
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To evaluate the effect of zoledronic acid, an anti-osteoporosis treatment, during the perioperative period on vertebral body bone mineral density (BMD) after spinal fusion surgery in postmenopausal women with osteoporosis.
Methods:
The medical records of postmenopausal patients with osteoporosis who underwent instrumented intervertebral fusion for lumbar degenerative disease between July 2016 and May 2018 were reviewed. Patients with comorbidities or condition which might affect bone metabolism were excluded. Forty-six patients did not receive anti-osteoporosis treatment before surgery and during the postoperative follow-up (untreated group). Another 46 patients who was treated with zoledronic acid perioperatively were matched for age and body mass index to patients in the untreated group. Preoperative and postoperative dual-energy X-ray absorptiometry (DEXA) records and lumbar BMD values of the involved spinal segments and of the cephalad levels, as well as of the femoral neck were recorded.
Results:
A significant decrease of cephalad vertebral BMD values was observed in the untreated group (-11.47%, P < 0.001), with a slight decrease of the femoral neck (-1.28%, P > 0.05). Zoledronic acid prevented rapid bone loss after instrumented intervertebral fusion surgery, with a bone loss in the cephalad levels of -0.76 ± 4.71% compared to -11.47 ± 16.45% in the untreated group (P < 0.001). while the change in BMD of the femoral neck in the treated group was 1.52 ± 5.88% compared to -1.28 ± 6.58% in the untreated group (P = 0.036).
Conclusions:
Perioperative zoledronic acid treatment may offer protection against a significant decrease in BMD of cephalad vertebrae after spinal fusion surgery among postmenopausal women with osteoporosis.
Introduction
Spinal instrumented fusion using segmental pedicle screws is a widely accepted treatment for lumbar degenerative diseases which provides improved pain control and functional scores.1,2 However, as more patients undergo spinal fusion, reports of fusion-related complications have increased.3,4 Fracture of vertebral levels adjacent to rigid pedicle screw fixation have been described.5,6 This increased risk of fracture might result from altered spinal kinematics after arthrodesis, resulting in relative hypermobility of spinal segments adjacent to the fused level.7,8 This change in segmental spinal biomechanics may result in a higher incidence of proximal vertebral compression fractures (VCFs). Osteoporosis further increases the fracture risk, especially among postmenopausal women.
Rigid spinal instrumentation can lead to device-related osteoporosis of the fused segment, as well as in a decrease in the bone mineral density (BMD) of adjacent vertebrae, which may contribute to adjacent level VCFs after spinal fusion surgery.9-11 This decrease in BMD may be related to the immobilization itself or to the altered biomechanics resulting from arthrodesis. However, the mechanism of BMD loss after spinal fusion surgery remains to be fully clarified. Zoledronic acid (ZA) is an effective osteoporosis treatment among postmenopausal women, significantly reducing the risk of vertebral, hip, and other fractures. 12 Moreover, ZA use does not appear to prevent successful lumbar fusion.13,14 However, to our knowledge, no previously published clinical studies have investigated the influence of ZA on the change in BMD of the vertebral body of adjacent to the fused segment after instrumented intervertebral fusion. Therefore, our aim in this study was to evaluate whether ZA is effective in decreasing the BMD of the adjacent vertebral body after spinal surgery among postmenopausal women with osteoporosis.
Materials and Methods
Statement of Ethics
Our study design was approved by the Ethics Committee of Tangdu Hospital (approval ID: 2019A072).
Patients
Electronic medical records of all postmenopausal women with osteoporosis who underwent lumbar instrumented intervertebral fusion surgery between July 2016 and May 2018 were retrospectively reviewed. Postmenopause was defined by a minimum of 12 consecutive months of amenorrhea. Intervertebral spinal fusion was indicated for lumbar degenerative diseases, including disc herniation with instability, spinal stenosis, degenerative spondylolisthesis, isthmic spondylolisthesis, and degenerative scoliosis. Osteoporosis was defined by a T-score ≤-2.5 on dual-energy X-ray absorptiometry (DEXA) measures obtained 2 weeks before surgery. Only patients who underwent follow-up DEXA evaluation at 6–12 months after surgery were included. Excluded patients were those who required intervertebral fusion of >3 levels or for whom the first lumbar vertebra (L1) was included. Moreover, at least one lumbar level had to be free of pedicle screws to allow BMD measurement, because only L1-L4 were included during lumbar BMD measurement by DEXA in our hospital. Additionally, patients with a prior history of lumbar surgery and those who required lumbar surgery during the follow-up period were excluded. Patients with non-degenerative lumbar disorders that may affect bone metabolism (such as cancer, infection, and trauma) and those with osteoporosis secondary to various metabolic diseases (such as thyroid or parathyroid disease, and other endocrine diseases), those who required use of a lumbar brace for >2 months after surgery, and those with any disability that limited the patient’s walking ability for >1 week during the follow-up period were excluded. Of note, all patients were asked to use a lumbar brace while walking for 4–6 weeks after surgery.
After screening for inclusion and exclusion criteria, 291 patients were eligible for our study. Of these, 46 patients did not receive anti-osteoporosis treatment either before surgery or during the follow-up period for surgeons or patients’ concern about the impact of side effect after lumbar spinal fusion surgery. The anti-osteoporosis treatments include the use of bisphosphonates, parathyroid hormone, calcitonin, estrogen. The remaining 245 patients received anti-osteoporosis therapy; of these, 193 patients were treated with intravenous ZA (one dose, 5 mg), during the perioperative period, and with other anti-osteoporosis drugs used in the other 52 patients, including alendronate, teriparatide, and calcitonin. All 291 patients received oral calcium and vitamin D supplements during the follow-up period. To control for important confounding factors, 46 patients from the 193 treated with ZA were matched to the 46 in the untreated group for age and body mass index (BMI).
Surgical Procedure
All spinal surgeries, including open posterior/transforaminal lumbar interbody fusion (PLIF/TLIF), minimally invasive TLIF (MI-TLIF) and oblique lateral interbody fusion (OLIF) with pedicle screw (PS) implantation, are performed by senior surgeons in our department. The proper kind of operation and the extent of dorsal decompression are determined by the extent of dorsal decompression. All the operations are performed under general anesthesia at prone posture, except for OLIF in which right-sided lateral position is used.
PLIF/TLIF: Posterior midline incision is made and the posterior elements of the spine are exposed. After pedicle screw insertion, a medial facetectomy was performed. Then the nerve root is mobilized medially to get access to the disc space. In TLIF procedure, the superior and inferior articular processes of the facet joint are resected and the disc is exposed in the neuroforamen. After removal of the disc and scraping of the endplates, the anterior part of the disc space is packed with autologous bone chips. The disc space is measured by trial insertion of variously sized spacers, then a sizeable cage is inserted.
MI-TLIF: The mobile C/G-arm x-ray machine is used to confirm the desired operative level. A parasagittal incision was made 4 to 5 cm lateral to the midline, and sequential soft tissue dilators are inserted down to the facet complex. Subsequently, facetectomy and discectomy are performed. After bone chips and a sizeable cage inserted, the percutaneous pedicle screw-rod construct is placed through the same incision and another similar construct through a contralateral incision.
OLIF: A skin incision of about 4 cm on the front line of the iliac crest is made at the left lower abdomen and blunt forceps are used to separate subcutaneous tissue and muscle of abdomen. The mobile C/G-arm x-ray machine is used to confirm the desired operative level, then sequential soft tissue dilators and the working channel are inserted down. After removal of the disc and scraping of the endplates, a proper sized cage is inserted. After the anterolateral procedure, patients are placed in the prone position for percutaneous pedicle screw fixation which is guided under C/G-arm fluoroscopy.
Data Collection
All data was collected retrospectively from patients’ medical records using standardized forms, including demographics (age, BMI, years since menopause); surgical details of levels included (fusion levels and cephalad levels); discharge time after surgery and BMD values. BMD values (g/cm2) were recorded for the overall lumbar spine, for the levels cephalad to the fused segments, and the femoral neck.
Statistical Analysis
Continuous variables were reported as a mean ± standard deviation. Pre- to postoperative change in BMD was evaluated using paired t-tests, with the significance of identified differences confirmed using the non-parametric Wilcoxon signed-rank test. Differences between the untreated and ZA-treated groups were evaluated using Student’s t-test or a chi-squared test, as appropriate for the data distribution. All analyses and case match were performed using Statistical Analysis System (version 9.4, SAS Institute Inc., Cary, NC, USA) and Microsoft Excel, with a P-value <0.05 considered significant.
Results
Of the 92 patients in the 2 groups, the mean age of the study group was 67.25 ± 10.27 years, with a mean follow-up period of 8.89 ± 1.8 months. Patients’ baseline demographic characteristics were balanced between groups (Table 1). There was also no significant difference about the year since menopause in treated and untreated groups, 17.72 ± 10.48 and 18.02 ± 10.25, respectively.
Description of Demographic And Surgery Information of Treated Group and Untreated Group.
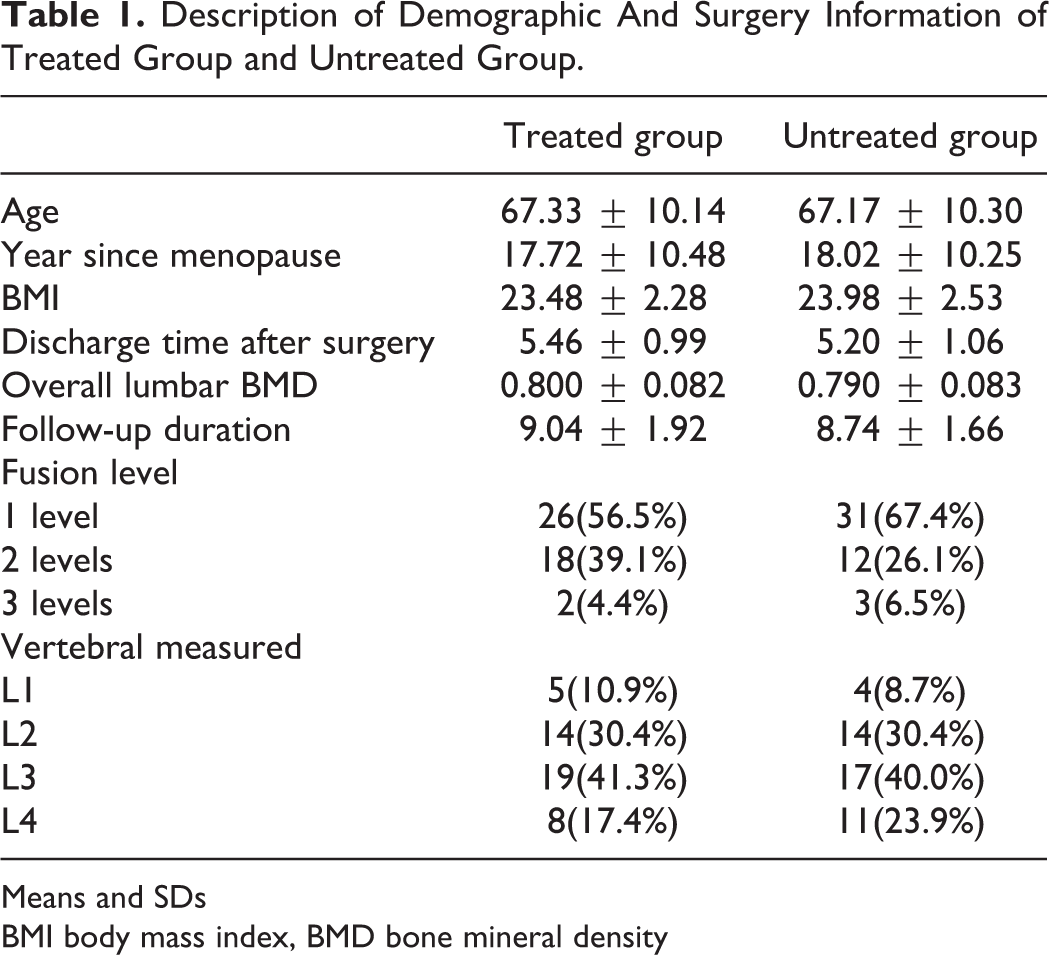
Means and SDs
BMI body mass index, BMD bone mineral density
The number and location of lumbar levels involved, and BMD parameters for both the ZA-treated and untreated groups were similar between groups. In the ZA-treated group, 26 patients underwent fusion at one level, 18 at 2 levels, and 2 at 3 levels. In the untreated group, 31 underwent fusion at one level, 12 at 2 levels, and 3 at 3 levels. The overall lumbar BMD was 0.800 ± 0.082 g/cm2 and 0.790 ± 0.083 g/cm2 in the treated and untreated group, respectively. There was also no significant difference in discharge time after surgery (treated group: 5.46 ± 0.99, untreated group: 5.20 ± 1.06).
The femoral neck BMD increased in the ZA-treated group, from 0.629 ± 0.074 g/cm2 to 0.639 ± 0.081 g/cm2, while decreasing in the untreated group, from 0.618 ± 0.067 g/cm2 to 0.611 ± 0.087 g/cm2 (Supplemental File 1). Although both of these within-group changes were non-significant, the pre- to postoperative change in femoral neck BMD between the 2 groups was significant (1.52 ± 5.88% vs. -1.28 ± 6.58% for the ZA-treated and untreated groups, respectively, P = 0.036). The mean postoperative vertebral BMD value of the cephalad region in the untreated group was significantly lower than the preoperative value (0.710 ± 0.142 g/cm2 vs. 0.807 ± 0.105 g/cm2, respectively, P < 0.001), with no significant difference in the ZA-treated group (0.808 ± 0.095 g/cm2 vs. 0.814 ± 0.091 g/cm2, respectively, P > 0.05). The adjacent vertebral BMD loss was significantly higher in the non-treated than in the ZA-treated group (-11.47 ± 16.45% vs. -0.76 ± 4.71%, respectively, P < 0.001; Table 2). There was no correlation between BMD loss and the number of fused segments in both groups.
Cephalad Adjacent Vertebral and Femoral Neck BMD Value Change.
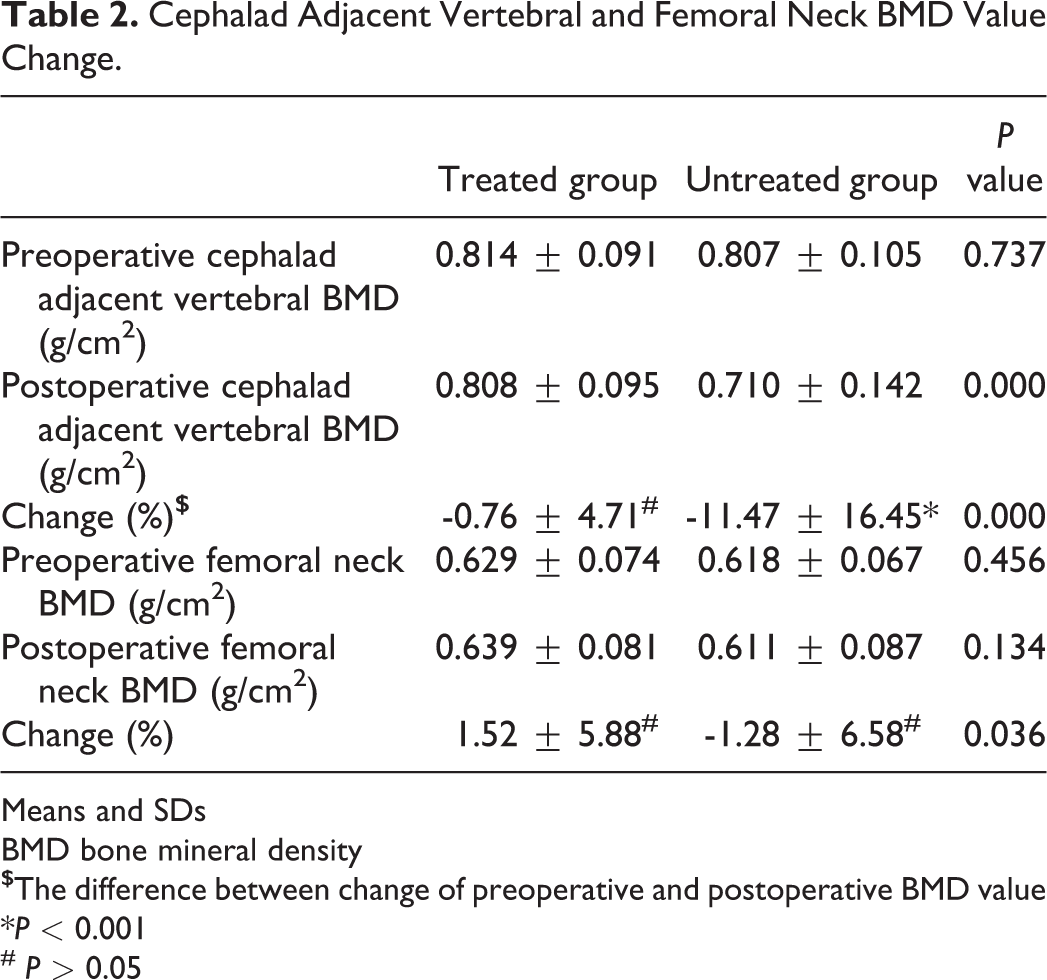
Means and SDs
BMD bone mineral density
*P < 0.001
# P > 0.05
Discussion
To the best of our knowledge, this is the first study which compared the effect of anti-osteoporosis treatment, using intravenous, ZA during the perioperative period on the adjacent vertebral body BMD, over a mean follow-up period of 9 months, among postmenopausal women with osteoporosis.
Anti-osteoporotic treatment using ZA prevented a rapid bone loss and decrease in vertebral BMD after instrumented intervertebral fusion surgery which was significant, with a decrease of only -0.76 ± 4.71% compared to -11.47 ± 16.45% for the untreated group. Significant decrease in adjacent cephalad vertebral BMD has been reported after spinal instrumentation surgery.9-11 Lipscomb et al. reported an average BMD loss of 15.7% after spinal instrumentation surgery, with a maximum loss occurring between 3 to 12 months postoperatively, and at 7 months on average. 10 Bogdanffy et al. reported a significant decrease in vertebral BMD within the one and two spinal segments above of the level of arthrodesis at 3 months postoperatively, with the bone density remaining low up to 6 months postoperatively. 9 Ozaksoy et al. noted a decrease in vertebral body BMD values for the segments adjacent (cephalad and caudad) to the segment fused using transpedicular screw fixation, at an average of 9 months postoperatively. 11 In our study, patients had a mean follow-up period of 9 months (range, 6–12 months), with an average bone loss of 11.47% in the cephalad vertebra adjacent to the level of arthrodesis. The absence of a significant correlation between BMD loss and the number of fused segments that we identified was consistent with previous findings. 11 We note that the average duration of menopause in our study group was 18 years and 17 years in the ZA-treated and untreated groups, respectively. A previous study reported a decrease in the rate of bone loss among postmenopausal women after the age of 60 years, with an increase in the lumbar spine and total body BMD. 15 This may explain the fact that bone loss after spinal fusion was not higher among postmenopausal women with osteoporosis than reported in younger patients.9-11 The cause of early vertebral BMD loss after spinal fusion surgery is not yet fully understood. One possible explanation is postoperative immobilization, altered segmental biomechanics after fusion, and bone remodeling. The effect of bracing after surgery is inconclusive due to limited and low-quality evidence.16,17 In our study, use of a lumbar brace was recommended for 4–6 weeks postoperatively. Fear of movement after spinal fusion surgery has previously been reported, leading to relative inactivity. 18 We note that we did not evaluate patients’ physical activity during the postoperative follow-up but did exclude patients who had a >1-week limitation in walking. Even with this exclusion, a significant bone loss of adjacent cephalad vertebral BMD was still found after spinal fusion.
A previous study reported a gradual increase in BMD of the adjacent cephalad vertebrae at 1-year after spinal fusion, after an early rapid bone loss. 10 Ozaksoy et al. 11 reported a decrease in BMD values for the vertebra above the fusion segment over an average follow-up of 9 months after surgery and that the significant BMD loss persisted over an average follow-up of 32 months postoperatively. These results suggest that rapid bone loss of the adjacent cephalad vertebra is more severe within the first year of spinal instrumentation surgery. Future studies should focus on the mechanisms of early rapid bone loss in adjacent cephalad vertebrae.
The impact of lumbar instrumented intervertebral fusion on the development of adjacent VCFs has been discussed in some studies, with evidence of an increased risk after spinal arthrodesis.4,5,19-22 Yang et al. reported new VCFs in 150 of 1348 patients (11.1%) after posterior lumbar interbody fusion, with 108 of these (72%) being at adjacent segments. 19 Although no study has examined the relationship between new VCFs at the adjacent segment and bone loss after spinal instrumentation surgery directly, it is known that women, the elderly, and patients with osteoporosis have a specific higher incidence of new VCFs after spinal fusion, especially within the first 12 months postoperatively.5,19 In our study, the rate of bone loss in the vertebral body was not significantly higher than previously reported; however, our patients, who were postmenopausal women with osteoporosis, had a lower baseline BMD and, thus, were at a higher risk for osteoporotic vertebral fracture. 23 Consequently, any decrease in BMD of the adjacent vertebral body after instrumented intervertebral fusion in postmenopausal patients with osteoporosis is a serious concern.
Although instrumented spinal fusion surgery is widely used and the clinical outcomes are usually satisfactory, studies have shown the benefit of aggressive treatment of osteoporosis as a key factor for reducing the risk of subsequent VCFs after spinal fusion surgery. Both bisphosphonate and teriparatide treatment have been associated with a reduce incidence of subsequent VCFs after instrumented fusion surgery.13,24,25 Although vertebral body BMD loss associated with spinal fusion surgery during the early term follow-up, which may increase the risk for adjacent VCFs, has been well described in humans, interventional treatments to decrease the rapid rate of BMD loss early after spinal fusion have not been documented. In this regard, our study is the first to report a significant decrease in BMD of the adjacent cephalad vertebra among postmenopausal women with osteoporosis, placing these women at high risk for new VCFs after spinal fusion, further evidence of possible complications after spinal surgery. Although the antiresorptive mechanism is not completely understood, it’s found that ZA, a third generation of bisphosphonates, inhibits osteoclastic activity and induces osteoclast apoptosis in vitro. Approval is given for osteoporosis, multiple myeloma and metastatic bone lesions from solid tumors with different doses. It’s proved that an annual infusion of 5 mg of ZA significantly increased vertebra and hip BMD and also reduced the risk of fracture at all key osteoporotic fracture sites. 26 Our findings reveal the benefit of perioperative intravenous ZA, as an anti-osteoporotic treatment, in preventing rapid bone loss of surrounding vertebral BMD after instrumented intervertebral fusion surgery, with the measured effect being significantly different from the untreated group. Considering the high risk of new VCFs after spinal fusion, the results indicate that aggressive treatment of osteoporosis should be provided perioperatively to postmenopausal women with osteoporosis. However, attentions should be paid to side effects of ZA. The most common adverse reactions include fever, muscle pain, nausea and arthralgia, and the patients’ status and benefit should be taken into account enough for anti-osteoporotic treatment by ZA.
The limitations of our study need to be acknowledged. The first is that it is a retrospective study with a relatively small sample size and short following-up period; as such, a selection bias cannot be denied, with consequent limit in between-group comparability. We do note that we used a case-control design to overcome these disadvantages. Although we did not compare the difference of the fusion rate and the change of clinical function score in our study, previous studies have proved that the treatment with ZA in osteoporotic patients improves the fusion rate and the clinical outcomes. The second limitation was our use of DEXA which was used to evaluate the change in vertebral BMD which may not be sensitive to degenerative changes. As well, presence of aortic calcification might also affect DEXA-based BMD measurements. Quantitative computerized tomography, which provides true volumetric measurements, should be used for the measurement of BMD in the future.
Topics for further research in this area include investigating the relationship between the decreased BMD in cephalad vertebrae and the incidence of proximal VCFs after spinal fusion surgery directly, as well as the prevention of bone loss in cephalad vertebrae and the incidence of VCFs. More studies about the major mechanisms of the adjacent vertebral body bone mineral density change after instrumented intervertebral fusion are warranted.
Conclusion
The findings of our study revealed a significant decrease in cephalad vertebral BMD values among postmenopausal women with osteoporosis following spinal fusion surgery. Anti-osteoporosis treatment, provided perioperatively using intravenous with ZA, can significantly protect against a loss of BMD of the adjacent vertebral body.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_21925682211027833 - Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis
Supplemental Material, sj-docx-1-gsj-10.1177_21925682211027833 for Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis by Junjun Fan, Tao Liu, Xin Dong, Siguo Sun, Hongtao Zhang, Chunbao Yang, Xin Yin, Bo Liao and Xiaoxiang Li in Global Spine Journal
Supplemental Material
Supplemental Material, sj-docx-2-gsj-10.1177_21925682211027833 - Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis
Supplemental Material, sj-docx-2-gsj-10.1177_21925682211027833 for Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis by Junjun Fan, Tao Liu, Xin Dong, Siguo Sun, Hongtao Zhang, Chunbao Yang, Xin Yin, Bo Liao and Xiaoxiang Li in Global Spine Journal
Supplemental Material
Supplemental Material, sj-docx-3-gsj-10.1177_21925682211027833 - Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis
Supplemental Material, sj-docx-3-gsj-10.1177_21925682211027833 for Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis by Junjun Fan, Tao Liu, Xin Dong, Siguo Sun, Hongtao Zhang, Chunbao Yang, Xin Yin, Bo Liao and Xiaoxiang Li in Global Spine Journal
Supplemental Material
Supplemental Material, sj-pptx-4-gsj-10.1177_21925682211027833 - Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis
Supplemental Material, sj-pptx-4-gsj-10.1177_21925682211027833 for Effect of Zoledronic Acid on the Vertebral Body Bone Mineral Density After Instrumented Intervertebral Fusion in Postmenopausal Women With Osteoporosis by Junjun Fan, Tao Liu, Xin Dong, Siguo Sun, Hongtao Zhang, Chunbao Yang, Xin Yin, Bo Liao and Xiaoxiang Li in Global Spine Journal
Footnotes
Acknowledgment
The authors would like to thank Ms. Li Shuang for her comments and contributions to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.