
Abstract
Study Design:
Retrospective cohort study.
Objective:
To study the prevalence of pre-operative osteoporosis treatment, and its effect on risk of ORC, revision surgery and costs in osteoporotic patients undergoing ≥3-level spinal fusion for degenerative pathology.
Methods:
Patients and procedures of interest were included using International Classification of Diseases (ICD) and Current Procedural Terminology (CPT) coding. Our outcome measures were ORC at 1-year post-operatively and included instrumentation complications, pathological fracture, and revision surgery. Kaplan-Meier survival curves and Cox proportional hazards analysis was done to study the effect of osteoporosis treatment on risk of ORC.
Results:
We included a total of 849 patients with documented osteoporosis undergoing ≥3-level spinal fusion. White (85.6%), female (82.7%), and 60-79 years of age (79.9%) was the most common demographic. Of entire cohort, 121(14.3%) were on osteoporosis treatment prior to spinal fusion. Of treated patients, 52/121 (43.0%) had continued prescriptions at 1 year post-operatively. Treated patients and not-treated patients had 1-year ORC incidence of 9.1% and 15.0%, respectively. The average 1-year reimbursement/patient for managing ORC was $3,053 (treated) and $21,147 (not-treated). On adjusted cox analysis, pre-operative osteoporosis treatment was associated with a lower risk of ORC (HR: 0.53, 95% CI: 0.28-0.99, p = 0.04).
Conclusions:
Pre-operative osteoporosis treatment is associated with lower risk of ORC and revision surgery at 1-year after ≥3-level spinal fusion. There is a low incidence of osteoporosis treatment prior to spinal fusion, and subsequently a low rate of treatment continuation after surgery. These findings highlight the need for heightened awareness, patient education and management of osteoporosis before elective multi-level spinal fusion.
Keywords
Introduction
Osteoporosis is characterized by low bone mineral density (BMD), resulting in weak bone microarchitecture and higher risk of fracture. As defined by the World Health Organization (WHO), a T-score ≤ −2.5 standard deviation below healthy adult mean BMD on dual energy x-ray absorptiometry (DEXA) is considered osteoporosis.1,2 It is estimated that 10.3% of adults more than 50 years old in the United States have osteoporosis based on this definition. 3
Numerous studies have shown that there is a higher risk of compression fracture,4,5 pedicle screw loosening or failure of instrumentation,4,6,7 proximal junctional kyphosis,4,8,9 and pseudoarthrosis7,10 due to osteoporosis in patients undergoing spinal fusion. Consequently, there is growing emphasis on peri-operative medical management of osteoporosis in these patients. 11 While treatment of osteoporosis with bisphosphonates or teriparatide has shown to reduce vertebral fractures in nonsurgical patients, its clinical impact on osteoporosis related complications (ORC) in spinal fusion is limited.1,12-14 A recent meta-analysis of 536 patients in 9 heterogenous studies reported high fusion rates and decreased risk of ORC in medically treated osteoporosis patients undergoing spinal fusion. 12 However, these numbers also highlight the need for more evidence from bigger patient populations. Administrative database analyses have the advantage of studying a large cohort of patients with good accuracy and are increasingly being used to supplement evidence from clinical studies.15,16
The objective of this claims data analysis from a large national payor was to study the prevalence of pre-operative osteoporosis treatment, and its effect on risk of ORC, revision surgery and costs in osteoporotic patients undergoing ≥3-level spinal fusion for degenerative pathology. This data will add evidence to existing clinical literature and guide pre-operative decision making in this at-risk population.
Materials and Methods
Data Source
The Humana national claims database (2007-Q3 2016) covering 22 million commercial and Medicare Advantage beneficiaries was used for analysis. Using this database, longitudinal research can be performed over the full data set using one or combination of identifiable fields on claims records. These include but are not limited to; International Classification of Diseases, ninth and 10th Revision (ICD-9 and 10) diagnosis and procedural coding, Diagnosis Related Group (DRG), Current Procedural Terminology (CPT), generic drug codes, prescription National Drug Code (NDC), discharge status, physician specialty, etc. Data is de-identified and HIPAA (Health Insurance Portability and Accountability Act, 1996) compliant and was accessed through the PearlDiver Technologies research platform (PearlDiver Inc., Colorado Springs, CO). 17
Data Extraction
The first occurrence of ≥3-level spinal fusion for degenerative pathology was queried using respective ICD-9 codes (81.63 for 3-7 level, 81.64 for 8 or more level) between 2007 and Q3 2015. Procedures were queried up to Q3 2015 to allow analysis of 1-year outcome measures till Q3 2016. To reduce confounding effects of major trauma/surgery on outcomes, patients with a current/prior diagnosis of spinal fusion, spine fracture/neoplasm, infection, lower extremity arthroplasty/fracture fixation, rheumatoid arthritis, etc. were excluded. Subsequently, we queried patients with active insurance enrollment at least 1-year prior to 1-year after surgery. To create our final study cohort, we selected patients who had a diagnosis of osteoporosis (ICD 733.00, 733.01, 733.02, 733.09) and underwent dual-energy X-ray absorptiometry (DEXA) scan (CPT-77080, 77081, 77082) within 1-year before index surgery. Given the lack of ability to study DEXA scores with this database, follow-up DEXA scans were not studied in our patient cohort. The codes and definitions used for inclusion/exclusion of patients have been given in Supplemental Appendix, Table A1.
Pharmacological Treatment of Osteoporosis
We divided our final study cohort in 2 groups: treated and not-treated, based on whether they received anti-osteoporosis treatment within the year before index surgery. However, to maintain uniformity we excluded patients who were not-treated before surgery but had anti-osteoporosis treatment after surgery. We used prescription data to identify most widely accepted pharmacological treatments for osteoporosis, which included bisphosphonates (Risedronate sodium, Ibandronate sodium and Alendronate sodium, Zoledronic Acid), and Teriparatide.1,11-14 In our patient cohort, there were less than 10 patients who had Denosumab treatment. These patients were excluded from analysis to maintain consistency and include only most prevalent pharmacotherapies.
Outcome Measures
Our primary outcome measure was occurrence of post-operative ORC. These included instrumentation complications (ICD 996.49, 996.40, 996.78) and pathological vertebral fracture (ICD 733.13). We also identified patients who underwent revision fusion (ICD 81.32, 81.33, 81.34, 81.35, 81.36, 81.37, 81.38, 78.69) for these complications within 1-year after index surgery. We ensured that these were new complications by excluding patients who already had these diagnoses or procedures prior to index surgery. The definitions for these complications have been given in Supplemental Appendix, Table A2.
Data Analysis
Quantitative variables have been reported as frequency and percentage, and quantitative variables as mean with standard deviation. Kaplan-meier survival curves were generated to depict survival (freedom from ORC) in patients treated and not-treated for osteoporosis before spinal fusion. To analyze significance of pre-operative osteoporosis treatment on risk of ORC, multivariate Cox proportional hazards analysis with adjustment for various demographic and clinical variables was done. Demographics such as age, gender, ethnicity, region, and clinical comorbidity burden using Charlson Comorbidity Index (CCI) 18 and comorbidity definitions (as defined in the Medicare Research Chronic Conditions Data Warehouse) 19 were used for adjustment. To adjust for the type and magnitude of spinal fusion, we identified cervical fusions (anterior, ICD 81.02, posterior, 81.03, and combined) and thoraco-lumbar fusions (81.04, 81.05, 81.06, 81.07, 81.08) in both study groups. We also distinguished patients who received osteotomies (CPT-22206, 22207, 22208, 22210, 22212, 22214, 22216). These variables are important risk factors for post-operative complications and have been included in our adjusted analysis.
For estimation of risk of ORC, adjusted hazard ratio with 95% confidence interval (CI) in treated osteoporosis patients has been reported, with not-treated patients serving as reference. The global significance of the cox model was judged by significant p-values on Likelihood ratio, Wald and score log-rank tests. For all analyses, a p-value of <0.05 has been considered statistically significant. Statistical analysis was carried out in R (The R Project for Statistical Computing) through the PearlDiver interface.
Results
We included a total of 849 patients in our analysis. Majority of patients were white (85.6%), female (82.7%), and 60-79 years of age (79.9%). In our study cohort, 121 (14.3%) patients were on osteoporosis treatment before surgery. Univariate analysis of demographic and clinical variables among patients treated and not-treated for osteoporosis have been given in Table 1.
Univariate Analysis of Demographic and Clinical Variables in Osteoporotic Patients Who Underwent ≥3-Level Spinal Fusion. Humana Database (2007-Q3 2015).
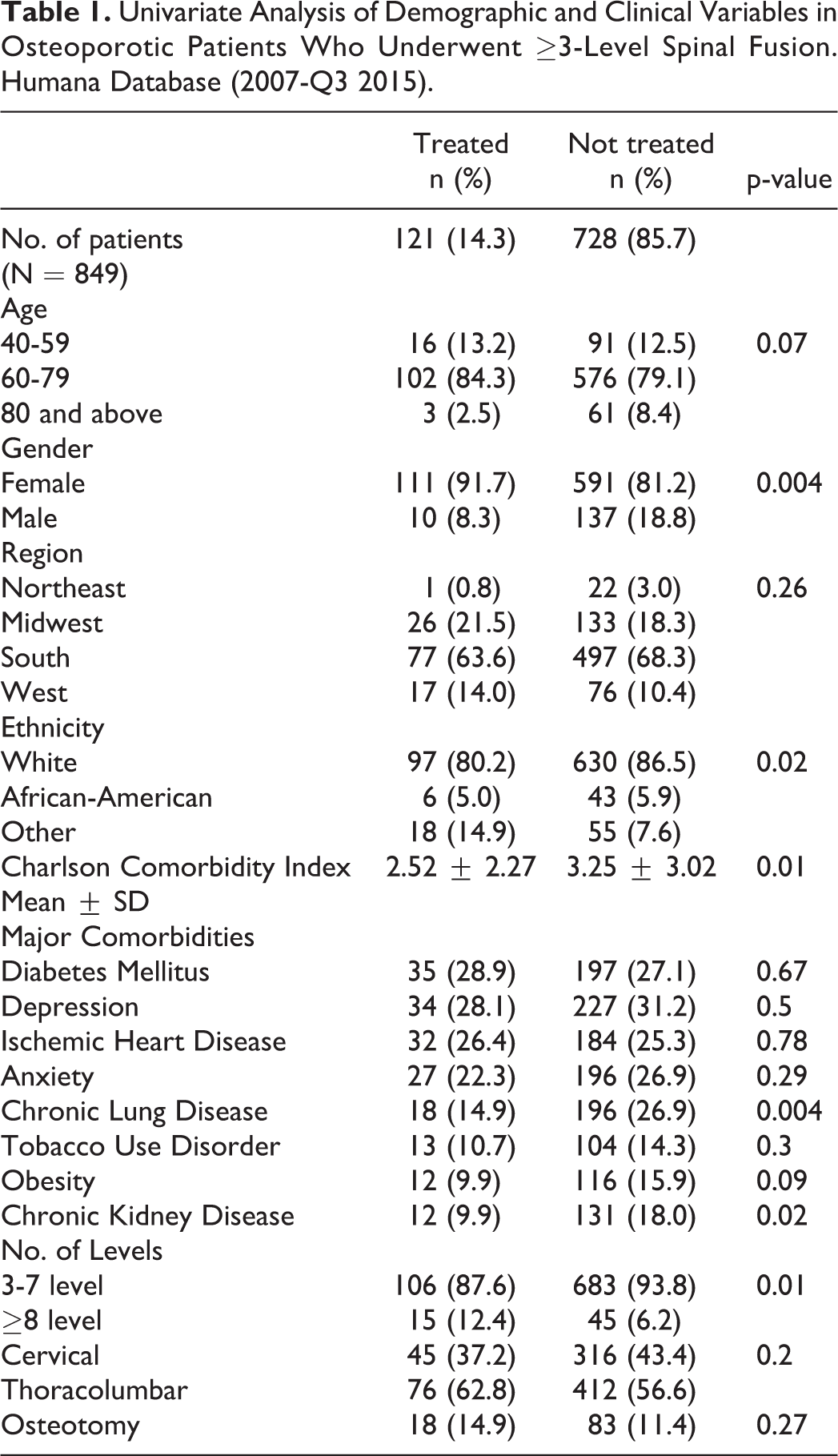
Out of 121 patients on osteoporosis treatment, 106 (87.6%) received bisphosphonates and 15 (12.4%) were on teriparatide. The average reimbursement for bisphosphonate and teriparatide treatment was $596 and $6,200 per patient in the year before spinal fusion. Of the treated patients, 52/121 (43.0%) had continued prescriptions at 1 year post-operatively.
Treated patients had a 1-year ORC cumulative incidence of 9.1% (95% CI: 3.8-14.1%), and not-treated patients had a 15.0% (95% CI: 12.3-17.5%) complication rate (Figure 1). Out of the 11/121 (9.1%) patients in the treated group who had ORC, 8 (72.7%) had a diagnosis of instrumentation related complications, 2 (18.2%) had new pathological vertebral fracture, and 1 (9.1%) had both. None of these patients underwent refusion within a year after index surgery. As a sub-group analysis, the rate of ORC was 9.6% (5/52) and 8.7% (6/69) in treated patients with and without continued 1-year post-operative therapy, respectively.
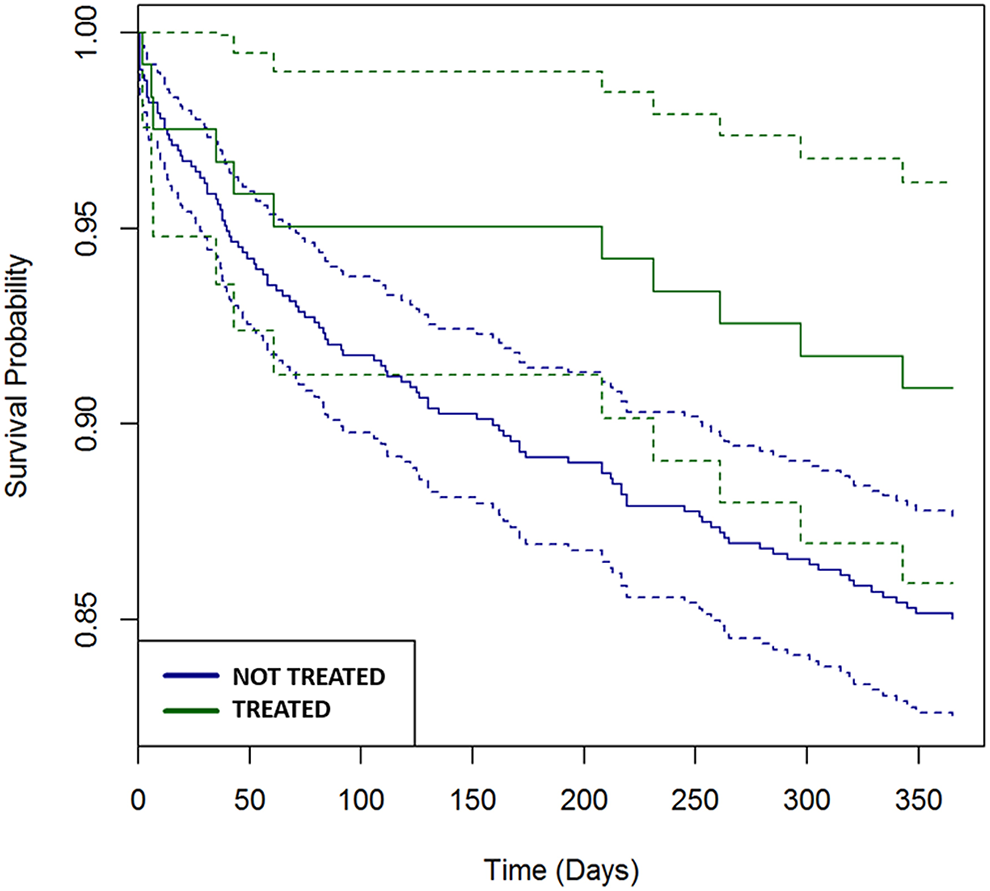
Kaplan-Meier survival curves showing freedom from osteoporosis related complications (ORC) at 1-year among treated and not-treated osteoporotic patients undergoing multi-level spinal fusion. Humana database (2007-Q3 2015).
In the 15.0% (109/728) not-treated patients who had ORC, 72 (66.1%) and 35 (32.1%) had instrumentation related complications and new vertebral pathological fracture, respectively. Two (1.8%) patients had diagnoses of both. In patients with ORC, 20 (18.3%) patients underwent revision fusion for these complications at 1-year post-operatively.
The total and average per patient 1-year reimbursement for managing ORCs in treated patients (n = 11) was $33,583 and $3,053, respectively. The total cost of care for ORCs in not-treated patients (n = 109) was $2,305,206, with an average reimbursement of $21,147 per patient. Revision surgery in this group had an average per patient reimbursement of $28,629 with average hospital length of stay of 9.0 days.
On adjusted cox analysis, pre-operative osteoporosis treatment was associated with a lower risk of ORC (HR: 0.53, 95% CI: 0.28-0.99, p=0.04). Cervical fusions (vs. Thoraco-lumbar) were also associated with a lower risk of ORC (HR: 0.61, 95% CI: 0.40-0.93, p=0.02), whereas spinal osteotomy (vs. no osteotomy) was significantly associated with ORC (HR: 2.52, 95% CI: 1.58-4.02, p < 0.001). While number of levels of surgery was significantly higher in the treated group on univariate analysis (Table 1), it was not significant for ORC on adjusted Cox analysis (HR 1.61, 95% CI: 0.62-0.94, P = 0.08).
Discussion
There are various recommendations to minimize risk of ORC in patients undergoing spinal fusion.1,2,11,13 However, the published clinical evidence on the benefit of pharmacologic treatment of osteoporosis in spinal fusion is limited.1,12-14 We have analyzed a cohort of 849 patients with osteoporosis who underwent ≥3-level spinal fusion for degenerative pathology to study the effect of osteoporosis treatment on risk of ORC. A distinct advantage of a study such as ours is that we were able to include more patients in a single analysis than a meta-analysis of heterogenous studies. 12 Additionally, we were able to describe prevalence of pre- and post-operative osteoporosis treatment in a national cohort of multi-level spinal fusion patients with data reflecting the costs to the healthcare system due to ORC. We found that pre-operative pharmacological treatment of osteoporosis is independently associated with significantly lower risk of ORC and revision surgery in patients undergoing ≥3-level spinal fusion for degenerative pathology.
Our cohort was predominantly white, females between the age of 60 and 79 which corresponds to the most common demographic with primary senile osteoporosis. 20 Of the entire cohort, only 14.3% osteoporotic patients were on osteoporosis treatment before surgery. Prior studies have found low rates of osteoporosis screening and treatment in patients above 50 years of age undergoing spinal fusion.21-23 There remains a gap in osteoporosis treatment with reports of low rate of initiation of anti-osteoporosis treatment after sustaining fragility 20 and new vertebral compression fractures. 24 In patients undergoing multi-level thoracolumbar fusions, it will be beneficial to screen and treat patients for osteoporosis. This will require additional efforts on the part of the spine surgeon for coordination of care with primary care provider or endocrinologist. Due to the potential for ORC and additional costs in untreated osteoporotic patients, it seems prudent in order to improve the quality and value of care. There are some barriers to this, however. Given there is still controversy on monitoring of osteoporosis treatment,25,26 it is difficult to estimate adequate duration of osteoporosis treatment before scheduling elective spinal fusion in at-risk patients. Till further clinical evidence is available, it seems reasonable to at least initiate treatment pre-operatively and maintain compliance after surgery.
In our analysis, 15% not-treated osteoporotic patients had ORC within a year after index spinal fusion. Two-third had instrumentation related complications and one-third sustained a new vertebral pathological fracture. Of patients with ORC in this group, 18.3% underwent revision surgery with an average reimbursement of $28,629 from payors. In contrast, treated patients had a 9.1% post-operative ORC rate, and no patients underwent revision surgery within 1-year after index spinal fusion. Adjusted risk analysis revealed lower risk of ORC and revision surgery due to ORC in osteoporosis treated patients. Our results add to existing literature regarding the beneficial effects of osteoporosis treatment on spinal fusion outcomes. Bisphosphonates increase BMD by inhibiting osteoclasts, whereas intermittent teriparatide therapy works by activating osteoblasts.2,11,14 Despite some concerns that bisphosphonates inhibit fusion due to its mechanism, literature suggests that both bisphosphonate and teriparatide treatment lead to good fusion. Although, fusion rates are somewhat higher with teriparatide as compared to bisphosphonates. 12 Limited evidence from prior literature also suggests decreased risk of cage subsidence and vertebral fractures after spinal fusion in bisphosphonate treated patients as compared to control. 12 A couple of studies have compared the risk of complications after spinal fusion between teriparatide and bisphosphonates, with results favoring teriparatide.27,28 A comparative analysis among the 2 classes of medications was not considered feasible in our analysis given only 15 patients in the teriparatide treatment group.
The higher risk of ORC in not-treated patients also leads to significant financial burden as we found additional costs averaging over $20,000 per patient. This is important given the increasing emphasis on healthcare cost reduction and value-based care. Given the elective nature of spinal fusion for degenerative pathology, it is certainly beneficial to manage osteoporosis pre-operatively in these patients. This is especially true in multi-level thoraco-lumbar fusions with planned osteotomies, as these were also significantly associated with ORC in our analysis.
Not only did our analysis suggest low rates of osteoporosis treatment before spinal fusion, but less than half of treated patients continued treatment in the year after surgery. We hypothesize suboptimal osteoporosis follow-up and/or care coordination postoperatively with provider managing osteoporosis treatment. A recent review of literature found poor overall patient persistence and adherence with oral bisphosphonate therapy which drops significantly over time. Some determinants for this include medication type and frequency, age, race/ethnicity, gender, educational status and income. 29 Cost of medications may be another determinant of compliance. We found the average annual cost of bisphosphonate therapy before spinal fusion to be just under $600, and teriparatide more than 10-times higher. High patient copayments for teriparatide may be a factor for poor compliance with treatment. 30 As mentioned above, close coordination with medical provider will be required to ensure maintenance of osteoporosis therapy after surgery.
Our study is limited by its retrospective analysis of insurance claims data. There may be inaccuracies due to coding methodology or missing data. Although we have included patients based on ICD codes for osteoporosis who underwent DEXA scans, the BMD measurement and T-scores are not available from claims data. We were unable to study clinical and surgical variables such as severity of disease, imaging studies, patient reported outcomes, surgical technique, cement augmentation, screw size/density, interbody cages, nature of instrumentation related complications, reason for revision surgery, etc. We have reported cost of medications and complications from payor reimbursement; however, we are unable to study cost-effectiveness of various treatments. We were also unable to compare risk of complications between bisphosphonates and teriparatide.
In conclusion, our analysis of osteoporosis patients undergoing multi-level spinal fusion for degenerative pathology found that pre-operative osteoporosis treatment is associated with lower risk of ORC and revision surgery at 1-year post-operatively. There is a low incidence of osteoporosis treatment prior to spinal fusion, and subsequently a low rate of treatment continuation after surgery. These findings highlight the need for heightened awareness, patient education and management of osteoporosis before elective spinal fusion. Given the higher burden of healthcare costs in these patients, there will be implications in value based and bundled payment models moving forward. Future directions include studying the adequate treatment duration before scheduling spinal fusion in osteoporotic patients, determining cost-effectiveness of bisphosphonates vs. teriparatide, identifying reasons for poor patient compliance with treatment, and improving care coordination with medical providers to ensure consistent treatment.
Supplemental Material
Supplemental Material, Supplementary_Table_1 - Prevalence of Osteoporosis Treatment and Its Effect on Post-Operative Complications, Revision Surgery and Costs After Multi-Level Spinal Fusion
Supplemental Material, Supplementary_Table_1 for Prevalence of Osteoporosis Treatment and Its Effect on Post-Operative Complications, Revision Surgery and Costs After Multi-Level Spinal Fusion by Nikhil Jain, Lawal Labaran, Frank M. Phillips, Safdar N. Khan, Amit Jain, Khaled M. Kebaish and Hamid Hassanzadeh in Global Spine Journal
Supplemental Material
Supplemental Material, Supplementary_Table_2 - Prevalence of Osteoporosis Treatment and Its Effect on Post-Operative Complications, Revision Surgery and Costs After Multi-Level Spinal Fusion
Supplemental Material, Supplementary_Table_2 for Prevalence of Osteoporosis Treatment and Its Effect on Post-Operative Complications, Revision Surgery and Costs After Multi-Level Spinal Fusion by Nikhil Jain, Lawal Labaran, Frank M. Phillips, Safdar N. Khan, Amit Jain, Khaled M. Kebaish and Hamid Hassanzadeh in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.