
Abstract
Study Design:
Cross-sectional.
Objectives:
To evaluate the perception and satisfaction among adolescent idiopathic scoliosis (AIS) patients on Neck Tilt with Medial Shoulder Imbalance and Lateral Shoulder Imbalance.
Methods:
Lenke 1 and 2 AIS patients were stratified into 6 groups of preoperative/ postoperative Balanced (
Results:
A total of 120 Lenke 1 and 2 AIS patients were recruited.
Conclusion:
NT and LSI were major concerns among AIS patients. Both
Keywords
Introduction
Postoperative shoulder imbalance (PSI) is a common phenomenon among adolescent idiopathic scoliosis (AIS) patients. The incidence of PSI was reported to be as high as 25%. 1 The radiological aspects of shoulder imbalance among AIS patients have been well appraised. Coracoid height difference (CHD), clavicle-rib intersection distance (CRID), clavicle angle (Cla-A) and radiographic shoulder height (RSH) are recognized radiological parameters that correlated with shoulder imbalance.2-5 Several studies reported the relation of clinical shoulder imbalance to its radiological parameters. Kuklo et al. 2 proposed a clinical shoulder grading based on RSH where difference in shoulder height of <1 cm was defined as Grade 0 (balanced), 1-2 cm was Grade 1 (minimal imbalance), 2-3 cm was Grade 2 (moderate imbalance) and >3 cm was classified as Grade 3 (significant imbalance). Ono et al. 3 subsequently reclassified shoulder imbalance into medial shoulder imbalance and lateral shoulder imbalance. Medial shoulder imbalance was reflected by T1 tilt, first rib angle and upper thoracic curve size whereas lateral shoulder imbalance was correlated to Cla-A. Kwan et al. 4 introduced a clinical neck tilt classification based on the presence of neck tilt and trapezius muscle height difference which were corresponding to the T1 tilt and Cervical Axis (CA). Grade 0 was defined as no neck tilt, Grade 1 was correctable neck tilt with equal trapezius muscle height, Grade 2 was non-correctable neck tilt with trapezius muscle height difference of ≤1 cm and Grade 3 was non-correctable neck tilt with trapezius muscle height of >1 cm. Neck tilt was later recognized as a common phenomenon among preoperative and postoperative AIS patients.6-8
Surgeons’ primary aim had always been correcting the coronal curvature. However, PSI became a concern as patients’ perspective on their postoperative appearances including shoulder balance was found to be imperative in determining the cosmetic outcomes of the surgery8-21,22 The focus of surgical concern was then shifted to achieve a balanced postoperative shoulder instead. Various methods were introduced to circumvent PSI such as upper thoracic spine leveling, upper instrumented vertebra (UIV) level selection, UIV tilt angle, fusion level selection, preoperative shoulder balance, proximal thoracic (PT) correction rate and its extent of correction of main thoracic (MT) curve.9-17
Nevertheless, the effects of neck and shoulder imbalance on patients’ clinical outcomes in terms of their self-awareness, satisfaction and perception of severity had not been well established. Most of the studies listed spinal deformity aspects such as body curves, rib prominence and shoulder balance as factors taken into account of the patients’ perception and satisfaction.18-21 However, patients’ perception of neck imbalance was not reported. Hence, the purpose of this study was to determine the perception and satisfaction among preoperative/ postoperative AIS patients with regard to Neck Tilt with Medial Shoulder Imbalance (NT) as compared to Lateral Shoulder Imbalance (LSI), and its influence on patients’ Health Related Quality of Life (HRQoL).
Methods
This was a cross-sectional study conducted in a single academic institution. Ethical approval was obtained from University Malaya Medical Centre Medical Research Ethics Committee (20171030-5719). Patients were recruited consecutively in outpatient settings. Inclusion criteria were preoperative or postoperative AIS patients with Lenke 1 or 2 curve type, who had either isolated Balanced Neck and Shoulder
Patients who met the inclusion criteria were identified by three different spine consultants (MKK, CYWC, CKC) in the outpatient setting. Patients who fit either one of the categories were shown figures of Balanced Neck and Shoulder
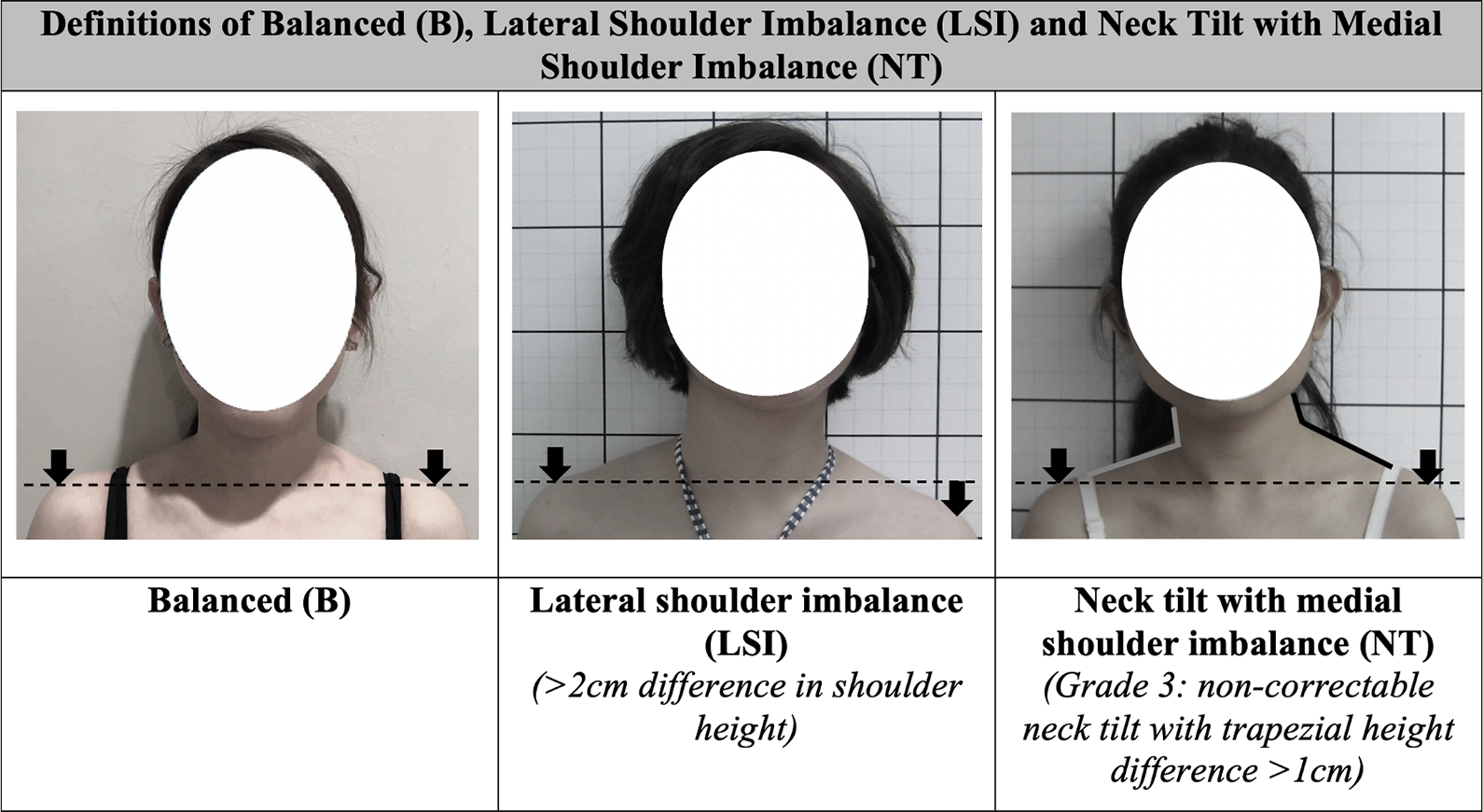
Definitions of Balanced (B), Lateral Shoulder Imbalance (LSI) and Neck Tilt with Medial Shoulder Imbalance (NT).
The Objectives of This Study
To evaluate the perception and satisfaction among preoperative/ postoperative AIS patients with regard to clinical NT and LSI.
To determine the radiological parameters of AIS patients with NT and LSI.
To study the influence of NT and LSI on patients’ HRQoL based on SRS-22r scores.
Demographic data collected were age, gender, height, weight and body mass index (BMI). Data collected and measured was Lenke classification, proximal thoracic (PT), main thoracic (MT)/ lumbar (L) Cobb angle, coronal balance (CB), T1 tilt angle, CA, Cla-A, RSH, UIV tilt angle and lowest instrumented vertebra (LIV) tilt angle. The radiological parameters listed were measured preoperatively and postoperatively using a digital software (Centricity PACS, version 5.0, GE Healthcare, Chicago, IL, USA).
For the radiological parameters listed, positive values signified right sided tilting whereas negative values signified left sided tilting. Definitions of relevant radiological parameters were described as below: T1 tilt angle: the angle between a line drawn parallel to the upper end-plate of T1 vertebra and a horizontal reference line (in degree). Cervical Axis (CA): the angle between a longitudinal axis of cervical spine (center of C2 odontoid process and center of C7) with a vertical reference line (in degree). Clavicle Angle (Cla-A): the angle that is subtended between a horizontal reference line (which is drawn perpendicular to the lateral edge of the radiograph and touches the most cephalad portion of the elevated clavicle) and a line which touches the most cephalad aspect of both the right and left clavicles (in degree). Radiographic Shoulder Height (RSH): the difference between the level of soft tissue shadow above the acromioclavicular joint at both ends and the horizontal line (in millimeters).
Statistical Analysis
All data was analyzed using SPSS software version 22.0 (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp). Continuous variables were described as mean ± standard deviation and analyzed using one-way analysis of variance (ANOVA). Categorical variables were presented in frequency as well as percentage and further analyzed using Fisher’s exact test. For neck and shoulder questionnaires, Fisher’s exact test was performed separately for preoperative groups and postoperative groups. For the post-hoc pairwise comparisons of neck and shoulder questionnaires, the Bonferroni corrected threshold for statistical significance was α < .017. 23
Results
Our study population was consistent with AIS population where there was a female predominance (85.8%). The mean age of patients at the time of recruitment was 18.0 ± 6.3 years old. Majority of the patients (65.8%) had Lenke 1 curve type. The mean height was 156.9 ± 7.8 cm with the average weight of 44.6 ± 7.8 kg (Table 1). The mean preoperative and postoperative T1 tilt were 6.2 ± 5.1° and 4.4 ± 5.0° respectively. Mean preoperative and postoperative CA were 3.6 ± 2.9° and 3.4 ± 3.1°, respectively. Preoperative and postoperative Cla-A were 2.9 ± 2.4° and 2.3 ± 1.7°, whereas preoperative and postoperative RSH were 12.7 ± 9.2 mm and 10.0 ± 7.8 mm, respectively. The mean UIV tilt angle in this study was -3.7 ± 7.0° and the LIV tilt angle was 4.7 ± 4.9º (Table 2).
Demographic Data (n = 120).
Radiological Parameters.
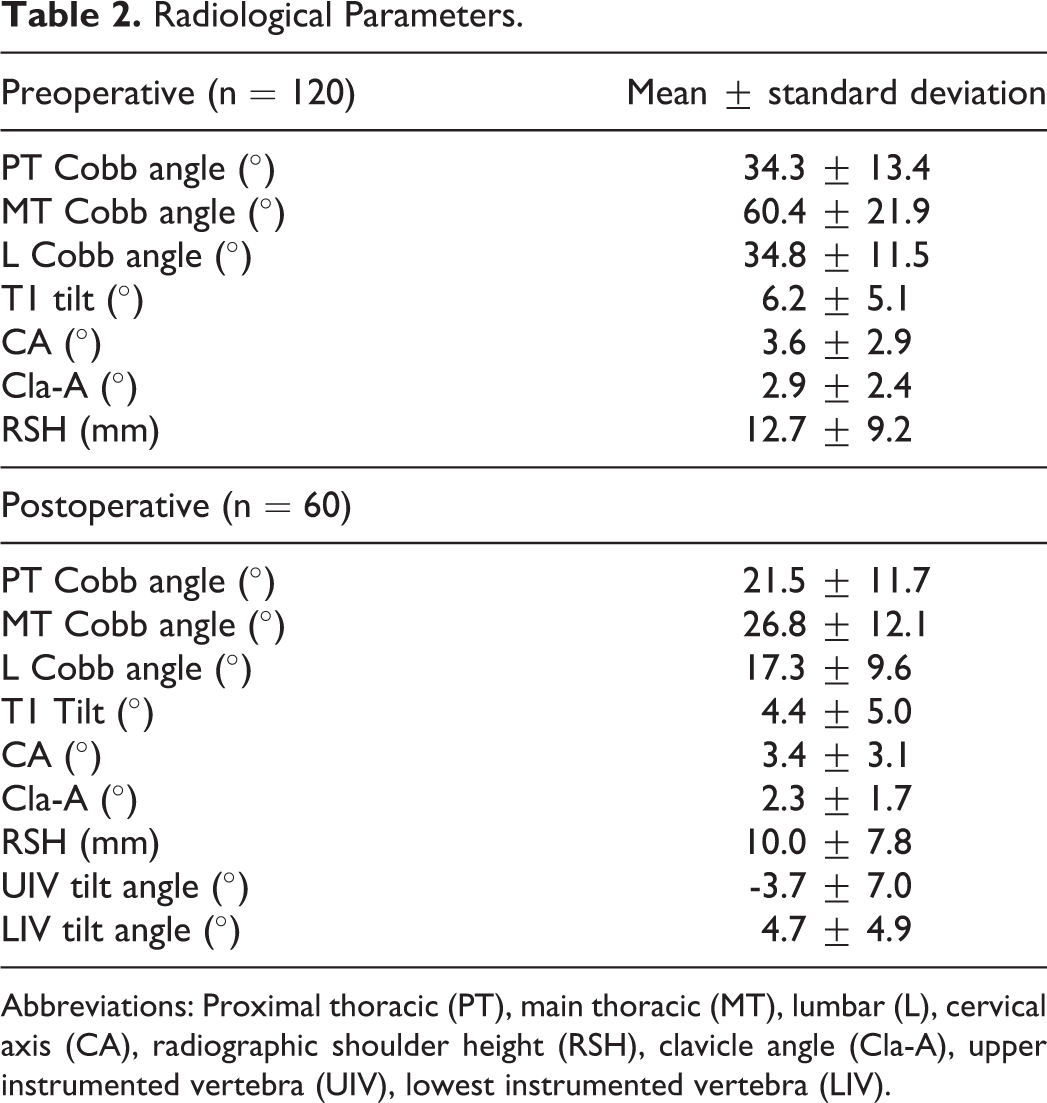
Abbreviations: Proximal thoracic (PT), main thoracic (MT), lumbar (L), cervical axis (CA), radiographic shoulder height (RSH), clavicle angle (Cla-A), upper instrumented vertebra (UIV), lowest instrumented vertebra (LIV).
Neck Questionnaire
Preoperative Groups
In comparison of responses for preoperative B, LSI and NT groups to the neck appearance question, all patients in the B group and 95% of the LSI group acknowledged the neck as balanced preoperatively. However, none of the patients in NT group acknowledged their neck as balanced preoperatively where 45% of them noticed it tilted slightly right and 25% of them noticed it tilted slightly left (Figure 2a).
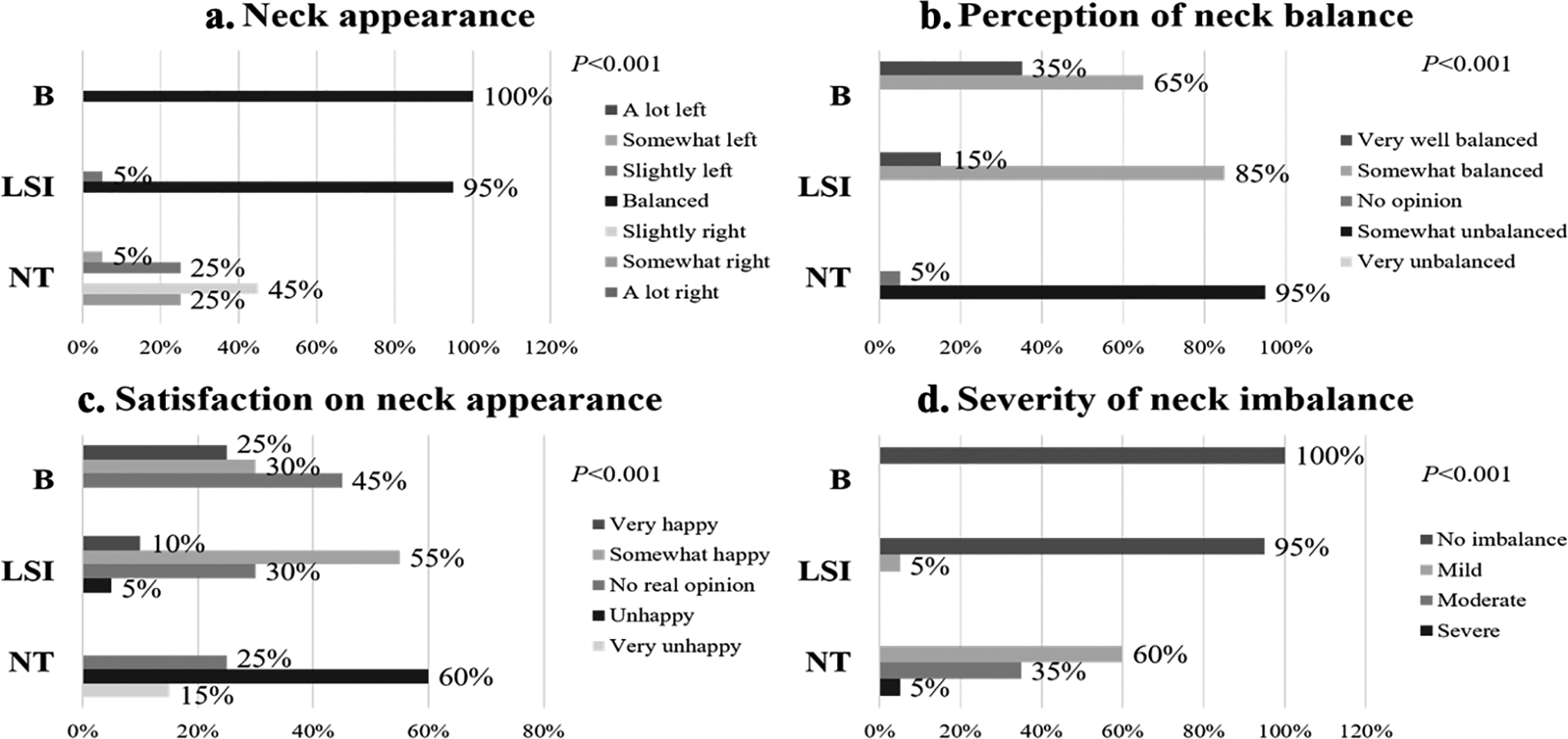
Neck appearance (a), perception of neck balance (b), satisfaction (c) and severity of neck imbalance (d) among preoperative Balanced (B), Lateral Shoulder Imbalance (LSI) and Neck Tilt with Medial Shoulder Imbalance (NT) groups (n = 60).
With regard to the perception of neck balance, 65% of the B group perceived it as somewhat balanced and 35% of them perceived it as very well balanced. 85% of the LSI group perceived it as somewhat balanced. In contrast, 95% of the NT group perceived their neck as somewhat unbalanced (Figure 2b).
Majority of the preoperative B group (45%) had no real opinion and 30% of them were somewhat happy about their neck appearance. Majority of the LSI group (55%) were somewhat happy with their neck balance. Meanwhile, most of the NT group patients (60%) were unhappy about their neck appearance (Figure 2c). All patients in the B group and 95% of the LSI group graded the severity of neck imbalance as no imbalance. On the contrary, majority of the NT patients (60%) graded the severity of neck imbalance as mild (Figure 2d).
Significant differences were found between the responses of preoperative B versus NT group, LSI versus NT group and comparison of all three preoperative B, LSI and NT groups in terms of the neck appearance, perception of neck balance, satisfaction of neck appearance and severity of neck imbalance questions (P < .001). Nevertheless, no significant difference was detected between the B and LSI group for all neck questions (Table 3).
P Values for Neck and Shoulder Questionnaires Comparing Preoperative/ Postoperative B, LSI and NT Groups.
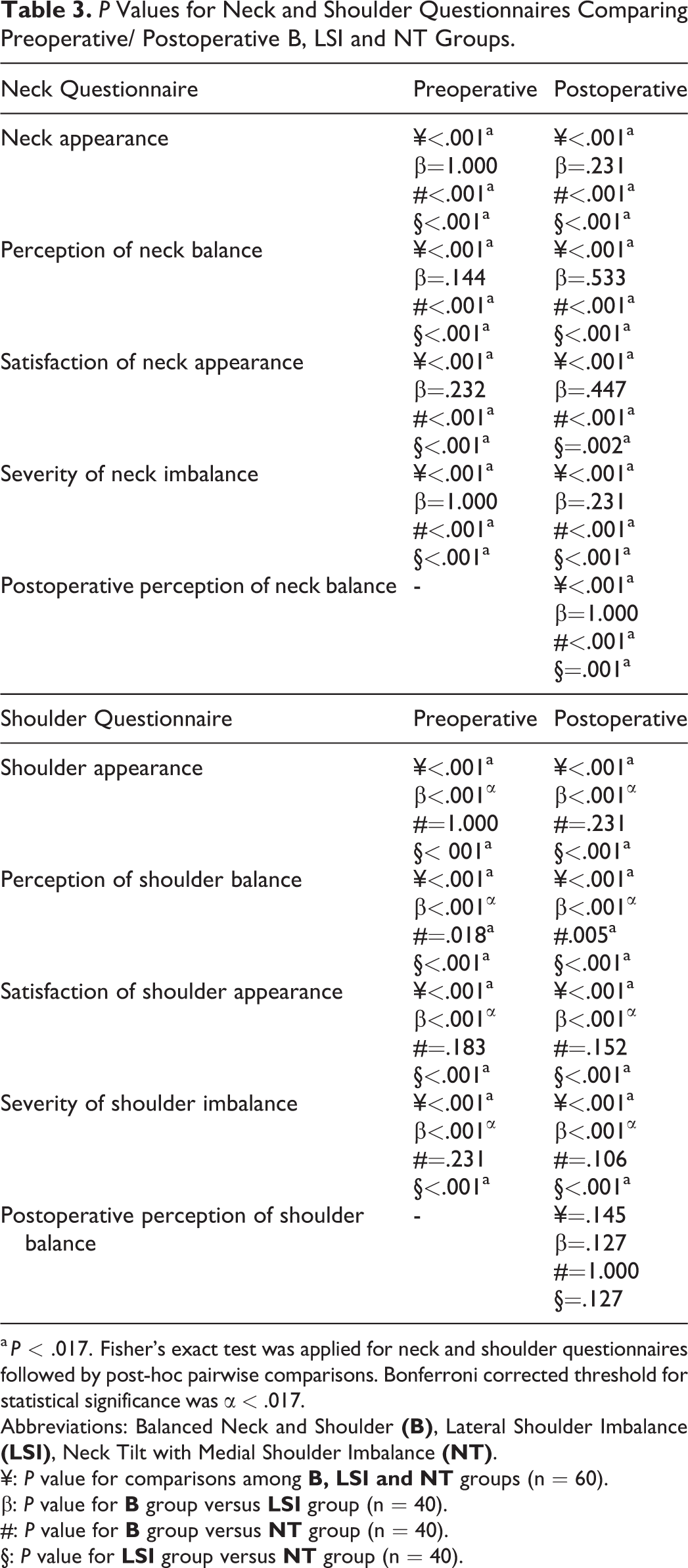
a P < .017. Fisher’s exact test was applied for neck and shoulder questionnaires followed by post-hoc pairwise comparisons. Bonferroni corrected threshold for statistical significance was α < .017.
Abbreviations: Balanced Neck and Shoulder
¥: P value for comparisons among
β: P value for
#: P value for
§: P value for
Postoperative Groups
All patients in postoperative B group and 85% of the patients in postoperative LSI group acknowledged their necks as balanced postoperatively. Nevertheless, none of the patients in postoperative NT group acknowledged their neck as balanced postoperatively where 60% of them noticed it tilted slightly to the right and 20% noticed it tilted slightly to the left (Figure 3a).
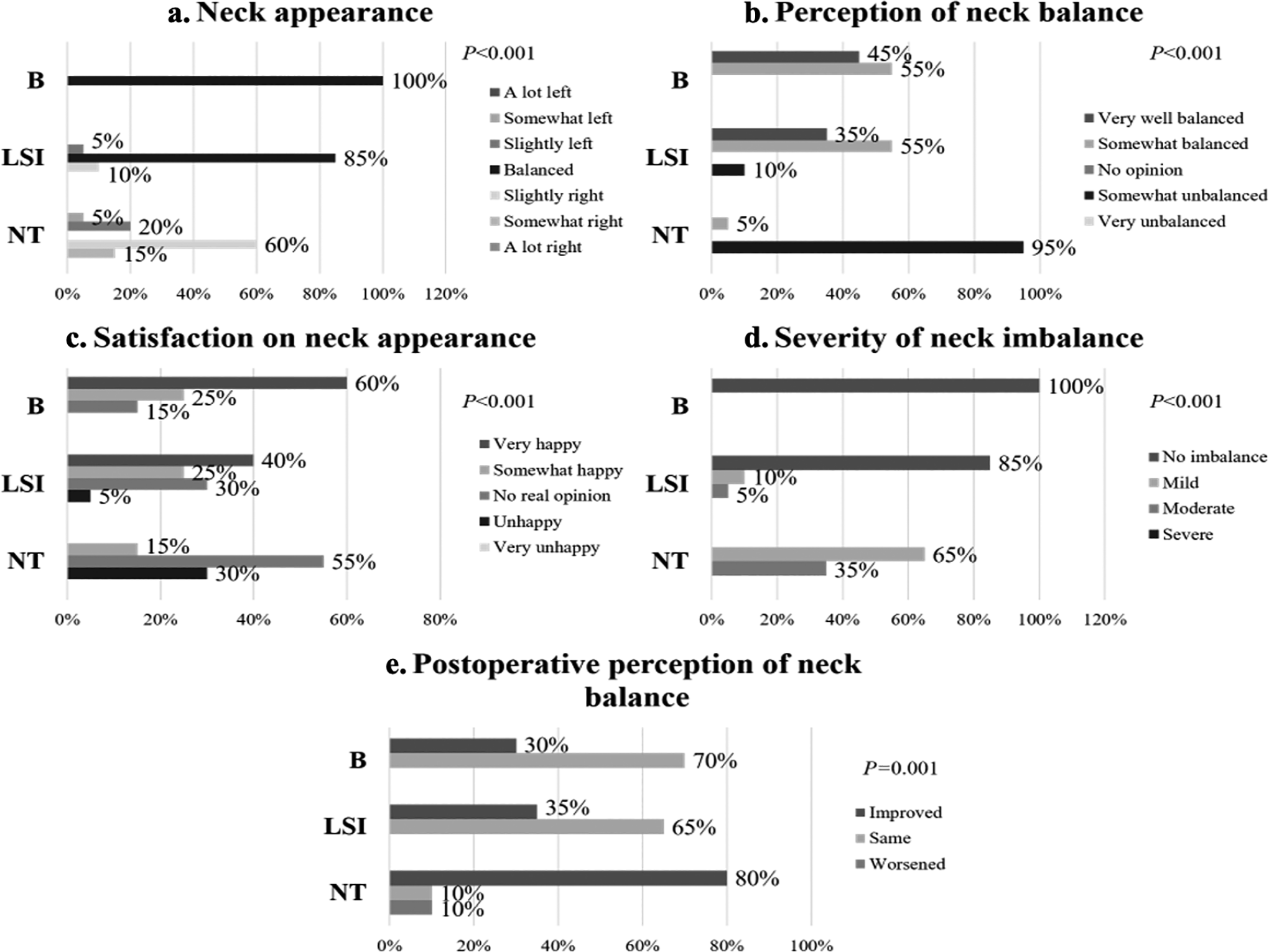
Neck appearance (a), perception of neck balance (b), satisfaction (c), severity of neck imbalance (d) and postoperative perception of neck balance (e) among postoperative Balanced (B), Lateral Shoulder Imbalance (LSI) and Neck Tilt with Medial Shoulder Imbalance (NT) groups (n = 60).
Majority of patients in both B group (55%) and LSI group (55%) perceived their neck as somewhat balanced. On the other hand, most of the postoperative NT patients (95%) perceived their neck appearances as somewhat unbalanced (Figure 3b). Majority of the B group (60%) and LSI group (40%) were very happy about their neck appearance. Meanwhile, 55% of the NT group patients had no real opinion about their neck appearance and 30% of them were unhappy about it (Figure 3c). All patients in the B group and 85% of the patients in LSI group graded the severity of neck imbalance as no imbalance (P < .001). 65% of the patients in NT group graded it as mild imbalance whereas 35% of them graded it as moderate imbalance (Figure 3d).
Majority of the patients in B group (70%) perceived that their neck balance remained the same postoperatively while 30% of them felt that it had improved. 65% of the patients in LSI group perceived that their neck balance remained the same postoperatively. 80% of the NT group patients perceived that their neck balance improved postoperatively whereas 10% considered it remained the same and 10% of them perceived that it had worsened postoperatively (Figure 3e).
There were significant differences found between the responses of postoperative B versus NT group, LSI versus NT group and comparison of all three postoperative B, LSI and NT groups to the neck appearance, perception of neck balance, satisfaction of neck appearance, severity of neck imbalance and postoperative perception of neck balance questions respectively (P < .01) However, no significant difference was found between B and LSI group for all neck questions (Table 3).
Shoulder Questionnaire
Preoperative Groups
All patients in preoperative B group and 95% of the patients in preoperative NT group were aware of their balanced shoulders preoperatively. On the other hand, none of the LSI group patients acknowledged their shoulders as balanced preoperatively where 40% noticed their right shoulders were slightly raised and 20% noticed their left shoulders were slightly raised (Figure 4a).
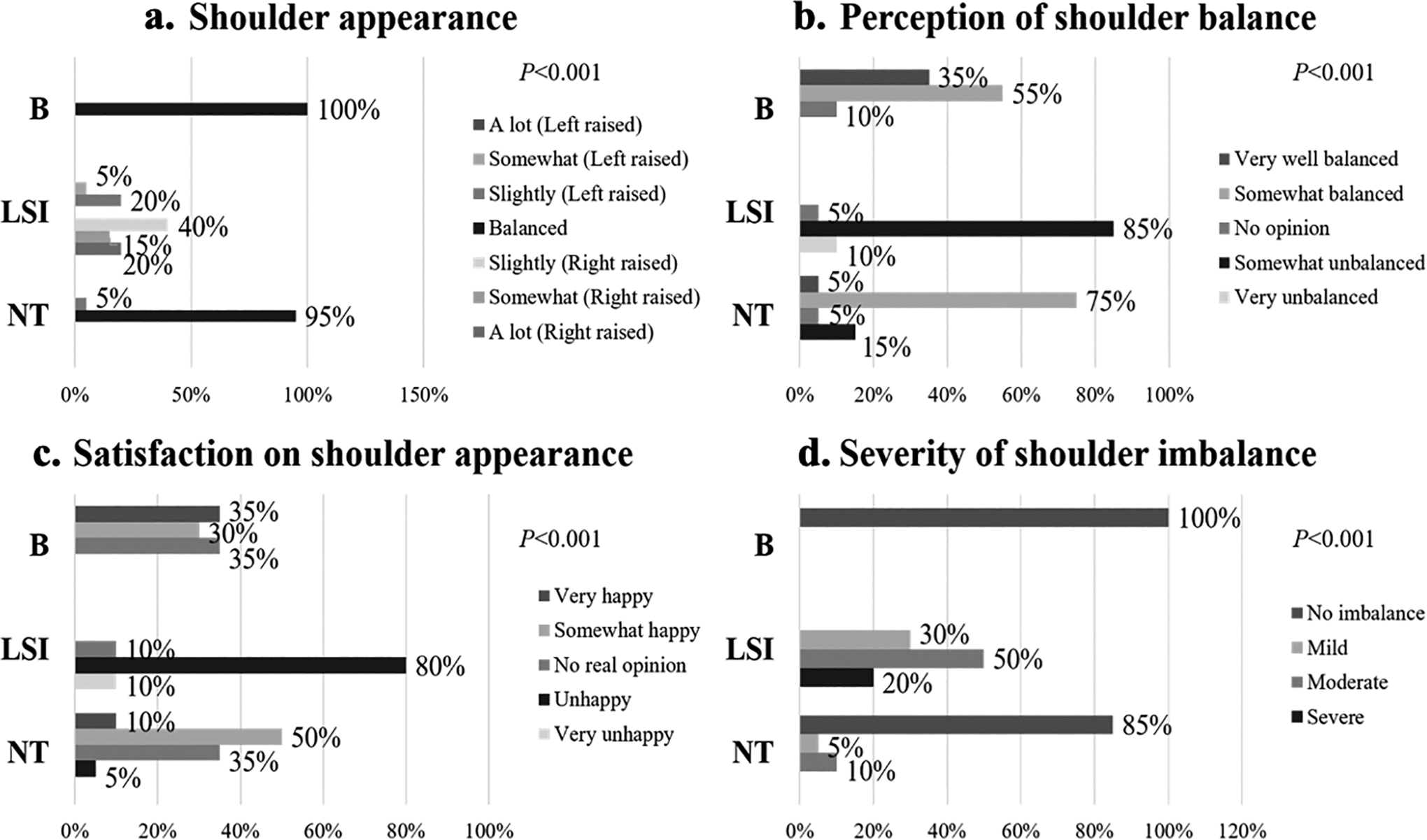
Shoulder appearance (a), perception of shoulder balance (b), satisfaction (c) and severity of shoulder imbalance (d) among preoperative Balanced (B), Lateral Shoulder Imbalance (LSI) and Neck Tilt with Medial Shoulder Imbalance (NT) groups (n = 60).
55% of the patients in B group and 75% of NT group patients perceived their shoulders as somewhat balanced. Meanwhile, most of the LSI group patients (85%) perceived their shoulders as somewhat unbalanced and 10% of them rated it as very unbalanced (Figure 4b). Majority of the patients in B group were very happy (35%) or had no real opinion (35%) about their shoulder appearances. 50% of the NT group patients were somewhat happy and 35% of them had no real opinion about their shoulder balance. Conversely, majority of the patients in LSI group (80%) were unhappy about their shoulder appearances (Figure 4c).
All preoperative B group patients and 85% of the NT group patients graded their shoulders as no imbalance. On the contrary, 50% of the LSI patients graded their shoulders as moderate imbalance, 30% of them graded it as mild and 20% of them graded it as severe (Figure 4d).
Statistically significant differences were identified between the responses of preoperative B versus LSI group, LSI versus NT group and comparison of all three preoperative B, LSI and NT groups in terms of the shoulder appearance, perception of shoulder balance, satisfaction of shoulder appearance and severity of shoulder imbalance questions (P < .05). Meanwhile, no significant difference was found between B and NT group for all shoulder questions other than the perception of shoulder balance question (P = .018) (Table 3).
Postoperative Groups
All patients in postoperative B group and 85% of the postoperative NT group patients acknowledged their balanced shoulders postoperatively. However, none of the patients in postoperative LSI group acknowledged their shoulders as balanced postoperatively where 65% noticed their left shoulders were slightly raised and 20% noticed their right shoulders were slightly raised (Figure 5a).
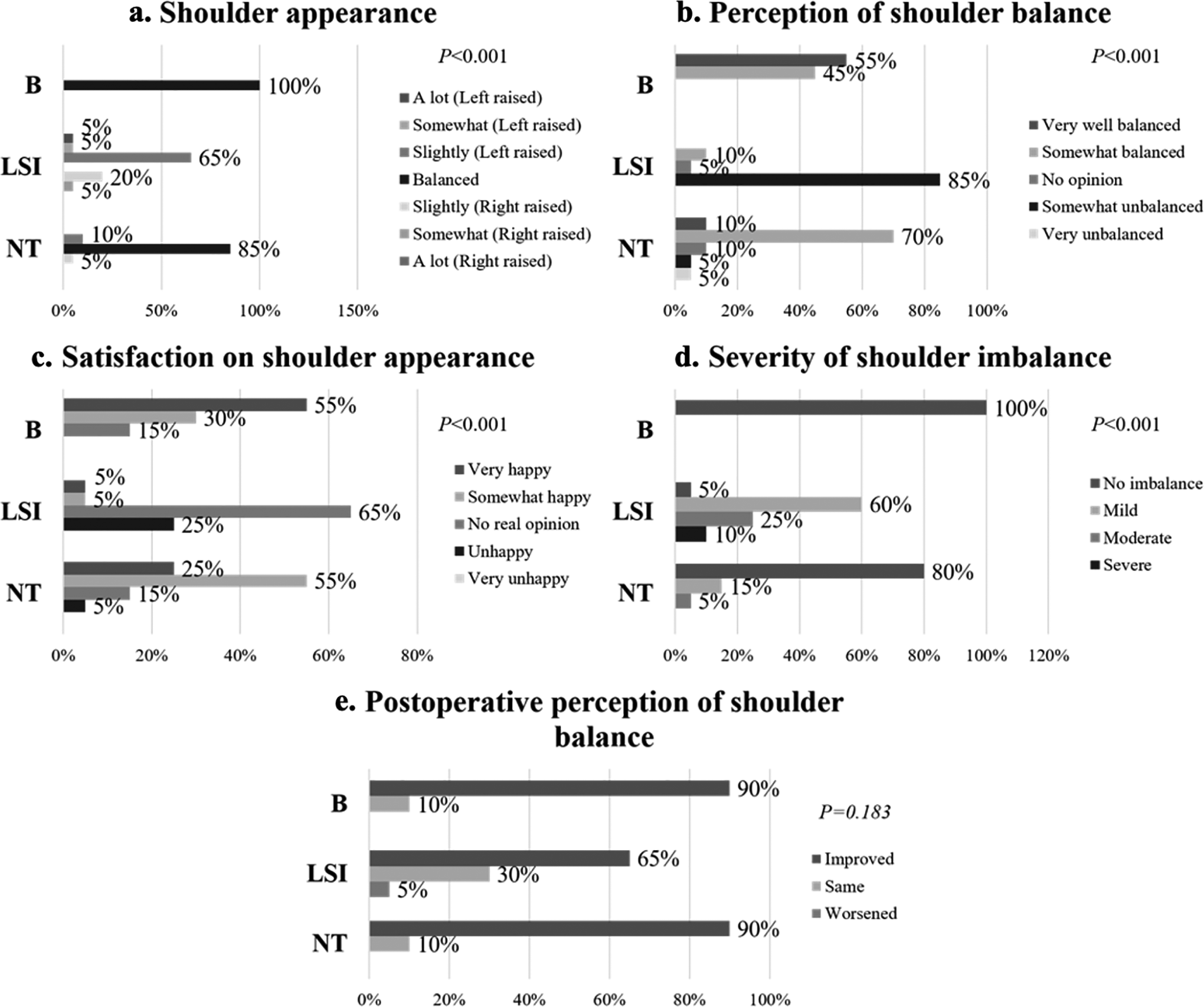
Shoulder appearance (a), perception of shoulder balance (b), satisfaction (c), severity of shoulder imbalance (d) and postoperative perception of shoulder balance (e) among postoperative Balanced (B), Lateral Shoulder Imbalance (LSI) and Neck Tilt with Medial Shoulder Imbalance (NT) groups (n = 60).
Most of the patients in B group (55%) perceived their shoulders as very well balanced and 70% of the patients in NT group perceived it as somewhat balanced. Meanwhile, 85% of the postoperative LSI group perceived their shoulders as somewhat unbalanced (Figure 5b). Majority of the patients in B group (55%) were very happy about their shoulder appearances. Similarly, majority of the patients in NT group (55%) were somewhat happy about their shoulder appearances. In contrast, 65% of the LSI group patients had no real opinion and 25% of them were unhappy about their shoulder appearances (Figure 5c). All patients in postoperative B group and 80% of the patients in NT group graded the severity of shoulder imbalance as no imbalance whereas 60% of the LSI group patients graded their shoulder imbalance as mild and 25% of them graded it as moderate (Figure 5d).
90% of the patients in both postoperative B group and NT group as well as 65% of the patients in LSI group perceived that their shoulder balance improved postoperatively. Meanwhile, 30% of the LSI group patients considered it remained the same (Figure 5e).
There were significant differences detected between the responses of postoperative B versus LSI group, LSI versus NT group and comparison of all postoperative B, LSI and NT groups to the shoulder appearance, perception of shoulder balance, satisfaction of shoulder appearance and severity of shoulder imbalance (P < .001). The responses for postoperative perception of shoulder balance between groups were comparable (P > .05). Otherwise, no significant difference was found between B and NT group for all shoulder questions except perception of shoulder balance (P = .005). (Table 3).
SRS-22r Scores
Postoperative B group scored the highest in overall SRS-22r scores especially in self-image domain (4.0 ± 0.5, P < .001), mental domain (4.2 ± 0.5, P = .002), satisfaction domain (4.4 ± 0.5, P < .001) and total average (4.2 ± 0.3, P < .001) (Table 4).
Mean ± Standard Deviation of SRS-22r Scores for Preoperative/ Postoperative B, LSI and NT Groups.
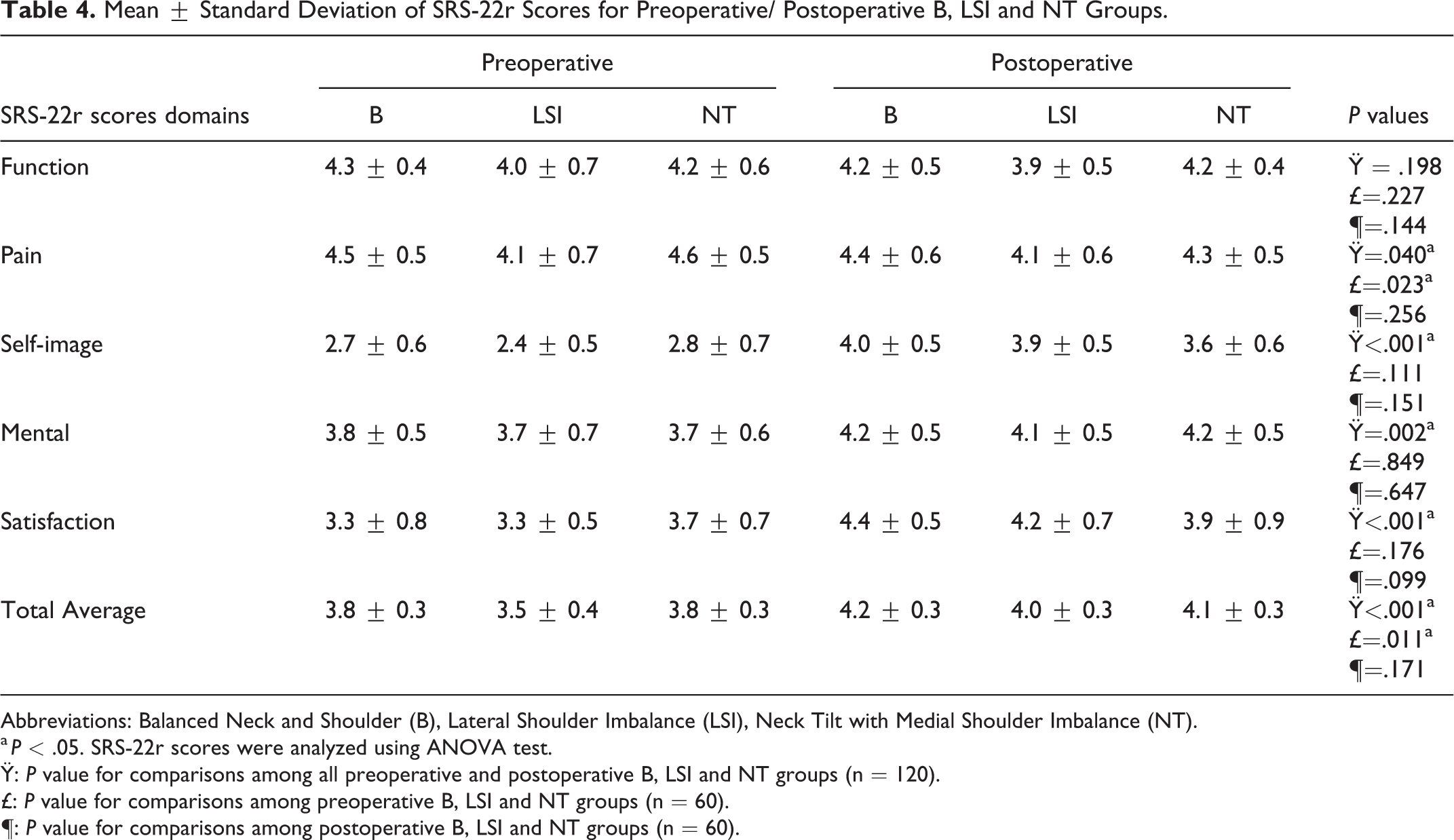
Abbreviations: Balanced Neck and Shoulder (B), Lateral Shoulder Imbalance (LSI), Neck Tilt with Medial Shoulder Imbalance (NT).
a P < .05. SRS-22r scores were analyzed using ANOVA test.
Ÿ: P value for comparisons among all preoperative and postoperative B, LSI and NT groups (n = 120).
£: P value for comparisons among preoperative B, LSI and NT groups (n = 60).
¶: P value for comparisons among postoperative B, LSI and NT groups (n = 60).
Meanwhile, preoperative LSI group scored the lowest in terms of pain (4.1 ± 0.7, P = .040), self-image (2.4 ± 0.5, P < .001), mental (3.7 ± 0.7, P = .002), satisfaction (3.3 ± 0.5, P < .001) and total average (3.5 ± 0.4, P < .001) domains (Table 4).
In general, all postoperative B, LSI and NT groups scored higher in self-image (P < .001), mental (P = .002), satisfaction (P < .001) and total average (P < .001) domains as compared to all preoperative B, LSI and NT groups (Table 4). Comparisons among preoperative B, LSI and NT groups did not exhibit any significance except for pain (P = .023) and total average (P = .011) domains. Otherwise, no significant difference was detected for comparisons among postoperative B, LSI and NT groups (Table 4).
Radiological Outcomes
Preoperative NT group patients had significantly higher preoperative T1 tilt (9.2 ± 5.0°; P < .001) and CA (4.6 ± 3.1°; P = .004). Meanwhile, patients with preoperative LSI had significantly higher Cla-A (4.8 ± 2.8°; P < .001) and RSH (20.1 ± 9.4 mm; P < .001) (Table 5; Figure 6). Postoperative NT patients had higher T1 tilt (9.5 ± 5.3°; P < .001) and CA (7.0 ± 2.0°; P < .001) comparatively whereas postoperative LSI patients had higher Cla-A (4.0 ± 1.3°; P < .001) and RSH (17.0 ± 6.6 mm; P < .001) (Table 6; Figure 7).
Radiological Parameters for Preoperative B, LSI and NT Groups (n = 60).
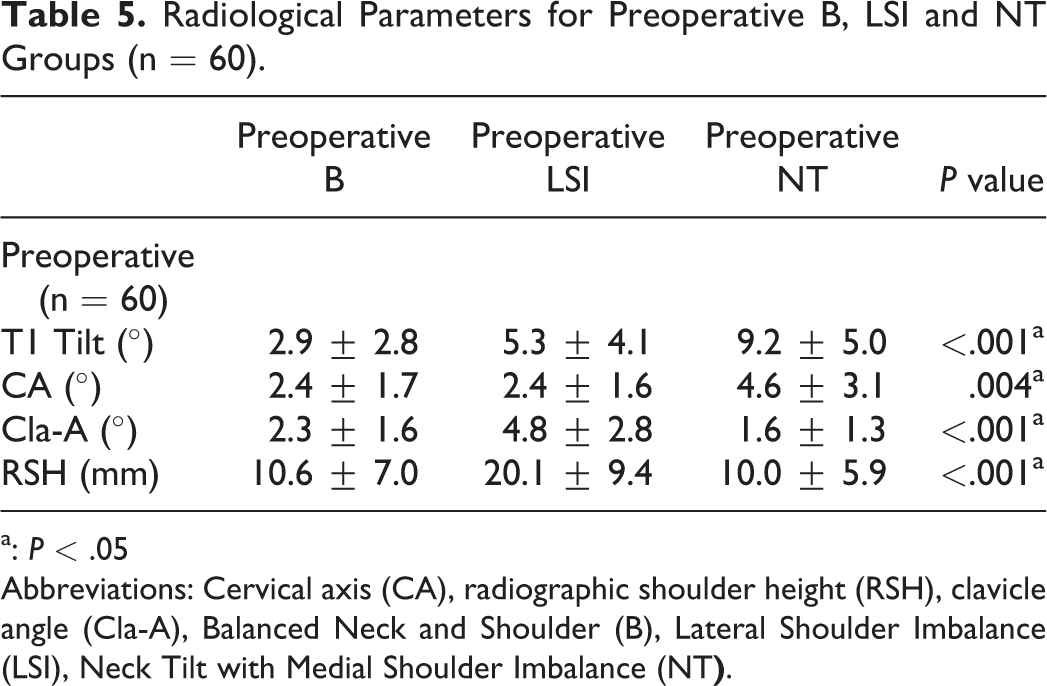
a: P < .05
Abbreviations: Cervical axis (CA), radiographic shoulder height (RSH), clavicle angle (Cla-A), Balanced Neck and Shoulder (B), Lateral Shoulder Imbalance (LSI), Neck Tilt with Medial Shoulder Imbalance (NT
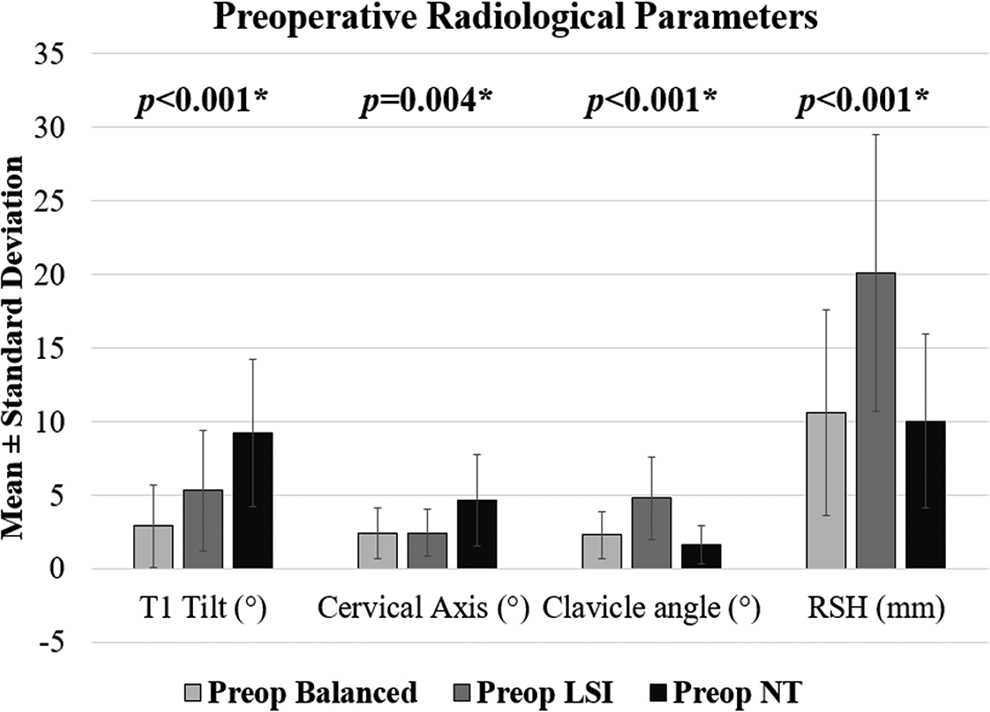
Radiological parameters for preoperative Balanced (B), Lateral Shoulder Imbalance (LSI) and Neck Tilt with Medial Shoulder Imbalance (NT) groups (n = 60).
Radiological Parameters for Postoperative B, LSI and NT Groups (n = 60).
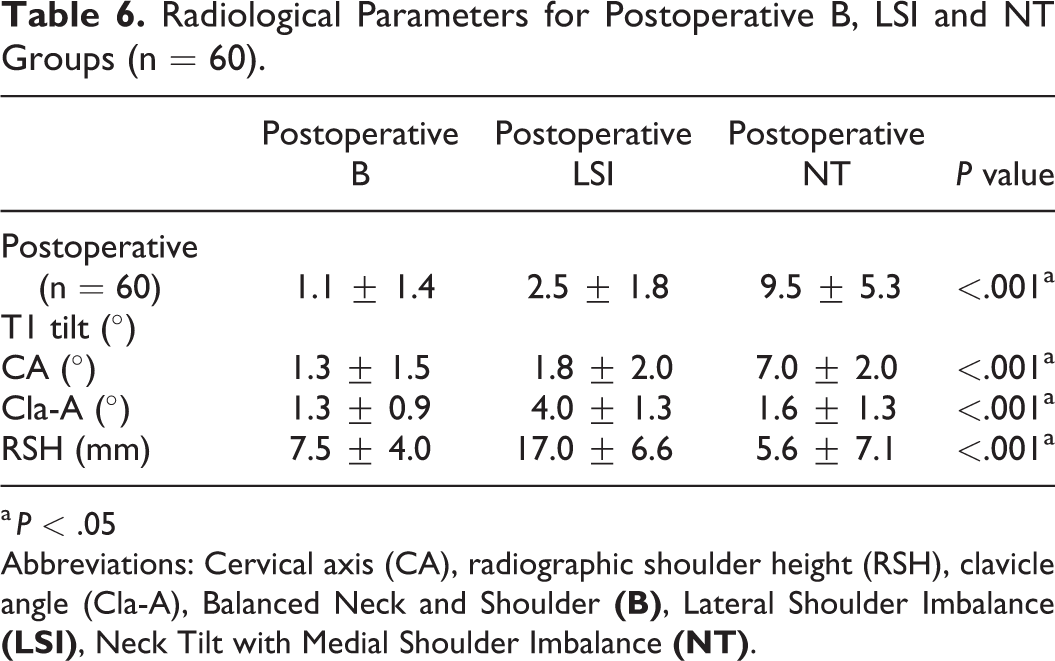
a P < .05
Abbreviations: Cervical axis (CA), radiographic shoulder height (RSH), clavicle angle (Cla-A), Balanced Neck and Shoulder
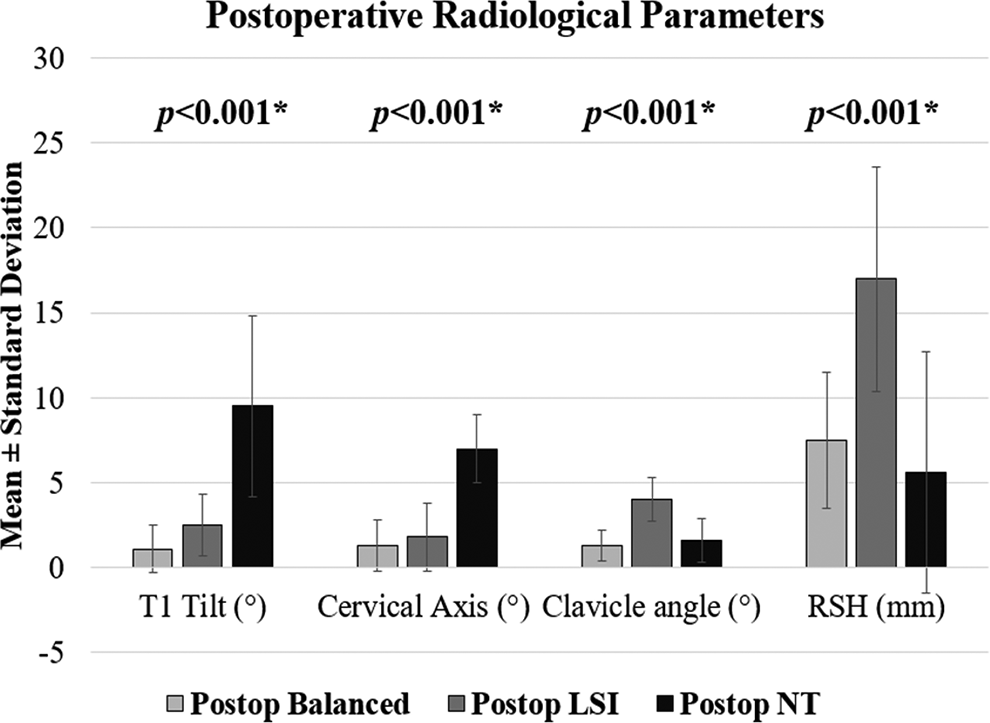
Radiological parameters for postoperative Balanced (B), Lateral Shoulder Imbalance (LSI) and Neck Tilt with Medial Shoulder Imbalance (NT) groups (n = 60).
Discussion
Postoperative shoulder imbalance (PSI) among AIS patients had been widely recognized with the reported incidence of 25%. 1 Kontodimopoulos et al. 24 in 2018 highlighted that the self-image of patients improved with corrective spinal surgeries. Surgically treated AIS patients in the validation sample scored significantly higher in SRS-22 questionnaire self-image domain than untreated AIS patients. However, PSI commonly caused dissatisfaction among AIS patients and their parents.18,22 Misterska et al. 25 illustrated majority of the patients rated rib prominence (29%) and shoulder symmetry (24%) as the trunk deformities that troubled them. Besides, patients were found to have a worse perception of cosmetic outcomes as compared to their parents. 22 Therefore, addressing patients’ concerns of their neck and shoulder imbalance was imperative to meet their postoperative expectations.
Ono et al. 3 described shoulder imbalance as two different entities (Medial Shoulder Imbalance and Lateral Shoulder Imbalance) with LSI showing discrepancy to T1 tilt. To date, studies in neck tilt were limited despite being a common phenomenon among postoperative AIS patients.4,6-8 Therefore, we investigated both LSI as well as Neck Tilt with Medial Shoulder Imbalance (NT) in this study. LSI was defined as >2 cm difference in shoulder height based on the clinical shoulder grading by Kuklo et al. 2 whereas NT was defined as non-correctable neck tilt with trapezial height difference >1 cm based on the clinical neck tilt grading by Kwan et al. 4 Validated instruments such as Modified Neck/ Shoulder Appearance (Kuklo et al., 2002) and SRS-22r questionnaires were used to assess patients’ perception, satisfaction on neck and shoulder balance and their HRQoL objectively.
Neck and shoulder balance parameters of this study population were measured radiographically and clinically by surgeons according to the clinical neck tilt and shoulder grading. This study primarily highlighted the effect of patients’ clinical neck and shoulder appearances on their perception and satisfaction of neck/ shoulder balance regardless of their Lenke types. In 2015, Matamalas et al. 19 conducted a study in 80 preoperative AIS patients to investigate the correlation between clinical/ radiological measurements and patients’ perceived shoulder balance in which balanced was defined as a shoulder height angle of <3.0°. However, no significant correlation was found between clinical/ radiological and perceived shoulder balance. 19 On the contrary, the patients in this study were able to recognize their deformities in concordance to the clinical grading measured by the surgeons. None of the patients in NT group acknowledged their neck as balanced. They were aware that their neck was tilted to either left or right side. Similarly, none of the patients in LSI group acknowledged their shoulders as balanced. They recognized that their left/ right shoulders were slightly raised. All patients in the preoperative and postoperative B group acknowledged their balanced neck/ shoulders.
Most of the AIS patients suffered from the disease-related physical disfigurement. Despite grading the severity of their neck and shoulder imbalance as mild, majority of the patients in this study were still unhappy about it. Studies had found that AIS patients were associated with eating disorders and mood disorders such as anxiety and depression due to their physical appearance disturbance. 26 A case-control study by Akazawa et al. 27 demonstrated that idiopathic scoliosis patients scored lower than healthy subjects in the SRS-22 function and self-image domains.
In correlating the radiological and clinical outcomes of the patients, NT group were found to have a larger T1 tilt angle and CA whereas LSI group had a larger Cla-A and RSH. This was corresponding to the findings by Ono et al. 3 where medial shoulder imbalance was reflected by T1 tilt, first rib angle and upper thoracic curve size whereas lateral shoulder imbalance was correlating to clavicle angle. Kwan et al. 4 also described neck tilt with medial and lateral shoulder imbalance as two distinct entities with T1 tilt and cervical axis demonstrating good clinical correlation to Neck Tilt whereas shoulder imbalance correlated with CHD, RSH, CRID and clavicle angle. Likewise, Jiang et al. 6 also recognized cervical tilt and described its positive correlation to T1 tilt.
Mental health as well as self-image of AIS patients significantly improved after corrective spinal surgeries. 28 AIS patients who had undergone corrective surgeries were found to have better perception of their physical appearances as compared to the preoperative patients.28-31 In this study, we concluded that postoperative B group scored the highest in the self-image, mental, satisfaction and total average domains. Meanwhile, preoperative LSI group scored the lowest in most of the domains in SRS-22r scores. This group of patients had either mild or moderate LSI and majority of them were unhappy about it. In general, postoperative patients scored higher in overall SRS-22r scores in comparison with preoperative patients.
One of the limitations for this study was patients’ postures during clinical measurement may contribute to the measurement error. All patients were standing on a flat surface during measurement and they were advised to position themselves in their most comfortable posture. However, photographs of the patients were not taken in this setting. As Lateral Shoulder Imbalance was defined by shoulder height difference of >2 cm, voluntary shoulder elevation by patients may lead to the inaccuracy of measurement. These patients were clinically graded by three different spine surgeons (MKK, CYWC, CKC) in our academic institution. Nevertheless, all patients recruited had radiographs taken and assessed. Furthermore, patients’ perception and satisfaction of neck/ shoulder balance could also be influenced by their preoperative physical characteristics, psychological characteristics and expectations as well. 32
This study only emphasized on patients’ perception and satisfaction of neck/ shoulder balance in relation to their clinical neck and shoulder balance, regardless of the Lenke types. Besides, preoperative and postoperative groups recruited were of different patients. In view of some preoperative patients in our study were not planned for operation at the time of recruitment, we could not recruit them postoperatively. In addition, the focus of the study was to compare the responses for each group of preoperative as well as postoperative patients with balanced or imbalanced neck/ shoulder. Patients who had preoperative lateral shoulder imbalance might achieve a balanced shoulder postoperatively or vice versa. The SRS-22r scores in this study were also incomparable for Minimum Clinically Important Difference (MCID) as the comparison for improvement of SRS-22r scores postoperatively was not applicable in this study.33,34 Future studies could involve a larger sample size with the same group of patients for comparison of MCID in their SRS-22r scores as well. Lastly, different fusion levels between postoperative groups could also affect patients’ postoperative pain and function. In our institution, we acknowledged that having an optimal UIV tilt angle is required to prevent neck tilt with medial shoulder imbalance besides the selection of fusion level based on the current recommendations. 11 However, this was not analyzed as half of the patients recruited were preoperative patients.
Conclusion
Lateral Shoulder Imbalance (LSI) groups were aware and unhappy with their lateral shoulder imbalance and they had a significant larger Cla-A and RSH. Similarly, Neck Tilt with Medial Shoulder Imbalance (NT) groups were aware and unhappy with their neck and medial shoulder imbalance and they had a significant larger T1 tilt and CA. Postoperative Balanced (B) group scored higher in self-image, mental, satisfaction and total average domains for SRS-22r scores whereas preoperative LSI scored the lowest in these domains.
Footnotes
Acknowledgements
We would like to acknowledge Winnie Loke Lai Sing and Chua Sock Koon for their contribution in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.