
Abstract
Objective:
The purpose of this study was to evaluate the feasibility of posterior occipital condyle screw (OCS) placement analysis of the safe trajectory area for screw insertion.
Methods:
Computed tomographic angiography scans of patients (46 males and 27 females) with normal occipitocervical structures were obtained consecutively. Vertebral artery (VA)-occiput distance <4.0 mm was defined as “unfeasible” for OCS fixation, and occipital-atlas angulation was measured to assess the feasibility of screw placement. Next, the placement of 3.5 mm diameter OCS was simulated, the probability of breach of structures surrounding occipital condyles was calculated, and placement parameters were analyzed.
Results:
OCS placement was feasible in 91.1% (133/146) of occipital condyles, and the feasible probability also presented a significant sex-related difference: The probability was higher for males than for females (95.7% vs. 83.3%, p < 0.05). The incidence of anatomical structures injured under screw placement limitation was 18.8% (VA), 81.2% (hypoglossal canal), 59.4% (occipital-atlas joint), and 40.6% (occiput bone surface). There were no significant differences between the left and right condyles in relation to the measured parameters (p > 0.05). The screw range of motion was significantly smaller in females than in males (p < 0.05). The feasibility of OCS placement and OCS range of motion were significantly greater in the kyphosis group (>5°) than in the other two groups (p < 0.05).
Conclusion:
OCS placement is a feasible technique for occipital-cervical fusion. The male group and occipitocervical region kyphosis group had a wider available space for OCS placement. Tangent angulation may be useful for the accurate and safe placement of an OCS.
Keywords
Occipital condyle screws (OCSs), initially described by Uribe et al. 1 and La Marca et al. 2 in 2008, are an alternative to standard occipital plates as the cephalad fixation points in occipital-cervical fusion. According to recent studies, 3 –8 the OCS offers the following advantages over a traditional occipital plate: (1) provides decreased lever arm length, longer screw length, and stronger pullout strength 9,10 ; (2) can be used in patients who underwent a previous suboccipital craniectomy 3 ; (3) has a low profile that leaves more available bony surface area for grafting and provides biomechanics characteristics equivalent to those of standard occipital plates 9,11 ; and (4) is in line with the ideal occipital-cervical fixation criteria proposed by Grob. 12
However, OC is a complex anatomic area surrounded by many important anatomical structures that restrict screw placement, especially the hypoglossal canal (HC) and vertebral artery (VA). Hence, the safe insertion of screws is crucial and needs further study.
To date, few studies have considered the horizontal segment of the VA in the planning of the OCS trajectory. Therefore, this study aimed to investigate the feasibility and safe trajectory area for OCS placement using computed tomographic angiography (CTA) and three-dimensional (3-D) reconstruction software.
Materials and methods
This study was approved by the institutional review board of the hospital. The study consisted of a review of 73 patients who underwent CTA from January 2015 to September 2017. Patients included 46 males and 27 females, ranging in age from 21 to 65 (average 40.3 ± 9.99) years. None of the patients had any evidence of infection, trauma, neoplastic lesions, cervical malformation, or VA anomalies.
Three-dimensional reconstruction
All CTA images were taken using a General Electric CT scanner (Philips Brilliance 64 CT; Philips Medical Systems, Eindhoven, The Netherlands) with the following parameters: scan voltage 120 kV, scan current 280 mA, matrix 512 × 512, and slice thickness 1 mm. All data were obtained in a DICOM format file and inputted into Mimics 19.0 (Materialise, Leuven, Belgium) for generation of a 3-D reconstruction model of the occiput, atlas, axis, and VA (Figure 1).

(a) Posterior and (b) sagittal views of 3-D reconstruction based on CTA data. CTA: computed tomographic angiography.
Anatomic parameter measurements
The 3-D model after screw placement was inputted into 3-matic Research 11.0 (Materialise), with the assistance of the Analyze and Sketch module. The following screw placement parameters were measured:
Occipital-atlas angulation (OAA): the angle between the McRae line and middle of the atlas arch line (Figure 2(a)). All patients were classified into three groups as follows: lordosis group (<−5°), neutral group (−5° to 5°), and kyphosis group (>5°). VA-occiput distance (VOD): the vertical distance from the inferior margin of the occipital bone to the superior surface of the VA (Figure 2(b)). We defined a VOD <4.0 mm as “unfeasible” for OCS fixation because the screw diameter in this technique should always be 3.5–4.0 mm (Figure 2(c)).

(a) McRae line and middle of the atlas line form OAA. (b) The vertical distance from the inferior margin of the occipital bone to the superior surface of the vertebral artery is the VOD. (c) A case of VOD < 4 mm could not accommodate a screw placement. (The red arrows showed the screw injure in the surrounding structures.) OAA: occipital-atlas angulation; VOD: vertebral artery-occiput distance.
Screw placement simulation
The screw in STL format with a diameter of 3.5 mm and a length of 32 mm was introduced into the 3-D model with a VOD >4 mm, and the middle entry point for the OC described by Lee et al. was applied. 7 The OCS placement on each side was simulated with maximum cranial limitation (screw injured the HC or the course of the VA) and minimum cranial limitation (screw injured the occipital-atlas joint (OAJ) or the occiput bone surface), respectively. We ensured that the screw was parallel to the macro-axis of the OC to realize the maximum screw placement length during OCS simulated placement. Next, the screw position was reconfirmed on the sagittal view and coronal view (Figure 3).
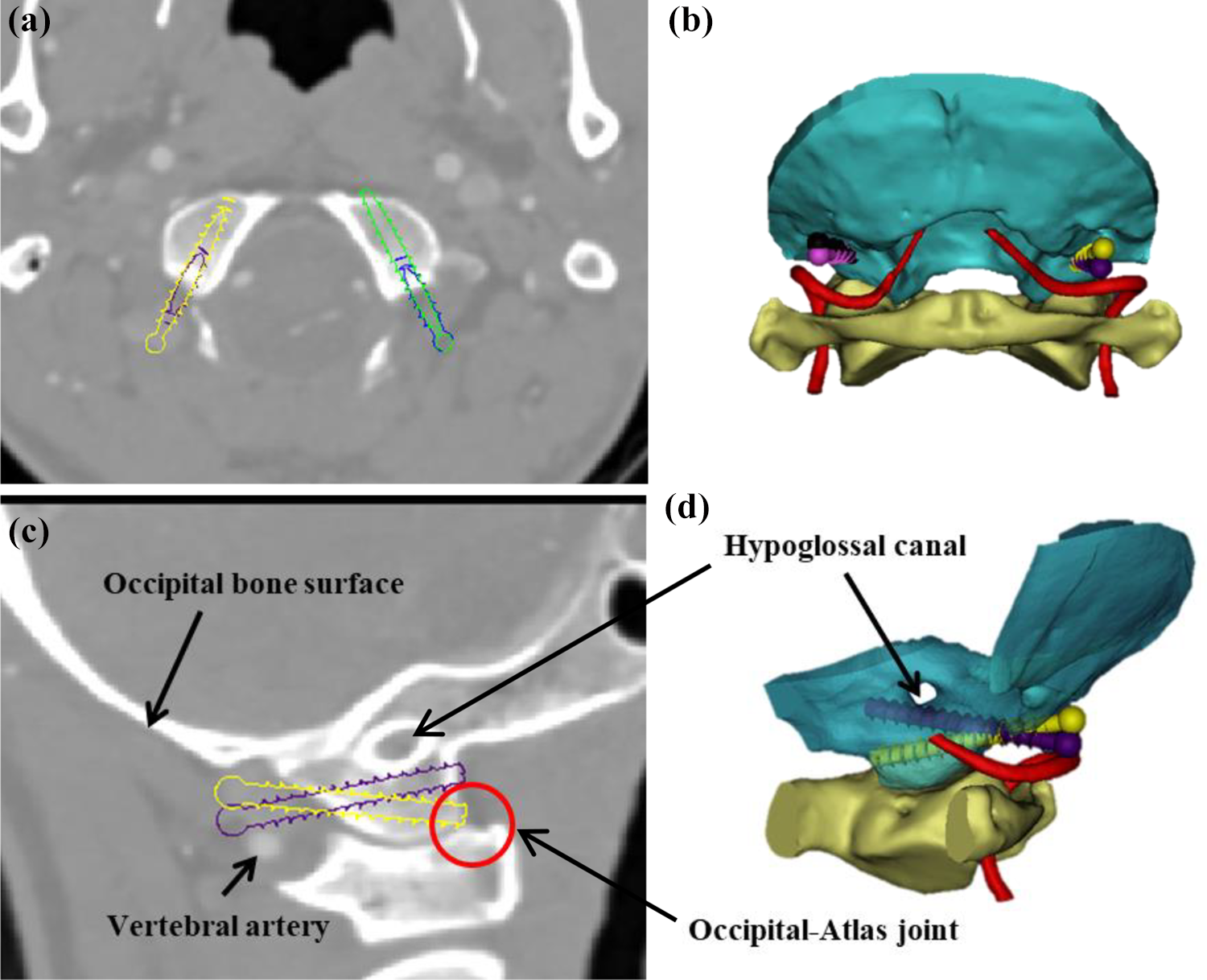
The screw position and the relationship between the OCS and surrounding structures after simulated placement. OCS: occipital condyle screw. (a) Transverse and (c) sagittal views showed the screw position and relationship between the OCS and surrounding structures after simulated placement. (b)(d) 3-D reconstruction after simulated placement. OCS: Occipital Condyle Screw.
Placement parameter measurements
After the simulated screw placement, the model was inputted into 3-matic Research 11.0 again. Then, with the Analyze and Sketch module, the base plane of the occiput was determined by the midpoint of the anterior and posterior edge of the foramen magnum, and the axis of the screw was established. In addition, a sketch section of the screw sagittal plane was established, and the occipital tangent line leading from the entry point was marked. The following screw placement parameters were measured: Maximum cranial angulation and minimum cranial angulation (Max-CA and Min-CA, respectively): the angle between the axis of the screw and the base plane of the occipital bone with maximum cranial limitation and minimum cranial limitation, respectively (Figure 4(a)). Cranial angulation range (CA-R): the difference between Max-CA and Min-CA. Maximum tangent angulation and minimum tangent angulation (Max-TA and Min-TA, respectively): the angle between the tangent line and the axis of the screw with maximum cranial limitation and minimum cranial limitation, respectively (Figure 4(b)). Tangent angulation range (TA-R): the difference between Max-TA and Min-TA.

(a) The base plane of the occiput and the axis of the screw form CA. (b) The tangent line of the occipital and the axis of the screw form TA. CA: cranial angulation; TA: tangent angulation.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (IBM, Armonk, New York, USA). The mean ± standard deviation and 95% confidence interval were calculated for all parameters. Sex differences in measurements were assessed using independent samples’ t-test, while paired student’s t-test was used to compare the difference between the right and left sides. One-way analysis of variance (ANOVA) was performed to compare the placement parameters of the different OAA groups. A χ 2 test was used to compare the feasibility of screw placement among the different OAA groups. Pearson correlation coefficients were calculated to determine the correlation between CA-R and VOD with OAA.
Results
A total of 73 consecutive patients completed 3-D reconstruction of the occipital-cervical junction, and 91.1% of the OCs could accommodate 3.5 diameter screw placement. The measurement and comparison results of the placement parameters are listed in Table 1. There was no sex difference in OAA (p > 0.05). There were no significant differences between the left and right condyles in relation to the measured parameters (p > 0.05). Males had significantly higher VOD, Max-CA, Max-TA, CA-R, and TA-R values, while Min-CA and Min-TA were significantly lower in males than in females (p < 0.05). The OAA factor seemed to present a good correlation with the VOD and CA-R (VOD: r = 0.760; CA-R: r = 0.765, p < 0.05).
Measurement results of screw placement parameters.

OAA: occipital-atlas angulation; Max-CA: maximum cranial angulation; Min-CA: minimum cranial angulation; Max-TA: maximum tangent angulation; Min-TA: minimum tangent angulation; CA-R: cranial angulation range; TA-R: tangent angulation range; VOD: vertebral artery-occiput distance; SD: standard deviation.
aCA-R versus TA-R, statistical insignificance.
The structure was injured by screw placement with maximum cranial limitation, and the minimum cranial limitation of each OAA group is presented in Table 2. The χ 2 test suggested significant differences in the incidences of structural injury. The incidences of VA compromise in screw placement with maximum cranial limitation were 60%, 18.4%, and 5.8% for the lordosis, neutral, and kyphosis groups, respectively. The incidences of OAJ injury in screw placement with minimum cranial limitation in the three groups were 20%, 57.9%, and 76.2%.
The results of anatomical structure injury with screw placement limitation.

Max-CA: maximum cranial angulation; Min-CA: minimum cranial angulation.
The screw placement parameters of different curvatures are presented in Table 3. The mean Max-CA, Max-TA, CA-R, TA-R, and VOD values were significantly greater in the kyphosis group than in the other two groups (p < 0.05). The lordosis group had larger Min-CA and Min-TA values than did the neutral and kyphosis groups (p < 0.05). The kyphosis group had the highest feasibility (100%) of screw placement, followed by the neutral (95%) and the lordosis group (62.5%; Table 4).
Measurement results of screw placement parameters in the different OAA groups.

OAA: occipital-atlas angulation; Max-CA: maximum cranial angulation; Min-CA: minimum cranial angulation; Max-TA: maximum tangent angulation; Min-TA: minimum tangent angulation; CA-R: cranial angulation range; TA-R: tangent angulation range.
a−5° to 5° versus <−5°, statistical significance.
b>5° versus −5° to 5°, statistical significance.
The feasible probability of OCS placement in the different sex and OAA groups.
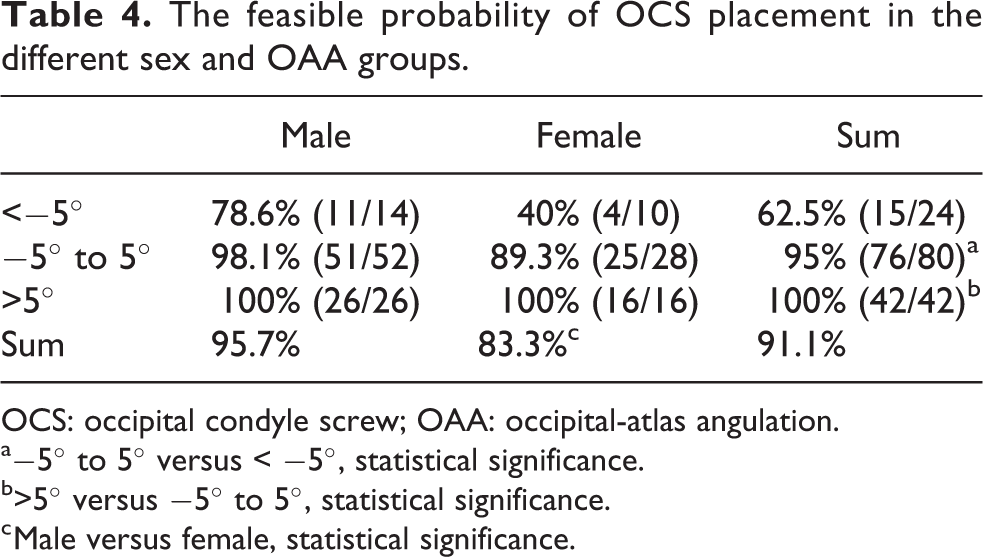
OCS: occipital condyle screw; OAA: occipital-atlas angulation.
a−5° to 5° versus < −5°, statistical significance.
b>5° versus −5° to 5°, statistical significance.
c Male versus female, statistical significance.
Discussion
The occipital bone, atlas, and axis constitute the functional unit of occipitocervical movement, that is, the craniovertebral junction. 13,14 The OC is an important part of craniovertebral junction and is the cephalad of the atlanto-occipital joint. The OCS has recently been developed as an alternative fixation point. 1,2
Lee et al. 7 performed a CT-based feasibility analysis and reported that OCS placement is feasible in up to 93% of cases. Moreover, Zhou et al. 15 concluded that the success rate of OCS placement was 92%, as measured by using digital 3-D reconstruction. In this study, a total of 133 OCs could accommodate the placement of screws with a diameter of 3.5 mm. Our results revealed that males had significantly higher values in the VOD and range of screw placement motion, which was attributed to the anatomical parameters of males being much greater than those of females, Zhou et al. 15 and Srivastava et al. 16 confirmed this result via morphometric analysis of the OC based on CT. Hence, males have more sufficient OC volume to accommodate screw placement, and they have a higher feasibility of OCS placement than females do (95.7% vs. 83.3%). In addition, we found that the VOD and OAA factors seemed to be positively correlated with OAA, which means that kyphosis patients have a wider posterior area for OCS insertion (Figure 5). On the premise of choosing the middle entry point of the posterior area of OC, screw placement in the kyphosis group would have a wider range of motion and a higher feasibility than that in the other groups.

(a) VOD and (b) CA-R showed a positive correlation with OAA. VOD: vertebral artery-occiput distance; CA-R: cranial angulation range; OAA: occipital-atlas angulation.
The topographical anatomy of the OC is rather complex due to its intimate relation with many anatomical structures. The HC and the course of the VA are the most important anatomical structures affecting screw placement in the OC. In this study, we performed a simulation to evaluate the impact of the peripheral structures of the OC on screw placement through CTA 3-D reconstruction. We found that 25 screws (18.8%) breached the VA under maximum cranial limitation, while 79 screws (59.4%) breached the OAJ under minimum cranial limitation. The HC is easier to injure during the placement of an OCS, and the method described by Uribe et al. 1 that involved pulling the horizontal segment of the VA outward and downward during the operation may reduce the risk of VA injury. Since the lordosis group had a narrow VOD, there was insufficient space for screw placement and motion, thus, the injury probabilities of the VA and OS were higher in the lordosis group than in the other groups (Figure 6).

(a) The frequency of HC and VA injury in the different OAA groups. (b) The frequency of OAJ and OS injury in the different OAA groups. HC: hypoglossal canal; VA: vertebral artery; OAA: occipital-atlas angulation; OS: occiput bone surface; OAJ: occipital-atlas joint.
The HC is a supracondylar structure surrounded by the cortical bone 17 . Frankel et al. 6 conducted a cadaveric study and demonstrated that HC injury could be avoided as the sagittal plane angulation was less than 10° cranially. EI-Gaidi et al. 18 reported that the average CA was 4° ± 6.2°. The results of this study showed that the average Max-CA and Min-CA were 11.11° ± 2.72° and −1.64° ± 2.72°, respectively. However, the CA could not guide the screw placement accurately because the base plane of the occiput is hard to pinpoint. Hence, we proposed a new placement parameter for the OCS, termed occipital TA. TA is formed by the tangent line from the entry point to the posterior surface of the occiput and the axis of the screw. TA could be estimated visually during the operation, and TA does not change with body position. In theory, TA varies with CA with the condition of an unchanged condylar entry point, and the TA-R should be consistent with the CA-R. Moreover, TA could combine the entry point and medial angulation to form a unique screw placement trajectory to assist in accurate screw placement. We found that the average Max-TA and Min-TA were 20.80° ± 3.28° and 8.12° ± 2.53°, respectively. The average value of the TA-R was almost the same as that of the CA-R, and the difference may be caused by measurement errors. Based on our findings, TA can be accurately evaluated instead of CA to assist in posterior OCS placement, which can increase the safety and success rate of screw implantation.
This study has limitations. The measurements in our study were performed by a single assessor, which might lead to observer bias. The sample size of the patients might not be ideal for a normative study. Moreover, we did not conduct a cadaveric study to verify the feasibility of TA for assisting in OCS placement.
Conclusions
Our study provides a simulation for the OCS placement based on CTA data. We recommend preoperative CTA and screw placement simulation as critical produces. The OAA could assess the feasibility of OCS placement. In summary, a new parameter was introduced to guide OCS placement more accurately and securely than CA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.