
Abstract
Study Design:
Retrospective cohort study.
Objective:
To compare the outcomes of patients with adult spinal deformity (ASD) following spinal fusion with the lowest instrumented vertebra (LIV) at L4/L5 versus S1/ilium.
Methods:
A multicenter ASD database was evaluated. Patients were categorized into 2 groups based on LIV levels—groups L (fusion to L4/L5) and S (fusion to S1/ilium). Both groups were propensity matched by age and preoperative radiographic alignments. Patient demographics, operative details, radiographic parameters, revision rates, and health-related quality of life (HRQOL) scores were compared.
Results:
Overall, 349 patients had complete data, with a mean follow-up of 46 months. Patients in group S (n = 311) were older and had larger sagittal and coronal plane deformities than those in group L (n = 38). After matching, 28 patients were allocated to each group with similar demographic, radiographic, and clinical parameters. Sagittal alignment restoration at postoperative week 6 was significantly better in group S than in group L, but it was similar in both groups at the 2-year follow-up. Fusion to S1/ilium involved a longer operating time, higher PJK rates, and greater PJK angles than that to L4/L5. There were no significant differences in the complication and revision rates between the groups. Both groups showed significant improvements in HRQOL scores.
Conclusions:
Fusion to S1/ilium had better sagittal alignment restoration at postoperative week 6 and involved higher PJK rates and greater PJK angles than that to L4/L5. The clinical outcomes and rates of revision surgery and complications were similar between the groups.
Keywords
Introduction
In most patients with adult spinal deformity (ASD), posterior fusions extend to the sacrum or ilium; however, some patients may present as good candidates for fusions that stop short of the sacrum. In addition, fusions to S1 are associated with their own set of complications, such as postoperative sacral insufficiency fractures; increased operating time and estimated blood loss (EBL) due to the need for iliac fixation in some cases; and higher rates of proximal junctional kyphosis (PJK) and pseudarthroses.1-6 The general published indications for fusion to the sacrum or ilium are L5–S1 spondylolisthesis, previous L5–S1 surgery, existing L5–S1 stenosis, subluxation of L5 (>15°), and a severely degenerated disc. 7 The advantages of distal fixation to the sacrum (± ilium) are increased stability8,9 and better sagittal alignment restoration.1,3 However, the increase in operating time, morbidity, and the rate of surgical revision due to pseudarthrosis are disadvantages of fusions to S1/ilium.3-5
Furthermore, there are disadvantages of fusions ending at lumbar levels (L4 or L5), such as symptomatic adjacent distal disc degeneration, leading to a loss of lumbar lordosis (LL), sagittal decompensation, and the need to extend the fixation to the sacrum. 2 This is coupled with high reported revision rates within 1 year (12.5%–15.4%),10,11 2.1 years (28.2%), 12 and 3.3 years (32%) of follow-up. 6 Therefore, the risks and benefits of selecting distal fusion levels should be carefully evaluated.
The purpose of this study was to compare the outcomes in ASD patients with fusion to either distal lumbar levels (L4 or L5) or the sacrum (± ilium). The primary outcome was the rate of surgical revision, while the secondary outcomes were clinical and radiographic parameters and the health-related quality of life (HRQOL) scores at a minimum follow-up of 2 years.
Materials and Methods
Patient Population
This was a retrospective study of prospectively collected data from a multicenter ASD database from 2008 to 2016. Institutional review board approval was obtained from each of the 11 participating centers across the country. Informed consent was obtained from all participants. The database inclusion criteria were patients aged >18 years meeting at least 1 of the following radiographic criteria of spinal deformity: scoliosis with Cobb angle ≥20°, sagittal vertical axis (SVA) ≥5 cm, pelvic tilt (PT) ≥25°, and/or thoracic kyphosis (TK) ≥60°. Additional criteria specific to the current investigation included the following: (1) posterior fusion with an upper instrumented vertebra (UIV) above T12 and lowest instrumented vertebra (LIV) of L4, L5, S1 or the ilium and (2) a minimum 2-year follow-up period. Patients with prior fusions including the L2–ilium levels were excluded from the study.
Data Collection and Radiographic Assessment
Baseline demographics and operative details included age, sex, instrumented levels, EBL, operating time, interbody fusion (IBF) with cage, any osteotomy, and use of 3-column osteotomy (3CO). Radiographic data was collected using full-length standing posteroanterior (PA) and lateral spine radiographs at baseline and at the 6-week and 2-year follow-ups. Radiographic parameters included TK, LL, PT, pelvic incidence (PI), sacral slope (SS), PI minus LL (PI-LL), SVA, T1 pelvic angle (T1PA; the angle between the line from the center of the femoral heads to the center of S1 and the line from the femoral head to the center of T1), coronal alignment (C7PL; distance from the C7 plumb line to the central sacral vertical line on PA view), PJK angle (the Cobb angle between the inferior endplate of the UIV to the superior endplate of the 2 vertebrae above), and distal junctional kyphosis (DJK) angle (the angle between the superior endplate of the LIV and the inferior endplate of the second distal vertebra below). Abnormal radiographic PJK and DJK were defined as a junctional kyphosis angle of ≥10° and a postoperative increase of ≥10°.13,14 The Scoliosis Research Society (SRS)-Schwab adult deformity classification of each patient was also recorded. 15
HRQOL was assessed using the Oswestry disability index (ODI), the SRS questionnaire, and the Short Form-36 mental and physical component scores (SF-MCS and SF-PCS, respectively). Clinical outcome scores were collected at baseline and at the 6-week and 2-year follow-ups.
The recorded complications included implant failure, infection, wound problems, neurological, cardiopulmonary, gastrointestinal, vascular, operative, renal, radiographic complications, and death. The number of major and minor complications was tallied, and the total number of complications requiring revision surgery was assessed.
Patient Matching and Statistical Analyses
The patients were categorized into 2 groups based on LIV levels—group L (fusion to L4 or L5) and group S (fusion to S1 or ilium). Patients were then propensity matched based on the significantly different baseline characteristics including age, PI, PI-LL, C7PL, and T1PA. Statistical analyses were performed using IBM SPSS (version 22.0; IBM Corp., Armonk, NY, USA). Categorical data was compared using the chi-square or Fisher’s exact test, while continuous data was compared using an independent t-test or the Wilcoxon rank-sum test where appropriate. The evolution of radiographic parameters over time was measured using 1-way repeated measures analysis of variance, followed by post hoc Bonferroni correction. A 2-tailed significance level was set at 5% confidence interval (P < 0.05).
Results
A total of 437 patients met the inclusion criteria for this study. A subset of 349 patients who had the complete dataset and were followed up at all timepoints were finally enrolled in the study. In total, there were 59 (16.9%) men and 290 (83.1%) women. The average age was 61.1 years, with a mean follow-up period of 46 months. Group L included 38 patients, group S included the remaining 311 patients (10 had sacrum LIV and 301 had ilium LIV). Patients in group S were significantly older (62.9 vs. 45.6 years; P < 0.001) and had larger sagittal and coronal plane deformities than those in group L. The PI-LL was 17.6° in group S and -0.6° in group L (P < 0.001). The PT was 25.2° in group S and 16.4° in group L (P < 0.001). The SVA was 67.8 mm in group S and 12.9 mm in group L (P < 0.001). The coronal alignment was 37.1 mm in group S and 27.0 mm in group L (P = 0.005). According to the SRS-Schwab classification, the coronal curve type was different between the groups (63.2% double curve in group L and 48.9% thoracolumbar/lumbar curve in group S; P < 0.001; Table 1).
Demographic and Classifications of the Unmatched and Matched Patients in Groups L and S.
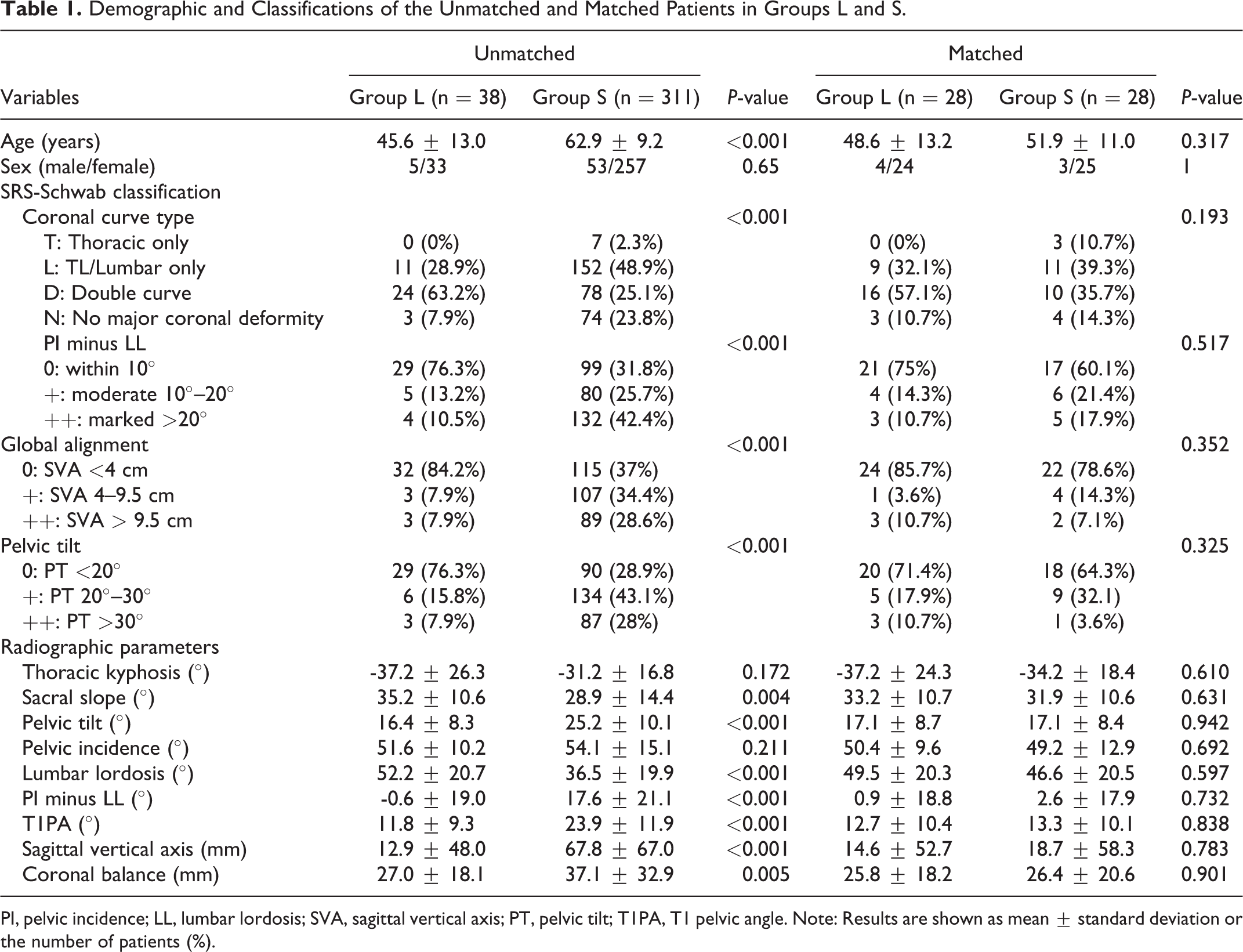
PI, pelvic incidence; LL, lumbar lordosis; SVA, sagittal vertical axis; PT, pelvic tilt; T1PA, T1 pelvic angle. Note: Results are shown as mean ± standard deviation or the number of patients (%).
Because of these preoperative differences, the 2 groups were then propensity matched by age, PI, PI-LL, C7PL, and T1PA. After matching, there were 28 patients in each group. Subsequent analyses demonstrated that age, sex, classification, and all preoperative radiographic parameters were not statistically different between the groups (Table 1). Group S had a longer operating time than group L (504.9 vs. 366.2 min; P = 0.005). The EBL was greater in group S than in group L (1740.0 vs. 1288.4 mL), but the difference was not statistically significant (P = 0.278). The UIV distribution was not significantly different between the groups. The use of any osteotomy or 3CO was not different between the groups. Group S received more IBF with cage (67.9%) than group L (35.7%, P = 0.016). All patients in group S underwent distal fixation to the ilium (Table 2).
Operative Details and UIV Levels of the Matched Groups.
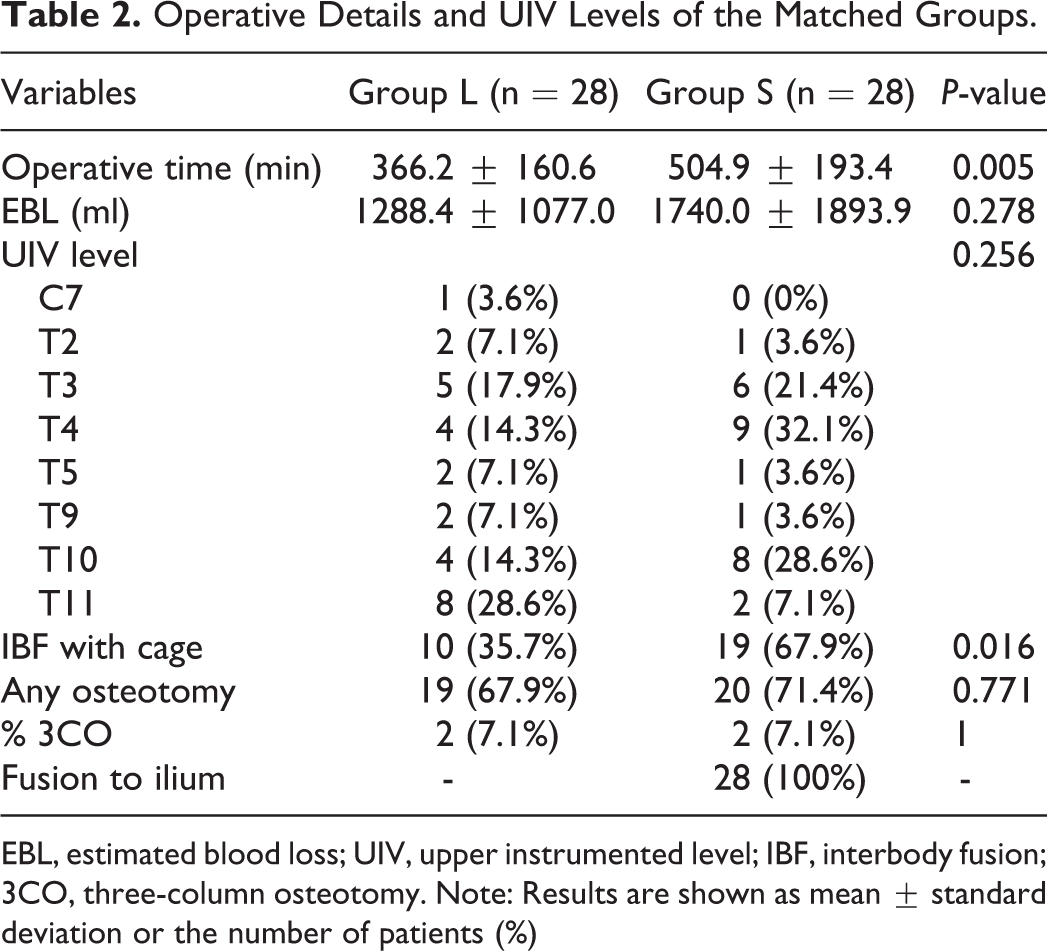
EBL, estimated blood loss; UIV, upper instrumented level; IBF, interbody fusion; 3CO, three-column osteotomy. Note: Results are shown as mean ± standard deviation or the number of patients (%)
Outcomes After Propensity Matching
Radiographic outcomes
The radiographic data showed that correction of sagittal alignment, including the PI-LL, PT, and SVA, was greater in group S than in group L at postoperative week 6 (Table 3). The incidence of radiographic PJK was higher in group S than in group L (64.3% vs. 32.1%; P = 0.031). At the 2-year follow-up, sagittal alignment was similar between the 2 groups (Table 3). The PJK angle in group S was greater than that in group L (-17.5° vs. -11.2°; P = 0.049). The incidence of PJK in both groups increased at the 2-year follow-up (78.6% in group S and 53.6% in group L; P = 0.089). The incidence of DJK in group L was 3.6% at postoperative week 6 and 7.1% at postoperative year 2. The DJK angle was stable during the 2-year follow-up period (24.4° and 28.8° at postoperative week 6 and year 2, respectively). The overall junctional kyphosis (PJK and DJK) was 35.7% in group L and 64.3% in group S at postoperative week 6 (P = 0.033) and 57.1% in group L and 78.6% in group S at postoperative year 2 (P = 0.086). Patients in group S had a significant and continuous change in radiographic parameters after surgery. The PT, LL, PI-LL, T1PA, and SVA were significantly improved by week 6, and a loss of correction was noticed at the 2-year follow-up (Figure 1).
Radiographic Outcomes of the Matched Groups.
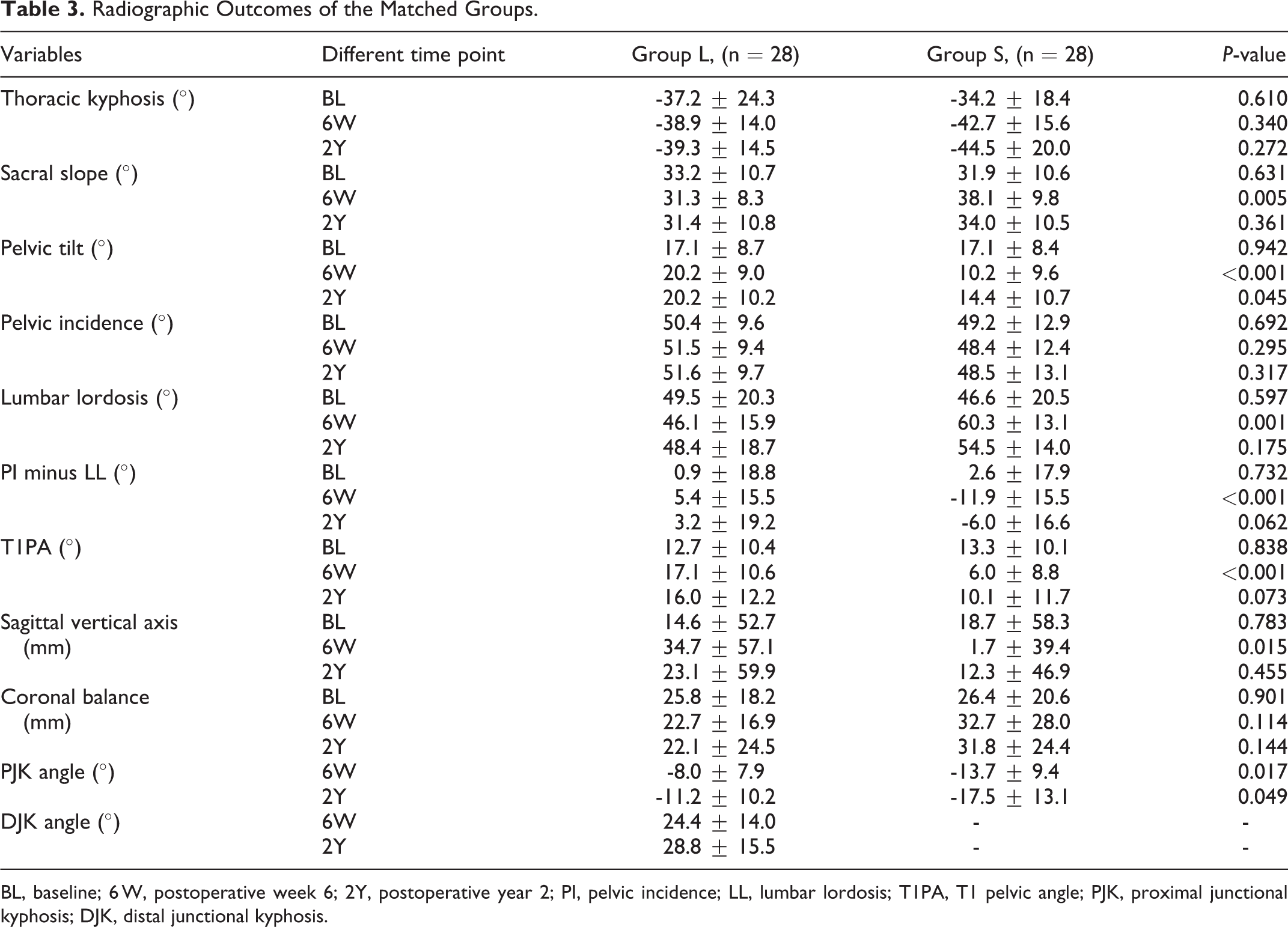
BL, baseline; 6 W, postoperative week 6; 2Y, postoperative year 2; PI, pelvic incidence; LL, lumbar lordosis; T1PA, T1 pelvic angle; PJK, proximal junctional kyphosis; DJK, distal junctional kyphosis.
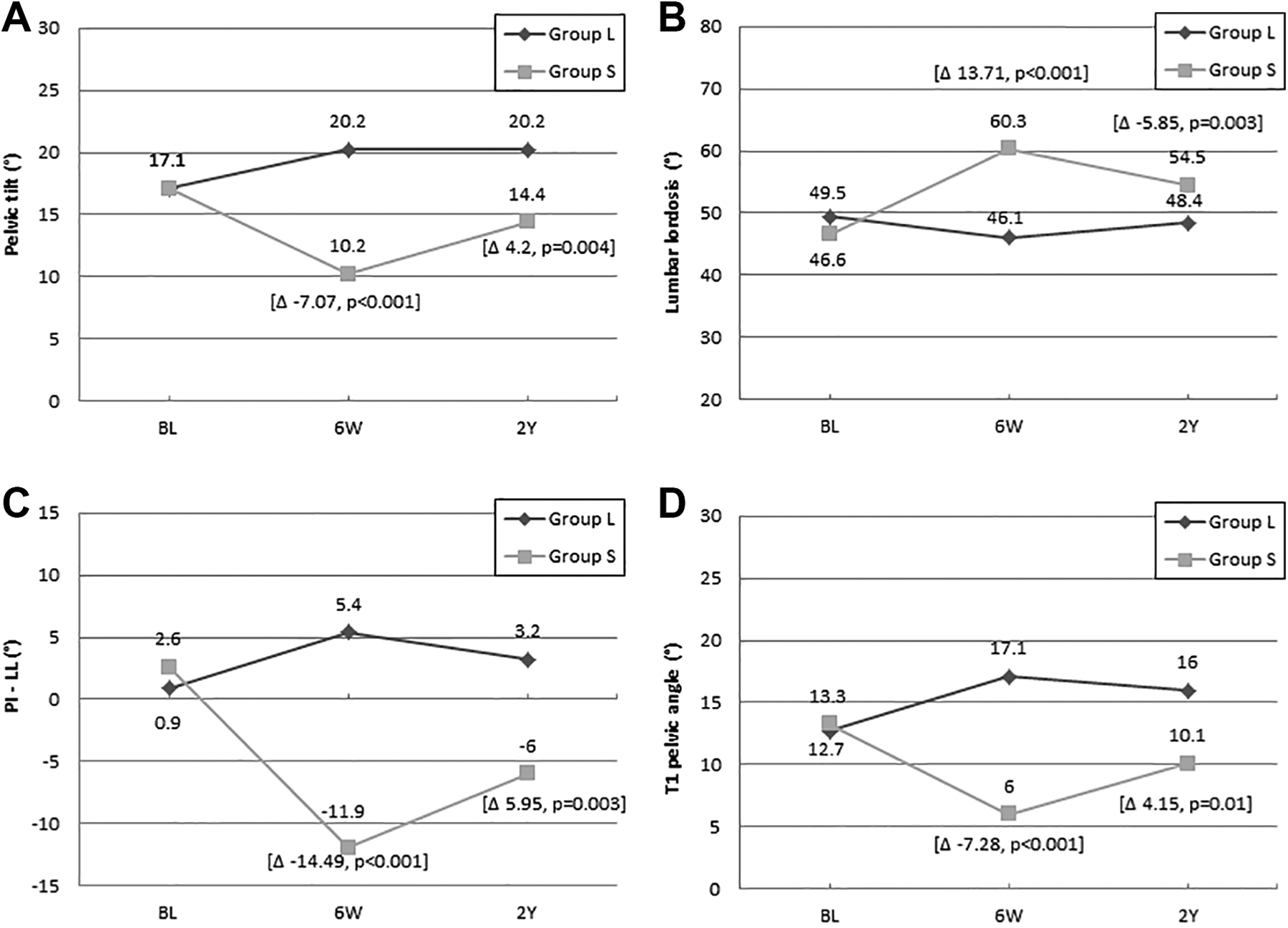
Significant changes in radiographic parameters between groups L and S (A) Pelvic tilting, (B) Lumbar lordosis, (C) PI minus lumbar lordosis, and (D) T1 pelvic angle at baseline and at each timepoint of follow-up. The numbers indicate the mean value of each score. Delta changes are shown for significant differences.
HRQOL
At baseline, the groups were well matched with regard to the SRS-total score (P = 0.189), ODI score (P = 0.116), and SF-MCS (P = 0.872). The SF-PCS was lower in group S than in group L (31.9 vs. 39.3; P = 0.007). At the 2-year follow-up, the SRS-total and ODI scores improved significantly in both groups. The SF-PCS only improved in group S, and the SF-MCS was not different between the groups. There were no significant differences between the groups for all 4 HRQOL outcomes (Table 4).
HRQOL Scores of the Matched Groups.
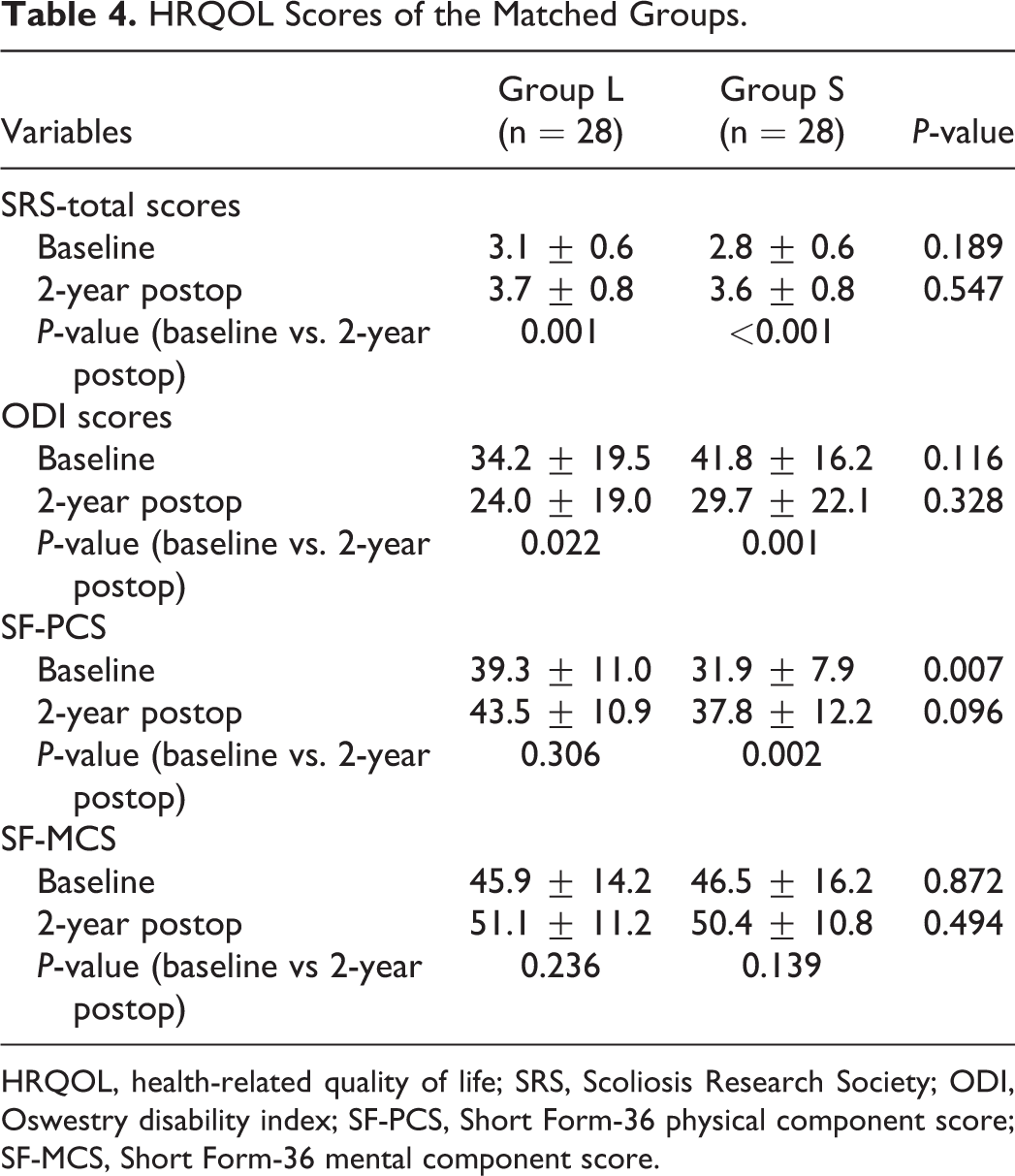
HRQOL, health-related quality of life; SRS, Scoliosis Research Society; ODI, Oswestry disability index; SF-PCS, Short Form-36 physical component score; SF-MCS, Short Form-36 mental component score.
Complications and revisions
The total number of major complications (10.7% vs. 28.6%; P = 0.177) and revision rate (25% vs. 35.7%; P = 0.562) were similar between groups L and S. Most of the revisions in group L were due to distal extension (71.4%). There was no difference in revisions due to PJK between the 2 groups (3.6% in group L vs. 10.7% in group S; P = 0.611). There was 1 revision due to DJK in group L, and the overall junctional failure was not significantly different between the 2 groups (7.1% in group L vs. 10.7% in group S; P = 1). There were no mortalities or recurrent revisions in either group (Table 5). Through subgroup analyses, 8 patients with L5 LIV in group L were identified. Of the 5 patients who needed revision, three patients needed revision due to distal extension, 1 patient needed revision due to painful implants, and 1 patient needed revision due to sagittal imbalance. The revision rate was 62.5% in the L5 LIV subgroup, while it was 12.5% in eight matched patients in group S (P = 0.119).
Complications and Revisions in the Matched Groups.
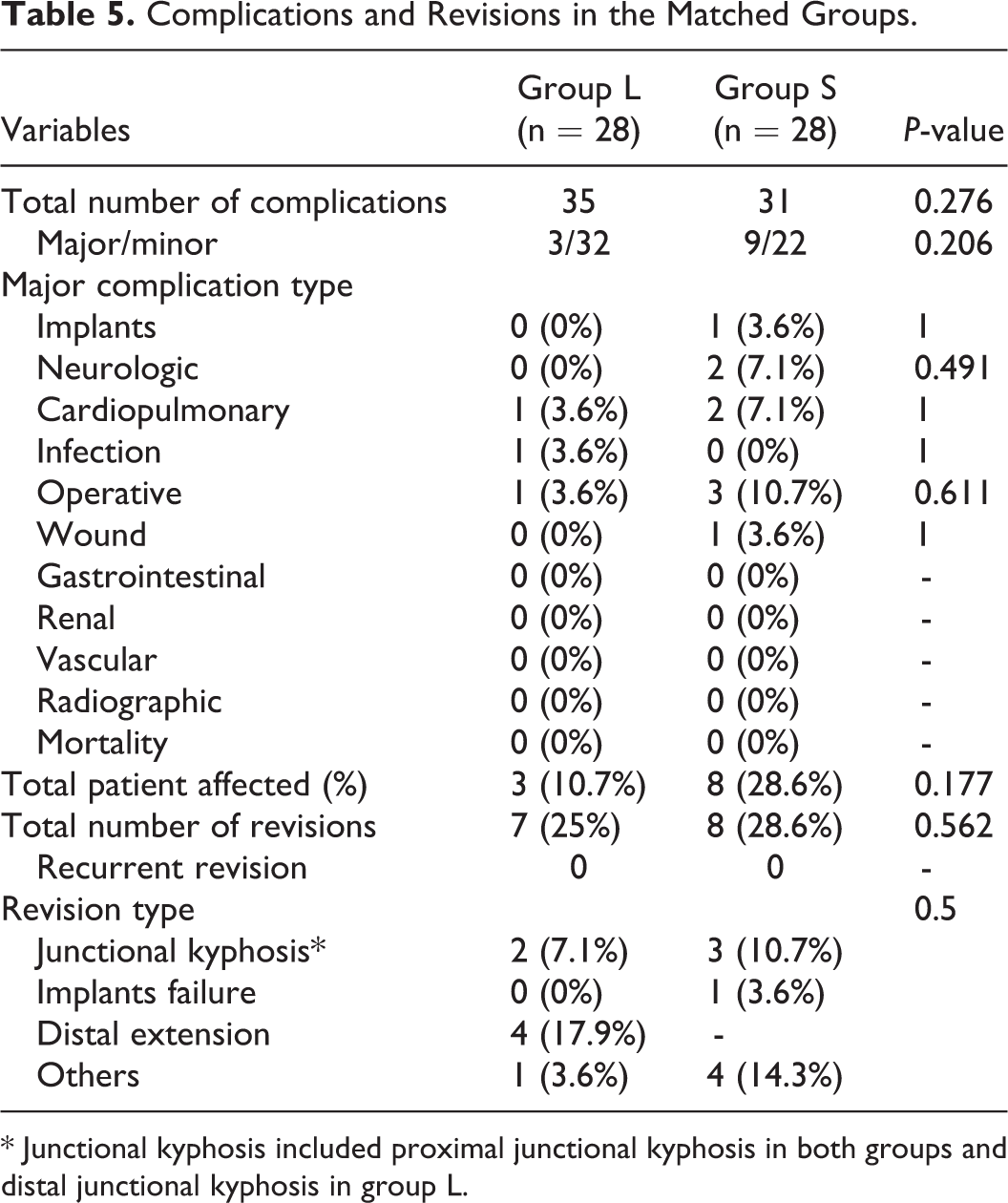
* Junctional kyphosis included proximal junctional kyphosis in both groups and distal junctional kyphosis in group L.
Discussion
To the best of our knowledge, this is the first propensity-matched study to compare the clinical and radiographic results between L4/L5 and S1/ilium LIVs. In the unmatched groups, age and deformity types were significantly different, which made it difficult to make strong comparisons. After matching, patients were of similar age (around 50 years old), had moderate coronal malalignment, had moderate-to-severe functional disability, had no severe sagittal malalignment, and mainly had lumbar or double coronal curves types. Our data showed that the correction of sagittal alignment was different between the 2 groups, with group S having significantly better sagittal deformity correction than group L (Table 3), although fusion to S1/ilium involved longer operative times and higher PJK rates. The overall complication rates, revision rates, and HRQOL scores were not different between the 2 groups.
Previous studies have reported better sagittal alignment correction in patients with S1 LIV. Edwards et al. 3 investigated L5 LIV versus S1 LIV and found that the postoperative SVA was superior in their sacrum cohort. Cho et al. 1 reported more LL restoration with S1 LIV compare to L5 LIV, mainly due to the greater L5–S1 lordotic angle restoration and greater loss of correction in group L. They suggested that for patients with sagittal misalignment and lumbar hypolordosis, L5–S1 should be included in the fusion even if the L5–S1 disc has minimal degeneration. Performing rigid sacropelvic fixation with iliac screws or S2 alar-iliac screws could also improve correction by increasing the biomechanical strength of LIV fixation. Yasuda et al. 16 found that the correction of sagittal parameters, including SVA, LL, and PT, was better with iliac screws for LIV fixation than with non-iliac screws. They also found that the lumbosacral failure rate significantly decreased when using iliac screws and recommended fusion to the ilium for long spinal fusion in ASD. Our data confirmed that the correction of sagittal parameters was better in S1/ilium LIV than in L4/L5 LIV.
We found that sagittal alignment restoration was maintained in group L, while significant loss of correction was found in group S at the 2-year follow-up (Figure 1). One explanation of the sagittal decompensation in group S was the higher postoperative PJK angle in group S than in group L. Sagittal decompensation has been attributed to the increase in kyphosis at the unfused spine, such as reciprocal change of TK or junctional kyphosis. 17 A previous study has reported that in ASD patients with L5 LIV, collapse of the remaining distal disc may cause distal junctional kyphosis and result in sagittal decompensation. 18 However, we did not find correction loss in group L, and the DJK angle was maintained because of the young population and relatively short follow-up period in our series. Loss of correction over the fused segments has been reported in the literature. Banno et al. 19 reported a loss of correction of 27% among 63 patients with ASD with lower thoracic fusion to the pelvis. They reported that greater body mass index, high-grade osteotomies, and use of titanium rods were associated with a loss of correction that resulted in sagittal malalignment (higher T1PA, SVA, and PT after 2 years). In another study, the authors reported that loosening of the iliac screw indicated instability of the lumbosacral junction that could result in sagittal malalignment and a poor outcome. 20
Risk of revision is one of the most important considerations in the selection of the distal fusion level and in the inclusion or exclusion of the sacrum. The total revision rate was higher in patients with distal fixations to the sacrum than in patients with distal fixations to L5.21,22 The revision rate of ASD surgery has been reported to range from 12.5% to 15.4% within the first year,10,11 28.2% within 2.1 years, 12 and 32% within 3.3 years of follow-up. 6 The reasons for revision include implant-related complications, PJK, infection, pseudoarthrosis, and adjacent segment degeneration. In patients with an LIV of L4 or L5, symptomatic adjacent segment degeneration and the need for extension to the sacrum are the major indications for revision. The reported revision rate for extension to the sacrum is 23%. 23 However, in our study, it was 17.9%, which accounted for 71.5% (5 of 7) of all the revisions performed in group L. The reported rate of L5–S1 pseudoarthrosis is 17%–42%.2-6 The higher rates of pseudarthrosis and complications in patients with fusion extending to the sacrum were due to high mechanical demand and relatively low bone marrow density in the sacrum. Our data showed no difference in the rate of pseudoarthrosis between the 2 groups. This may be because all patients in our matched group S underwent sacropelvic fixation and had greater rates of IBF with cage than those in group L. According to the literature, interbody fusion and rigid sacropelvic fixation could provide better anterior support to the sacral screws, leading to decreased pseudarthrosis and screw loosening at the lumbosacral junction.1,8,9,16,18
Fusion of longer segments to the sacrum or ilium is a risk factor for PJK. The etiology of PJK is multifactorial and includes surgical, radiographic, and patient-related risk factors. The reported PJK rate after ASD surgery ranges from 20% to 39%.24-27 Sacrum LIV has been reported to increase the risk of PJK more than lower lumbar LIV. 26 Yagi et al. 27 reported a 30% increased PJK incidence when the LIV extended to the sacrum. In this study, the rates of radiographic PJK and PJK angle were significantly higher in group S than in group L at the 6-week and 2-year follow-ups. This may be due to the greater LL and SVA correction postoperatively, which have been considered risk factors for PJK by Kim et al. 28 The revision rate for PJK was higher in group S (10.7%) than in group L (3.6%), but the difference was not statistically significant.
The choice of LIV is controversial. Fusion ending at L5 may result in retention of lumbosacral motion, reduction of sacroiliac joint stress, decrease in operative time, avoidance of extensive dissection, and decrease in the risk of pseudarthrosis.29,30 Nonetheless, the risk of adjacent segment disease is high (68% reported by Kuhns et al. 23 ), and the rate of revision involving extension to the sacrum is 23%. 23 Generally, the indications for fusion to the sacrum or ilium are L5–S1 spondylolisthesis, previous L5–S1 surgery, existing L5–S1 stenosis, subluxation of L5 (>15°), and a severely degenerated disc. 7 Fusion ending at S1 could lead to higher rates of lumbosacral failure and revision than that ending at L5.1-5 Currently, the increased use of rigid sacropelvic fixation could reduce the rate of pseudoarthrosis and increase correction of sagittal deformity.16,31 In line with the current literature, worse spinal deformity and older age, which were associated with the unmatched group S, could have also increased the risk of revision. The revision rate was comparable in the matched groups including patients of a similar age (approximately 50 years) and with moderate deformities. However, the reasons for revision were different in the 2 groups; more distal extensions accounted for revisions in group L, whereas more PJK accounted for revisions in group S. We, therefore, suggest that decisions regarding L4/5 versus S1/ilium as the distal fusion ends for LIV should be largely based on the risks involved in deformity correction and revision surgeries. For patients with preserved distal discs with low risks of distal junctional failure, stopping the LIV at L4/5 could be considered. For patients needing extended fusion to the sacrum, the use of ilium or pelvic fixation is recommended to increase stability of the lumbosacral junction.
This study has several limitations. First, the number of matched patients was low. Second, the detailed procedures involved in the surgery were not analyzed, such as the type or level of osteotomy, type of fusion, or multiconstructs. Finally, the post-matched groups in this study were not necessarily representative of all adult patients with deformity since the post-matched patients were limited to those aged approximately 50 years with moderate coronal misalignment, moderate-to-severe functional disability, no severe sagittal malalignment, and mainly lumbar or double coronal curve types.
Conclusion
More fusions to S1 or the ilium were performed in older patients with larger sagittal plane deformities than fusions to L4 or L5. After propensity matching, patients in group S had better sagittal alignment restoration after surgery than those in group L. There was some deterioration of the sagittal parameters over time in group S, but the HRQOL scores between the 2 groups at all timepoints were similar. Fusion to S1/ilium involved a longer operating time, higher rates of PJK, and greater postoperative PJK angle than fusion to L4 or L5. The clinical outcomes and rates of revision surgery and complications were similar between the 2 groups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the International Spine Study Group foundation; Yu-Cheng Yao was supported by Taipei Veterans General Hospital - National Yang-Ming University Excellent Physician Scientists Cultivation Program, No. 108-V-A-010.