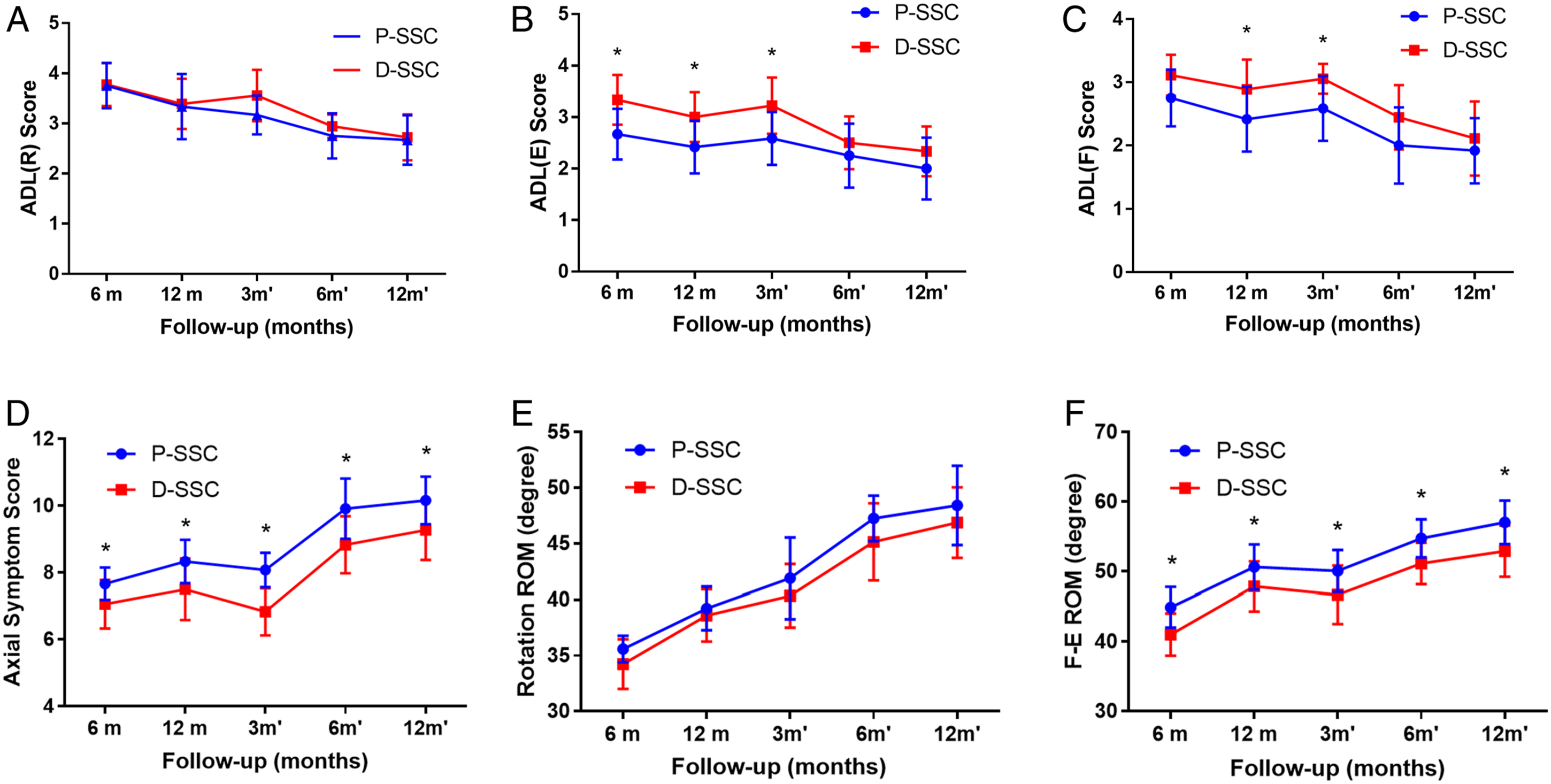
Changes in the ADL, Axial symptom score, and ROM evaluated postoperatively. (A∼C) The changes of limitations of activities of daily living (ADL) accompanying extension, flexion, and rotation movements; (D) The changes of axial symptom scoring system; (E,F) The changes of the flexion to extension ROM (F-E ROM) and rotation ROM; The bars indicate standard deviations, *P < .05 significant differences between two groups by the independent samples t-test or Mann-Whitney U tests; 6/12m, 6/12 months after the first operation; 3/6/12m′, 3/6/12 months after the second operation.
Axial Symptom Scores
Axial symptom scores in Group P-SSC and Group D-SSC were listed in Table 4. The Ass scores in the Group P-SSC were constantly higher than that of Group D-SSC. The incidence and severity of axial symptoms were constantly lower in the Group P-SSC and significantly differed between the two groups in each postoperative follow-up (Mann-Whitney U test, Z = −2.315, −2.463, −2.123, −2.839, and −2.553, respectively; P = .035, .019, .048, .006, and .015, respectively; Figure 7D).
Cervical Range of Motion
The Rotation ROM and F-E ROM exhibited a trend of gradual increase, and the clinical assessment outcomes were listed in Table 4. The mean rotation ROM of C1-C2 in Group P-SSC increased gradually from 35.6°±1.1° to 48.4°±3.6°. As for Group D-SSC, the mean ROM increased gradually from 34.2°±2.2° to 46.9°±3.2°. The mean value of Group P-SSC was higher than that of Group D-SSC but there was no statistical difference between the two groups at each follow-up (P > .05; Figure 7E). During each follow-up, the F-E ROM in Group P-SSC was 44.9°±2.9°, 50.7°±3.2°, 50.1°±3.0°, 54.8°±2.7°, and 57.1°±3.2° respectively, which was significantly higher than that of Group D-SSC (41.0°±3.0°, 47.9°±3.6°, 46.7°±4.2°, 51.2°±3.0°, and 52.9°±3.7°). Significant differences remained until the end of the 12-month follow‐up (t-tests, F = .422, .064, 2.007, .240, and .122, respectively; P = .002, .037, .015, .002, and .003, respectively; Figure 7F).
Cross-Sectional Areas
Atrophy Rate of Cervical Posterior Muscles between P-SSC and D-SSC.
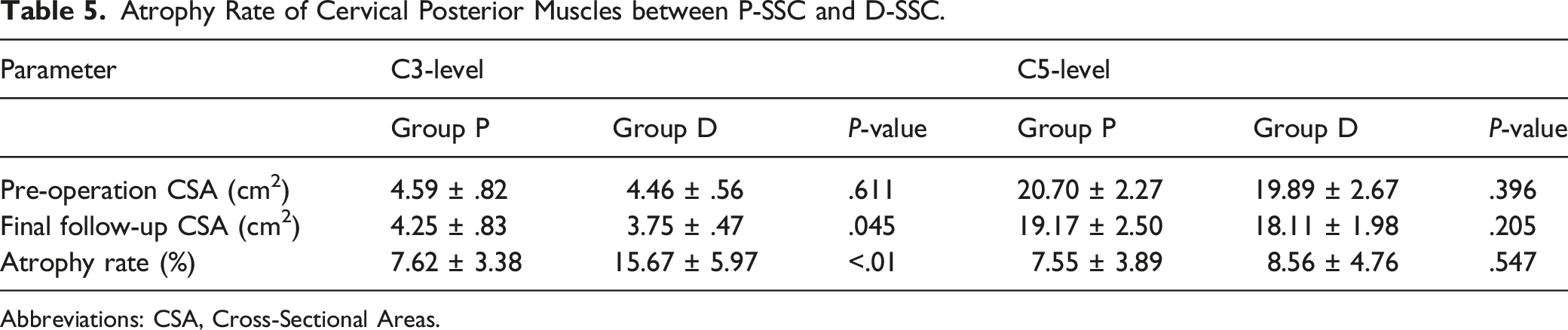
Abbreviations: CSA, Cross-Sectional Areas.
Discussion
Based on fracture line obliquity, displacement, and comminution to guide treatment options, Grauer et al have classified Anderson-D’Alonzo type II of odontoid fractures into three subtypes. 14 The type IIC fracture, which has an oblique fracture line from posterosuperior to anteroinferior that parallels screw trajectory, is a contraindication to anterior screw fixation since interfragmentary compression cannot be achieved using the odontoid screw. 15 Recently, temporary posterior fixation has been reported as a new cervical posterior surgery for treatment of Anderson-D’Alonzo type II odontoid fractures, which does not include the fusion of the atlantoaxial joint thus preserving the cervical movement. By comparing clinical outcomes and the range of motion (ROM) in rotation of these two non-fusion techniques, Guo et al have reported that temporary posterior fixation could spare the motion of the C1-C2 complex and achieve similar clinical outcomes to anterior screw fixation in the treatment of Anderson-D’Alonzo type II odontoid fracture.15,16
Unlike the posterior atlantoaxial fixation and fusion surgery, it is unnecessary to place autologous iliac crest graft between the posterior C1/2 articulation after grinding the cortical bone in temporary posterior fixation, thus avoiding the detachment of the deep extensor musculature. 10
The SSC, which are mostly inserted into the C2 spinous process, act as the primary dynamic stabilizers and as extensors of the cervical spine. According to existing research, the SSC and multifidus muscle pair show significant relative activation during head extension. They also have an essential postural role, which is likely to be affected by atrophy and loss of strength during exposure to microgravity or long-term bed rest. 17 Current research suggests that the posterior cervical deep muscles should be preserved without detachment from the C2 spinous process during the atlantoaxial posterior approach.8,18,19 Therefore, it is crucial to preserve SSC, especially in upper cervical spine surgery. Kazunari and colleagues have reported that the posterior cervical approach preserving the SSC insertion into C2 could reduce the postoperative axial symptoms compared to the conventional approach, which implies reattaching the muscle to the C2 spinous process. 20 Besides, some authors have verified that the preservation of neck extensor could benefit patients by restoring the lordotic angle of the cervical spine and reducing pain in patients with loss of cervical lordosis.20-22
In the current study, we evaluated and compared outcomes of ADL, ROM, axial symptoms, and CSA of cervical muscles of two non-fusion techniques in the treatment of fresh Anderson-D’Alonzo type II odontoid fractures. To our knowledge, there is no previous detailed clinical study on the effect of preserving the SSC inserted in the C2 spinous process in the atlantoaxial posterior approach. Clinical data demonstrated that the frequency of limitations of ADL accompanying extension or rotation in the Group P-SSC was lower than Group D-SSC. Moreover, objective data showed that the postoperative ranges of motion from flexion to extension (F-E ROM) in the Group P-SSC were significantly larger than those in the Group D-SSC. As the SSC inserted into the C2 spinous process acts as an essential extensor of the cervical spine, preserving the SSC in surgeries might allow a larger angle at extension and a reduction of limitations of ADL accompanying extension during follow-up.17,21 Nevertheless, Yukawa et al have compared a laminoplasty that preserved the SSC with skip laminectomy, observing no significant differences in the extension ROM. 23 In our study, we found that the atlantoaxial posterior approach with preservation of the SSC inserted into C2 did not influence the postoperative neck rotation ROM and limitations of ADL accompanying rotation.
As reported, the CSA of the posterior cervical muscles has a strong relationship with the movement strength during flexion and rotation.7,22 Decrease in the CSA of posterior extensor muscles was significantly associated with the development of shoulder stiffness, which has been related to dysfunctions or spasms in the posterior extensor muscles of the cervical spine. 24 Takeuchi et al have evaluated the CSA of the posterior cervical muscles prospectively after laminoplasty by preserving or reattaching the SSC inserted into C2. They reported that only the preservation of the SSC inserted into C2 could maintain the whole cervical posterior muscular volume. 7 Some studies have also reported that posterior surgeries may lead to atrophy and cause damage to these muscles, leading to instability or malalignment of the cervical spine.24,25 In our study, the average atrophy rate in the group preserving the SSC was significantly lower in the atrophy rate at the level C3. The difference was not significant at level C5, this might be due to the limited motion of the upper cervical fixation and increased compensatory activity of the lower cervical muscles, which in turn lead to the less obvious atrophy at lower levels.
In order to minimize muscle substance destruction and to maximally preserve both the mobility and stability of the cervical spine, various modified minimally invasive atlantoaxial fixation such as intramuscular and intermuscular exposure techniques have been used for preserving the posterior elements.19,26 They all achieved satisfactory clinical outcomes, verifying the importance of the deep extensor muscles of the neck. However, due to increased surgery risks and a steeper learning curve, this approach should only be taken by surgeons with rich experience.
Even though the C1–C2 temporary fixation with preservation of SSC technique leads to good outcomes, it cannot be used as the treatment of choice for all types of odontoid fracture. This technique has been indicated in Grauer type II fractures with good reduction. For irreducible fractures and elderly patients with severe osteoporosis, posterior C1–C2 fixation and fusion are more suitable approaches. The posterior approach is also not considered for fractures with Anderson-D’Alonzo type Ⅰand III fractures which have predictably good results by the external immobilization.
There are some limitations to our study. The sample size is relatively small. Further studies with larger sample size should be conducted to verify the current result. Moreover, we did not evaluate the role of function exercise, rehabilitation, and the individual variation between two groups, which may lead to variability in the results of this study.
Conclusions
Compared with the conventional technique, this modified surgical technique with preservation of semispinalis cervicis was effective in improving the axial symptoms, decreasing the atrophy rate of posterior cervical muscles, and increasing the cervical ROM accompanying neck extension and flexion.
Footnotes
Authors’ contributions
JL, EZJ; study design, analyses, and interpretation of data, draft of manuscript with tables and figures. JL, SL, EZJ, GHX; substantial contributions to conception and critical revision for important intellectual content. ZCS, GHX; substantial contributions to study design and data acquisition, JL, SL; data acquisition. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was funded by the clinical management optimization project of Shanghai Shenkang Hospital Development Center (SHDC22020211).
Abbreviations
SSC: semispinalis cervicis; P-SSC: preserving SSC; D-SSC: detaching the SSC; ROM: range of motion; CT: Computed tomography; ADL: activities of daily living; Ass: axial symptom scoring system.
Ethics approval and consent to participate
The study was approved by the ethical committee of Changzheng Hospital. All the patients gave written consent for research applications of their clinical data. The patient data were anonymized in this study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding authors upon reasonable request.