
Abstract
Study Design:
Retrospective analysis.
Objectives:
Cervical disc arthroplasty (CDA) was designed to replace the degenerated disc with the prosthesis to preserve cervical motion. The commonly used artificial discs are designed symmetric, whereas the facet joints were reported to be asymmetric in many people. This study aimed to evaluate the effect of facet tropism on the cervical range of motion (ROM) after single-level CDA using Prestige LP.
Methods:
A total of 90 patients who underwent single-level CDA using Prestige LP from 2012 to 2017 were retrospectively reviewed. Radiographs were taken at each time point to measure the C2-C7 ROM and the ROM at the surgical segment. The pre-operation CT scans were utilized to reconstruct and calculate the angular direction of facet joints with respect to transverse, coronal, and sagittal reference planes. Facet tropism above 7° was defined as facet joint asymmetry.
Results:
No significant difference was found in flexion-extension C2-C7 ROM or ROM at the surgical segment between patients with symmetric and asymmetric fact joints regarding the sagittal plane. Patients with coronal asymmetric facet joints had lower flexion-extension ROM at the surgical level. Patients with transverse asymmetric facet joints had both lower flexion-extension C2-C7 ROM and ROM at the surgical level. After CDA surgery, patients obtained good clinical outcomes including increased Japanese Orthopedic Association (JOA) and decreased Neck Disability Index (NDI) as well as Visual Analogue Scale (VAS).
Conclusion:
The coronal and transverse tropism seemed to be correlated with decreased flexion-extension ROM after CDA using Prestige LP.
Introduction
Cervical disc arthroplasty (CDA) has been widely used in the treatment of cervical spondylosis. As compared to anterior cervical discectomy and fusion (ACDF), CDA can preserve the segmental range of motion (ROM) and seem to decrease the incidence of adjacent level degeneration.1-3 ROM is one of the important indicators to evaluate the postoperative effect of CDA. However, some patients have poor postoperative segmental ROM during the follow-up period. The related factors of the segmental ROM reported in the literature include the type of prosthesis, 4 the height of the intervertebral space and prosthesis,5-7 the center of rotation (COR), 8 the sagittal alignment of the cervical spine, 9 the level of surgical segment 10 and the preoperative segmental ROM.11,12
The facet joints, also known as the zygapophyseal joint, are located at the posterolateral side of the vertebral body.13,14 The left and right facet joints and the anterior intervertebral disc form an integrated functional unit, the 3-joint complex, which plays an important role in the movement function and stable maintenance of the functional spinal units. 15 CDA can replace the original degenerated intervertebral disc by implanting the artificial joint prosthesis. The prosthesis and bilateral facet joints were reassembled into a new 3-joint complex after surgery. Previous studies have repeatedly focused on the details of surgical operations, intervertebral space conditions, or other factors that could affect the function of the prosthesis. But few researchers have paid attention to the other component, the bilateral facet joints. Structural abnormalities in any part of the 3-joint complex could affect the other 2 parts, affecting the function of the entire 3-joint complex.15,16
Facet tropism was defined as the absolute difference of angle value between the left facet joint and the right facet joint with respect to a specific reference plane.17,18 If the facet tropism exceeds a certain value, this pair of bilateral facet joints could be considered asymmetric. Previous research has established that the facet asymmetry in the cervical spine was a common phenomenon, and the incidence of facet tropism above 7° in the population is between 17.5% and 39%. 19 Some scholars believed that the cervical facet joint asymmetry was related to the occurrence of cervical degenerative diseases, such as cervical degenerative spondylolisthesis 20 and cervical disc herniation. 21 Biomechanical studies have also suggested that the cervical facet joint asymmetry could increase the facet contact force and the intradiscal pressure. 22
After CDA, the facet joints still play an important role in maintaining and guiding the cervical segmental movements, despite the motion mode and mechanical environment of the new 3-joint complex changed obviously.23-25 Certain types of prosthesis seemed able to increase facet contact force after CDA.26,27 It is unclear whether asymmetric facet joints will affect the motion function of the new 3-joint complex. Besides, prostheses used in the CDA were mostly designed as symmetric artificial joints and designed to provide symmetric flexion, extension, and axial rotation. This designing scheme did not take account of the asymmetric facet joints, which commonly exist in the population. 28 The mismatch of the symmetric prosthesis and the asymmetric facet joints may lead to a poor motion function of the new 3-joint complex. 29 Therefore, there is a great research value to explore the correlation between the facet joint tropism and the ROM after CDA.
Methods
Study Design
We retrospectively included patients who underwent single-level CDA using Prestige LP prosthesis in our hospital from 2012 to 2017. Prestige LP is one of the commonly used artificial discs prosthesis. This ball-and-trough articulation is designed to allow for a variable COR and simulate the physiological motion of the intervertebral disc. The inclusion criteria were as follows: (1) Patients were diagnosed with cervical spondylotic myelopathy or radiculopathy refractory to conservative treatment. (2) Patients’ cervical spine had good mobility and no instability, the flexion-extension motion of the surgical segment being in the range of 3∼11°. (3) Patients had complete imaging data at 6 follow-up time points: pre-operation, discharge, 3, 6, 12, and 24 months post-operation. And the quality of imaging data met the measuring requirement. The following patients were excluded: (1) Patients with a history of cervical spine surgery or trauma. (2) Patients were diagnosed with cervical spine deformity, osteoporosis, tumor, infection, rheumatic disease, or other diseases. (3) Patients with ossification of the posterior longitudinal ligament, osseous spinal stenosis, severe facet degeneration, severe intervertebral foramen stenosis, or other relative contraindications of CDA. (4) Multi-level CDA or cervical fusion and non-fusion hybrid surgery. (5) CDA using prostheses other than Prestige LP. According to the inclusion and exclusion criteria, 454 patients who underwent CDA in our institution were screened. Among them, 90 patients who underwent single-level CDA using Prestige LP prosthesis with complete follow-up data was included in this study. All patients had given informed consent to allow their information to be used for research purposes. And the study protocol was approved by the Ethics Committee of West China Hospital of Sichuan University (Project License Number 20 190 946). All patients were operated on by the same surgeon with many years of surgical experience, and we did not include the surgeon’s early cases (from 2008 to 2011), to minimize the influence of the doctor’s personal technique and experience.
Radiological Measurement
The C2-C7 Cobb angle and the shell angle of the surgical segment at flexion and extension view were measured. The lateral bending angle (left and right) on the lateral bending view was measured (Figure 1). The 3 ROMs to describe the cervical spine motor function were calculated as follows:
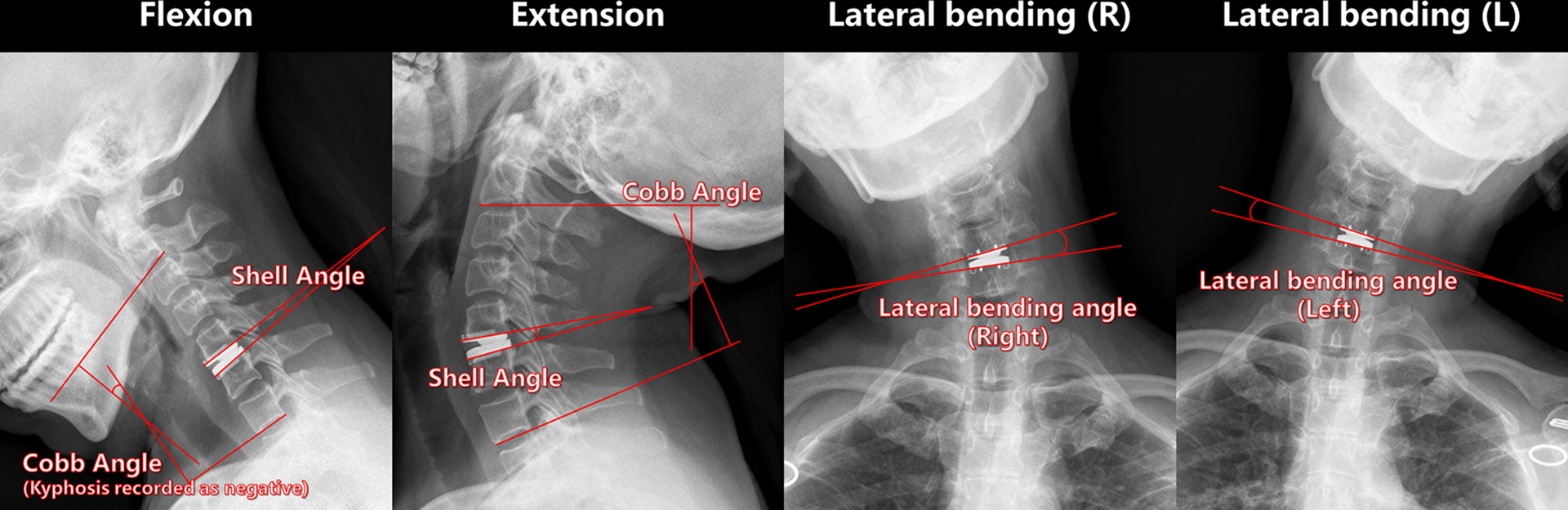
Radiological measurements.
Flexion-Extension ROM of C2-C7 = Cobb Angle (Extension) − Cobb Angle (Flexion)
Flexion-Extension ROM of Surgical Segment = Shell Angle (Extension) − Shell Angle (Flexion)
Lateral Bending ROM of Surgical Segment = Lateral Bending Angle (Left) + Lateral Bending Angle (Right)
The Japanese Orthopedic Association (JOA), Neck Disability Index (NDI), and Visual Analogue Scale (VAS) scores at pre-operation and the last follow-up were used to evaluate the clinical outcomes.
We used the 3-dimensional reconstruction model of computed tomography (CT) and space vector calculation to measure the spatial orientation of cervical facet joints. Three types of facet tropism were determined as we previously reported.19,28 The CT data in DICOM format was imported into the software Mimics (Version 17.0, Materialize, Belgium) to reconstruct the cervical spine. Bilateral facet planes and 3 reference planes (transverse, sagittal, and coronal) at the surgical level were reconstructed, and coordinates of the normal vector of each plane were recorded. The inclined angles between each facet joint plane and the transverse, sagittal, or coronal reference plane (Figure 2) were calculated by vector operations. The cosine formula was used to calculate the dihedral angle between 2 planes:

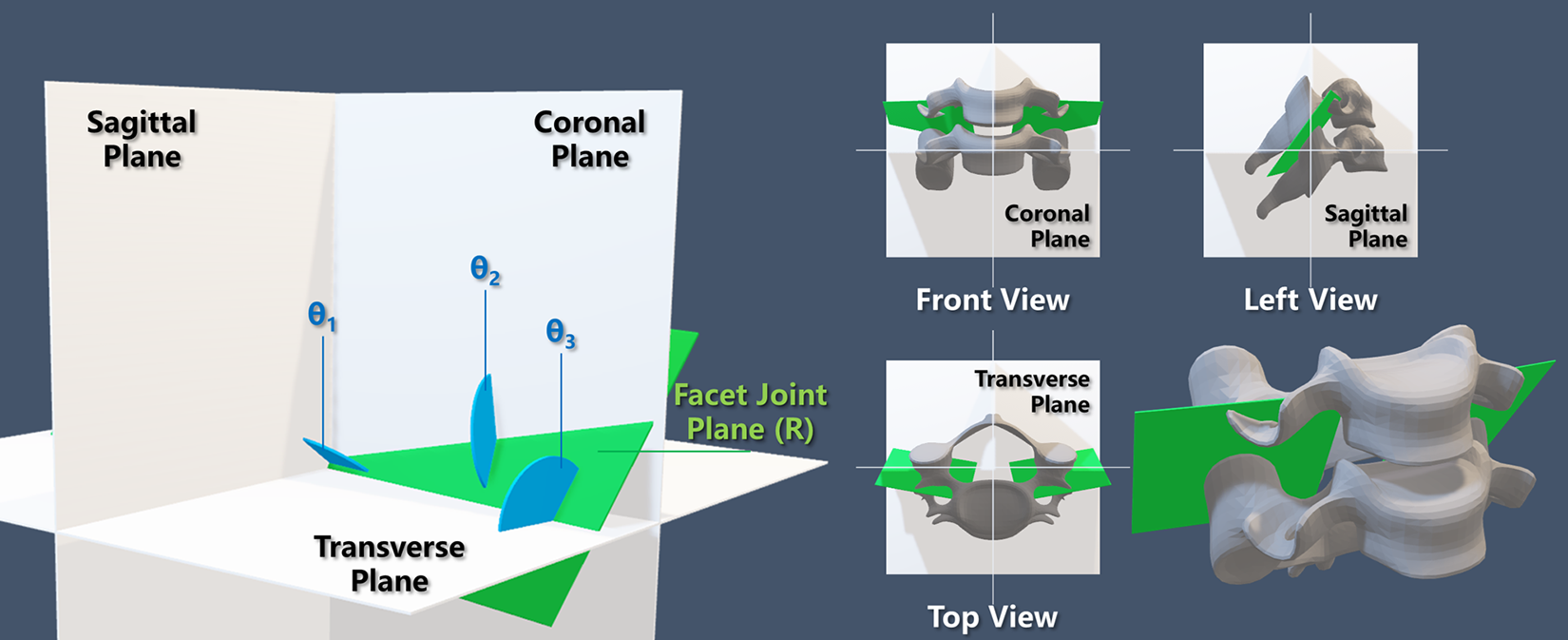
The dihedral angles between the facet joint and the 3 reference planes. The dihedral angle θ1 is the angle between the facet joint plane and the sagittal plane; the dihedral angle θ2 is the angle between the facet joint plane and the coronal plane; the dihedral angle θ3 is the angle between the facet joint plane and the transverse plane.
A more than 7° difference in bilateral angles with respect to the same reference plane was defined as facet joint asymmetry.19,28 According to this criterion, patients were assigned to the sagittal symmetric group and sagittal asymmetric group, coronal symmetric group and coronal asymmetric group, transverse symmetric group and transverse asymmetric group. The differences in ROM between the symmetric group and the asymmetric group were compared.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows (Version 23.0, IBM Corp., Armonk, New York, USA). Quantitative data was presented as Mean ± Standard Deviation (SD). The independent t-test was used to compare the difference of ROMs (including the flexion-extension ROM of C2-C7, the flexion-extension ROM of surgical segment, the lateral bending ROM of surgical segment) between the symmetric group and the asymmetric group at all time points. Similarly, the independent t-test was also used to compare the clinical symptom scores (including JOA, NDI, VAS-neck, and VAS-arm) between the symmetric and asymmetric groups. The paired t-test was used to compare whether the ROMs at each postoperative follow-up time (discharge, 3 m, 6 m, 12 m, and 24 m) were different from those at pre-operation in each group. And the paired t-test was also used to compare the clinical symptom scores before and after surgery in each group. A value of P less than 0.05 was considered to be statistically significant.
Results
Patient Demographic Data
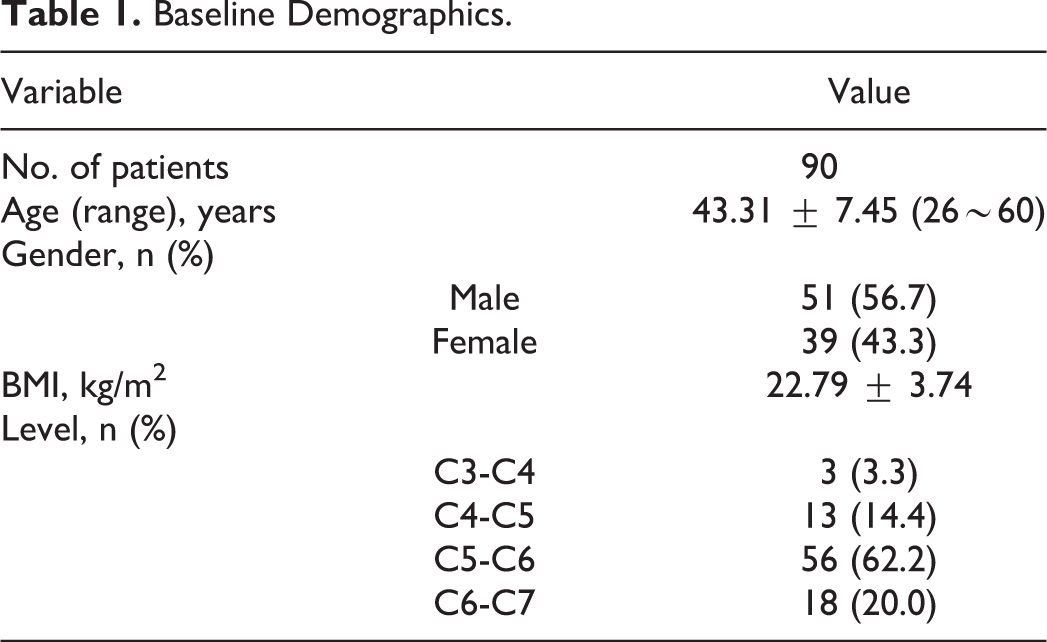
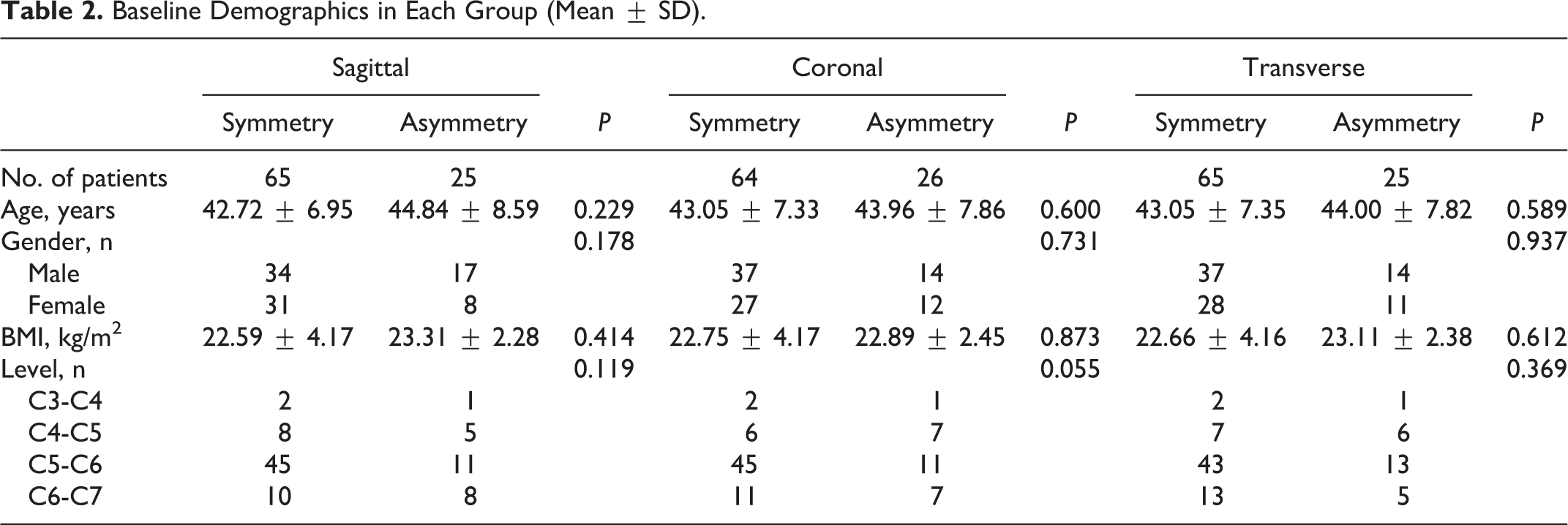
A total of 90 patients were retrospectively enrolled in this study. The mean age was 43.3 years old (ranging from 26 to 60 years old). The CDA surgery included 4 levels, C3-C4, C4-C5, C5-C6, and C6-C7, with the largest number of cases in the C5-C6 level. The patients were grouped according to the facet tropism at the surgical level. In 90 patients, 65 had sagittal symmetry and 25 had sagittal asymmetry; 64 had coronal symmetry and 26 had coronal asymmetry; 65 had transverse symmetry and 25 had transverse asymmetry. Baseline demographics of patients are shown in Table 1 and Table 2. The statistical tests did not show any significant difference in the basic data of age (independent t-test), gender (Pearson chi-square test), BMI (independent t-test), or level (Fisher’s exact test) between each symmetric group and asymmetric group.
Baseline Demographics.
Baseline Demographics in Each Group (Mean ± SD).
Flexion-Extension C2-C7 ROM
The flexion-extension ROM of C2-C7 is shown in Table 3 and Figure 3.
The Flexion-Extension ROM of C2-C7 (Mean ± SD°).
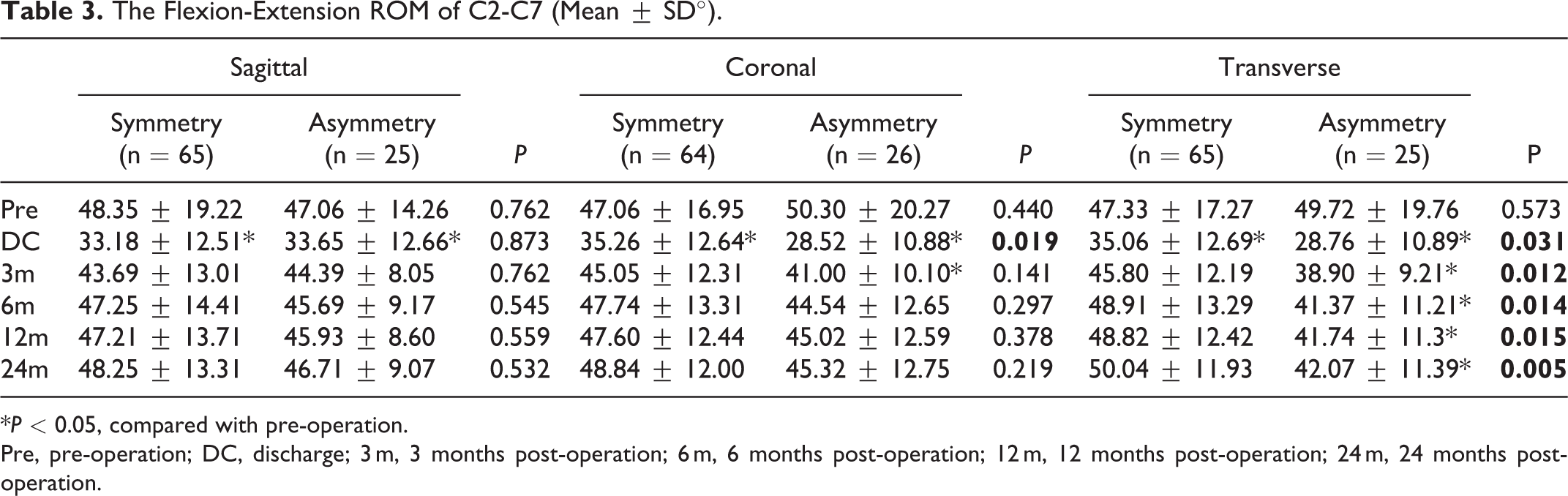
*P < 0.05, compared with pre-operation.
Pre, pre-operation; DC, discharge; 3 m, 3 months post-operation; 6 m, 6 months post-operation; 12 m, 12 months post-operation; 24 m, 24 months post-operation.
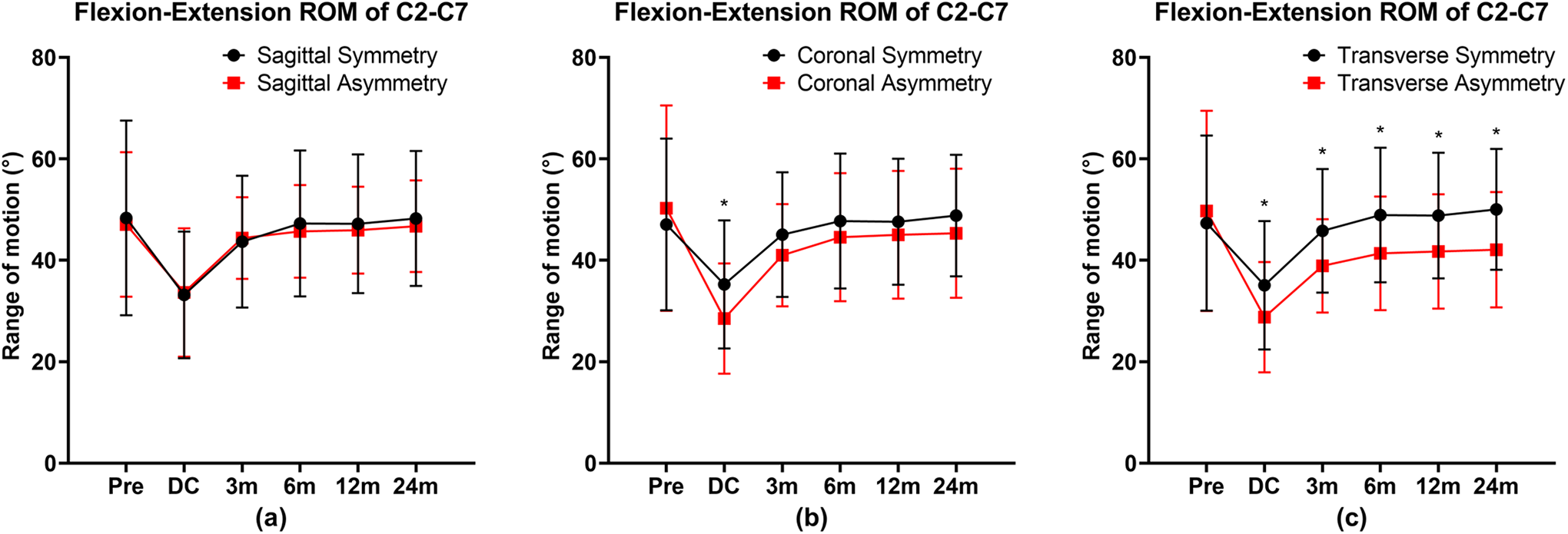
The flexion-extension ROM of C2-C7 at each timepoint. Facet joint symmetry and asymmetry with respect to the sagittal plane (a). Facet joint symmetry and asymmetry with respect to the coronal plane (b). Facet joint symmetry and asymmetry with respect to the transverse plane (c). *P < 0.05, indicates significant difference between the symmetric group and the asymmetric group. Error bars indicate standard deviation (SD).
The independent t-test showed that there was no significant difference in C2-C7 ROM between the sagittal symmetric group and the sagittal asymmetric group at all follow-up times. The postoperative discharge C2-C7 ROM of the coronal asymmetry group was significantly lower than that of the coronal symmetry group (P = 0.019), but there was no significant difference between the 2 groups at other follow-ups. There was no significant difference in C2-C7 ROM between the transverse symmetry group and the transverse asymmetry group at pre-operation, while the C2-C7 ROM of the transverse asymmetry group at all 5 postoperative follow-up times was significantly lower than that of the transverse symmetry group (discharge, P = 0.031; 3 months post-operation, P = 0.012; 6 months post-operation, P = 0.014; 12 months post-operation, P = 0.015; 24 months post-operation, P = 0.005).
The paired t-test results are as follows. In the sagittal symmetry group, only the postoperative discharge C2-C7 ROM was significantly lower than the preoperative ROM in the 5 follow-up times (P < 0.001). Similarly, in the sagittal asymmetry group, only the discharge C2-C7 ROM was significantly lower than the preoperative ROM in the 5 follow-up times (P = 0.002). In the coronal symmetry group, the discharge C2-C7 ROM was significantly lower than pre-operation (P < 0.001). In the coronal asymmetry group, the C2-C7 ROM at discharge and 3 months post-operation was significantly lower than pre-operation (discharge, P < 0.001; 3 months post-operation, P = 0.016). In the transverse symmetry group, only the discharge C2-C7 ROM was significantly lower than pre-operation (P < 0.001). But in transverse asymmetry group, the C2-C7 ROM at all 5 postoperative follow-up times was significantly lower than pre-operation (discharge, P < 0.001; 3 months post-operation, P = 0.004; 6 months post-operation, P = 0.013; 12 months post-operation, P = 0.023; 24 months post-operation, P = 0.029).
Flexion-Extension ROM at the Surgical Segment
The flexion-extension ROM at the surgical segment is shown in Table 4 and Figure 4.
The Flexion-Extension ROM of Surgical Segment (Mean ± SD°).
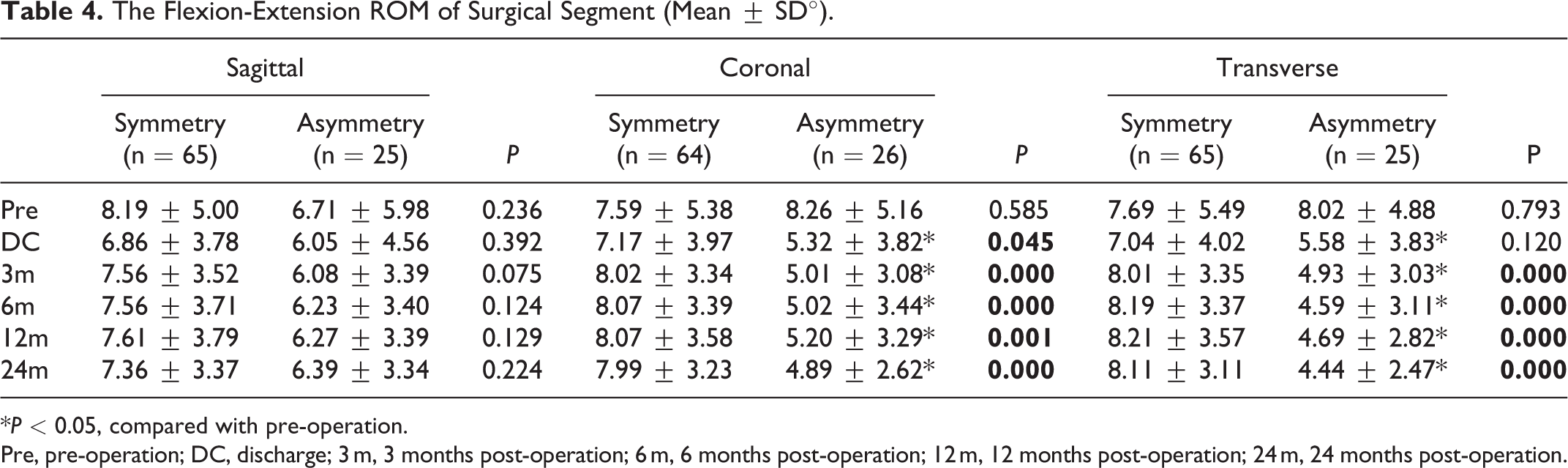
*P < 0.05, compared with pre-operation.
Pre, pre-operation; DC, discharge; 3 m, 3 months post-operation; 6 m, 6 months post-operation; 12 m, 12 months post-operation; 24 m, 24 months post-operation.
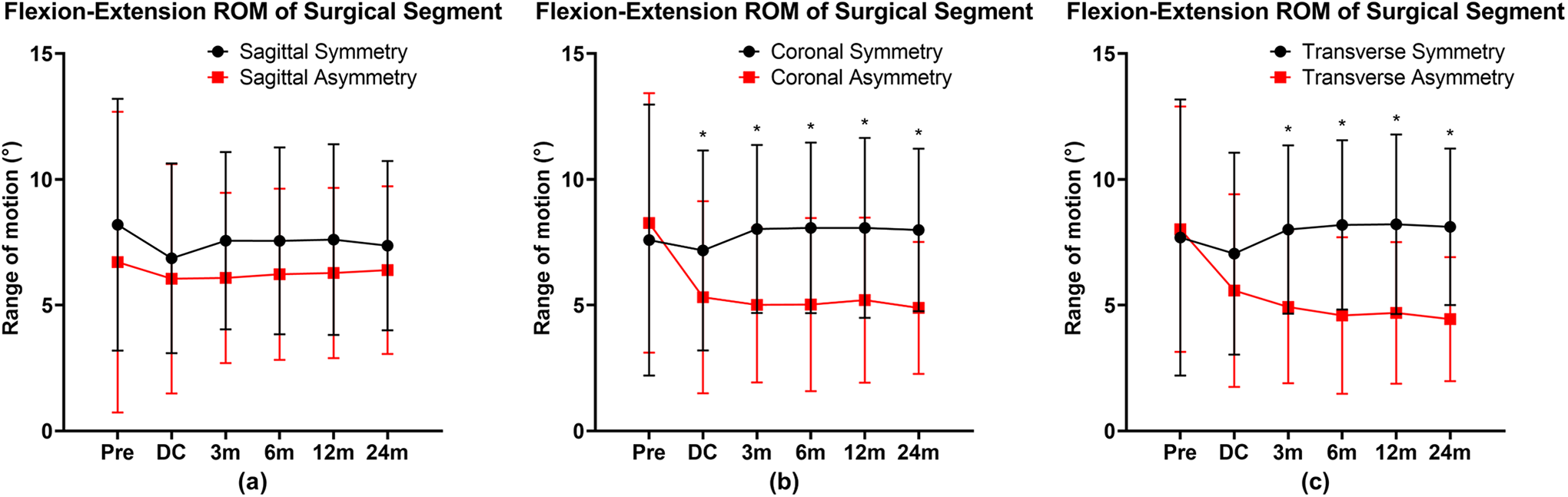
The flexion-extension ROM of surgical segment at each timepoint. Facet joint symmetry and asymmetry with respect to the sagittal plane (a). Facet joint symmetry and asymmetry with respect to the coronal plane (b). Facet joint symmetry and asymmetry with respect to the transverse plane (c). *P < 0.05, indicates significant difference between the symmetric group and the asymmetric group. Error bars indicate standard deviation (SD).
The independent t-test showed that there was no significant difference between the sagittal symmetry group and the sagittal asymmetry group at all follow-up times. Compared with the coronal asymmetry group, the coronal symmetry group had no significant difference only at pre-operation. The surgical segmental ROM of the coronal asymmetry group at all 5 postoperative follow-up times was significantly lower than that of the coronal symmetry group (discharge, P = 0.045; 3 months post-operation, P < 0.001; 6 months post-operation, P < 0.001; 12 months post-operation, P = 0.001; 24 months post-operation, P < 0.001). Compared with the transverse symmetry group, the transverse asymmetry group had no significant difference at pre-operation and discharge, and the surgical segmental ROM in other 4 follow-up times was significantly lower than that of the transverse symmetry group (3 months post-operation, P < 0.001; 6 months post-operation, P < 0.001; 12 months post-operation, P < 0.001; 24 months post-operation, P < 0.001).
The paired t-test showed that there was no significant difference in surgical segmental ROM at each follow-up time in the sagittal symmetry group, the sagittal asymmetry group, the coronal symmetry group, and the transverse symmetry group. However, the surgical segmental ROM in the coronal asymmetry group was lower than pre-operative at all 5 postoperative follow-up times (discharge, P = 0.001; 3 months post-operation, P = 0.005; 6 months post-operation, P = 0.015; 12 months post-operation, P = 0.015; 24 months post-operation, P = 0.005). The surgical segmental ROM in the transverse asymmetry group were also lower than pre-operative at all 5 postoperative follow-up times (discharge, P = 0.002; 3 months post-operation, P = 0.008; 6 months post-operation, P = 0.009; 12 months post-operation, P = 0.007; 24 months post-operation, P = 0.002).
Lateral Bending ROM at the Surgical Segment
The relationship between the facet tropism and the lateral bending ROM of surgical segment is shown in Table 5 and Figure 5. The independent t-test did not show any significant difference between each related symmetry group and asymmetry group. The presence of sagittal asymmetry, coronal asymmetry, or transverse asymmetry did not affect the lateral bending ROM of surgical segment after CDA surgery.
The Lateral Bending ROM of Surgical Segment (Mean ± SD°).
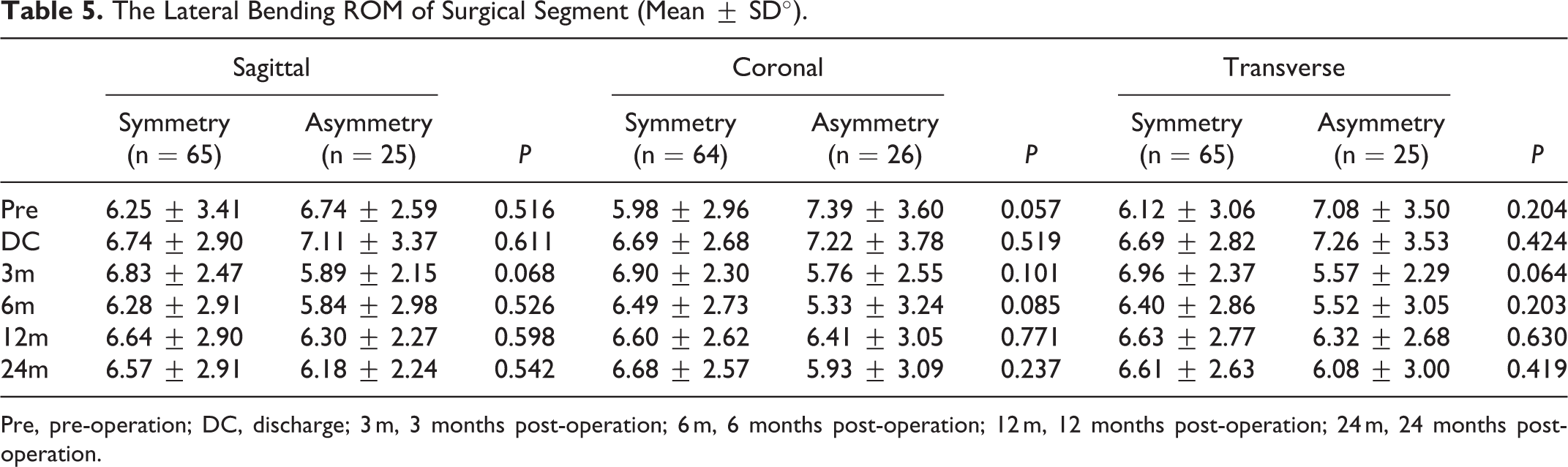
Pre, pre-operation; DC, discharge; 3 m, 3 months post-operation; 6 m, 6 months post-operation; 12 m, 12 months post-operation; 24 m, 24 months post-operation.
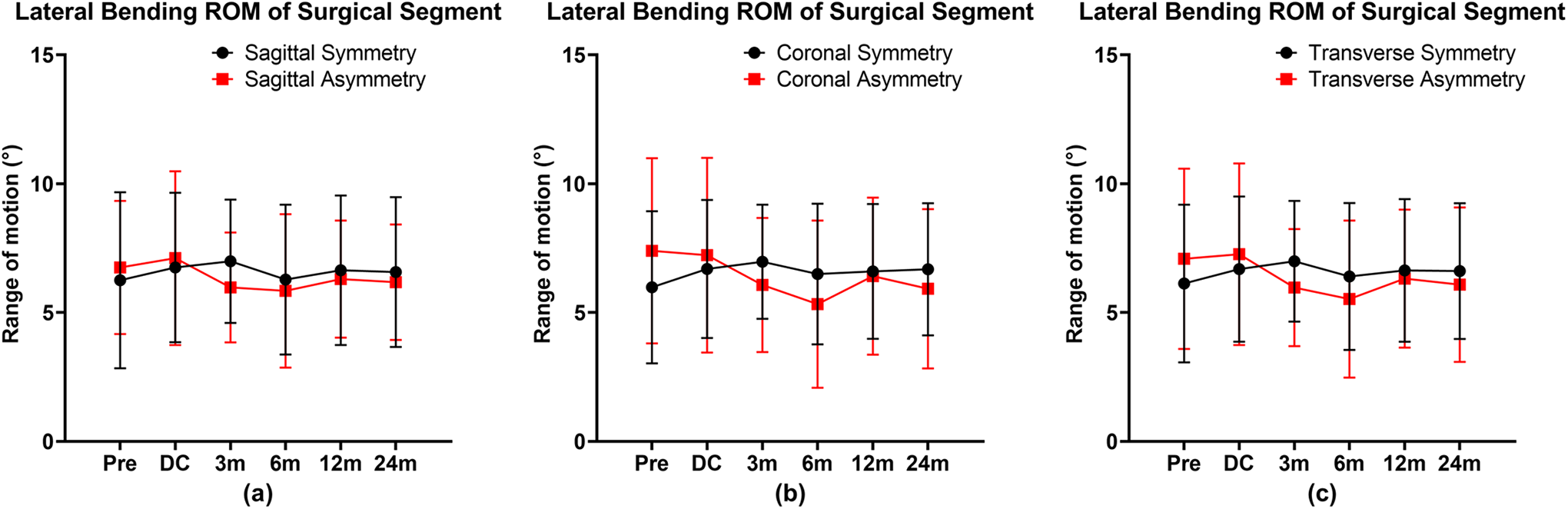
The lateral bending ROM of surgical segment at each timepoint. Facet joint symmetry and asymmetry with respect to the sagittal plane (a). Facet joint symmetry and asymmetry with respect to the coronal plane (b). Facet joint symmetry and asymmetry with respect to the transverse plane (c). Error bars indicate standard deviation (SD).
Clinical Outcomes
The relationship between the facet tropism and the lateral bending ROM of surgical segment is shown in Table 6 and Figure 6. The independent t-test did not show any difference between the symmetry group and the asymmetry group in 4 scores. The paired t-test showed that the JOA, NDI, VAS-arm, and VAS-neck scores at the final follow-up were significantly better than those at the pre-operation (P < 0.001). It indicates that the clinical symptoms of patients in all groups have improved significantly.
The JOA, NDI, VAS-Neck, and VAS-Arm Scores (Mean ± SD).
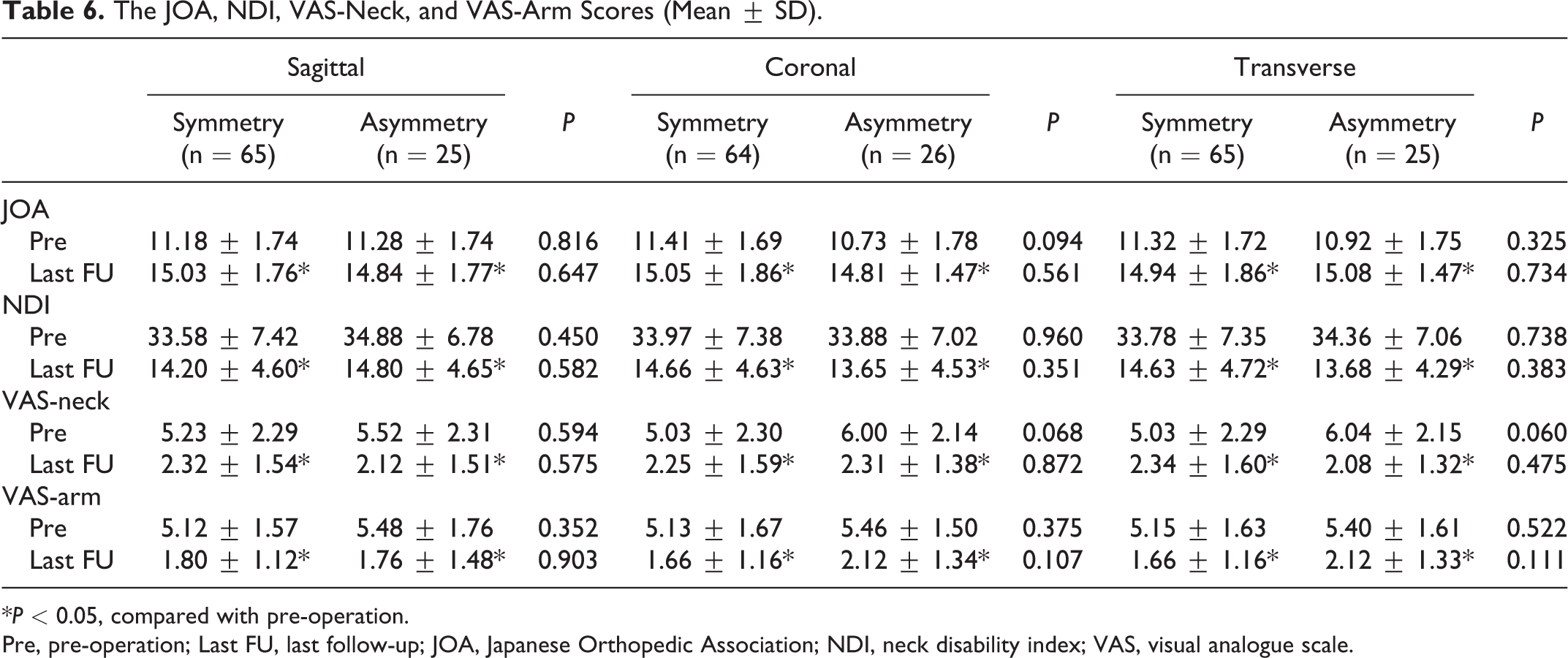
*P < 0.05, compared with pre-operation.
Pre, pre-operation; Last FU, last follow-up; JOA, Japanese Orthopedic Association; NDI, neck disability index; VAS, visual analogue scale.
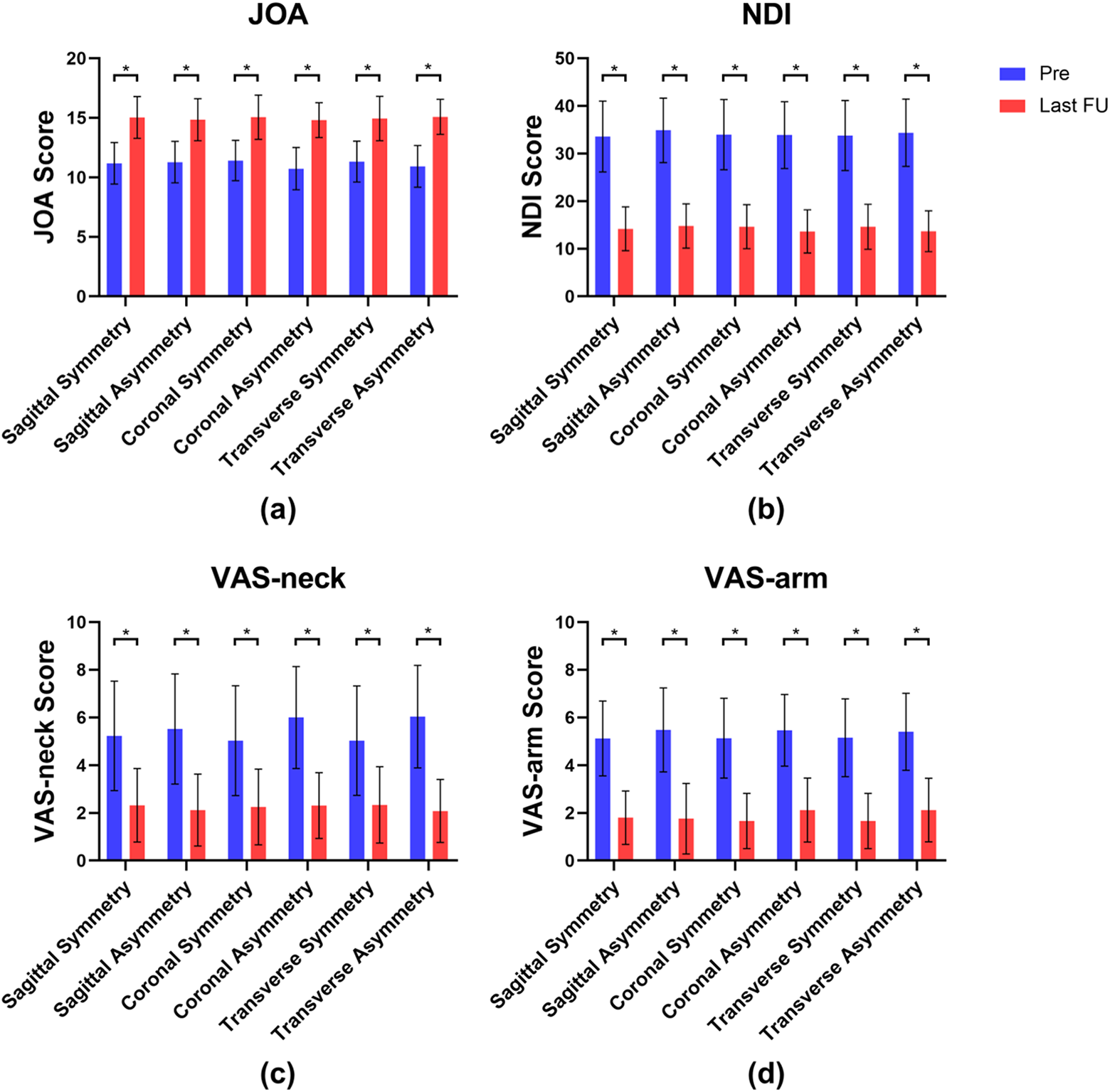
The JOA (a), NDI (b), VAS-neck (c), and VAS-arm scores (d). *P.
Discussion
Our results showed that the flexion-extension ROM at the surgical segment and the flexion-extension C2-C7 ROM both indicated a trend of decreasing initially after surgery and then increasing gradually, then becoming stabilized or slightly decreased during the mid-term follow-up in most cases. However, patients with coronal asymmetric facet joints or transverse asymmetric facet joints at the surgical level showed poor recovery in the flexion-extension ROM at the surgical segment. Also, patients with transverse asymmetric facet joints had a lower C2-C7 ROM than the transverse symmetry group at each postoperative follow-up time. The lateral bending ROM at the surgical segment had little difference at each follow-up time. No significant difference was found between symmetric groups and asymmetric groups with regard to lateral bending ROM. The majority of patients obtained significantly improved clinical outcomes after CDA and no significant difference in scores was found between each symmetry and asymmetry group. We believe the improvement of symptoms was mainly due to the thorough decompression and the delicate operative skills with less damage to the surrounding tissues during the surgery.
The results suggested that the existence of facet joint asymmetry did not reflect a significant difference in preoperative ROM. However, the effect of facet joint asymmetry on ROM was prominent after CDA. This might be related to the different motion characteristics of the original 3-joint complex and the prosthetic 3-joint complex. The native intervertebral disc might be more adaptable to the asymmetric facet joints than the prosthesis. The prosthesis Prestige LP (Medtronic Sofamor Danek, Memphis, Tennessee, USA) 30 used in this study, made of titanium alloy/titanium carbide composite (Ti-6Al-4V/TiC), is a semi-constrained ball-and-trough arthroplasty device. 31 This ball-and-trough designed articulation has 4 kinematic degrees of freedom (DOF). It allows for independent rotations about 3 orthogonal axes (flexion-extension, lateral bending, and axial rotation) and translation in the sagittal plane32-34 (Figure 7). Prestige LP has a movable instantaneous COR to simulate the physiological motor function,35,36 and can theoretically reduce the problem of facet impingement and abnormal facet stress in prosthesis with a fixed COR prostheses. 37 Other prostheses are varied in the articulation design, such as the saddle joint, the ball-and-socket joint, the biconvex core articulation, and the non-articulating discs with compliant cores.32,34 Our results may not represent any other type of prostheses. Nevertheless, in consideration of the findings of other researchers, it is still difficult to replicate the physiological COR with disc replacement.37-42 Hence, it could be hypothesized that the mechanical characteristics of physiological intervertebral discs would counteract the negative effects of asymmetric facet joints to a certain extent, while the prostheses with a simple structure cannot fully simulate the complex biomechanical properties of the intervertebral discs.
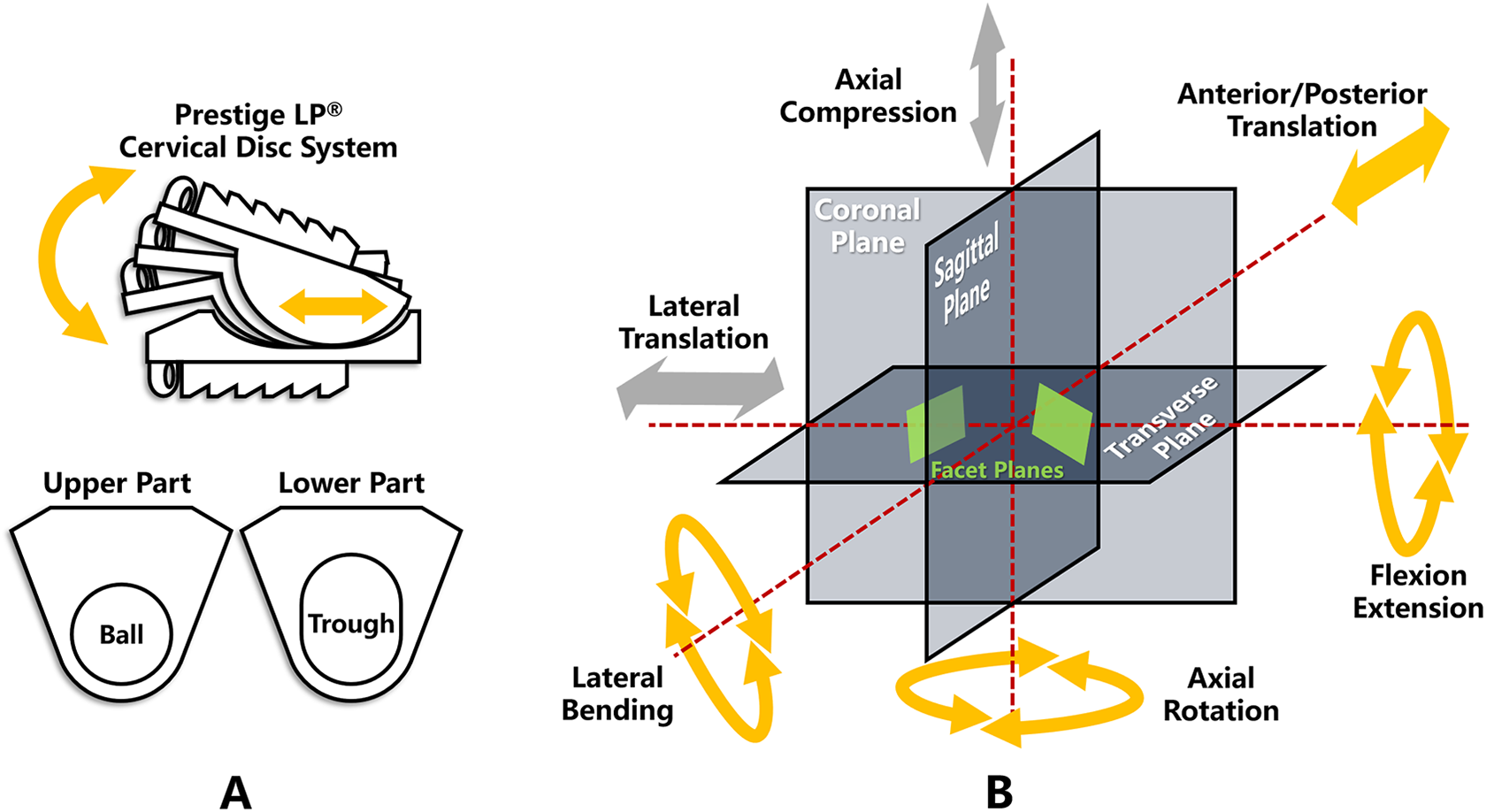
The kinematic DOF of Prestige LP artificial cervical disc. (A) The ball-and-trough articulation structure in Prestige LP allows for the combined motion of anterior/posterior translation and flexion/extension, and provide a variable COR in the sagittal plane. (B) This figure illustrates the positional relationship of the DOF, the 3 reference planes, and the bilateral facet joint planes. The native intervertebral disc has 6 DOF (rotation independently about 3 axes and translation independently along 3 axes). The Prestige LP artificial disc has 4 DOF (without lateral translation and axial compression).
In other studies, the angles of the cervical facet joints were often measured only through 2-dimensional axial tomographic images on CT or Magnetic Resonance Imaging (MRI).20,21,43 However, it is difficult to accurately describe the 3-dimensional orientation of the facet joint planes by drawing lines on the 2-dimensional images, especially considering the oblique position of the cervical facet joints. The 3-dimensional measurement method we used can divide tropism into 3 types: tropism with respect to the sagittal plane (sagittal tropism), tropism with respect to the coronal plane (coronal tropism), and tropism with respect to the transverse plane (transverse tropism). These 3 types of tropism of the bilateral facet joints are mutually independent, and 1 or more asymmetries randomly exist in the patient. The critical value of facet asymmetries was determined by the standard deviation of the normal distribution of the facet tropism angular values in the population. 19 So, the proportions of 3 kinds of asymmetries in the population are roughly the same and the sample sizes were similar in all 3 asymmetric groups. It can be seen from Figure 2 and Figure 7 that the additional resistance from different directions due to the facet joint asymmetry may have different effects on the flexion-extension movement of the Prestige LP prosthesis. Our results also show that different types of asymmetry have different effects on ROM after CDA and the sagittal asymmetry has the least effect on the asymmetric prosthetic 3-joint complex. One possible explanation is the sagittal asymmetry causes an additional lateral force, which is perpendicular to the direction of the flexion-extension vertebrae movements, rather than a direct resistance caused by coronal or transverse asymmetry.
On the other hand, researchers believe that there is a correlation between facet joint asymmetry and facet joint degeneration.19,44 Preoperative cervical degeneration, including osteophyte formation and facet joint degeneration, are considered as relative contraindications for disc replacement, because it may be related to poor postoperative ROM and heterotopic ossification (HO).45,46 Although we excluded patients with severe facet joint degeneration not suitable for CDA, facet asymmetry may still be associated with some potential degeneration, which could also result in decreased ROM after CDA surgery. However, no significant progression of facet joint degeneration was observed during the 2-year follow-up period. A longer follow-up time may be needed to assess the impact of facet joint asymmetry on the development of facet joint degeneration after CDA surgery. Moreover, the correlations between the ROM differences and some other anatomical features still need to be confirmed. Another interesting result was that the difference in surgical segmental ROM was not sufficient to explain the difference in C2-C7 ROM. This discrepancy could be attributed to other level segments. Or the asymmetric 3-joint complex led to a change in cervical sagittal alignment and further led to a change in C2-C7 ROM.
The effect of neck pain on ROM should also be considered. The facet joints are densely innervated and the facetogenic pain is a frequent cause of neck pain.47-49 After CDA surgery, the kinematic and biomechanical changes could have adverse effects on the facet joints,32,50,51 and the non-physical stress on the facet joints could result in facetogenic neck pain, especially in asymmetric 3-joint complex.22,52 Differences in pain may account for the decreased C2-C7 ROM in the asymmetric group. Whereas, clinical scores showed no difference between symmetric and asymmetric groups in our study. We think that the complex source of neck pain should be noted. Pain caused by surgical trauma may affect ROM but does not correlate with the facet joint. Pain caused by psychological and social factors may affect clinical scores but not ROM. And the facetogenic pain may affect ROM while it could be associate with facet joint tropism. The clinical scores in our study can only assess the improvement of patients’ symptoms after CDA surgery but are not sufficient for the differential diagnosis of the source of pain, which requires a thorough history and physical examination, as well as facet blocks if necessary. Further work should be undertaken to identify the source of neck pain and determine whether the effect of facet joint asymmetry on ROM is caused by facetogenic pain.
Much of the current literature on CDA pay particular attention to the ROM. Some researchers53-56 defined ROM success as at least 4° of flexion-extension motion at the surgical segment after CDA. Kang et al. 57 summarized these research in a meta-analysis, the statistical test revealed the success rate of surgical segmental ROM ranged from 68.8% to 84.5%, and the pooled success rate was 79.4%. Some researchers hold that a low preoperative ROM was associated with a low postoperative ROM. Sasso et al. 58 performed a prospective randomized multicenter clinical trial including 242 CDA patients using Byran prosthesis. The regression analysis indicated a statistically significant relationship between preoperative and postoperative motion at 24 months. Another study conducted by Kim et al. 12 including 39 CDA patients using Byran prosthesis also reached similar conclusions. The height of the intervertebral disc space and prosthesis is also considered to be an important factor affecting postoperative segmental ROM. Li et al. 5 involved 160 CDA patients using Prestige LP prosthesis with a 30-month follow-up. They reported patients with less than 4 mm of preoperative intervertebral disc height had a larger incremental in postoperative ROM, and patients with 6-8 mm of postoperative intervertebral disc height could get the maximal ROM. Similarly, another study launched by Peng et al. 6 involving 166 CDA patients using Prodisc-C prosthesis reported similar results. Patients with less than 4 mm preoperative intervertebral disc height benefit more in postoperative ROM. They concluded that 5-7 mm is the optimal postoperative disc height to get the maximal ROM. Different surgical segment levels may also lead to different ROMs. Park et al. 10 conducted a study involving 146 single-level CDA patients using Prodisc-C prosthesis. In that study, the C4-C5 level had larger postoperative ROM compared with other levels before surgery. However, there was no significant difference in postoperative ROMs among each level. Different prosthesis designs might also affect the postoperative ROM. Kowalczyk et al. 4 included 60 CDA patients, involving 20 cases each receiving the Bryan, Prodisc-C, or Prestige LP disc prosthesis. The results showed Bryan and Prestige LP prosthesis preserved the preoperative ROM, whereas the Prodisc-C prosthesis increased postoperative segmental ROM. Rong et al. 8 tried to explain the change of ROM from the perspective of COR. By measuring and analyzing 24 CDA patients, they concluded that the postoperative ROM would be well preserved if the COR simulated by the prosthesis after CDA was close to the inherent location. Contrarily, the farther the simulated COR deviated from the preoperative location, the smaller the ROM would become. The sagittal alignment was also considered to be an influencing factor. Rabin et al. 9 involved 15 CDA patients using Prodisc-C prosthesis and found the shell angle was correlated significantly with ROM from neutral to the extension. The study by Kang et al., 59 including 41 CDA patients receiving Byran, Prodisc-C, and Prestige LP prosthesis with over 24 months follow-up, showed the segmental ROM at last follow-up was significantly correlated with the disc height increment. We proposed a new possible influencing factor in the present research. For the first time, we explored the correlation between the facet joint tropism and the postoperative ROM. According to the results, we can infer that the facet joint asymmetry at the surgical segment would affect the movement of the 3-joint complex after CDA. Therefore, we believe that it is necessary to include facet tropism in preoperative evaluation of CDA and identify the appropriate surgical patient, to obtain a better postoperative ROM.
The present study had several limitations. Firstly, the study is retrospective research with a relatively small sample size. Some surgical patients were not included in this study due to incomplete follow-up. Secondly, we included 4 levels of surgical segment from C3-C4 to C6-C7 in this study, neglecting the possibly different impact of facet joints on ROM at the different cervical levels. Thirdly, many factors could affect the ROM after CDA. Previous studies have suggested some factors, but their conclusions are not consistent. There may be confounding factors in this study that we did not pay attention to which could bias the results. Lastly, in the current study we only analyzed the Prestige LP, a ball-and-trough prosthesis. Further researches with more focus on the biomechanical characteristics of different prosthesis designs and the impact of facet joint asymmetry on the motion of different disc prostheses are therefore suggested.
Conclusions
The coronal and transverse asymmetry of the facet joints seemed to be correlated with decreased flexion-extension ROM at the surgical segment after CDA using Prestige LP. Regardless of the existence of asymmetric facet joints, most patients obtain significantly improved clinical outcomes after CDA surgery.
Footnotes
Author Contribution
Ziyang Liu and Xin Rong contributed equally to this study and should be considered co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by 2017 AOSpine China Research Grant (AOSCN(R)2017-18) and the Sichuan Province Science and Technology Program of China (No. 18ZDYF2182).